

Kids Save Lives by Learning through a Serious Game

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Design and Development of the Videogame
2.3. Assessment of the CPR Competencies
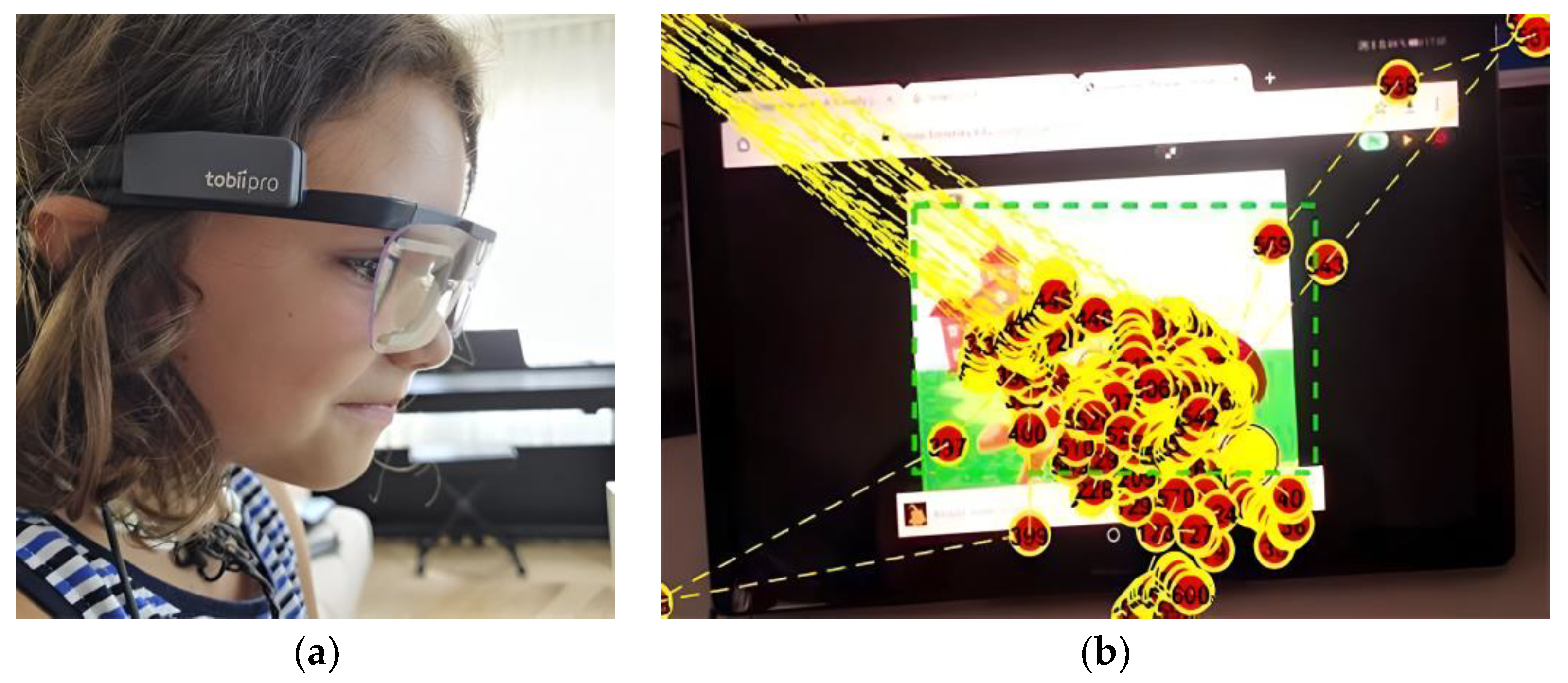
2.4. Eye Tracking System
2.5. Intervention
- A preliminary assessment (Pre) on the knowledge about the action protocol for performing CPR. For this, a scene was recreated in the classroom, composed of a CPR manikin in the supine position and a telephone close to the victim (manikin). The recreated scenario consists of the child being at the home of a family member, and the family member being unconscious on the floor. From this point on, the child is asked to act.
- The educational intervention took place after the preliminary assessment. Each child was invited to play the game, going through each of the 4 levels of its structure with assistance. The platform utilized was a computer with a mouse. A supervisor, in the role of assistant, ensured that each phase was satisfactorily completed, until arriving to the end of the game.
