Abstract
The main objectives of this research are, firstly, to determine the state of Autism Spectrum Disorder (ASD) caregivers in objective and subjective burden, psychological distress, and resilience, and, secondly, to assess the role of resilience as a mediator variable that could buffer the effect of objective burden on perceived burden and psychological distress. The method is descriptive, cross-sectional with a sample of 250 family caregivers. Results show that levels of burden were high, with half of the sample presenting psychological distress, and that the resilience level was above that of the general population. Additionally, the relational pattern showed significant positive relationships between burden and psychological distress, but negative relationships between these variables and resilience. Finally, as expected, resilience has worked as a buffer, decreasing the effect of objective burden, measured as hours/day caring, on subjective burden and psychological distress. The direct impact of resilience on burden and psychological distress, two of the more important risk factors for the mental health of ASD caregivers, as highlighted in this study, points to the necessity of implementing intervention or training programs that help caregivers to cope with stressors associated with the daily tasks of caring, to enhance resilience and personal growth out of stressful situations.
1. Introduction
Autism Spectrum Disorder (ASD) is a neurodevelopmental disorder that is characterized by deficits in social communication and social interactions, such as difficulties in social-emotional reciprocity, difficulties in nonverbal communication, or deficits in developing and maintaining relationships with other people, with restricted and repetitive behavior, interests, or activities, often added to the above [1]. Reviews performed in ASD have shown that the prevalence level is 1/1000 [2,3,4] although there are areas in Eastern Europe, Central/South America, and Africa not represented in these reviews. ASD has shown higher prevalence in boys than girls, with a male/female ratio of 3:1 [5], although in the case of clinical or school-based population, the ratio increased to 5:1 [6]. ASD people present differences in their abilities/disabilities, differing along a continuum of severity [7]. Some of them show superior levels of intellectual functioning, while others display profound impairment. Accordingly, some live independently without any support, but others, with serious difficulties, need lifelong care. Consequently, an important proportion of ASD people need family members, mainly parents, to provide care and support in basic daily life activities. Moreover, some ASD people present comorbidity with other conditions. The presence of a single comorbidity in ASD people has a prevalence twice that of people without a diagnosis of ASD. Learning and intellectual disabilities appear in one out of every five cases, with attention deficit hyperactivity disorder (ADHD) being the most prevalent [8]. The addition of comorbidities to the specific features of ASD places their caregivers in a position of high levels of stress, negative affect, depression and anxiety symptoms, and mild to severe levels of burden, which could seriously affect their mental health [8,9,10,11].
The maintenance of good mental health in caregivers is a priority due to the dependence of the care recipient and the consequent positive effect on him/her. That is why it is common in research to separate positive or protective factors from negative or risk factors in the mental health of caregivers of dependent people [12,13]. In the risk factor category, burden, sleep problems, anxiety, or depression are usually included [14], whilst variables related to positive psychology such as happiness, optimism, quality of life, social support, gain in caregiving tasks, or resilience are included as protective factors [12,15,16]. Studies showing mental health problems in caregivers of ASD people vary from those showing hassles in the daily tasks [17], stress [18,19], anxiety [20,21], to depression [17,18]. On the other hand, factors related to good mental health include, among others, low burden, in the form of objective burden, measured as a low number of hours per day caring for an ASD relative [21], subjective burden, measured as low perceived burden [22,23,24], low stress [19,25], high household income [26,27,28], and lack of co-occurring difficulties in the relative [26,29].
Two studies that have compared the burden in ASD caregivers with other types of caregivers have shown that it is higher than that presented by caregivers of children with schizophrenia [22] and higher than that displayed by caregivers of children without ASD [30]. Additionally, the study performed by Al-Qahtani in ASD caregivers [31] measuring perceived burden with the Zarit Burden Interview [32] and taking into account the burden levels proposed by Mulud and McCarthy [33], found that 86.6% of the caregivers presented different levels of burden: 49% were classified at the mild level, 35% at the moderate level, and 2.5% at the severe level, with the average score being 41, a score classified as the moderate level. The relationship between burden and psychological distress is so close in ASD caregivers that the best predictors of burden have been depressive symptoms [22,23,24,34] and anxiety [17].
On the other hand, resilience has been studied as a protective factor in the mental health of caregivers [13,16]. One of the most challenging objectives in the study of resilience is its definition. Originating in the field of physics-engineering in the 19th century as the capacity of a material to recover its original shape after being perturbed by deforming pressure [35], it was adapted to psychology by Bowlby in 1951 [36]. In the early studies of resilience in psychology, resilience was defined as a personality trait, assuming that individuals differ in the adaptation process to adverse and stressful events across domains and time [37]. Walsh [38] broadened resilience from the individual to the family, community, or culture, where concepts such as family resilience, community resilience, or culture resilience were used to analyze resilience in systems from a small to a bigger approach. This broad tendency was also followed by Southwick et al. in 2014 [39], proposing biological, psychological, social, or cultural factors affecting resilience, adding the study of resilience as a personality trait, as a process of dynamic adaptation, and as an outcome of this adaptation process, with resilience being studied from different fields: from the origin of physics-engineering to medicine, economics, or mental health.
