


Factors Associated with Prolonged Mechanical Ventilation and 30-Day Mortality in Intubated COVID-19 Patients with Invasive Fungal Infections: A Retrospective Observational Study

 ,
,  ,
,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Data Collection
2.3. Detection of Fungi
2.4. Definitions
2.5. Outcomes
2.6. Statistical Analysis
3. Results
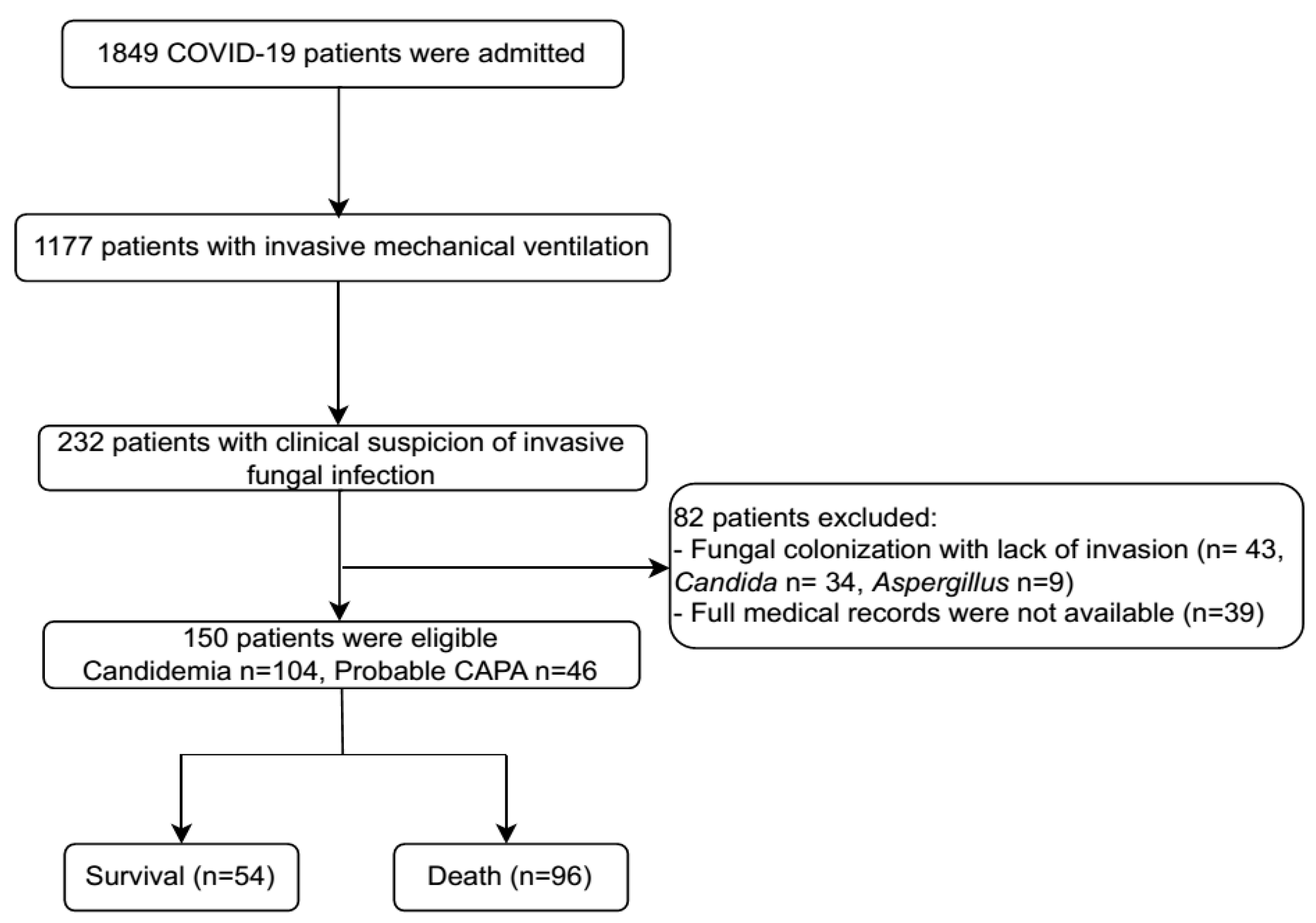
3.1. Characteristics of the Study Patients and Outcomes
3.2. Laboratory Parameters on the Day of IFI Diagnosis of the Study Patients
3.3. Radiologic Findings, Interventions and Medications
3.4. Factors Associated with PMV
3.5. Risk Factors for 30-Day Mortality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AKI | Acute Kidney Injury |
| BMI | Body Mass Index |
| CAIFIs | COVID-19-associated Invasive Fungal Infections |
| CAM | COVID-19-associated Mucormycosis |
| CAPA | COVID-19-associated Pulmonary Aspergillosis |
| CCA | Chromogenic Candida Agar |
| CKD | Chronic Kidney Disease |
| COPD | Chronic Obstructive Pulmonary Disease |
| COVID-19 | Corona Virus Disease 2019 |
| CRP | C-Reactive Protein |
| CT | Computed Tomography |
| ECMO | Extracorporeal Membrane Oxygenation |
| ETA | Endotracheal Aspirate |
| IFIs | Invasive Fungal Infections |
| ICUs | Intensive Care Units |
| IMV | Intensive Mechanical Ventilation |
| LMICs | Low- and middle-income Countries |
| PMV | Prolonged Mechanical Ventilation |
| CRRT | Continuous Renal Replacement Therapy |
| RT-PCR | Reverse Transcription Polymerase Chain Reaction |
| SARS-CoV-2 | Severe Acute Respiratory Syndrome Coronavirus 2 |
| SDA | Sabouraud Dextrose Agar |
| VAP | Ventilator-associated Pneumonia |
References
- Reyes, L.F.; Rodriguez, A.; Fuentes, Y.V.; Duque, S.; García-Gallo, E.; Bastidas, A.; Serrano-Mayorga, C.C.; Ibáñez-Prada, E.D.; Moreno, G.; Ramirez-Valbuena, P.C. Risk factors for developing ventilator-associated lower respiratory tract infection in patients with severe COVID-19: A multinational, multicentre study, prospective, observational study. Sci. Rep. 2023, 13, 6553. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. COVID-19 Epidemiological Update. Available online: https://www.who.int/publications/m/item/covid-19-epidemiological-update-edition-172 (accessed on 15 November 2024).
