A New Model of a Macular Buckle and a Refined Surgical Technique for the Treatment of Myopic Traction Maculopathy


Abstract
1. Introduction
1.1. The New Medical Device—NPB
1.2. The NPB Loading Device
- To allow a fluent insertion.
- To allow a comfortable check of the NPB position by facilitating the dynamic indentation movements.
- To keep the NPB stable during the suture’s applications.
2. Surgical Technique
Surgery Step by Step
- 1.
- Conjuctival and Tenon Separation. The aim of this step is to perfectly expose the sclera in the superotemporal quadrant, preserving the conjunctiva and Tenon for the final suture and making it able to cover the macular buckle with tissue well at the end of surgery.
- Superior and temporal circumferential conjunctival peritomy is performed in the perilimbal area, preserving the limbus, from 11 to 4 o’clock in the left eye and from 8 to 1 o’clock in the right eye. A radial conjunctival peritomy is advised at the edges of the circumferential peritomy and it should be 2–3 mm at the superonasal edge and 10 mm at the inferotemporal edge.
- The Tenon is dissected from the sclera, trying to preserve its integrity as much as possible.
- The sclera in the superotemporal quadrant is freed from bleeding vessels by applying spot diathermy to obtain a clean surface on which to place the NPB.
- 2.
- Mobilise the Eye. It is important to be able to mobilize the eye during this type of surgery. There are many methods to reach this goal.
- The lateral and superior rectus muscles are exposed by at least 4 mm by gently polishing the insertion from the Tenon capsule. A violent and deeper exposure of the muscle might induce an inflammatory reaction with fibrotic scars. A thick traction thread (for example, Vycril 0\0) is placed around the insertion of the lateral rectus muscle and then knotted (Figure 4). The same is performed for the superior rectus muscle. Traction threads around the muscle insertion allow an easier mobilization of the globe without damaging any tissue. This is what we have always used.