More recent definitions centered on three main categories: resilience as an ability to resist, to bounce back, or to grow from stressors, adversity, or traumatic events [40]. In the first category, resilience is defined as an ability to resist change and maintain mental health after stressor or traumatic experiences; in other words, the absence of psychopathology after stressful events [41]. A second approach proposed resilience as a comeback to previous functioning after stressful circumstances; in Hill’s literal words, “the dynamic process by which a biopsychosocial system returns to the previous level of functioning, following a perturbation caused by a stressor” [42] (p. 367). Finally, the third category presented resilience as an ability for adaptation and growth in response to a stressor. Connor and Davidson defined resilience as “the personal qualities that enable one to thrive in the face of adversity” [43] (p. 76). Growth is understood as phenotypic plasticity, where success in a history of stressors or adverse situations enables more resilient people to develop more adequate responses to stressful events compared to individuals who encountered little or no adversity in their lives [44]. This last approach to resilience surpasses the definition of resilience in the second category because growth goes beyond previous functioning [45]. Each of the categories represents a step forward from one to the next, with the third being the most complete and encompassing the previous ones. Then, resilience could be defined as a group of psychological characteristics that make it possible to resist, cope with, bounce back from, and succeed in stressful or traumatic events [40]. One of the proposed measures to assess this conceptualization of resilience is the CD-RISK, the scale used in this research [43].
Resilience as a protective factor for the mental health of ASD caregivers has been studied as a buffer against stress [46,47], as performing a mediating role in positive emotions that affects burden [48] and as being negatively associated with symptoms of depression and anxiety [49,50]. However, there are no published studies to date that analyze the buffer effect of resilience between objective burden and subjective burden, ultimately affecting psychological distress in ASD caregivers. Therefore, the main objectives of this research are, firstly, to determine the state of ASD caregivers caring for dependent ones, in objective and subjective burden, resilience, and psychological distress, and, secondly, to assess the role of resilience as a mediating variable that could buffer the effect of objective burden on perceived burden and psychological distress. The hypotheses proposed are as follows:
- ASD caregivers will present high levels of burden—objective, measured as hours per day of care, and subjective, measured as perceived burden—psychological distress, and low levels of resilience.
- Caregivers with high levels of psychological distress will present a higher burden, both objective and subjective, and lower resilience than caregivers with low levels of psychological distress.
- The expected relationship pattern will show significant and positive relationships between psychological distress and objective and subjective burden, and significant but negative relationships between these three variables and resilience.
- A serial mediation of resilience and subjective burden will be full between objective burden and psychological distress.
2. Materials and Methods
2.1. Participants
The sample was composed of 250 family caregivers of people diagnosed with ASD in Spain. The participants made up a convenience sample of volunteers from ASD centers in the whole country. 196 (78.4%) were female caregivers and 54 (21.6%) male caregivers with a mean age of 42.59 years ± 6.75, and an age range of 29–65 years. The mean age and age range of the care recipients were 8.46 years ± 5.28 and 1–31 years respectively.
The inclusion criteria were (1) a diagnosis of ASD in the care recipient; (2) a relative with ASD living in the community; (3) age of the caregiver equal or higher than 18 years; (4) no reading or understanding problem when completing the information requested. The exclusion criteria were (1) caregiver under 18 years old, (2) caregiver caring for a relative diagnosed with any disorders different from ASD, (3) caregiver caring for an institutionalized relative with ASD, and (4) caregiver with incomplete information requested or answers not completed in the questionnaires. The ASD diagnosis was performed in all cases by the ASD center’s neuropsychologist.
2.2. Design and Procedure
The study employed a descriptive cross-sectional design. All participants signed the informed consent, and the assessment was performed individually. Each participant was assigned a number in order to preserve his/her anonymity. No reward was provided for participation in the study. The data collection was conducted in person when the residence of the participants and the authors coincided, or by email when the residence did not coincide. This research has the approvals of the Ethical Committee for Scientific Research in the University of Valencia (H1367489852167) and the corresponding ASD centers.
2.3. Measures
2.3.1. Psychological Distress
The 12-item General Health Questionnaire, GHQ-12 [51], in its Spanish adaptation [52], was used to evaluate psychological stress. The items were scored using a response scale of four levels (0–1–2–3). The highest score indicates the greatest level of distress. The GHQ Inx score of ≥14, proposed by Lunding et al. [53] as the best threshold (sensibility = 85.5% and specificity = 83.2%), was applied to discriminate the percentage of people with and without psychological distress. The internal consistency obtained by Cronbach’s Alpha was 0.87 in this study.
2.3.2. Subjective Burden
The perceived burden associated with the provision of care was assessed with the 22-item Zarit Burden Interview, ZBI [32], in its Spanish adaptation [54]. The items were rated with a five-level scale ranging from zero (never) to four (nearly always). The highest score indicates the greatest level of perceived burden. Following Mulud and McCarthy [33], the cut-off scores applied were no burden (≤20), mild burden (21–40), moderate burden (41–60), and severe burden (≥61). The internal consistency obtained by Cronbach’s Alpha was 0.90 in this study.
2.3.3. Resilience
The Connor–Davidson Resilience Scale (CD-RISC) [43] was used to measure resilience as the ability to thrive in the face of adversity. The 25 items were responded in the 5-point response scale ranging from 0 to 4, with higher scores indicating greater resilience. A cut-off score of ≤63 separated high from low resilience levels, based on two criteria: (1) 63.84 is the mean score obtained with the CD-RISC-25items in Spanish caregivers [55], and (2) the score of 63 is an extrapolation of the cut-off score of 29 from the CD-RISC-10items to the CD-RISC-25items used in the Okuyama et al. study [56]. The internal consistency obtained by Cronbach’s Alpha was 0.85 in this study.
