

Design and Implementation of a Low-Power Device for Non-Invasive Blood Glucose


Abstract
1. Introduction
2. Research and System Design
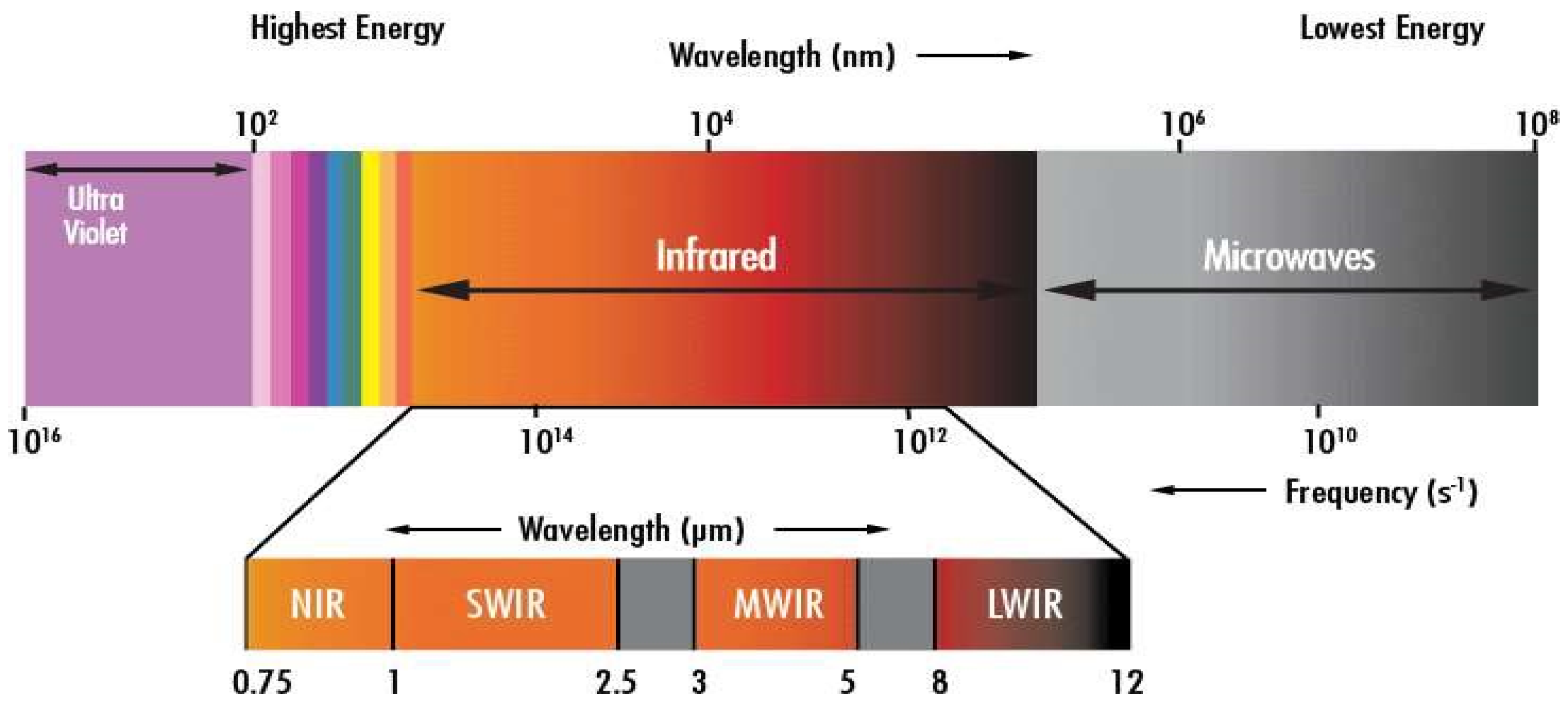
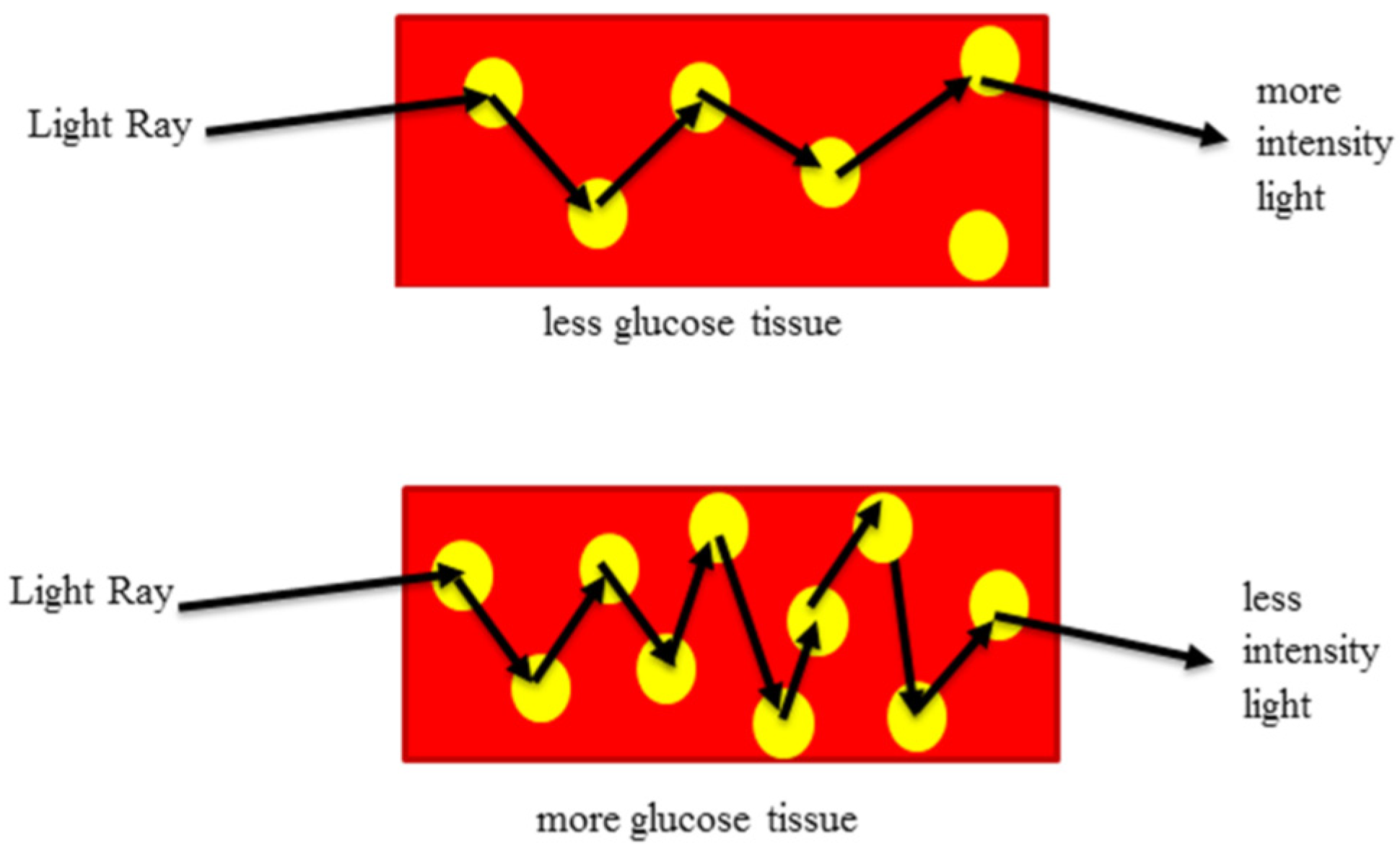
2.1. Light Spectrum and 940 nm Infrared Spectrum
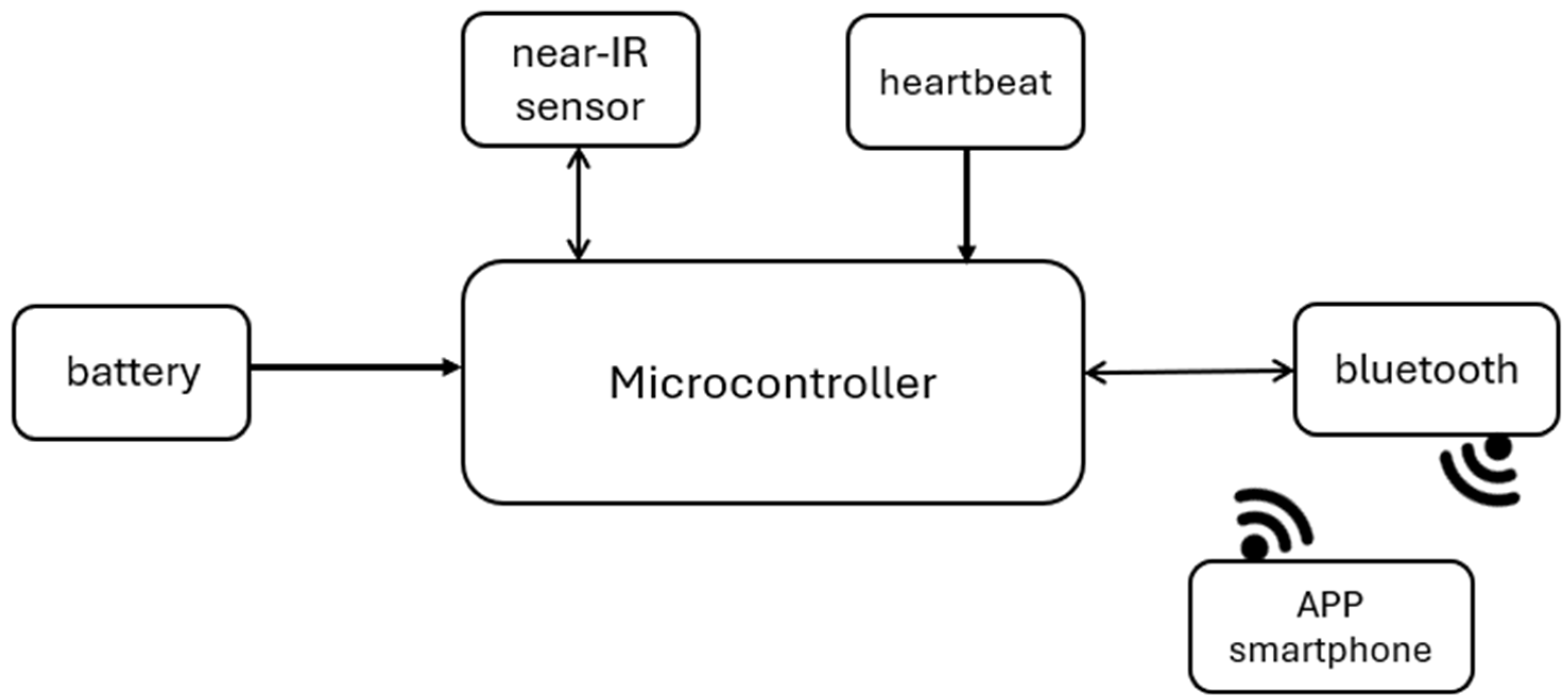
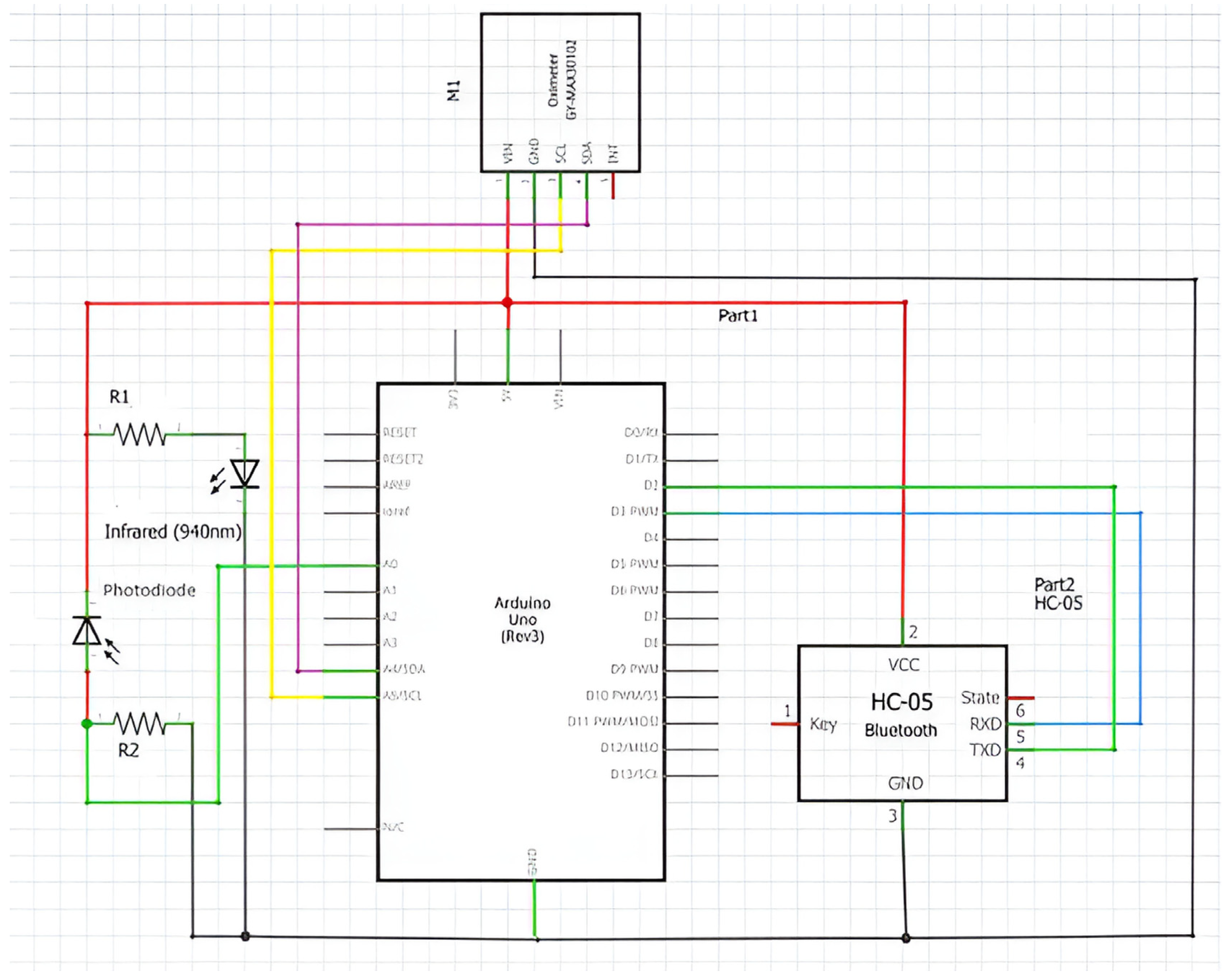
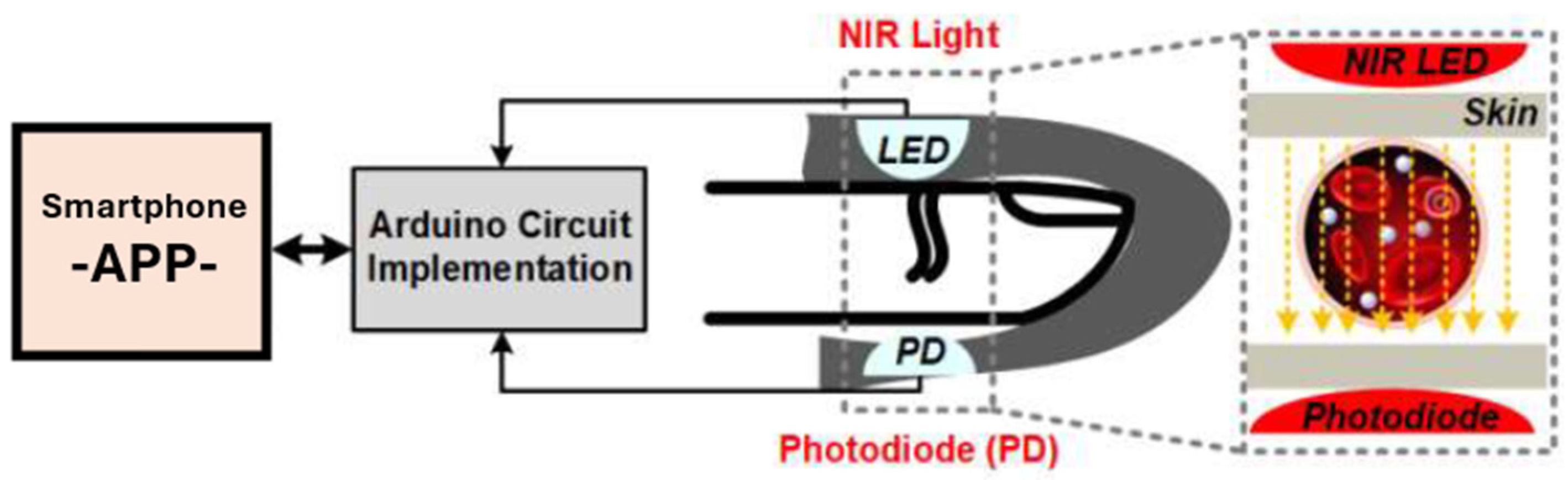
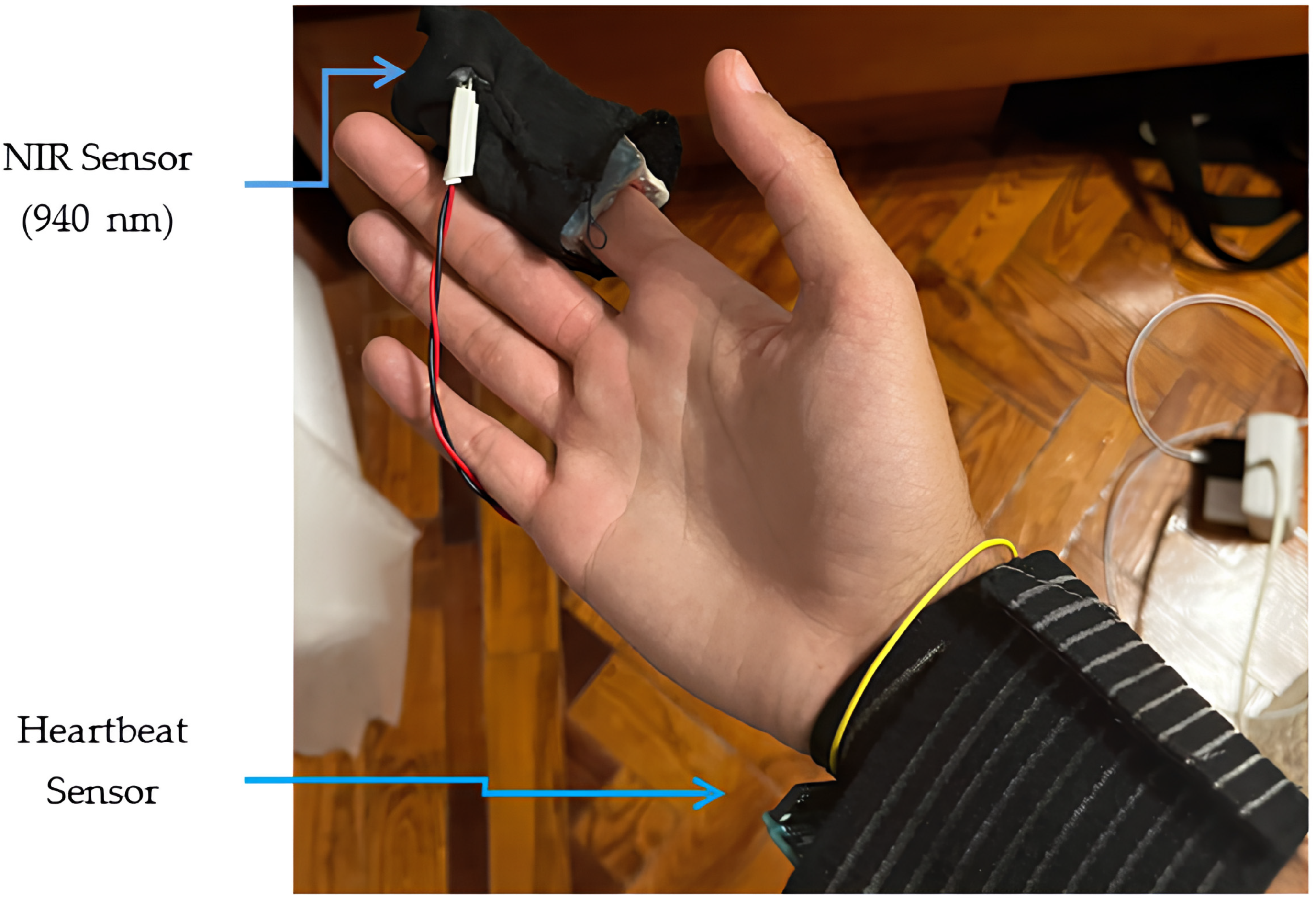
2.2. System Design
- -
- Ten-bit resolution: Converts analog signals into digital ones, allowing through this resolution the production of 210 (1024) possible values for each conversion.
- -