- Meier, N.; Perner, A.; Plovsing, R.; Christensen, S.; Poulsen, L.M.; Brøchner, A.C.; Rasmussen, B.S.; Helleberg, M.; Jensen, J.U.; Andersen, L.P. Long-term outcomes in COVID-19 patients admitted to intensive care in Denmark: A nationwide observational study. Acta Anaesthesiol. Scand. 2023, 67, 1239–1248. [Google Scholar] [CrossRef] [PubMed]
- Grasselli, G.; Greco, M.; Zanella, A.; Albano, G.; Antonelli, M.; Bellani, G.; Bonanomi, E.; Cabrini, L.; Carlesso, E.; Castelli, G. Risk factors associated with mortality among patients with COVID-19 in intensive care units in Lombardy, Italy. JAMA Intern. Med. 2020, 180, 1345–1355. [Google Scholar] [CrossRef]
- Ceballos, M.E.; Nuñez, C.; Uribe, J.; Vera, M.M.; Castro, R.; García, P.; Arriata, G.; Gándara, V.; Vargas, C.; Dominguez, A. Secondary respiratory early and late infections in mechanically ventilated patients with COVID-19. BMC Infect. Dis. 2022, 22, 760. [Google Scholar] [CrossRef]
- Bartoletti, M.; Pascale, R.; Cricca, M.; Rinaldi, M.; Maccaro, A.; Bussini, L.; Fornaro, G.; Tonetti, T.; Pizzilli, G.; Francalanci, E.; et al. Epidemiology of Invasive Pulmonary Aspergillosis Among Intubated Patients with COVID-19: A Prospective Study. Clin. Infect. Dis. 2020, 73, e3606–e3614. [Google Scholar] [CrossRef]
- Dellière, S.; Dudoignon, E.; Fodil, S.; Voicu, S.; Collet, M.; Oillic, P.-A.; Salmona, M.; Dépret, F.; Ghelfenstein-Ferreira, T.; Plaud, B.; et al. Risk factors associated with COVID-19-associated pulmonary aspergillosis in ICU patients: A French multicentric retrospective cohort. Clin. Microbiol. Infect. 2021, 27, 790.E1–790.E5. [Google Scholar] [CrossRef] [PubMed]
- Gangneux, J.-P.; Dannaoui, E.; Fekkar, A.; Luyt, C.-E.; Botterel, F.; De Prost, N.; Tadié, J.-M.; Reizine, F.; Houzé, S.; Timsit, J.-F.; et al. Fungal infections in mechanically ventilated patients with COVID-19 during the first wave: The French multicentre MYCOVID study. Lancet Respir. Med. 2022, 10, 180–190. [Google Scholar] [CrossRef]
- Kayaaslan, B.; Eser, F.; Kaya Kalem, A.; Bilgic, Z.; Asilturk, D.; Hasanoglu, I.; Ayhan, M.; Tezer Tekce, Y.; Erdem, D.; Turan, S. Characteristics of candidemia in COVID-19 patients; increased incidence, earlier occurrence and higher mortality rates compared to non-COVID-19 patients. Mycoses 2021, 64, 1083–1091. [Google Scholar] [CrossRef]
- Hoenigl, M.; Seidel, D.; Sprute, R.; Cunha, C.; Oliverio, M.; Goldman, G.H.; Ibrahim, A.S.; Carvalho, A. COVID-19-associated fungal infections. Nat. Microbiol. 2022, 7, 1127–1140. [Google Scholar] [CrossRef]
- Søvik, S.; Barrat-Due, A.; Kåsine, T.; Olasveengen, T.; Strand, M.W.; Tveita, A.A.; Berdal, J.E.; Lehre, M.A.; Lorentsen, T.; Heggelund, L.; et al. Corticosteroids and superinfections in COVID-19 patients on invasive mechanical ventilation. J. Infect. 2022, 85, 57–63. [Google Scholar] [CrossRef]
- Shishido, A.A.; Mathew, M.; Baddley, J.W. Overview of COVID-19-associated invasive fungal infection. Curr. Fungal Infect. Rep. 2022, 16, 87–97. [Google Scholar] [CrossRef] [PubMed]