2.3.4. Sociodemographic Variables and Objective Burden
The sociodemographic variables measured for the caregiver included age, marital status (single/separated/widow and married/cohabiting), educational level (primary, secondary, and university studies), and relation with the care recipient (parents and others). The care recipient’s age and hours per day of caring were also recorded, with the latter serving as a measure of objective burden.
2.4. Statistical Analysis
Firstly, the sociodemographic variables of the number and percentages of men and women, educational levels, marital status, and relation with the care recipient were obtained. Additionally, means, standard deviations, number and percentages of participants in variables objective and subjective burden, psychological distress, and resilience were included, considering the cut-offs described in the corresponding measure. Secondly, taking psychological distress as a categorical variable, comparisons were performed between those caregivers with high and low levels of psychological distress in the variables of caregiver age, care recipient age, hours/day caring, subjective burden, and resilience. Thirdly, Pearson correlations were performed in the cited variables, except for hours/day caring, where Spearman correlation was performed due to its categorical status. Finally, based on the relationships shown, a serial mediational analysis was performed to discover the possible mediational role of resilience and subjective burden (perceived burden) between objective burden (hours/day caring) and psychological distress. The mediation performed is based on (a) ordinary least squares regression and (b) the bootstrap method. The significance of an indirect mediating effect upon the bootstrap method is based on whether the mediating variable’s point estimate is zero in the 95% bias-corrected and accelerated confidence interval (BCaCI); therefore, a variable will be considered significant when no point estimate is within the zero interval. The bootstrapping method repeatedly samples randomly with replacement from the original sample. An advantage of this method is that it does not require distributional assumptions in the sample. Model 6 [57] with 10,000 bootstrap samples was performed to obtain the indirect effects with 95% bias-corrected bootstrap confidence interval. Furthermore, a contrast test of specific indirect effects was calculated to find the more powerful one. The multiple serial mediational analysis was performed with objective burden (hours per day caring) as the independent variable, psychological distress as the dependent variable, and resilience and perceived burden as serial mediators. The statistical software used to perform the analyses was SPSS version 28 and the PROCESS macro for SPSS.
3. Results
Descriptive data from sociodemographic variables are presented in Table 1. Most of the caregivers were women (78%), with university studies (50%), married or living with a partner (87.6%), and parents of the care recipient (96%).

Table 1.
Sociodemographic variables.
Table 2 presents the different levels of the variables objective burden, subjective burden, psychological distress, and resilience. Means and standard deviations are also presented for the last three variables. Most caregivers cared for more than 15 h per day (42.4%), perceived a moderate burden (50%), were almost split in half in relation to high-low psychological distress, and over half presented high resilience (56.8%). Looking at the means, all of them were over the cut-off scores for moderate perceived burden, high psychological distress, and high resilience.
Table 2.
Means, standard deviations and levels in objective burden, subjective burden, psychological distress, and resilience.
The comparison between high and low psychological distress groups is presented in Table 3. There are no significant differences in caregivers’ age or in care recipients‘ age; however, significant differences were shown in burden and resilience. Caregivers showing a high level of psychological distress were those caring for more hours per day, perceiving high burden, and a lower level of resilience. The differences in perceived burden and resilience were high, with a size effect greater than 1 standard deviation (d = 1.19).
Table 3.
Differential analysis between the psychological distress levels.
According to the pattern presented in the difference analysis, the relationships, shown in Table 4, between burden, both objective and subjective, and psychological distress were positive and significant, whereas those with resilience were significant but negative. Although the variables caregivers‘ age and care recipients‘ age produced no differences in psychological distress, in the correlation analysis, a few significant relationships were present. Older caregivers cared for older ASD relatives and for fewer hours per day than younger caregivers.
Table 4.
Correlation analysis.
Based on previous relationships, a serial mediational analysis was performed to test the mediational role of resilience and perceived burden between hours per day of caring and psychological distress. The results are shown in Figure 1.
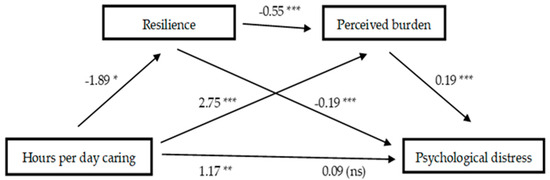
Figure 1.
Multiple serial mediation of resilience and perceived burden between hours per day of caring and psychological distress. * = p ≤ 0.05; ** = 0.01; *** = p ≤ 0.001.
Step 1: As can be seen, the total effect (B = 1.17, SE = 0.39, t = 3.00, p < 0.003, 95% CI [0.40, 1.93]) of hours per day of caregiving on psychological distress was statistically significant.
Step 2: In addition, the direct effects of daily hours of caregiving on resilience (B = −1.89, SE = 0.78, t = −2.42, p = 0.016, 95% CI [−3.44, −0.35]), and on perceived burden (B = 2.75, SE = 0.79, t = 3.48, p < 0.001, 95% CI [1.19, 4.30]) were also significant. The direct effect of resilience as the first mediating variable on the second mediating variable, perceived burden (B = −0.55, SE =0.06, t = −8.61, p < 0.001, 95% CI [−0.67, −0.42]) was also at a significant level.