- As an alternative, without exposing the whole muscle insertion, a traction suture can be placed directly into the insertion of the muscles (the superior corner of the lateral and the temporal corner of the superior muscle), but this maneuver could stretch and damage the insertion.
- One more alternative is to place the suture into the anterior sclera. We do not recommend this if the sclera is thin.
- 3.
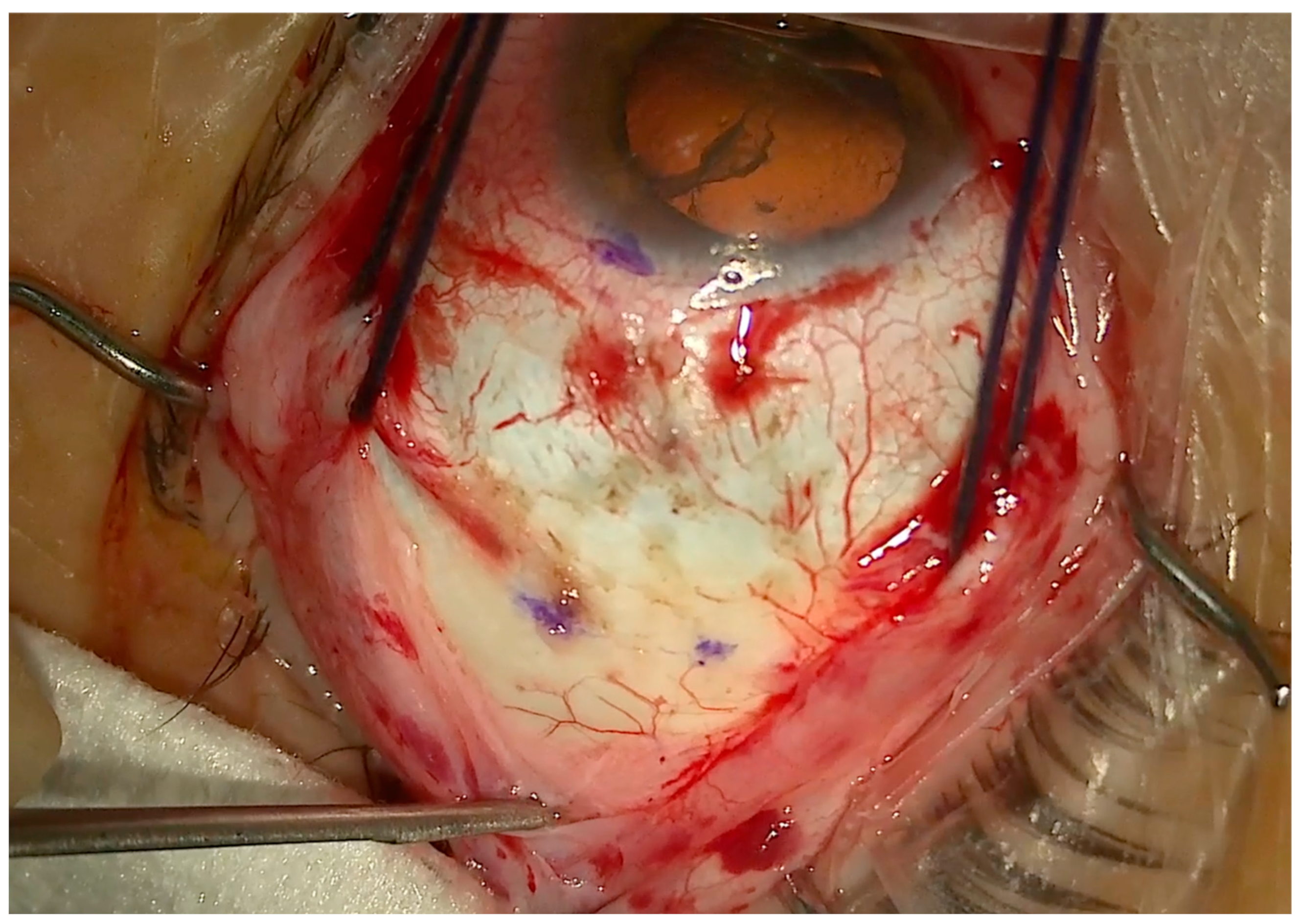
- Determining the DLN. The suture placement is the most important step of the whole surgery. The distance from limbus–needle (DLN) is marked to indicate where to enter with the needle to place the anterior superior and temporal sutures (Figure 4). Three points are marked with a caliper and staining, ideally marking the three corners of a triangle, with the apex at the limbus. The limbal point is marked at the 2:30 position in the left eye and at the 10:30 position in the right eye. The superior and temporal DLN points are marked according to the nomogram (described below).
- 4.
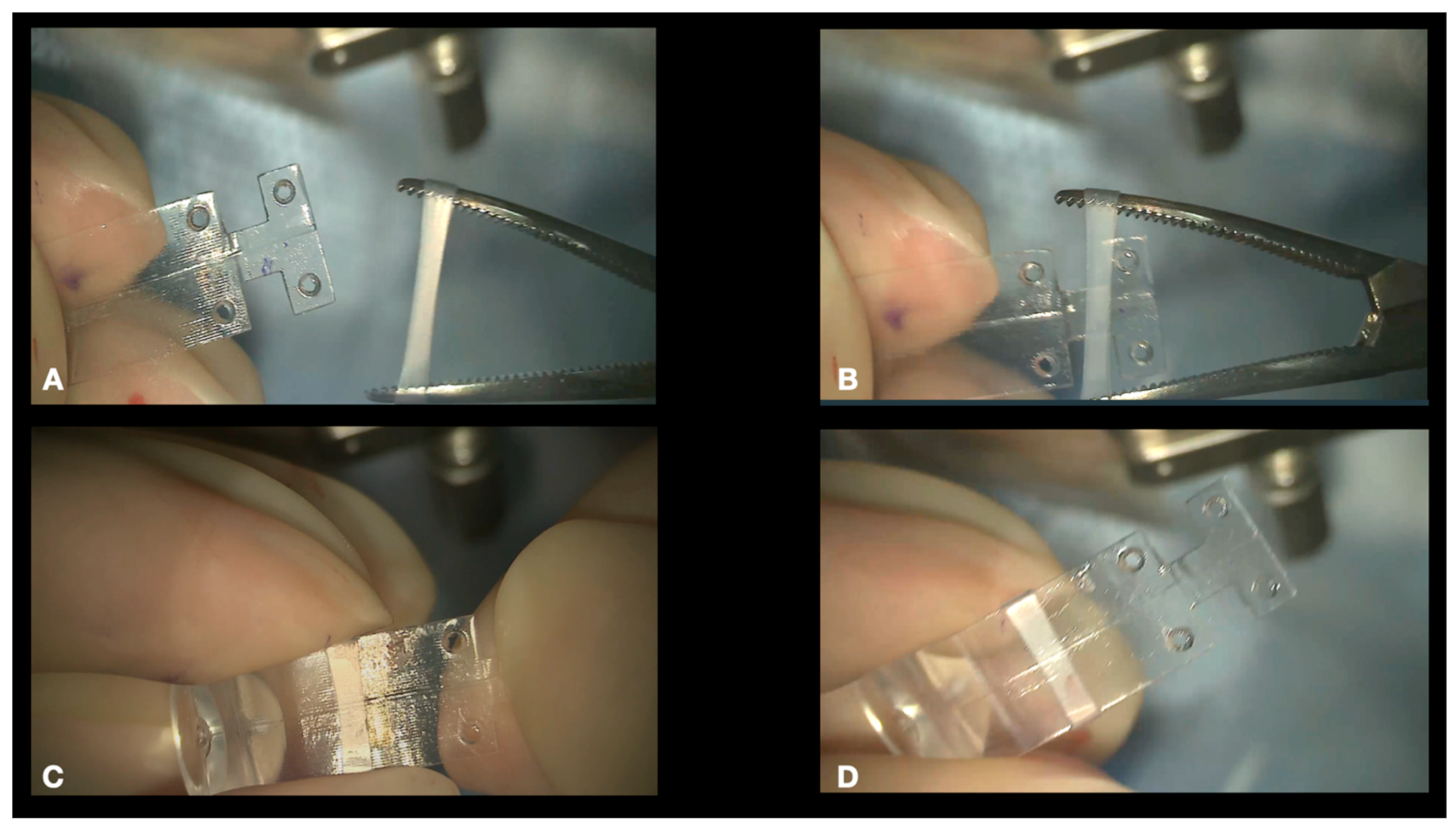
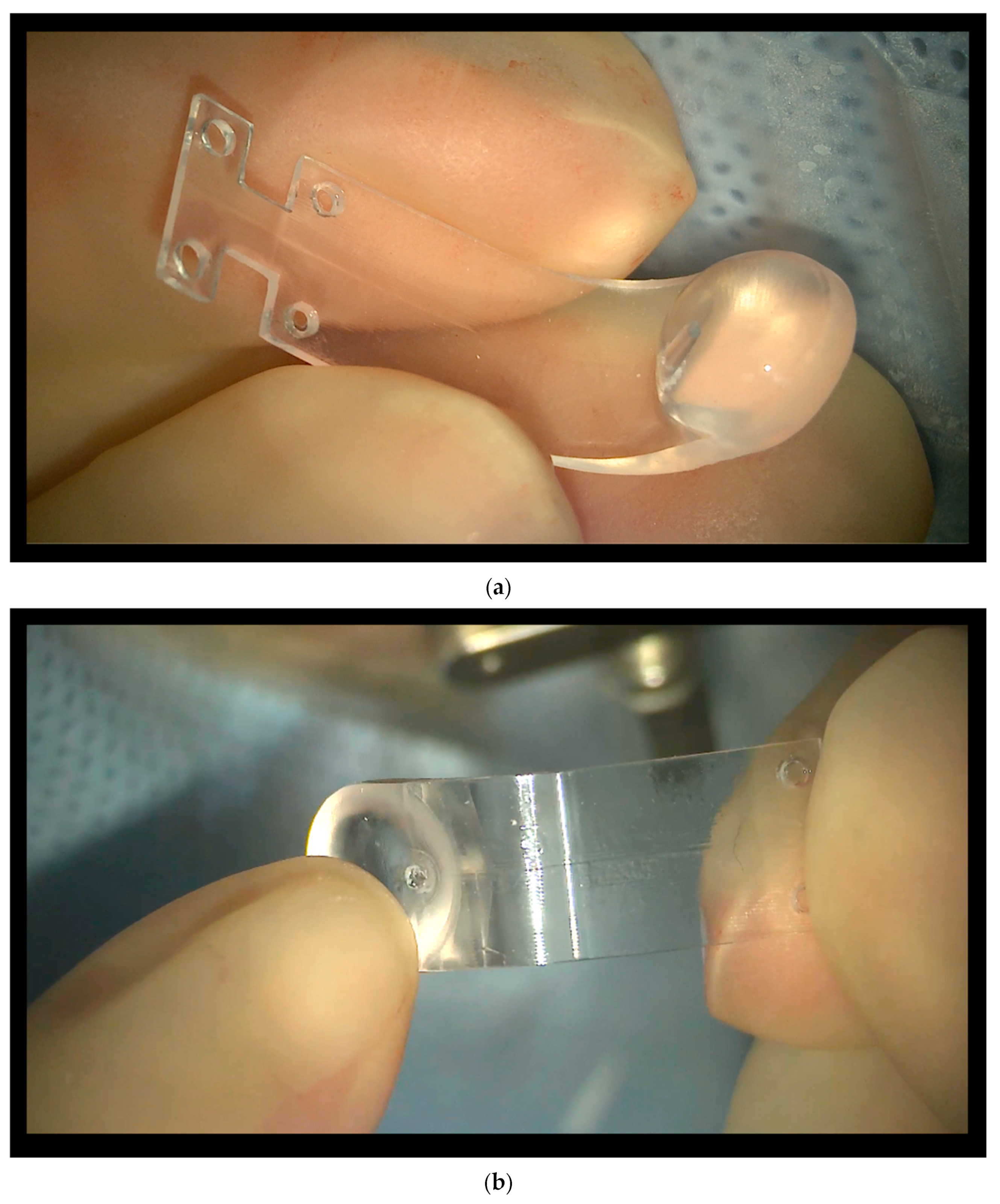