- Giamarellos-Bourboulis, E.J.; Netea, M.G.; Rovina, N.; Akinosoglou, K.; Antoniadou, A.; Antonakos, N.; Damoraki, G.; Gkavogianni, T.; Adami, M.-E.; Katsaounou, P. Complex immune dysregulation in COVID-19 patients with severe respiratory failure. Cell Host Microbe 2020, 27, 992–1000.e3. [Google Scholar] [CrossRef]
- Luyt, C.-E.; Sahnoun, T.; Gautier, M.; Vidal, P.; Burrel, S.; Pineton de Chambrun, M.; Chommeloux, J.; Desnos, C.; Arzoine, J.; Nieszkowska, A. Ventilator-associated pneumonia in patients with SARS-CoV-2-associated acute respiratory distress syndrome requiring ECMO: A retrospective cohort study. Ann. Intensive Care 2020, 10, 158. [Google Scholar] [CrossRef] [PubMed]
- Helms, J.; Tacquard, C.; Severac, F.; Leonard-Lorant, I.; Ohana, M.; Delabranche, X.; Merdji, H.; Clere-Jehl, R.; Schenck, M.; Fagot Gandet, F. High risk of thrombosis in patients with severe SARS-CoV-2 infection: A multicenter prospective cohort study. Intensive Care Med. 2020, 46, 1089–1098. [Google Scholar] [CrossRef]
- Tsitsiklis, A.; Zha, B.S.; Byrne, A.; Devoe, C.; Levan, S.; Rackaityte, E.; Sunshine, S.; Mick, E.; Ghale, R.; Jauregui, A. Impaired immune signaling and changes in the lung microbiome precede secondary bacterial pneumonia in COVID-19. Res. Sq. 2021. [Google Scholar] [CrossRef]
- Hurt, W.; Youngs, J.; Ball, J.; Edgeworth, J.; Hopkins, P.; Jenkins, D.R.; Leaver, S.; Mazzella, A.; Molloy, S.F.; Schelenz, S. COVID-19-associated pulmonary aspergillosis in mechanically ventilated patients: A prospective, multicentre UK study. Thorax 2024, 79, 75–82. [Google Scholar] [CrossRef]
- Briano, F.; Magnasco, L.; Sepulcri, C.; Dettori, S.; Dentone, C.; Mikulska, M.; Ball, L.; Vena, A.; Robba, C.; Patroniti, N. Candida auris candidemia in critically ill, colonized patients: Cumulative incidence and risk factors. Infect. Dis. Ther. 2022, 11, 1149–1160. [Google Scholar] [CrossRef]
- Hoenigl, M.; Seidel, D.; Carvalho, A.; Rudramurthy, S.M.; Arastehfar, A.; Gangneux, J.-P.; Nasir, N.; Bonifaz, A.; Araiza, J.; Klimko, N. The emergence of COVID-19 associated mucormycosis: A review of cases from 18 countries. Lancet Microbe 2022, 3, e543–e552. [Google Scholar] [CrossRef]
- Huang, H.Y.; Huang, C.Y.; Li, L.F. Prolonged Mechanical Ventilation: Outcomes and Management. J. Clin. Med. 2022, 11, 2451. [Google Scholar] [CrossRef]
- Damuth, E.; Mitchell, J.A.; Bartock, J.L.; Roberts, B.W.; Trzeciak, S. Long-term survival of critically ill patients treated with prolonged mechanical ventilation: A systematic review and meta-analysis. Lancet Respir. Med. 2015, 3, 544–553. [Google Scholar] [CrossRef]
- Melamed, R.; Paz, F.; Jepsen, S.; Smith, C.; Saavedra, R.; Mulder, M.; Masood, A.; Huelster, J.; Kirkland, L.; Guenther, A. Prognostic factors and outcomes in COVID-19 patients requiring prolonged mechanical ventilation: A retrospective cohort study. Ther. Adv. Respir. Dis. 2022, 16, 17534666221086415. [Google Scholar] [CrossRef] [PubMed]
- 4689/QĐBYT; Guideline for Diagnosis and Treatment of COVID-19. Ministry of Health of Vietnam: Hanoi, Vietnam, 2021.
- 250/QĐBYT; Guideline for Diagnosis and Treatment of COVID-19. Ministry of Health of Vietnam: Hanoi, Vietnam, 2022.
- 26/QĐBYT; Guidelines for Technical Procedures in Medical Microbiology. Ministry of Health of Vietnam: Hanoi, Vietnam, 2013.