Step 3: On the other hand, the direct effects of the mediating variables on psychological distress showed that the effects of resilience (B = −0.19, SE = 0.03, t = −7.20, p < 0.001, 95% CI [−0.24, −0.14]) and perceived burden (B = 0.19, SE = 0.02, t = 8.33, p < 0.001, 95% CI [0.15, 0.24]) were also significant.
Step 4: When the amount of daily hours of caregiving and the mediating variables were simultaneously entered into the equation, the relation between the amount of daily hours caregiving and psychological distress was not at a significant level (B = 0.09, SE = 0.29, t = 0.33, p = 0.745, 95% CI [−4.88, 0.67]).
The overall model was significant (F(3,246) = 83.36, p < 0.001) and explained 50% of the total variance in psychological distress.
Finally, the contrast of indirect effects presented in Table 5 showed that neither the serial multiple mediation of resilience through subjective burden nor the separate mediating effect of subjective burden was found statistically different from each other. On the other hand, the variable resilience was observed to have stronger mediation power than the serial multiple mediation of resilience and subjective burden or the separate mediation of subjective burden.
Table 5.
Indirect effects and comparison between them.
4. Discussion
The mental health of ASD caregivers is a key element in the wellbeing of both caregivers and care recipients due to the close dependency between them. Mental health is the dependent variable in our study, the one that is affected by any other variable included in it, where burden as a risk factor and resilience as a protective factor have played important roles.
The sample used in our study was comprised mainly women, mothers caring for a son or daughter, in most cases children. A wide majority of studies on caregivers have more women than men as participants, showing higher levels of burden and psychological distress than men [33,58,59,60,61]. Therefore, it could be said that our sample represents what is typical in the care of ASD people regarding gender.
Focusing on the results, the first hypothesis stated that ASD caregivers would present high levels of burden, objective, measured as hours per day of care, and subjective, measured as perceived burden, psychological distress, and low levels of resilience. The results confirm that the burden levels of the caregivers were high in both, objective burden, where most caregivers cared for more than 15 h every day, and perceived burden, where half of the caregivers presented moderate levels, and more than a quarter reported severe levels of perceived burden. Both the mean and the levels of burden were much higher in this study than those found by Al-Qahtani in ASD caregivers [31]: an average of 41.00 against 54.56 in our study, and 35% in the moderate level and 2.5% in the severe level against 50% in the moderate levels and 34% in the severe level in this study. Eighty-four percent of ASD caregivers showed moderate to severe levels in this research, whereas in Al-Qahtani [31], only thirty-five percent of ASD caregivers presented moderate to severe levels of burden. Therefore, the first hypothesis concerning burden is confirmed, giving support to other studies showing high levels of burden in ASD caregivers [22,23,30,31], reflecting the time and effort caregivers dedicate to their relatives.
The strong relationship usually found between burden and psychological distress in caregivers [12,15,16] led us to hypothesize that psychological distress, which is a wide spectrum of psychological symptoms, would also be high in our sample. This variable, also part of the first hypothesis, is also confirmed, with half of the sample (49.6%) being classified as suffering from high psychological distress, according to the levels proposed by Lunding et al. [53]. The research performed by Almazly and Abojedi [62] found symptoms of anxiety and depression in ASD caregivers dedicating more time to the care of their relative than in those who dedicated less time. Likewise, the percentage of caregivers showing high psychological distress in this study, 49,6%, is very similar to the 48% of the ASD caregivers found by Kalb et al. [63].
Resilience as a protective factor has been assessed in ASD caregivers in the context of growth, where caregivers not only resist and recover from the stressful situation but also grow from these situations [64,65,66]. The last two cited studies used the CD-RISC scale used in this study; however, only the study of Qin [65] found a mean in ASD caregivers (64.49) close to the mean obtained in this study (65.27), stating that caring for a child with ASD is an important related factor for parents’ growth. The research presented by Rasoulpoor [66] showed lower scores in resilience in Iran (52.7) using the same scale and with the same type of caregivers. It would be interesting to find out why there are such differences between the studies carried out in China, Iran, and Spain, as they may be related to cultural factors.
Finally, although our results confirm the first hypothesis concerning the high levels of burden and psychological distress in ASD caregivers, they do not confirm the hypothesis when it comes to resilience, as it seems to be high rather than low, contrary to what we predicted. High resilience in ASD caregivers has been found in those with high social support [67,68,69], having no difficulties dealing with the ASD relative’s behavior [68], focused on problem coping strategies, and showing high quality of life and self-efficacy [69]. Tentatively, these variables could play an important role in the high levels of resilience found in this study.
The second and third hypotheses are related, and both are based on bivariate analyses, the first differential and the second correlational, where significant and positive relationships between burden and psychological distress and negative relationships between these variables and resilience were expected. Additionally, burden was expected to be high if psychological distress was also high, but resilience was expected to be low if psychological distress was high. Both hypotheses are completely confirmed by our results. Caregivers showing high psychological distress presented high burden, both as objective burden, caring for more hours, and as subjective burden, perceiving high levels of burden, but lower resilience, in any case with significant differences and, in the case of perceived burden and resilience, with strong effect sizes. This pattern is confirmed in the correlation matrix with positive and significant relationships between psychological distress and burden, but negative between those variables and resilience. Many studies have supported the close relationship between burden and depressive and anxiety symptoms in caregivers [12,15,16,17,22,23,24,36,62,63], in addition to those that found negative relationships between burden and psychological distress with resilience [64,65,66].