- Input voltage range: Possibility of measuring input voltages in the 0 V to 5 V range.
- -
- Input channels: This ADC offers six input channels, labelled ADC0 to ADC5, each of which can be individually selected for conversion.
- -
- Sample rate: The ADC’s maximum sample rate is 15,000 samples per second.
- C-H Bonds (Carbon–Hydrogen): C-H bonds are present everywhere in organic molecules. They appear as distinctive bands in NIR spectra between 2050 nm and 2180 nm.
- O-H Bonds (Water): Water molecules exhibit strong absorption in the NIR range. Their absorption bands are broad and dominant. The main absorption bands from liquid water are located around 1450 nm and 1940 nm.
- N-H Bonds (Protein): Protein content is challenging to spot at lower concentrations, but it manifests as two distinctive bands. These bands occur at 2050 nm and 2180 nm.
- S-H Bonds (Thiols): S-H bonds represent the presence of thiols, which are sulfur- containing organic compounds. Thiols are commonly found in proteins, amino acids, and other biological molecules. The absorption bands associated with S-H bonds typically occur around 2500 nm in the NIR spectrum.
- Second (Upper) Harmonic Band (750–1400 nm): This band corresponds to the second harmonic of fundamental vibrations.
- ◦
- Key Features:
- ▪
- Overtone Absorptions: In this range, we observe overtone absorptions related to fundamental vibrations of various chemical bonds.
- ▪
- C-H Bonds: The second harmonic band includes overtones (multiples of the fundamental frequency) of C-H bonds, which are prevalent in organic compounds.
- ▪
- Protein and Lipid Content: Researchers often use this band to assess protein and lipid content in samples.
- First Harmonic Band (1400–2000 nm): The first harmonic band corresponds to the fundamental vibrations of specific bonds.
- ◦
- Key Features:
- ▪
- O-H Bonds (Water): Water molecules exhibit strong absorption in this range. Monitoring water content is crucial for various applications.
- ▪
- Protein Bands: The first harmonic band includes absorption features related to protein content (e.g., amide bonds).
- ▪
- Starch and Sugar Bands: Starch and sugar content also contribute to the absorption in this region.
- Combined Harmonic Band (2000–2500 nm): This band combines both fundamental vibrations and overtones.
- ◦
- Key Features:
- ▪
- C-H, N-H, and O-H Bonds: The combined harmonic band includes absorption features related to C-H, N-H, and O-H bonds.
- ▪
- Thiols (S-H Bonds): Thiols (sulfur-containing compounds) also contribute to absorption in this range.