- Domecq, J.P.; Lal, A.; Sheldrick, C.R.; Kumar, V.K.; Boman, K.; Bolesta, S.; Bansal, V.; Harhay, M.O.; Garcia, M.A.; Kaufman, M. Outcomes of patients with coronavirus disease 2019 receiving organ support therapies: The international viral infection and respiratory illness universal study registry. Crit. Care Med. 2021, 49, 437–448. [Google Scholar] [CrossRef]
- Bassetti, M.; Azoulay, E.; Kullberg, B.J.; Ruhnke, M.; Shoham, S.; Vazquez, J.; Giacobbe, D.R.; Calandra, T. EORTC/MSGERC Definitions of Invasive Fungal Diseases: Summary of Activities of the Intensive Care Unit Working Group. Clin. Infect. Dis. 2021, 72, S121–S127. [Google Scholar] [CrossRef] [PubMed]
- Vaseghi, N.; Sharifisooraki, J.; Khodadadi, H.; Nami, S.; Safari, F.; Ahangarkani, F.; Meis, J.F.; Badali, H.; Morovati, H. Global prevalence and subgroup analyses of coronavirus disease (COVID-19) associated Candida auris infections (CACa): A systematic review and meta-analysis. Mycoses 2022, 65, 683–703. [Google Scholar] [CrossRef] [PubMed]
- Zuniga-Moya, J.C.; Papadopoulos, B.; Mansoor, A.-E.-R.; Mazi, P.B.; Rauseo, A.M.; Spec, A. Incidence and Mortality of COVID-19-Associated Invasive Fungal Infections Among Critically Ill Intubated Patients: A Multicenter Retrospective Cohort Analysis. Open Forum Infect. Dis. 2024, 11, ofae108. [Google Scholar] [CrossRef]
- Khiabani, K.; Amirzade-Iranaq, M.H.; Ahmadi, H. An Update on COVID-19 Associated Mucormycosis Characteristics, Risk Factors, and Outcomes: A Systematic Review and Meta-Analysis. Curr. Fungal Infect. Rep. 2023, 17, 282–295. [Google Scholar] [CrossRef]
- Duong, T.M.N.; Le, M.H.; Beardsley, J.; Denning, D.W.; Le, N.H.; Nguyen, B.N.T. Updated estimation of the burden of fungal disease in Vietnam. Mycoses 2023, 66, 346–353. [Google Scholar] [CrossRef]
- Fang, W.; Wu, J.; Cheng, M.; Zhu, X.; Du, M.; Chen, C.; Liao, W.; Zhi, K.; Pan, W. Diagnosis of invasive fungal infections: Challenges and recent developments. J. Biomed. Sci. 2023, 30, 42. [Google Scholar] [CrossRef]
- Gautam, A.K.; Verma, R.K.; Avasthi, S.; Sushma; Bohra, Y.; Devadatha, B.; Niranjan, M.; Suwannarach, N. Current Insight into Traditional and Modern Methods in Fungal Diversity Estimates. J. Fungi 2022, 8, 226. [Google Scholar] [CrossRef]
- Pappas, P.G.; Lionakis, M.S.; Arendrup, M.C.; Ostrosky-Zeichner, L.; Kullberg, B.J. Invasive candidiasis. Nat. Rev. Dis. Primers 2018, 4, 18026. [Google Scholar] [CrossRef]
- Riwes, M.M.; Wingard, J.R. Diagnostic methods for invasive fungal diseases in patients with hematologic malignancies. Expert Rev. Hematol. 2012, 5, 661–669. [Google Scholar] [CrossRef]
- Maschmeyer, G. Invasive fungal disease: Better survival through early diagnosis and therapeutic intervention. Expert Rev. Anti-Infect. Ther. 2011, 9, 279–281. [Google Scholar] [CrossRef] [PubMed]
- Grasselli, G.; Zanella, A.; Carlesso, E.; Florio, G.; Canakoglu, A.; Bellani, G.; Bottino, N.; Cabrini, L.; Castelli, G.P.; Catena, E.; et al. Association of COVID-19 Vaccinations with Intensive Care Unit Admissions and Outcome of Critically Ill Patients with COVID-19 Pneumonia in Lombardy, Italy. JAMA Netw. Open 2022, 5, e2238871. [Google Scholar] [CrossRef]
- Grapsa, E.; Adamos, G.; Andrianopoulos, I.; Tsolaki, V.; Giannakoulis, V.G.; Karavidas, N.; Giannopoulou, V.; Sarri, K.; Mizi, E.; Gavrielatou, E.; et al. Association Between Vaccination Status and Mortality Among Intubated Patients with COVID-19–Related Acute Respiratory Distress Syndrome. JAMA Netw. Open 2022, 5, e2235219. [Google Scholar] [CrossRef] [PubMed]
- de Moraes, E.V.; Pires, M.C.; Costa, A.A.A.; Nunes, A.G.S.; de Amorim, C.L.; Manenti, E.R.F.; Lucas, F.B.; Rodrigues, F.D.A.; Anschau, F.; do Nascimento, G.F.; et al. Comprehensive statistical analysis reveals significant benefits of COVID-19 vaccination in hospitalized patients: Propensity score, covariate adjustment, and feature importance by permutation. BMC Infect. Dis. 2024, 24, 1052. [Google Scholar] [CrossRef]
- World Health Organization. COVID-19 in Viet Nam Situation Report 68. Available online: https://www.who.int/vietnam/internal-publications-detail/covid-19-in-viet-nam-situation-report-68 (accessed on 15 November 2024).