Having confirmed the significant relations between burden, both objective and subjective, psychological distress, and resilience, the last hypothesis was intended to elucidate the role of resilience as a buffer of hours caring for an ASD relative in the burden perception and in the mental health of the caregivers. The serial mediation analysis performed has confirmed this fourth hypothesis. The introduction of resilience between the variables hours per day caring and perceived burden showed, firstly, the buffer effect of resilience in the lower perception of burden, despite long hours of care, and, secondly, the introduction of resilience as a mediating variable between hours per day caring and psychological distress also showed the positive effect of resilience on mental health, this being the strongest effect according to the comparison of the three models. In the third place, the serial effect of resilience and perceived burden being introduced in the equation between hours caring per day and psychological distress produced almost no effect (B = 0.09, non-significant) of hours per day caring on psychological distress, giving rise to full mediation. Previous studies have supported the mediational role of positive variables between burden and psychological distress in family caregivers of people with Alzheimer’s disease, such as happiness, gain in caregiving, quality of life [12], optimism [15], or resilience [16]. In a similar way, this study confirms that resilience also shows a mediational role in lowering the stressful situation of ASD caregivers, positively affecting burden and psychological distress.
Finally, some limitations should be considered. This is a cross-sectional design study; therefore, causal relationships cannot be made. The use of self-reports carries the risk of biases such as social desirability. Generalizations of results should consider two important factors: (i) the sample is a Spanish one with participants from different provinces; and (ii) gender, as most of the ASD caregivers were women, and specifically, mothers of the care recipients. Future research should focus on the factors that affect resilience in ASD caregivers. Finding out what contributes to increasing or enhancing resilience will have repercussions for the caregiver’s mental health. In addition, better representation of both parents, father and mother, should be considered.
5. Conclusions
The main objectives of this research were, firstly, to determine the state of ASD caregivers in objective and subjective burden, psychological distress, and resilience, and secondly, to assess the role of resilience as a mediator variable that could buffer the effect of objective burden on perceived burden and psychological distress. According to our results, ASD caregivers in our sample presented high levels of objective burden, caring for many hours, and most of them showed moderate to severe perceived burden. Half of the sample presented psychological distress, and over half presented high resilience. Our result also showed the buffer role of resilience on objective burden, hours a day caring, with a positive effect in lowering perceived burden and psychological distress. Lastly, these results point to the necessity of implementing intervention or training programs that help caregivers cope with stressors associated with the daily tasks of caring to, ultimately, enhance resilience and personal growth out of stressful situations.
Author Contributions
Conceptualization, R.H. and A.D.; methodology, R.H. and A.D.; formal analysis, R.H. and A.D.; investigation, R.H. and A.D.; data curation, R.H.; writing—original draft preparation, A.D.; writing—review and editing, R.H. and A.D.; supervision, A.D. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the University of Valencia (H1367489852167/19 February 2022).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- APA, American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Elsabbagh, M.; Divan, G.; Koh, Y.J.; Kim, Y.S.; Kauchali, S.; Marcín, C.; Montiel-Nava, C.; Patel, V.; Paula, C.S.; Wang, C.; et al. Global prevalence of autism and other pervasive developmental disorders. Autism Res. 2012, 5, 160–179. [Google Scholar] [CrossRef] [PubMed]
- Zeidan, J.; Fombonne, E.; Scorah, J.; Ibrahim, A.; Durkin, M.S.; Saxena, S.; Yusuf, A.; Shih, A.; Elsabbagh, M. Global prevalence of autism: A systematic review update. Autism Res. 2022, 15, 778–790. [Google Scholar] [CrossRef] [PubMed]
- WHO, World Health Organization. Autism. Available online: https://www.who.int/news-room/fact-sheets/detail/autism-spectrum-disorders (accessed on 5 February 2025).