- A posterior assessment (Post); this session took place a month after the first session, and consisted of repeating the assessment on the protocol and CPR (Post), and using the same scenario and the same rubric for its assessment.
2.6. Statistical Analysis
3. Results
3.1. Participant Characteristics
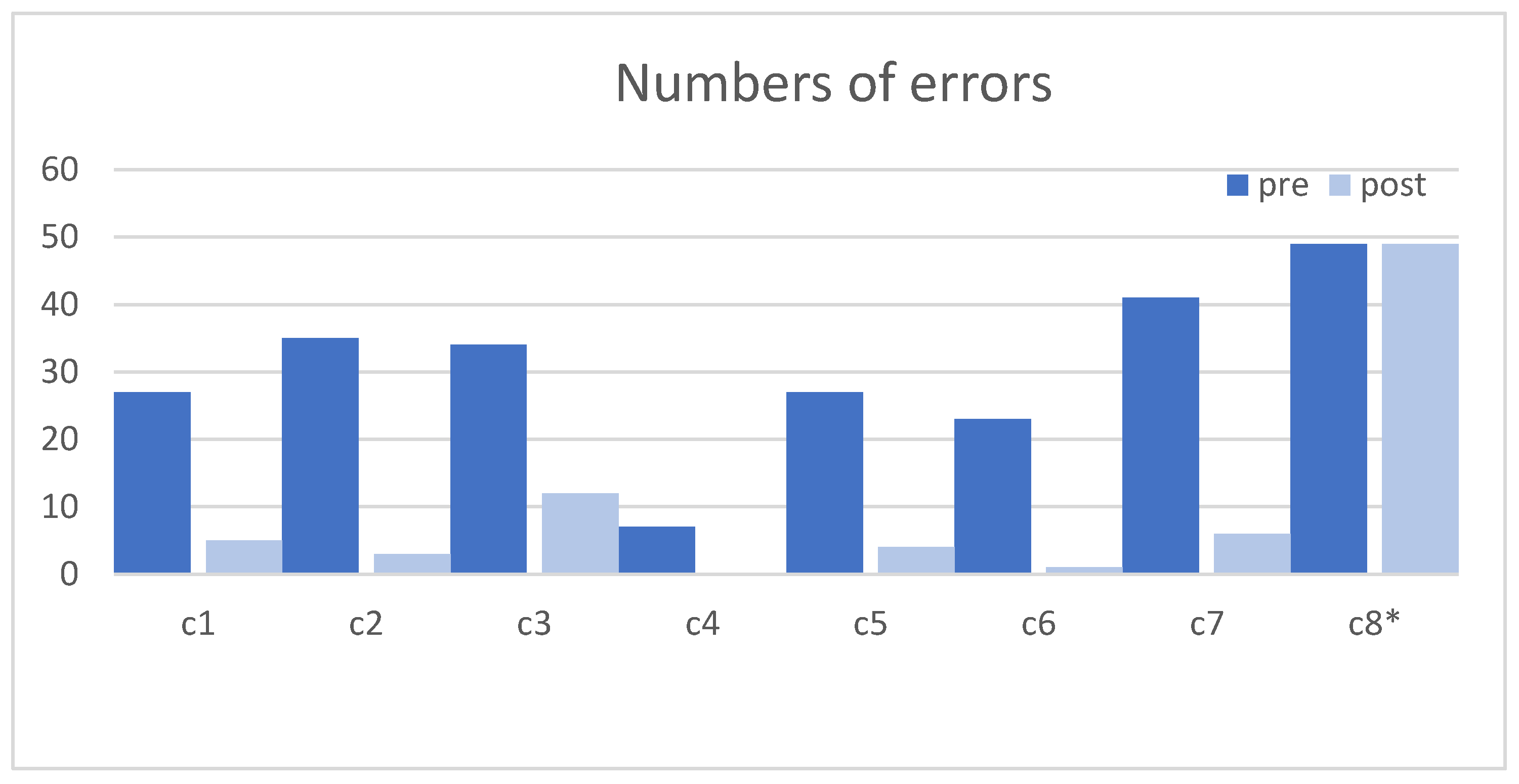
3.2. Knowledge on CPR (Questions 1–8)
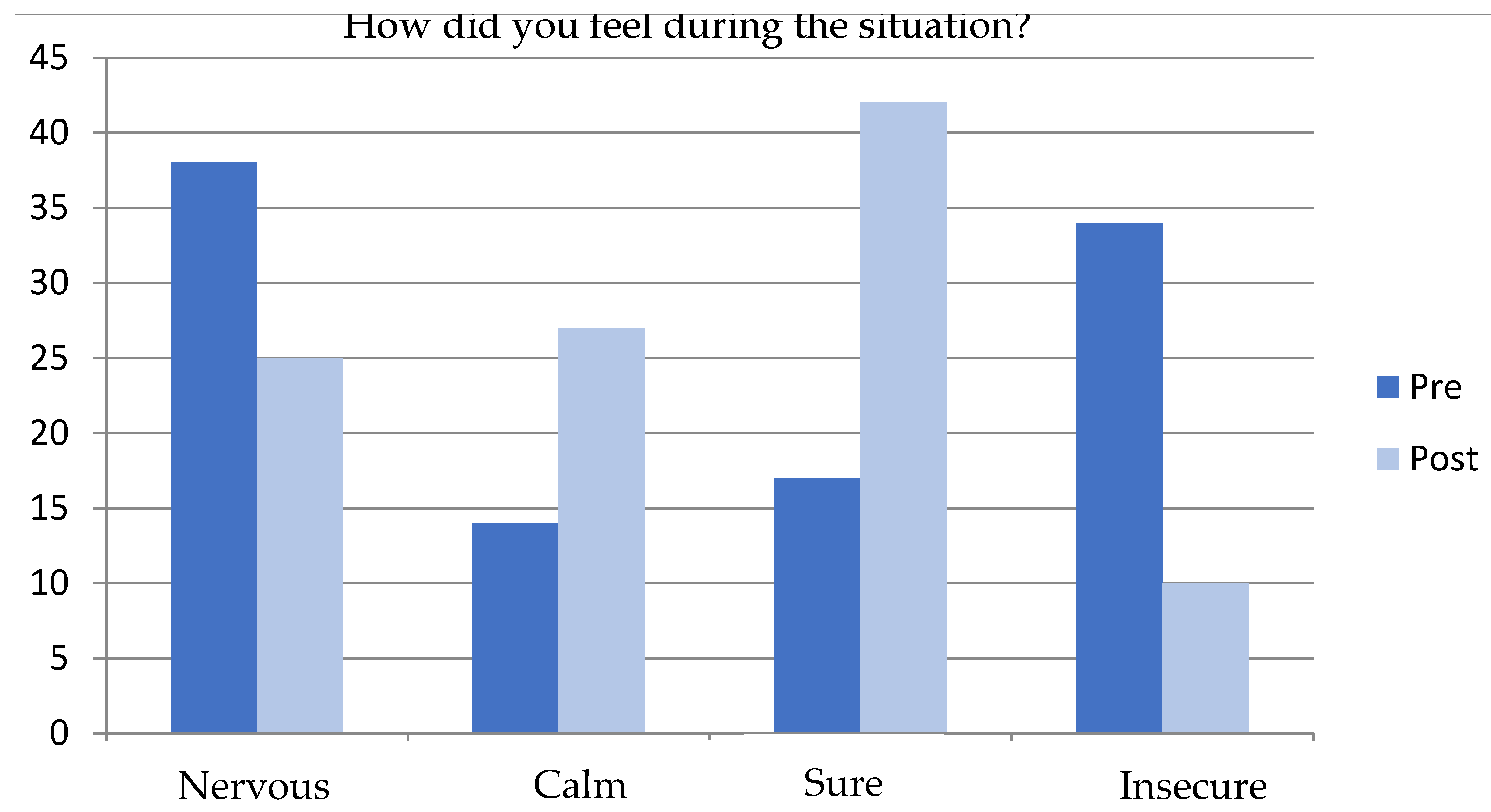
3.3. Emotional Responses (Questions 9–10)
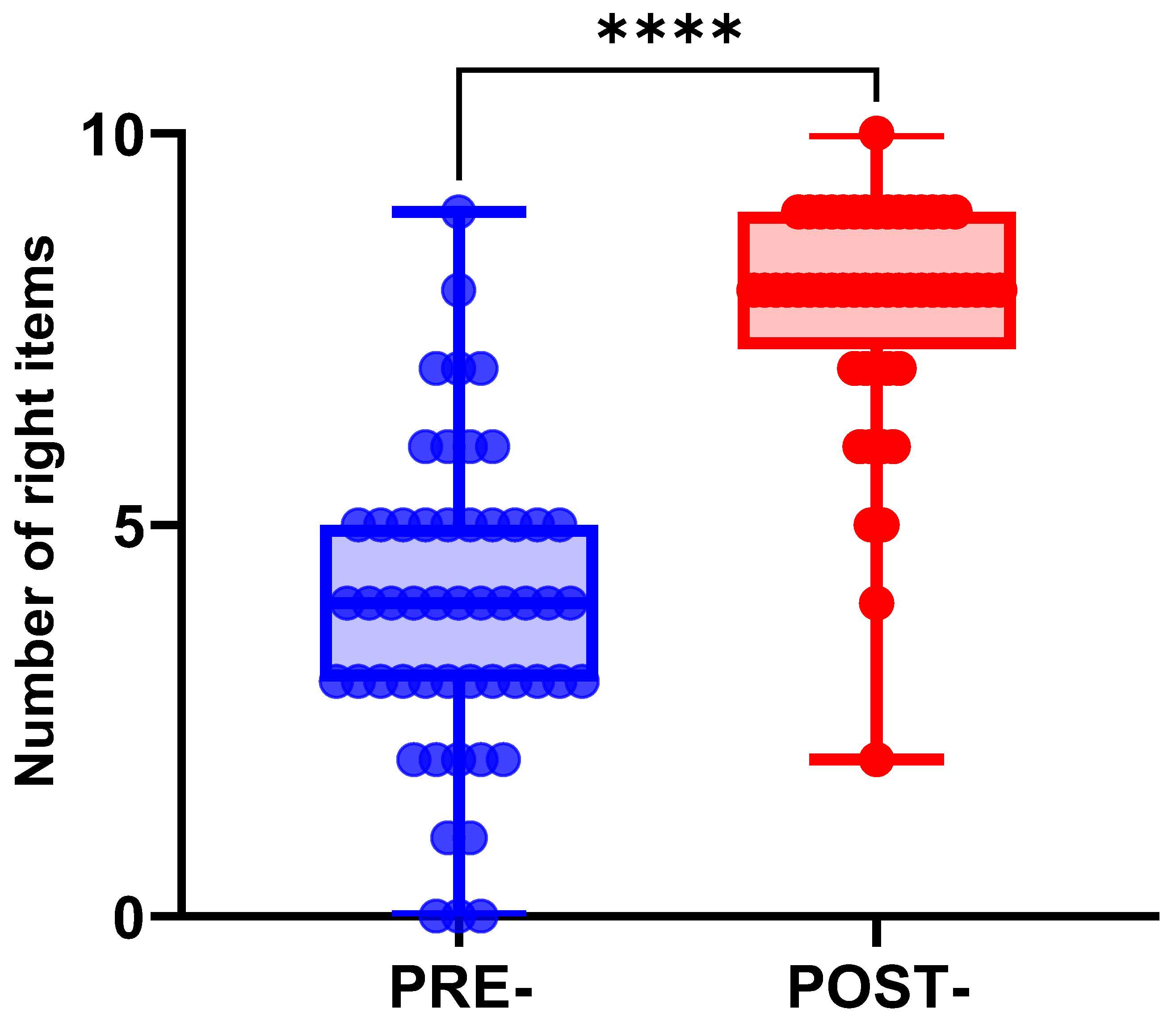
3.4. Overall CRP Knowledge
3.5. Videogame Exam
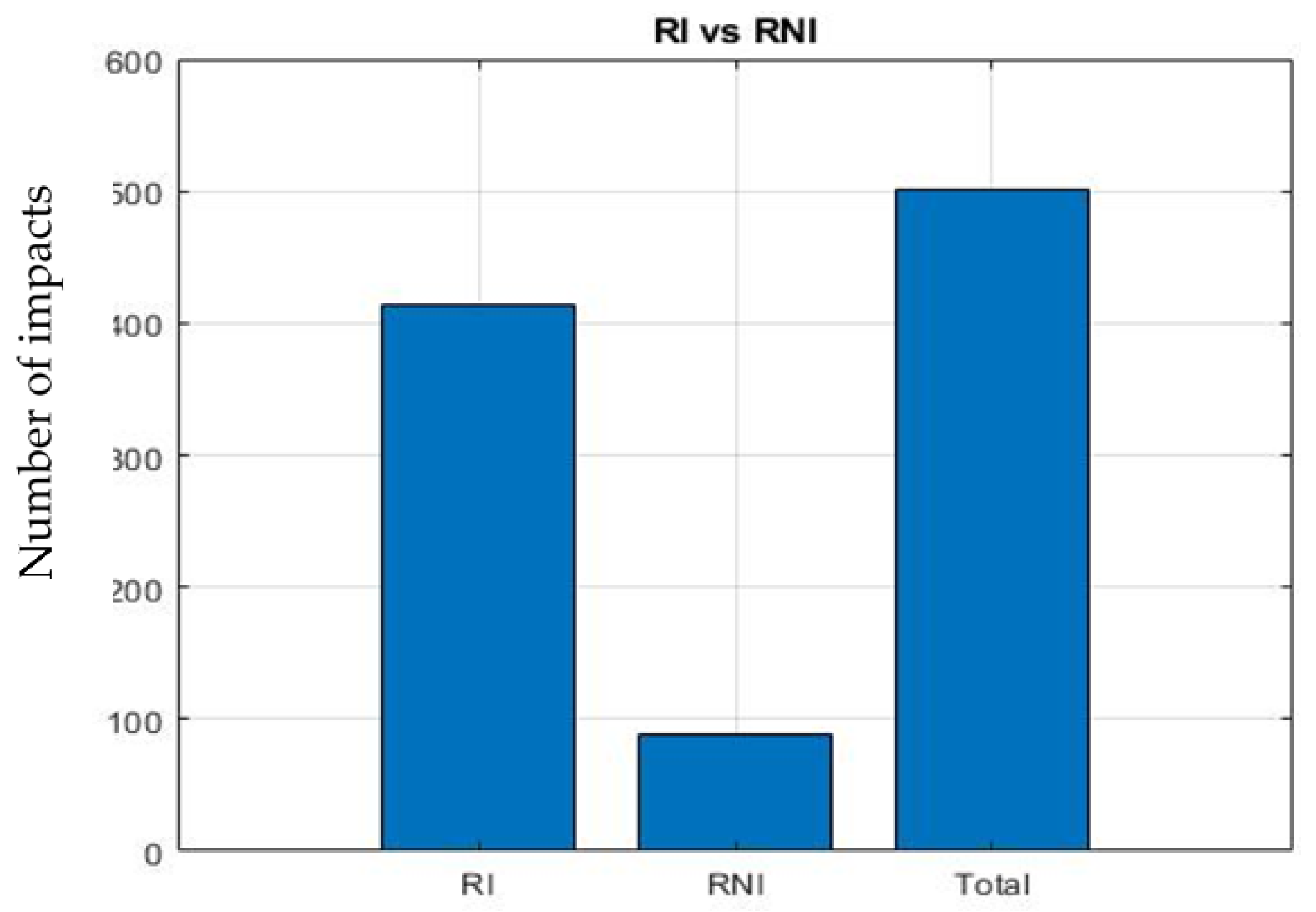
3.6. Eye Tracking Analysis
4. Discussion
5. Limitations, Future Work and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Level | Scenario | Objectives | Learning Results | Score |
|---|---|---|---|---|
| 1 | Forest with interactive characters | Familiarize the player with the device and the characters | Knowledge of the environment | +10 If the character is found |