- World Health Organization. COVID-19 in Viet Nam Situation Report 104. Available online: https://www.who.int/vietnam/internal-publications-detail/covid-19-in-viet-nam-situation-report-104 (accessed on 15 November 2024).
- Wang, Y.; Zhao, J.; Yang, L.; Hu, J.; Yao, Y. Value of the Neutrophil-Lymphocyte Ratio in Predicting COVID-19 Severity: A Meta-Analysis. Dis. Markers 2021, 2021, 2571912. [Google Scholar] [CrossRef]
- Melenotte, C.; Silvin, A.; Goubet, A.-G.; Lahmar, I.; Dubuisson, A.; Zumla, A.; Raoult, D.; Merad, M.; Gachot, B.; Hénon, C. Immune responses during COVID-19 infection. Oncoimmunology 2020, 9, 1807836. [Google Scholar] [CrossRef]
- Arcanjo, A.; Logullo, J.; Menezes, C.C.B.; de Souza Carvalho Giangiarulo, T.C.; Dos Reis, M.C.; de Castro, G.M.M.; da Silva Fontes, Y.; Todeschini, A.R.; Freire-de-Lima, L.; Decoté-Ricardo, D. The emerging role of neutrophil extracellular traps in severe acute respiratory syndrome coronavirus 2 (COVID-19). Sci. Rep. 2020, 10, 19630. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.; Que, J.; Peng, Y.; Ye, H.; Xiang, H.; Han, Y.; Wang, J.; Ji, K. The neutrophil-lymphocyte ratio: A promising predictor of mortality in coronary care unit patients—A cohort study. Int. Immunopharmacol. 2019, 74, 105692. [Google Scholar] [CrossRef]
- Marik, P.E.; Stephenson, E. The ability of Procalcitonin, lactate, white blood cell count and neutrophil-lymphocyte count ratio to predict blood stream infection. Analysis of a large database. J. Crit. Care 2020, 60, 135–139. [Google Scholar] [CrossRef]
- Choi, D.-E.; Kim, D.K.; Park, S.; Lee, S.H.; Park, O.; Kim, T.; Yeo, H.J.; Jang, J.H.; Cho, W.H.; Lee, S.I.; et al. Clinical characteristics and prognosis of patients with COVID-19 on mechanical ventilation undergoing continuous renal replacement therapy. PLoS ONE 2024, 19, e0297344. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Tian, S.; Guo, H. Acute kidney injury and renal replacement therapy in COVID-19 patients: A systematic review and meta-analysis. Int. Immunopharmacol. 2021, 90, 107159. [Google Scholar] [CrossRef]
- Fisher, M.; Neugarten, J.; Bellin, E.; Yunes, M.; Stahl, L.; Johns, T.S.; Abramowitz, M.K.; Levy, R.; Kumar, N.; Mokrzycki, M.H.; et al. AKI in Hospitalized Patients with and Without COVID-19: A Comparison Study. J. Am. Soc. Nephrol. 2020, 31, 2145–2157. [Google Scholar] [CrossRef] [PubMed]
- Batlle, D.; Soler, M.J.; Sparks, M.A.; Hiremath, S.; South, A.M.; Welling, P.A.; Swaminathan, S. Acute kidney injury in COVID-19: Emerging evidence of a distinct pathophysiology. J. Am. Soc. Nephrol. 2020, 31, 1380–1383. [Google Scholar] [CrossRef]
- Ahmadian, E.; Hosseiniyan Khatibi, S.M.; Razi Soofiyani, S.; Abediazar, S.; Shoja, M.M.; Ardalan, M.; Zununi Vahed, S. Covid-19 and kidney injury: Pathophysiology and molecular mechanisms. Rev. Med. Virol. 2021, 31, e2176. [Google Scholar] [CrossRef] [PubMed]
- Legrand, M.; Bell, S.; Forni, L.; Joannidis, M.; Koyner, J.L.; Liu, K.; Cantaluppi, V. Pathophysiology of COVID-19-associated acute kidney injury. Nat. Rev. Nephrol. 2021, 17, 751–764. [Google Scholar] [CrossRef]
- Cai, X.; Wu, G.; Zhang, J.; Yang, L. Risk Factors for Acute Kidney Injury in Adult Patients with COVID-19: A Systematic Review and Meta-Analysis. Front. Med. 2021, 8, 719472. [Google Scholar] [CrossRef]