- Loomes, R.; Hull, L.; Mandy, W.P. What is the male-to-female ratio in autism spectrum disorder? A systematic review and meta-analysis. J. Am. Acad. Child. Adolesc. Psychiatry 2017, 56, 466–474. [Google Scholar] [CrossRef]
- Hiller, R.M.; Young, R.L.; Weber, N. Sex differences in pre-diagnosis concerns for children later diagnosed with autism spectrum disorder. Autism 2016, 20, 75–84. [Google Scholar] [CrossRef]
- Lord, C.; Elsabbagh, M.; Baird, G.; Veenstra-Vanderweele, J. Autism spectrum disorder. Lancet 2018, 392, 508–520. [Google Scholar] [CrossRef]
- Snow, M.; Donnelly, J. Factors mediating dysphoric moods and help seeking behaviour among Australian parents of children with autism. J. Autism Dev. Disord. 2016, 46, 1941–1952. [Google Scholar] [CrossRef]
- Appah, J.; Senoo-Dogbey, V.E.; Armah, D.; Wuaku, D.A.; Ohene, L.A. A qualitative enquiry into the challenging roles of caregivers caring for children with autism spectrum disorders in Ghana. J. Pediatr. Nurs. 2024, 76, 23–29. [Google Scholar] [CrossRef] [PubMed]
- ten Hoopen, L.W.; de Nijs, P.F.A.; Duvekot, J.; Greaves-Lord, K.; Hillegers, M.H.J.; Brouwer, W.B.F.; Hakkaart-van Roijen, L. Children with an autism spectrum disorder and their caregivers: Capturing health-related and care-related quality of life. J. Autism Dev. Disord. 2020, 50, 263–277. [Google Scholar] [CrossRef]
- Eisenhower, A.S.; Baker, B.L.; Blacher, J. Preschool children with intellectual disability: Syndrome specificity, behaviour problems, and maternal well-being. J. Intellect. Disabil. Res. 2005, 49, 657–671. [Google Scholar] [CrossRef]
- Ponsoda, J.M.; Díaz, A. Psychological distress in family caregivers of people with Alzheimer’s disease: Positive and negative aspects of caregiving. Global Health Econ. Sustain. 2024, 2, 3145. [Google Scholar] [CrossRef]
- Bekhet, A.K.; Johnson, N.L.; Zauszniewski, J.A. Resilience in family members of persons with autism spectrum disorder: A review of the literature. Issues Ment. Health Nurs. 2012, 33, 650–656. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Zhang, H.; Zhang, M.; Li, T.; Ma, W.; An, C.; Chen, Y.; Liu, S.; Kuang, W.; Yu, X.; et al. Prevalence and risk factors of anxiety, depression, and sleep problems among caregivers of people living with neurocognitive disorders during the COVID-19 pandemic. Front. Psychiatry 2021, 11, 590343. [Google Scholar] [CrossRef] [PubMed]
- Díaz, A.; Ponsoda, J.M.; Beleña, M.A. Optimism as a key to improving mental health in family caregivers of people living with Alzheimer’s disease. Aging Ment. Health 2020, 24, 1662–1670. [Google Scholar] [CrossRef]
- Ponsoda, J.M.; Beleña, M.Á.; Díaz, A. Psychological distress in Alzheimer’s disease family caregivers: Gender differences and the moderated mediation of resilience. Healthcare 2023, 11, 3084. [Google Scholar] [CrossRef] [PubMed]
- Padden, C.; James, J. Stress among parents of children with and without autism spectrum disorder: A comparison involving physiological indicators and parent self-reports. J. Dev. Phys. Disabil. 2017, 9, 567–586. [Google Scholar] [CrossRef]
- Yamada, A.; Suzuki, M.; Kato, M.; Suzuki, M.; Tanaka, S.; Shindo, T.; Taketani, K.; Akechi, T.; Furukawa, T.A. Emotional distress and its correlates among parents of children with pervasive developmental disorders. Psychiatry Clin. Neurosci. 2007, 61, 651–657. [Google Scholar] [CrossRef]
- Johnson, N.; Frenn, M.; Feetham, S.; Simpson, P. Autism spectrum disorder: Parenting stress, family functioning and health-related quality of life. Fam. Syst. Health 2011, 29, 232–252. [Google Scholar] [CrossRef]
- Scherer, N.; Verhey, I.; Kuper, H. Depression and anxiety in parents of children with intellectual and developmental disabilities: A systematic review and meta-analysis. PLoS ONE 2019, 14, e0219888. [Google Scholar] [CrossRef]
- Ang, K.Q.P.; Loh, P.R. Mental health and coping in parents of children with autism spectrum disorder (ASD) in Singapore: An examination of gender role in caring. J. Autism Dev. Disord. 2019, 49, 2129–2145. [Google Scholar] [CrossRef]
- Yıldız, M.; Demir, Y.; Kırcalı, A.; İncedere, A. Caregiver burden in schizophrenia and autism spectrum disorders: A comparative study. Psychiatry Investig. 2021, 18, 1180–1187. [Google Scholar] [CrossRef]
- Baykal, S.; Karakurt, M.N.; Çakır, M.; Karabekiroğlu, K. An examination of the relations between symptom distributions in children diagnosed with autism and caregiver burden, anxiety and depression levels. Community Ment. Health J. 2019, 55, 311–317. [Google Scholar] [CrossRef] [PubMed]
- Ingersoll, B.; Hambrick, D. The relationship between the broader autism phenotype, child severity, and stress and depression in parents of children with autism spectrum disorders. Res. Autism Spectr. Disord. 2011, 5, 337–344. [Google Scholar] [CrossRef]