- Preparing the NPB. The NPB can be inserted into the superotemporal quadrant without any preparation. The maneuvers which are described in step 4 are not indispensable but useful to make the procedure easier and safer. Both maneuvers require the use of a silicone sleeve, which is provided with the NPB package. The silicone sleeve can be easily positioned around the arm of the buckle, roughly in the middle of the length of the arm (Figure 5).
- a.
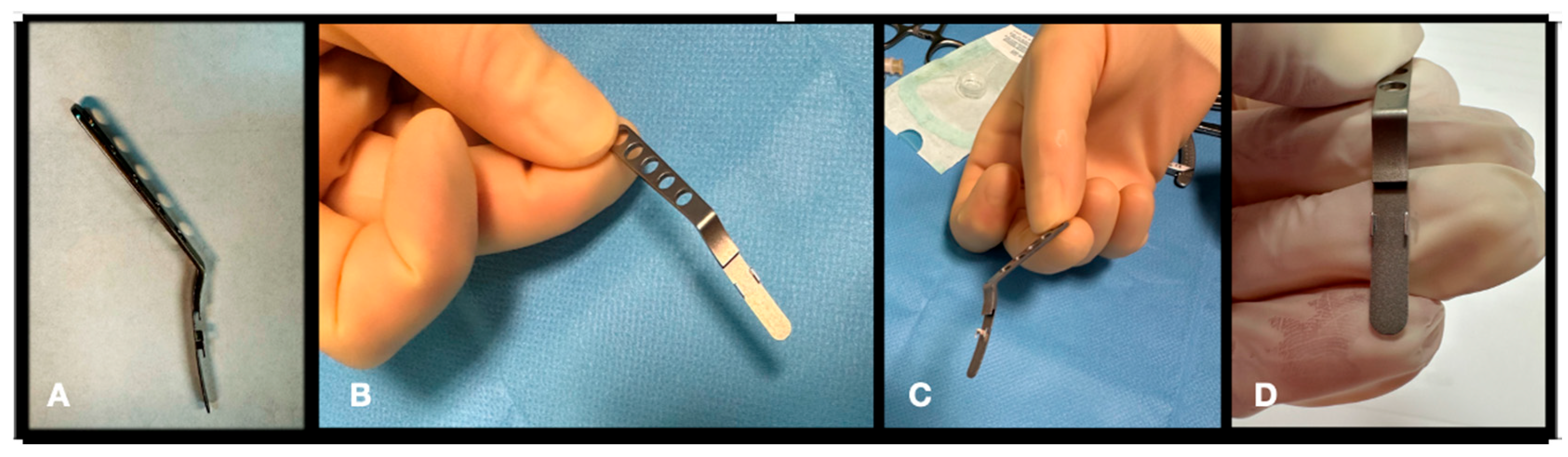
- Connecting the NPB on the NPD Loading device. We suggest connecting the NPB to the NPB loading device (Figure 6). As an alternative, the NPB can be held with bayoneted forceps, but attention should be taken not to break the NPB. To connect the NPB to the NPB loading device, it is necessary to execute the following steps:
- Hold the handle of the NPB loading device.
- Align the tip of the loading device to the external side of the NPB arm.
- Insert the tip of the loading device into the silicone sleeve with the help of non-toothed forceps.