- Lin, L.; Wang, X.; Ren, J.; Sun, Y.; Yu, R.; Li, K.; Zheng, L.; Yang, J. Risk factors and prognosis for COVID-19-induced acute kidney injury: A meta-analysis. BMJ Open 2020, 10, e042573. [Google Scholar] [CrossRef]
- Mehta, A.B.; Syeda, S.N.; Bajpayee, L.; Cooke, C.R.; Walkey, A.J.; Wiener, R.S. Trends in tracheostomy for mechanically ventilated patients in the United States, 1993–2012. Am. J. Respir. Crit. Care Med. 2015, 192, 446–454. [Google Scholar] [CrossRef]
- Breik, O.; Nankivell, P.; Sharma, N.; Bangash, M.N.; Dawson, C.; Idle, M.; Isherwood, P.; Jennings, C.; Keene, D.; Manji, M. Safety and 30-day outcomes of tracheostomy for COVID-19: A prospective observational cohort study. Br. J. Anaesth. 2020, 125, 872–879. [Google Scholar] [CrossRef]
- Martin-Villares, C.; Perez Molina-Ramirez, C.; Bartolome-Benito, M.; Bernal-Sprekelsen, M. Outcome of 1890 tracheostomies for critical COVID-19 patients: A national cohort study in Spain. Eur. Arch. Oto-Rhino-Laryngol. 2021, 278, 1605–1612. [Google Scholar] [CrossRef] [PubMed]
- Ji, Y.; Fang, Y.; Cheng, B.; Li, L.; Fang, X. Tracheostomy timing and clinical outcomes in ventilated COVID-19 patients: A systematic review and meta-analysis. Crit. Care 2022, 26, 40. [Google Scholar] [CrossRef] [PubMed]
- Trang, N.T.; Dien, T.C.; Tam, N.T.; Cuong, P.M.; Van Duyet, L.; Thuong, N.T.H.; Trang, V.D.; Thach, P.N.; van Doorn, H.R.; Kesteman, T.; et al. Detection of co-infection and recombination cases with Omicron and local Delta variants of SARS-CoV-2 in Vietnam. Sci. Rep. 2024, 14, 14225. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Parameter | Total (n = 150) | Length of MV | p-Value | |
|---|---|---|---|---|
| PMV (n = 65) | Short MV (n = 85) | |||
| Age (years) | 67 (58–76) | 66 (59–73) | 67 (57–77) | 0.341 |
| Gender | 0.553 | |||
| Male | 78 (52) | 32 (49.2) | 46 (54.1) | |
| Female | 72 (48) | 33 (50.8) | 39 (45.9) | |
| Comorbidity | ||||
| Diabetes | 37 (24.7) | 13 (20) | 24 (28.2) | 0.246 |
| CKD * | 13 (8.7) | 3 (4.6) | 10 (11.8) | 0.151 |
| Hypertension | 86 (57.3) | 32 (49.2) | 54 (63.5) | 0.096 |
| History of stroke * | 17 (11.3) | 2 (3.1) | 15 (17.6) | 0.008 |
| COPD * | 7 (4.7) | 3 (4.6) | 4 (4.7) | 0.979 |
| Malignancy * | 8 (5.3) | 4 (6.2) | 4 (4.7) | 0.727 |
| BMI | 0.021 | |||
| Non-obesity | 79 (52.7) | 27 (41.5) | 52 (61.2) | |
| Obesity | 71 (47.3) | 38 (58.5) | 33 (38.8) | |
| Prior COVID-19 vaccination | 38 (25.3) | 10 (15.4) | 28 (32.9) | 0.014 |
| SOFA score at IFI diagnosis | 4 (2–5) | 4 (2–5) | 3 (2–5) | 0.413 |
| Time to IFI diagnosis #, days | 9 (7–12) | 9 (7–13) | 8 (7–11) | 0.177 |
| PaO2/FiO2 at IFI diagnosis | 112.5 (81.3–156.8) | 100.0 (75.5–139.5) | 117.0 (89.3–170.8) | 0.136 |
| IFI diagnosis | 0.077 | |||
| Candidemia | 104 (69.3) | 40 (61.5) | 64 (75.3) | |
| Probable CAPA | 46 (30.7) | 25 (38.5) | 21 (24.7) | |
| Therapeutic interventions | ||||
| Tracheostomy | 80 (53.3) | 57 (87.7) | 23 (27.1) | <0.001 |
| ECMO * | 12 (8) | 11 (16.9) | 1 (1.2) | <0.001 |
| CRRT | 91 (60.7) | 51 (78.5) | 40 (47.1) | <0.001 |
| Corticoid treatment (days) | 11 (8–16) | 16 (9–23) | 10 (8–14) | 0.002 |
| Type of corticosteroid * | 0.860 | |||
| Dexamethasone | 135 (90) | 58 (89.2) | 77 (90.6) | |
| Methylprednisolone | 13 (8.6) | 6 (9.2) | 7 (8.2) | |