- Green, C.C.; Smith, J.; Bent, C.A.; Chetcuti, L.; Sulek, R.; Uljarević, M.; Hudry, K. Differential predictors of well-being versus mental health among parents of pre-schoolers with autism. Autism 2021, 25, 1125–1136. [Google Scholar] [CrossRef]
- Yorke, I.; White, P.; Weston, A.; Rafla, M.; Charman, T.; Simonoff, E. The association between emotional and behavioral problems in children with autism spectrum disorder and psychological distress in their parents: A systematic review and meta-analysis. J. Autism Dev. Disord. 2018, 48, 3393–3415. [Google Scholar] [CrossRef] [PubMed]
- Landon, J.; Shepherd, D.; Goedeke, S. Predictors of satisfaction with life in parents of children with autism spectrum disorder. J. Autism Dev. Disord. 2018, 48, 1640–1650. [Google Scholar] [CrossRef]
- Martin, F.; Clyne, W.; Pearce, G.; Turner, A. Self-management support intervention for parents of children with developmental disorders: The role of gratitude and hope. J. Child. Fam. Stud. 2019, 28, 980–992. [Google Scholar] [CrossRef]
- Quintero, N.; McIntyre, L.L. Sibling adjustment and maternal well-being: An examination of families with and without a child with an autism spectrum disorder. Focus Autism Other Dev. Disabil. 2010, 25, 37–46. [Google Scholar] [CrossRef]
- Stuart, M.; McGrew, J.H. Caregiver burden after receiving a diagnosis of an autism spectrum disorder. Res. Autism Spectr. Disord. 2009, 3, 86–97. [Google Scholar] [CrossRef]
- Al-Qahtani, F.S. Experienced burden by caregivers of autistic children. Med. J. Cairo Univ. 2018, 86, 1523–1528. [Google Scholar] [CrossRef][Green Version]
- Zarit, S.H.; Reever, K.E.; Bach-Peterson, J. Relatives of the impaired elderly: Correlates of feelings of burden. Gerontologist 1980, 20, 649–655. [Google Scholar] [CrossRef]
- Mulud, Z.A.; McCarthy, G. Caregiver burden among caregivers of individuals with severe mental illness: Testing the moderation and mediation models of resilience. Arch. Psychiatr. Nurs. 2017, 31, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Pruitt, M.M.; Rhoden, M.; Ekas, N.V. Relationship between the broad autism phenotype, social relationships and mental health for mothers of children with autism spectrum disorder. Autism 2018, 22, 171–180. [Google Scholar] [CrossRef] [PubMed]
- Gere, J.; Goodman, B.J. Mechanics of Materials, 4th ed.; Cengage Learning: Toronto, ON, Canada, 2009. [Google Scholar]
- Bowlby, J. Maternal care and mental health. Bull. World Health Organ. 1951, 3, 355–533. [Google Scholar]
- Block, J.H.; Block, J. The Role of Ego-Control and Ego Resiliency in the Organization of Behavior; Collins, W.A., Ed.; Minnesota Symposium on Child Psychology; Erlbaum: Hillsdale, NJ, USA, 1980; pp. 39–101. [Google Scholar]
- Walsh, F. Strengthening Family Resilience, 2nd ed.; Guilford Press: New York, NY, USA, 2006. [Google Scholar]
- Southwick, S.M.; Bonanno, G.A.; Masten, A.S.; Panter-Brick, C.; Yehuda, R. Resilience definitions, theory, and challenges: Interdisciplinary perspectives. Eur. J. Psychotraumatol. 2014, 5, 25338. [Google Scholar] [CrossRef]
- Den Hartigh, R.J.R.; Hill, Y. Conceptualizing and measuring psychological resilience: What can we learn from physics? New Ideas Psychol. 2022, 66, 100934. [Google Scholar] [CrossRef]
- Bonanno, G.A.; Westphal, M.; Mancini, A.D. Resilience to loss and potential trauma. Annu. Rev. Clin. Psychol. 2011, 7, 511–535. [Google Scholar] [CrossRef]
- Hill, Y.; Den Hartigh, R.J.R.; Meijer, R.R.; De Jonge, P.; Van Yperen, N.W. The temporal process of resilience. Sport Exerc. Perform. Psychol. 2018, 7, 363–370. [Google Scholar] [CrossRef]
- Connor, K.M.; Davidson, J.R.T. Development of a new resilience scale: The Connor-Davidson Resilience Scale (CD-RISC). Depress. Anxiety 2003, 18, 76–82. [Google Scholar] [CrossRef]
- Kiefer, A.W.; Silva, P.L.; Harrison, H.S.; Araújo, D. Antifragility in sport: Leveraging adversity to enhance performance. Sport Exerc. Perform. Psychol. 2018, 7, 342–350. [Google Scholar] [CrossRef]
- Hill, Y.; Kiefer, A.W.; Silva, P.L.; Van Yperen, N.W.; Meijer, R.R.; Den Hartigh, R.J.R. Antifragility in climbing: Determining optimal stress loads for athletic performance training. Front. Psychol. 2020, 11, 272. [Google Scholar] [CrossRef]
- Ghanouni, P.; Hood, G. Stress, coping, and resiliency among families of individuals with autism: A systematic review. J. Autism Dev. Disord. 2021, 8, 389–402. [Google Scholar] [CrossRef]
- Sowmida, M.S.; Novena, S.; Hothi, S.; Singh, V. Exploring the relationship between perceived social support, perceived stress, and resilience among caregivers of children with autism. Int. J. Soc. Sci. Rev. 2023, 11, 437–441. [Google Scholar]
- Bekhet, A.K.; Johnson, N.L.; Zauszniewski, J.A. Effects on resilience of caregivers of persons with autism spectrum disorder: The role of positive cognitions. J. Am. Psychiatr. Nurses Assoc. 2012, 18, 337–344. [Google Scholar] [CrossRef]
- Bitsika, V.; Sharpley, C.; Bell, R. The buffering effect of resilience upon stress, anxiety and depression in parents of a child with an autism spectrum disorder. J. Dev. Phys. Disabil. 2013, 25, 533–543. [Google Scholar] [CrossRef]