| 2 | Pantry with healthy and non-healthy foods | Feed the bear | Become responsible. Distinguish healthy food | +2 Healthy foods +1 Less healthy foods Maximum of 4 foods |
| 3 | Phase 1: Video Phase 2: Game | Learn about first aid | Instructions on the technique in the following order:
| Total of 25 points: 8 questions Correct answer add +2 and +5 Incorrect substract −1 |
| 4 | The bear suffers a cardiac arrest | Know the CPR technique | Correctly execute the position and rhythm of compressions | Total of 36 points Correct placement +1 |
| Call from a mobile phone without the need to unlock it |
References
- Koster, R.W.; Baubin, M.A.; Bossaert, L.L.; Caballero, A.; Cassan, P.; Castrén, M. European Resuscitation Council Guidelines for Resuscitation 2010 Section 2. Adult basic life support and use of automated external defibrillators. Resuscitation 2010, 81, 1277–1292. [Google Scholar] [CrossRef] [PubMed]
- Escalada, X.; Fabrega, X.; Diaz, N.; Sanclemente, G.; Gómez, X.; Villena, O. Programa de Reanimación Cardiopulmonar Orientado a Centros de Enseñanza Secundaria (PROCES): Conclusiones tras 5 años de experiencia. Emerg. Rev. Soc. Española Med. Urgenc. Emerg. 2008, 20, 229–236. [Google Scholar]
- Sesma, J.; Miró, Ò. Urgencias y emergencias: Al servicio del ciudadano. An. Sist. Sanit. Navar. 2010, 33, 5–6. [Google Scholar] [CrossRef]
- SAMUR—Protección Civil—Formación a la ciudadanía: Alertante y Primer Respondiente—Ayuntamiento de Madrid [Internet]. Available online: https://www.madrid.es/portales/munimadrid/es/Samur/SAMUR-Proteccion-Civil/?vgnextfmt=default&vgnextoid=c88fcdb1bfffa010VgnVCM100000d90ca8c0RCRD&vgnextchannel=84516c77e7d2f010VgnVCM1000000b205a0aRCRD&idCapitulo=10276015 (accessed on 7 September 2023).
- Miró, Ò.; Díaz, N.; Escalada, X.; Pérez Pueyo, F.J.; Sánchez, M. Revisión de las iniciativas llevadas a cabo en España para implementar la enseñanza de la reanimación cardiopulmonar básica en las escuelas. An. Sist. Sanit. Navar. 2012, 35, 477–486. [Google Scholar] [CrossRef]