2.3. Algorithm Design
- Declare integer variable i
- Declare float variable value and initialize to 0
- Declare integer variable numReadings and initialize to 3000
- Declare integer variable r
- Declare float variable rs
- Declare float variable gluc
- Loop infinitely:
- Read analog value from pin 0 into r
- Calculate rs:
- rs = (r * (5.0 / 1023.0)) * 1000
- For i from 0 to numReadings - 1
- Add rs to value
- Wait for 1 ms
- Calculate the average value:
- value = value / numReadings
- Calculate gluc:
- gluc = (−0.03 * value) + 221.45
- Send gluc via Bluetooth serial interface
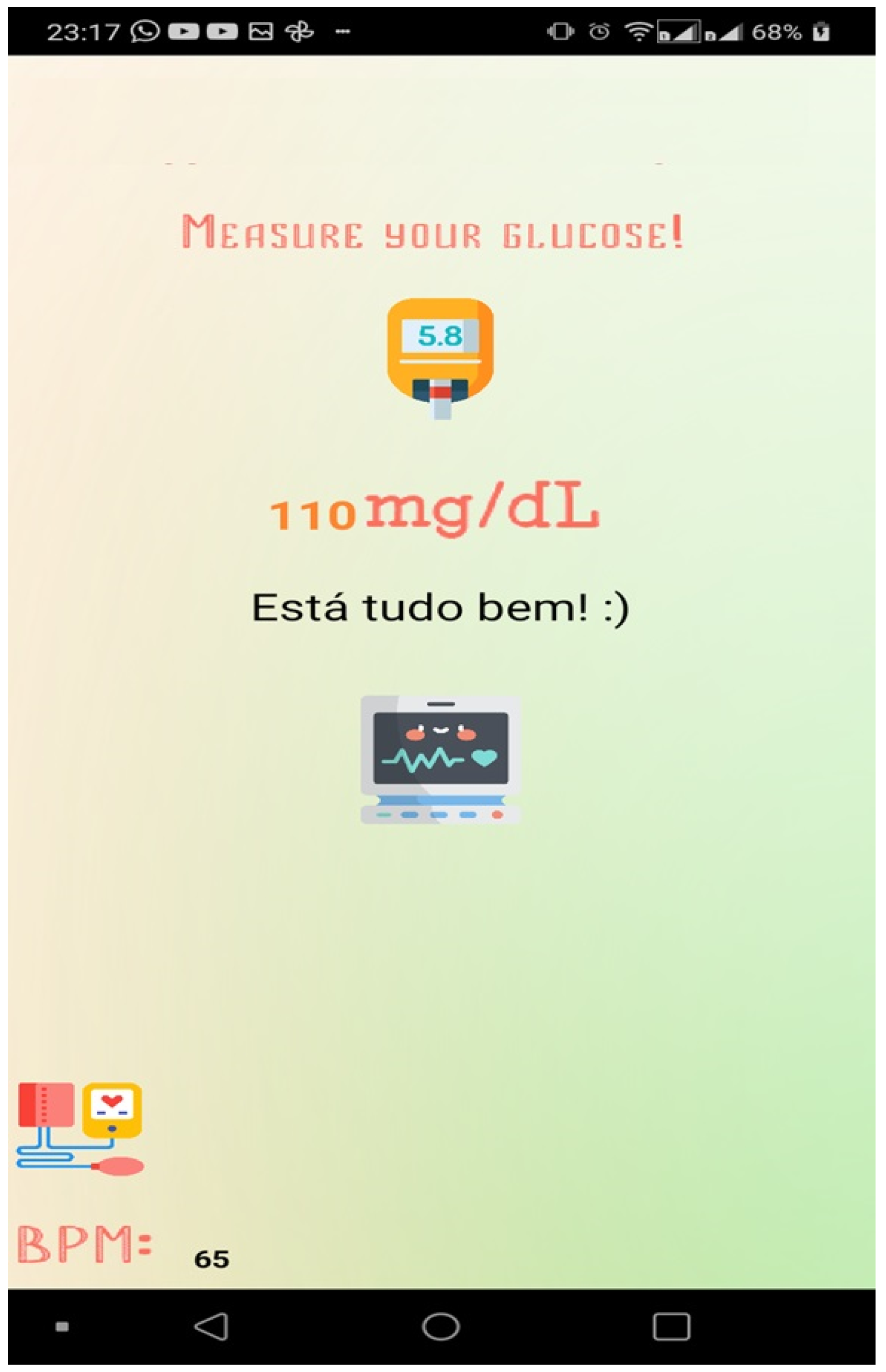
3. Results and Discussion
- -
- -
- ▪ Normal: less than 100 mg/dL;
- ▪ Prediabetes: between 100 and 125 mg/dL;
- ▪ Diabetes: 126 mg/dL or higher.
4. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Gonzales, W.V.; Mobashsher, A.T.; Abbosh, A. The progress of glucose monitoring—A review of invasive to minimally and non-invasive techniques, devices and sensors. Sensors 2019, 19, 800. [Google Scholar] [CrossRef] [PubMed]
- Cho, O.K.; Kim, Y.O.; Mitsumaki, H.; Kuwa, K. Noninvasive measurement of glucose by metabolic heat conformation method. Clin. Chem. 2004, 50, 1894–1898. [Google Scholar] [CrossRef]
- Lin, T.; Gal, A.; Mayzel, Y.; Horman, K.; Bahartan, K. Non-invasive glucose monitoring: A review of challenges and recent advances. Curr. Trends Biomed. Eng. Biosci. 2017, 6, 555696. [Google Scholar] [CrossRef]
- Di Filippo, D.; Sunstrum, F.N.; Khan, J.U.; Welsh, A.W. Non-Invasive Glucose Sensing Technologies and Products: A Comprehensive Review for Researchers and Clinicians. Sensors 2023, 23, 9130. [Google Scholar] [CrossRef]
- Xue, Y.; Thalmayer, A.S.; Zeising, S.; Fischer, G.; Lübke, M. Commercial and Scientific Solutions for Blood Glucose Monitoring—A Review. Sensors 2022, 22, 425. [Google Scholar] [CrossRef]
- Islam, M.M.; Manjur, S.M. Design and Implementation of a Wearable System for Non-Invasive Glucose Level Monitoring. In Proceedings of the 2019 IEEE International Conference on Biomedical Engineering, Computer and Information Technology for Health (BECITHCON), Dhaka, Bangladesh, 28–30 November 2019. [Google Scholar]
- Venkataramanan, S.; Kamble, D.; Bairolu, A.; Singh, A.; Rao, R. A Novel Heart Rate and Non-Invasive Glucose Measuring Device. In Proceedings of the International Conference on Communication and Signal Processing, Chennai, India, 6–8 April 2017. [Google Scholar]
- Naresh, M.; Peddakrishna, S. Non-invasive glucose measurement using 950 nm reflective short wave NIR technique. Res. Biomed. Eng. 2023, 39, 747–757. [Google Scholar] [CrossRef]
- Wang, C.; Gong, D.; Feng, P.; Cheng, Y.; Cheng, X.; Jiang, Y.; Zhang, D.; Cai, J. Ultra-Sensitive and Wide Sensing-Range Flexible Pressure Sensors Based on the Carbon Nanotube Film/Stress-Induced Square Frustum Structure. ACS Appl. Mater. Interfaces 2023, 15, 8546–8554. [Google Scholar] [CrossRef] [PubMed]
- Dai, Z.; Lei, M.; Ding, S.; Zhou, Q.; Ji, B.; Wang, M.; Zhou, B. Durable superhydrophobic surface in wearable sensors: From nature to application. Explor. J. 2023, 4, 20230046. [Google Scholar] [CrossRef] [PubMed]
- Quan, Y.-Y.; Chen, Z.; Lai, Y.; Huang, Z.-S.; Li, H. Recent advances in fabricating durable superhydrophobic surfaces: A review in the aspects of structures and materials. J. Mater. Chem. Front. 2021, 5, 1655–1682. [Google Scholar] [CrossRef]
- ISO. Available online: http://www.iso.org (accessed on 10 June 2024).
- ISO 15197:2013; In Vitro Diagnostic Test Systems—Requirements for Blood-Glucose Monitoring Systems for Self-Testing in Managing Diabetes Mellitus. International Organization for Standardization: Geneva, Switzerland, 2013.
- Pleus, S.; Jendrike, N.; Baumstark, A.; Mende, J.; Wehrstedt, S.; Haug, C.; Freckmann, G. Evaluation of System Accuracy, Precision, Hematocrit Influence, and User Performance of Two Blood Glucose Monitoring Systems Based on ISO 15197:2013/EN ISO 15197:2015. Diabetes Ther. 2014, 15, 447–459. [Google Scholar] [CrossRef] [PubMed]
- Parkes, J.L.; Pardo, S.; Slatin, S.L.; Ginsberg, B.H. A New Consesus Error Grid to Evaluate the Clinical Significance of Inaccuracies in the Measurement of Blood Glucose. Diabetes Care 2000, 23, 1143–1148. [Google Scholar] [CrossRef] [PubMed]
- Food Drug Administration. Available online: https://www.fda.gov/media/87721/download (accessed on 10 June 2024).
- Lewandrowski, K.; Cheek, R.; Nathan, D.M.; Godine, J.E.; Hurxthal, K.; Eschenbach, K.; Laposata, M. Implementation of capillary blood glucose monitoring in a teaching hospital and determination of program requirements to maintain quality testing. Am. J. Med. 1992, 93, 419–426. [Google Scholar] [CrossRef] [PubMed]
- Diabetes Daily. How Accurate Are Blood Sugar Meters and Continuous Glucose Monitors, Really?—Diabetes Daily. Available online: https://www.diabetesdaily.com/ (accessed on 10 June 2024).