| Hydrocortisone | 1 (0.7) | 1 (1.6) | 0 (0) | |
| No corticosteroid | 1 (0.7) | 0 (0) | 1 (1.2) | |
| Antiviral medications * | 0.045 | |||
| No antiviral treatment | 100 (66.7) | 51 (78.5) | 49 (56.6) | |
| Remdesivir | 49 (32.6) | 13 (20) | 36 (42.4) | |
| Favipiravir | 1 (0.7) | 1 (1.5) | 0 (0) | |
| Outcomes | ||||
| Hospital LOS (days) | 21 (14–30) | 31 (23–44) | 15 (10–20) | <0.001 |
| 30-day mortality | 78 (52.0) | 30 (46.2) | 48 (56.5) | 0.089 |
| 14-day mortality | 43 (28.7) | 17 (26.2) | 26 (30.6) | 0.498 |
| In-hospital mortality | 96 (64.0) | 40 (61.5) | 56 (65.9) | 0.583 |
| Parameter | Total (n = 150) | Length of MV | p-Value | |
|---|---|---|---|---|
| PMV (n = 65) | Short MV (n = 85) | |||
| WBC (×109/L) | 10.8 (7.1–14.5) | 10.7 (6.6–13.2) | 15.0 (11.3–19.1) | 0.195 |
| Neutrophils (%) | 89.4 (84.1–92.9) | 87.5 (83.3–91.3) | 90.4 (84.8–93.7) | 0.040 |
| Lymphocytes (%) | 5.95 (2.98–9.73) | 7.00 (3.50–10.00) | 5.20 (2.70–8.50) | 0.122 |
| Hemoglobin (g/L) | 122.0 (108.8–139.0) | 122.0 (105.5–139.5) | 122.0 (111.0–138.0) | 0.962 |
| Platelets (×109/L) | 186.5 (149.0–239.8) | 181.0 (140.0–238.5) | 195.0 (153.5–246.0) | 0.247 |
| Urea (mmol/L) | 6.80 (4.95–11.60) | 6.65 (4.98–10.68) | 7.50 (4.98–12.0) | 0.446 |
| Creatinine (µmol/L) | 79.9 (60.6–104.5) | 77.0 (57.3–95.5) | 81.0 (61.4–110.1) | 0.554 |
| Glucose (mmol/L) | 9.80 (7.45–13.70) | 9.20 (6.35–11.80) | 10.30 (7.55–15.28) | 0.220 |
| Protein (g/L) | 62.27 (8.0) | 59.73 (6.03) | 64.22 (8.77) | 0.029 |
| Albumin (g/L) | 30.12 (5.68) | 29.71 (5.48) | 30.43 (5.84) | 0.481 |
| AST (UI/L) | 48.0 (34.1–78.7) | 46.0 (31.8–68.8) | 54.0 (34.5–81.1) | 0.120 |
| ALT (UI/L) | 34.3 (24.8–51.1) | 34.0 (20.8–51.4) | 34.3 (23.0–51.0) | 0.997 |
| CRP (mg/L) | 80.2 (44.0–127.6) | 64.9 (32.9–112.0) | 89.9 (55.7–141.7) | 0.011 |
| Sodium (mmol/L) | 137.0 (133.4–140.0) | 136.6 (134.8–140.0) | 137.0 (133.0–140.5) | 0.678 |
| Potassium (mmol/L) | 3.93 (3.60–4.30) | 3.90 (3.60–4.25) | 3.96 (3.60–4.37) | 0.817 |
| Chloride (mmol/L) | 101.4 (97.8–105.7) | 101.5 (98.4–105.5) | 101.3 (26.8–106.0) | 0.607 |
| Procalcitonin (ng/mL) | 0.32 (0.14–0.95) | 0.30 (0.14–0.87) | 0.48 (0.13–1.14) | 0.530 |
| D-Dimer (ng/L) | 1287.0 (728.0–3849.0) | 1307.0 (639.0–4633.3) | 1287.0 (766.0–3727.0) | 0.921 |
| PT (%) | 75.8 (16.0) | 79.2 (15.9) | 73.3 (15.7) | 0.026 |
| APTT (s) | 32.7 (29.3–37.4) | 32.9 (29.4–37.8) | 32.3 (29.0–36.5) | 0.614 |
| INR | 1.21 (1.11–1.32) | 1.15 (1.09–1.27) | 1.24 (1.12–1.33) | 0.029 |
| Fibrinogen (g/L) | 4.56 (1.15) | 4.42 (1.10) | 4.67 (1.18) | 0.223 |
| NLR | 15.16 (8.85–30.59) | 12.77 (8.47–26.46) | 17.14 (10.31–34.79) | 0.112 |
| LCR | 0.65 (0.36–1.63) | 0.98 (0.40–2.07) | 0.56 (0.34–1.08) | 0.008 |
| Parameter | Category (Description) | Univariate | Multivariate | ||
|---|---|---|---|---|---|
| OR (95%CI) | p-Value | aOR (95%CI) | p-Value | ||
| BMI | Obesity vs. non-obesity | 2.218 (1.148–4.285) | 0.018 | 1.478 (0.390–5.601) | 0.565 |
| COVID-19 Vaccination | Yes vs. no | 0.370 (0.164–0.833) | 0.014 | 0.155 (0.029–0.835) | 0.030 |
| Duration of corticosteroid treatment | 1 day Increment | 1.049 (1.011–1.088) | 0.011 | 1.056 (0.978–1.140) | 0.167 |
| Neutrophils (%) | 1% Increment | 0.961 (0.927–0.996) | 0.031 | 0.924 (0.826–1.035) | 0.171 |
| Protein (g/L) | 1 g/L Increment | 0.925 (0.859–0.995) | 0.037 | 0.900 (0.819–0.989) | 0.028 |