- SEMES XCN. En 2022. Available online: https://www.semes.org/vigo-batira-el-record-en-formacion-de-ninos-en-rcp-en-el-congreso-nacional-de-medicina-de-urgencias-y-emergencias/ (accessed on 10 October 2023).
- Greif, C.; Lockey, A.; Conaghan, P.; Lippert, A.; Vries, W.; Monsieurs, K. European Resuscitation Council Guidelines for Resuscitation 2015: Section 10. Education and implementation of resuscitation. Resuscitation 2015, 95, 288–301. [Google Scholar] [CrossRef] [PubMed]
- Greif, R.; Lockey, A.; Breckwoldt, J.; Carmona, F.; Conaghan, P.; Kuzovlev, A.; Pflanzl-Knizacek, L.; Sari, F.; Shammet, S.; Scapigliati, A.; et al. European Resuscitation Council Guidelines 2021: Education for resuscitation. Resuscitation 2021, 161, 388–407. [Google Scholar] [CrossRef] [PubMed]
- Semeraro, F.; Monesi, A.; Gordini, G.; Del Giudice, D.; Imbriaco, G. Kids Save Lives: A blended learning approach to improve engagement of schoolchildren. Resuscitation 2023, 182, 109675. [Google Scholar] [CrossRef] [PubMed]
- Iglesias, A.; Martín, Y.; Hernández, A. Evaluación de la competencia digital del alumnado de Educación Primaria. Rev. De Investig. Educ. 2023, 41, 33–50. [Google Scholar] [CrossRef]
- Tomala-Gonzales, J.; Guaman-Quinche, J.; Guaman-Quinche, E.; Chamba-Zaragocin, W.; Mendoza-Betancourt, S. Serious Games: Review of methodologies and Games engines for their development. In Proceedings of the 15th Iberian Conference on Information Systems and Technologies (CISTI), Sevilla, Spain, 4–27 June 2020; pp. 1–6. [Google Scholar]
- Nacke, L.E.; Drachen, A.; Goebel, S. Methods for Evaluating Gameplay Experience in a Serious Gaming Context. IACSS [Internet]. 2010, Volume 9. Available online: https://research.cbs.dk/en/publications/methods-for-evaluating-gameplay-experience-in-a-serious-gaming-co (accessed on 10 October 2023).