- Ghanouni, P.; Eves, L. Resilience among parents and children with autism spectrum disorder. Ment. Illn. 2023, 2023, 2925530. [Google Scholar] [CrossRef]
- Goldberg, D.P.; Gater, R.; Sartorius, N.; Ustun, T.B.; Piccinelli, M.; Gureje, O. The validity of two versions of the GHQ in the WHO study of mental illness in general health care. Psychol. Med. 1997, 27, 191–197. [Google Scholar] [CrossRef]
- Cifre, E.; Salanova, M. Validación factorial de “General Health Questionnaire” (GHQ-12) mediante un análisis factorial confirmatorio [Factor validation of “General Health Questionnaire” (GHQ-12) through a confirmatory factor analysis]. J. Health Psychol. 2000, 12, 75–89. [Google Scholar]
- Lundin, A.; Ahs, J.; Asbring, N.; Kosidou, K.; Dal, H.; Tinghog, P.; Saboonchi, F.; Dalman, C. Discriminant validity of the 12-item version of the general health questionnaire in a Swedish case-control study. Nord. J. Psychiatry 2016, 71, 171–179. [Google Scholar] [CrossRef]
- Martín-Carrasco, M.; Otermin, P.; Pérez-Camo, V.; Pujol, J.; Agüera, L.; Martín, M.J.; Gobarrt, A.L.; Pons, S.; Balana, M. EDUCA study: Psychometric properties of the Spanish version of the Zarit Caregiver Burden Scale. Aging Ment. Health 2010, 14, 705–711. [Google Scholar] [CrossRef]
- Crespo, M.; Fernandez-Lansac, V.; Soberon, C. Spanish version of the Connor-Davidson Resilience Scale (CD-RISC) for chronic stress situations. Behav. Psychol. 2014, 22, 219–238. [Google Scholar]
- Okuyama, J.; Funakoshi, S.; Tomita, H.; Yamaguchi, T.; Matsuoka, H. Longitudinal characteristics of resilience among adolescents: A high school student cohort study to assess the psychological impact of the Great East Japan Earthquake. Psychiatry Clin. Neurosci. 2018, 72, 821–835. [Google Scholar] [CrossRef] [PubMed]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach, 3rd ed.; The Guilford Press: New York, NY, USA, 2018. [Google Scholar]
- Pinquart, M.; Sörensen, S. Gender differences in caregiver stressors, social resources, and health: An updated meta-analysis. J. Gerontol. B Psychol. Sci. Soc. Sci. 2006, 61, 33–45. [Google Scholar] [CrossRef] [PubMed]
- McDonnell, E.; Ryan, A.A. The experience of sons caring for a parent with dementia. Dementia 2014, 13, 788–802. [Google Scholar] [CrossRef] [PubMed]
- Penning, M.J.; Wu, Z. Caregiver stress and mental health: Impact of caregiving relationship and gender. Gerontologist 2016, 56, 1102–1113. [Google Scholar] [CrossRef]
- Revenson, T.A.; Konstadina, G.; Aleksandra, L.; Morrison, V.; Panagopoulou, E.; Vilchinsky, N.; Hagedoorn, M. Gender and Caregiving: The Costs of Caregiving for Women. In Caregiving in the Illness Context; Revenson, T.A., Griva, K., Luszczynska, A., Morrison, V., Panagopoulou, E., Vilchinsky, N., Eds.; Palgrave Macmillan: Basingstoke, UK, 2016; pp. 49–63. [Google Scholar]
- Alnazly, E.K.; Abojedi, A. Psychological distress and perceived burden in caregivers os person with autism spectrum disorder. Perspect. Psychiatr. Care 2019, 55, 501–508. [Google Scholar] [CrossRef]
- Kalb, L.G.; Badillo-Goicoechea, E.; Holingue, C.; Riehm, K.E.; Thrul, J.; Stuart, E.A.; Smail, E.J.; Law, K.; White-Lehman, C.; Fallin, D. Psychological distress among caregivers raising a child with autism spectrum disorder during the COVID-19 pandemic. Autism Res. 2021, 14, 2183–2188. [Google Scholar] [CrossRef]
- Safe, A.; Joosten, A.; Molineux, M. The experiences of mothers of children with autism: Managing multiple roles. J. Intellect. Dev. Disabil. 2012, 37, 294–302. [Google Scholar] [CrossRef]
- Qin, X.; Feng, Y.; Qu, F.; Luo, Y.; Chen, B.; Chen, M.; Zou, Y.; Zhang, L. Posttraumatic growth among parents of children with autism spectrum disorder in China and its relationship to family function and mental resilience: A cross-sectional study. J. Pediatr. Nurs. 2021, 57, e59–e67. [Google Scholar] [CrossRef]
- Rasoulpoor, S.; Salari, N.; Shiani, A.; Khaledi-Paveh, B.; Mohammadi, M. Determining the relationship between over-care burden and coping styles, and resilience in mothers of children with autism spectrum disorder. Ital. J. Pediatr. 2023, 49, 53. [Google Scholar] [CrossRef]
- Hayes, K.N.; Rossetti, K.G.; Zlomke, K. Community support, family resilience and mental health among caregivers of youth with autism spectrum disorder. Child Care Health Dev. 2023, 49, 130–136. [Google Scholar] [CrossRef]
- Al-Jadiri, A.; Tybor, D.J.; Mulé, C.; Sakai, C. Factors associated with resilience in families of children with Autism Spectrum Disorder. J. Dev. Behav. Pediatr. 2021, 42, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Chakurian, D. Resilience in family caregivers of adults with Autism Spectrum Disorder: An Integrative Review of the literature. Innov. Aging 2021, 17 (Suppl. S1), 817–818. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).