- Kulcu, E.; Tamada, J.A.; Reach, G.; Potts, R.O.; Lesho, M.J. Physiological Differences Between Interstitial Glucose and Blood Glucose Measured in Human Subjects. Diabetes Care 2003, 26, 2405–2409. [Google Scholar] [CrossRef] [PubMed]
- Lindner, N.; Kuwabara, A.; Holt, T. Non-invasive and minimally invasive glucose monitoring devices: A systematic review and meta-analysis on diagnostic accuracy of hypoglycaemia detection. Syst. Rev. J. 2021, 10, 145. [Google Scholar] [CrossRef] [PubMed]
- Karim, A.; Andersson, J.Y. Infrared detectors: Advances, challenges and new technologies. IOP Conf. Ser. Mater. Sci. Eng. 2013, 51, 012001. [Google Scholar] [CrossRef]
- Shaikh, S.; Nazneen, A.; Ramesh, M. Current Trends in the Application of Thermal Imaging in Medical Condition Analysis. Int. J. Innov. Technol. Explor. Eng. 2019, 8, 2708–2712. [Google Scholar]
- Edmundoptics. Available online: https://www.edmundoptics.com/knowledge-center/application-notes/imaging/what-is-swir/ (accessed on 24 April 2024).
- Arduino. Available online: http://arduino.cc/en/Main/ArduinoBoardUno (accessed on 8 March 2024).
- Microchip. Available online: https://www.microchip.com/en-us/product/atmega328 (accessed on 11 April 2024).
- Reich, G. Near-infrared spectroscopy and imaging: Basic principles and pharmaceutical applications. Adv. Drug Deliv. Rev. 2005, 57, 1109–1143. [Google Scholar] [CrossRef] [PubMed]
- Goodarzi, M.; Sharma, S.; Ramon, H.; Saeys, W. Multivariate calibration of NIR spectroscopic sensors for continuous glucose monitoring. TrAC Trends Anal. Chem. 2015, 67, 147–158. [Google Scholar] [CrossRef]
- Yadav, J.; Rani, A.; Singh, V.; Murari, B.M. Prospects and limitations of non-invasive blood glucose monitoring using near-infrared spectroscopy. Biomed. Signal Process. Control 2015, 18, 214–227. [Google Scholar] [CrossRef]
- Agelet, L.E.; Hurburgh, C.R. A Tutorial on Near Infrared Spectroscopy and Its Calibration. Crit. Rev. Anal. Chem. 2010, 40, 246–260. [Google Scholar] [CrossRef]
- One Touch Select Plus. Available online: https://www.onetouch.in/sites/default/files/2024-01/07262803B_Owners_Guide_SPS_IN_LEG_R1_web.pdf (accessed on 10 June 2024).
- Diabetes Diagnosis & Tests. Available online: https://diabetes.org/about-diabetes/diagnosis (accessed on 21 April 2024).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Values Obtained by IR (mV) | OneTouch Select Plus Meter (mg/dL) |
|---|---|
| 4354.98 | 89 |
| 4174 | 92 |
| 3841.71 | 103 |
| 3499.6 | 110 |
| 3465.3 | 116 |
| 3200 | 125 |
| OneTouch Select Plus Meter (mg/dL) | Values Calculated Using the Expression (mg/dL) | Error (%) |
|---|---|---|
| 89 | 90.8 | 2.02 |
| 92 | 96.23 | 4.59 |
| 103 | 106.19 | 3.09 |
| 110 | 116.46 | 5.87 |
| 116 | 117.49 | 1.28 |
| 125 | 125.45 | 0.36 |
| Values Obtained Heart Rate (BPM) | Average Value (BPM) |
|---|---|
| 56.79 | 57 |
| 56.87 | 57 |
| 54.79 | 55 |
| 54.88 | 55 |
| 56.79 | 57 |
| 56.79 | 57 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pires, L.M.; Martins, J. Design and Implementation of a Low-Power Device for Non-Invasive Blood Glucose. Designs 2024, 8, 63. https://doi.org/10.3390/designs8040063
Pires LM, Martins J. Design and Implementation of a Low-Power Device for Non-Invasive Blood Glucose. Designs. 2024; 8(4):63. https://doi.org/10.3390/designs8040063
Chicago/Turabian StylePires, Luis Miguel, and José Martins. 2024. "Design and Implementation of a Low-Power Device for Non-Invasive Blood Glucose" Designs 8, no. 4: 63. https://doi.org/10.3390/designs8040063
APA StylePires, L. M., & Martins, J. (2024). Design and Implementation of a Low-Power Device for Non-Invasive Blood Glucose. Designs, 8(4), 63. https://doi.org/10.3390/designs8040063