- Botto-Tobar, M.; Zambrano Vizuete, M.; Montes León, S.; Torres-Carrión, P.; Durakovic, B. Applied Technologies. In Proceedings of the 4th International Conference, ICAT 2022, Quito, Ecuador, 23–25 November 2022; Revised Selected Papers, Part I [Internet]; Springer Nature: Cham, Switzerland, 2023. (Communications in Computer and Information Science; Vol. 1755). Available online: https://link.springer.com/10.1007/978-3-031-24985-3 (accessed on 10 October 2023).
- Noboa Carrasco, G.N. Diseño de un Serious Game Para Concientizar a Niños de Educación Básica Sobre el Bullying [Internet] [Bachelorthesis]. Riobamba. 2021. Available online: http://dspace.unach.edu.ec/handle/51000/7790 (accessed on 10 October 2023).
- Rodríguez Carranza, Y.V. Diseño de Serious Game para la enseñanza de la Responsabilidad Social en la Educación Superior. Docencia Univ. 2018, 156–175. [Google Scholar] [CrossRef]
- CarrerasPlanas, C. Del Homo Ludens a lagamificación. Quaderns de Filosofia [Internet]. 21 de mayo de 2017. Volume 4. Available online: https://ojs.uv.es/index.php/qfilosofia/article/view/9461 (accessed on 10 October 2023).
- Newley, A.; Deniz, H.; Kaya, E.; Yesilyurt, E. Engaging Elementary and Middle School Students in Robotics through Hummingbird Kit with Snap! Visual Programming Language. Joltida 2016, 2016, 20–26. [Google Scholar]
- Marchiori, E.; Ferrer, G.; Fernández Manjón, B.; Povar Marco, J.; Suberviola González, J.F.; Giménez Valverde, A. Instrucción en maniobras de soporte vital básico mediante videojuegos a escolares: Comparación de resultados frente a un grupo control. Emerg. Rev. Soc. Española Med. Urgenc. Y Emerg. 2012, 24, 433–437. [Google Scholar]
- Espinosa, C.C.; Caballero, S.N.; Rodríguez, L.J.; Castejón-Mochón, J.F.; Melgarejo, F.S.; Martínez, C.M.S.; López, C.A.L.; Ríos, M.P. Estudio Aleatorizado de Formación en Reanimación Cardiopulmonar en 2.225 Alumnos: ¿Se Pueden Sustituir las Clases por Videos? EMERGENCIAS [Internet]. 22 de Diciembre de 2017; Volume 30. Available online: https://emergenciasojs.portalsemes.org/index.php/emergencias/article/view/524 (accessed on 10 October 2023).
- Marín Díaz, V.; García Fernández, M.D. Los Videojuegos su Capacidad Didáctico-Formativa. Video Games and Their Didactic-Formative Capacity [Internet]. 2005. Available online: https://idus.us.es/handle/11441/45606 (accessed on 10 October 2023).
- Pérez Rubio, M.T.; González Ortiz, J.J.; López Guardiola, P.; Alcázar Artero, P.M.; Soto Castellón, M.B.; Ocampo Cervantes, A.B.; Ríos, M.P. Realidad Virtual para Enseñar Reanimación Cardiopulmonar en el Grado de Educación Primaria: Estudio comparativo. RIED Revista Iberoamericana de Educación a Distancia [Internet]. 2023. Available online: https://redined.educacion.gob.es/xmlui/handle/11162/252752 (accessed on 10 October 2023).
- Creutzfeldt, J.; Hedman, L.; Heinrichs, L.; Youngblood, P.; Felländer-Tsai, L. Cardiopulmonary resuscitation training in high school using avatars in virtual worlds: An international feasibility study. J. Med. Internet Res. 2013, 15, e9. [Google Scholar] [CrossRef] [PubMed]
- Mendoza López, M.; Pérez Rubio, M.T.; Truque Díaz, C.; Pardo Ruiz, M. Enfermera Comunitaria Escolar e Innovación Docente para Enseñar Reanimación Cardiopulmonar en la Escuela a Través de una Flipped Classroom. Aten Primaria [Internet]. 1 de Junio de 2023. Volume 55. Available online: https://www.elsevier.es/es-revista-atencion-primaria-27-articulo-enfermera-comunitaria-escolar-e-innovacion-S0212656723000872 (accessed on 10 October 2023).