| CRP (mg/L) | 1 mg/l Increment | 0.994 (0.989–0.999) | 0.016 | 0.992 (0.981–1.003) | 0.154 |
| PT (%) | 1% Increment | 1.025 (1.003–1.048) | 0.029 | 0.944 (0.885–1.008) | 0.084 |
| Parameter | Category (Description) | Univariate | Multivariate | ||
|---|---|---|---|---|---|
| HR (95%CI) | p-Value | HR (95%CI) | p-Value | ||
| Age (years) | >60 vs. ≤60 | 2.161 (1.212–3.855) | 0.009 | 1.765 (0.775–4.023) | 0.176 |
| CKD | Yes vs. no | 2.287 (1.201–4.321) | 0.012 | 1.177 (0.214–6.469) | 0.851 |
| Hypertension | Yes vs. no | 2.048 (1.272–3.300) | 0.003 | 1.626 (0.801–3.299) | 0.179 |
| History of Stroke | Yes vs. no | 2.398 (1.250–4.600) | 0.008 | 1.318 (0.461–3.764) | 0.607 |
| COVID-19 Vaccination | Yes vs. no | 0.509 (0.315–0.822) | 0.006 | 0.475 (0.219–1.029) | 0.059 |
| WBC (×109/L) | 1 × 109/L Increment | 1.061 (1.021–1.103) | 0.003 | 1.011 (0.944–1.083) | 0.756 |
| Urea (mmol/L) | 1 mmol/L Increment | 1.042 (1.022–1.063) | <0.001 | 1.032 (0.979–1.087) | 0.239 |
| Glucose (mmol/L) | 1 mmol/L Increment | 1.003 (1.007–1.061) | 0.014 | 1.047 (1.003–1.093) | 0.036 |
| CRP (mg/L) | 1 mg/L Increment | 1.005 (1.002–1.007) | <0.001 | 1.002 (0.998–1.006) | 0.335 |
| INR | 1 unit Increment | 1.955 (1.235–3.096) | 0.004 | 1.623 (0.527–4.997) | 0.399 |
| NLR | 1 unit Increment | 1.015 (1.006–1.023) | 0.001 | 1.024 (1.009–1.039) | 0.002 |
| Tracheostomy | Yes vs. no | 0.337 (0.213–0.534) | <0.001 | 0.273 (0.127–0.589) | 0.001 |
| CRRT | Yes vs. no | 0.336 (0.212–0.533) | <0.001 | 0.789 (0.385–1.617) | 0.518 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Than, H.M.; Dao, T.V.; Cao, T.V.; Duong, T.V.; Pham, T.N.; Nguyen, C.T.; Vu, P.D.; Le, N.V.; Do, B.N.; Nguyen, P.V.; et al. Factors Associated with Prolonged Mechanical Ventilation and 30-Day Mortality in Intubated COVID-19 Patients with Invasive Fungal Infections: A Retrospective Observational Study. Trop. Med. Infect. Dis. 2025, 10, 124. https://doi.org/10.3390/tropicalmed10050124
Than HM, Dao TV, Cao TV, Duong TV, Pham TN, Nguyen CT, Vu PD, Le NV, Do BN, Nguyen PV, et al. Factors Associated with Prolonged Mechanical Ventilation and 30-Day Mortality in Intubated COVID-19 Patients with Invasive Fungal Infections: A Retrospective Observational Study. Tropical Medicine and Infectious Disease. 2025; 10(5):124. https://doi.org/10.3390/tropicalmed10050124
Chicago/Turabian StyleThan, Hung Manh, Thang Van Dao, Truong Van Cao, Tuyen Van Duong, Thach Ngoc Pham, Cap Trung Nguyen, Phu Dinh Vu, Nam Van Le, Binh Nhu Do, Phuong Viet Nguyen, and et al. 2025. "Factors Associated with Prolonged Mechanical Ventilation and 30-Day Mortality in Intubated COVID-19 Patients with Invasive Fungal Infections: A Retrospective Observational Study" Tropical Medicine and Infectious Disease 10, no. 5: 124. https://doi.org/10.3390/tropicalmed10050124
APA StyleThan, H. M., Dao, T. V., Cao, T. V., Duong, T. V., Pham, T. N., Nguyen, C. T., Vu, P. D., Le, N. V., Do, B. N., Nguyen, P. V., Vu, H. N., & Vu, D. M. (2025). Factors Associated with Prolonged Mechanical Ventilation and 30-Day Mortality in Intubated COVID-19 Patients with Invasive Fungal Infections: A Retrospective Observational Study. Tropical Medicine and Infectious Disease, 10(5), 124. https://doi.org/10.3390/tropicalmed10050124