- López Raventós, C. El videojuego como herramienta educativa. Posibilidades y problemáticas acerca de los serious games. Apert. Rev. Innovación Educ. 2016, 8, 136–151. [Google Scholar]
- Semeraro, F.; Greif, R.; Böttiger, B.W.; Burkart, R.; Cimpoesu, D.; Georgiou, M.; Yeung, J.; Lippert, F.; Lockey, A.S.; Olasveengen, T.M.; et al. European Resuscitation Council Guidelines 2021: Systems saving lives. Resuscitation 2021, 161, 80–97. [Google Scholar] [CrossRef] [PubMed]
- Semeraro, F.; Frisoli, A.; Ristagno, G.; Loconsole, C.; Marchetti, L.; Scapigliati, A.; Pellis, T.; Grieco, N.; Cerchiari, E.L. Relive: A serious game to learn how to save lives. Resuscitation 2014, 85, e109–e110. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, D.C.; Semeraro, F.; Greif, R.; Bray, J.; Morley, P.; Parr, M.; Nakagawa, N.K.; Iwami, T.; Finke, S.-R.; Hansen, C.M.; et al. KIDS SAVE LIVES: Basic Life Support Education for Schoolchildren: A Narrative Review and Scientific Statement From the International Liaison Committee on Resuscitation. Resuscitation 2023, 188, 109772. [Google Scholar] [CrossRef] [PubMed]
| Question | Number of Participants with Correct Answer | Χ2 | p (Sig.) | |
|---|---|---|---|---|
| Pre-Test | Post-Test | |||
| I1. Talk or call the victim loudly | 1 | 23 | 1.747 | <0.0001 |
| I2. Move the shoulders of the victim vigorously | 0 | 32 | 1.546 | <0.0001 |
| I3. Verifies that the victim is not breathing | 2 | 24 | 2.220 | <0.001 |
| I4. Asks for the phone | 45 | 45 | - | >1.000 |
| I5. Does he or she know the number to call? | 0 | 23 | 4.012 | <0.0001 |
| I6. Start CPR maneuvers | 0 | 22 | 1.286 | <0.0001 |
| I7. Places the arms and hands correctly | 0 | 35 | 1.820 | <0.0001 |
| I8. Asks for an AED | 0 | 2 | 51.000 | 1.000 |
| I9. How did you feel during the situation? (Right answer: calm) | 3 | 11 | 5.450 | 0.004 |
| I10. How did you feel during the situation? (Right answer: secure) | 17 | 25 | 3.315 | <0.0001 |
| Test Score | Mean Game Playing Time (s) | % Students |
|---|---|---|
| 2 (minimum) | 417.5 | 3.8 |
| 4 | 375.24 | 32.7 |
| 6 (maximum) | 350.5 | 63.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mendoza López, M.; Alcaraz Artero, P.M.; Truque Díaz, C.; Pardo Ríos, M.; Hernández Morante, J.J.; Melendreras Ruiz, R. Kids Save Lives by Learning through a Serious Game. Multimodal Technol. Interact. 2023, 7, 112. https://doi.org/10.3390/mti7120112
Mendoza López M, Alcaraz Artero PM, Truque Díaz C, Pardo Ríos M, Hernández Morante JJ, Melendreras Ruiz R. Kids Save Lives by Learning through a Serious Game. Multimodal Technologies and Interaction. 2023; 7(12):112. https://doi.org/10.3390/mti7120112
Chicago/Turabian StyleMendoza López, Miriam, Petronila Mireia Alcaraz Artero, Carlos Truque Díaz, Manuel Pardo Ríos, Juan José Hernández Morante, and Rafael Melendreras Ruiz. 2023. "Kids Save Lives by Learning through a Serious Game" Multimodal Technologies and Interaction 7, no. 12: 112. https://doi.org/10.3390/mti7120112
APA StyleMendoza López, M., Alcaraz Artero, P. M., Truque Díaz, C., Pardo Ríos, M., Hernández Morante, J. J., & Melendreras Ruiz, R. (2023). Kids Save Lives by Learning through a Serious Game. Multimodal Technologies and Interaction, 7(12), 112. https://doi.org/10.3390/mti7120112