- Connect the teeth of the loading device, embracing the NPB anterior wings.
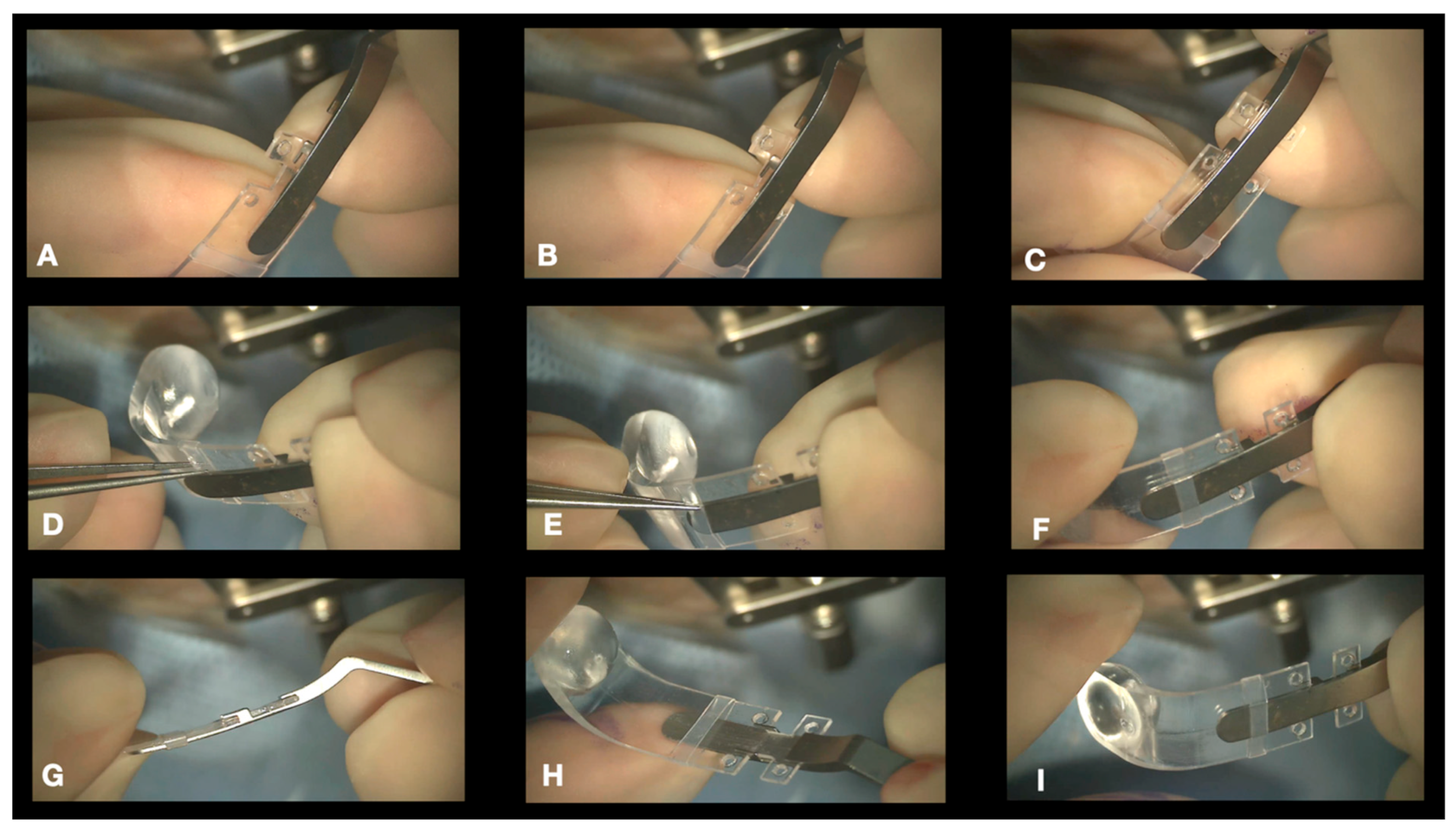
- b.
- Connecting the Illuminated Fiber to the NPB. A 25-, 27-, or 29-gauge illuminated fiber can be slid onto the external side of the arm through the silicone sleeve and finally inserted into a dedicated lodge under the head of the NPB (Figure 2b and Figure 7). The light helps with the transillumination function, but we observed that surgery can be performed without any light and using only the microscope view.
- 5.
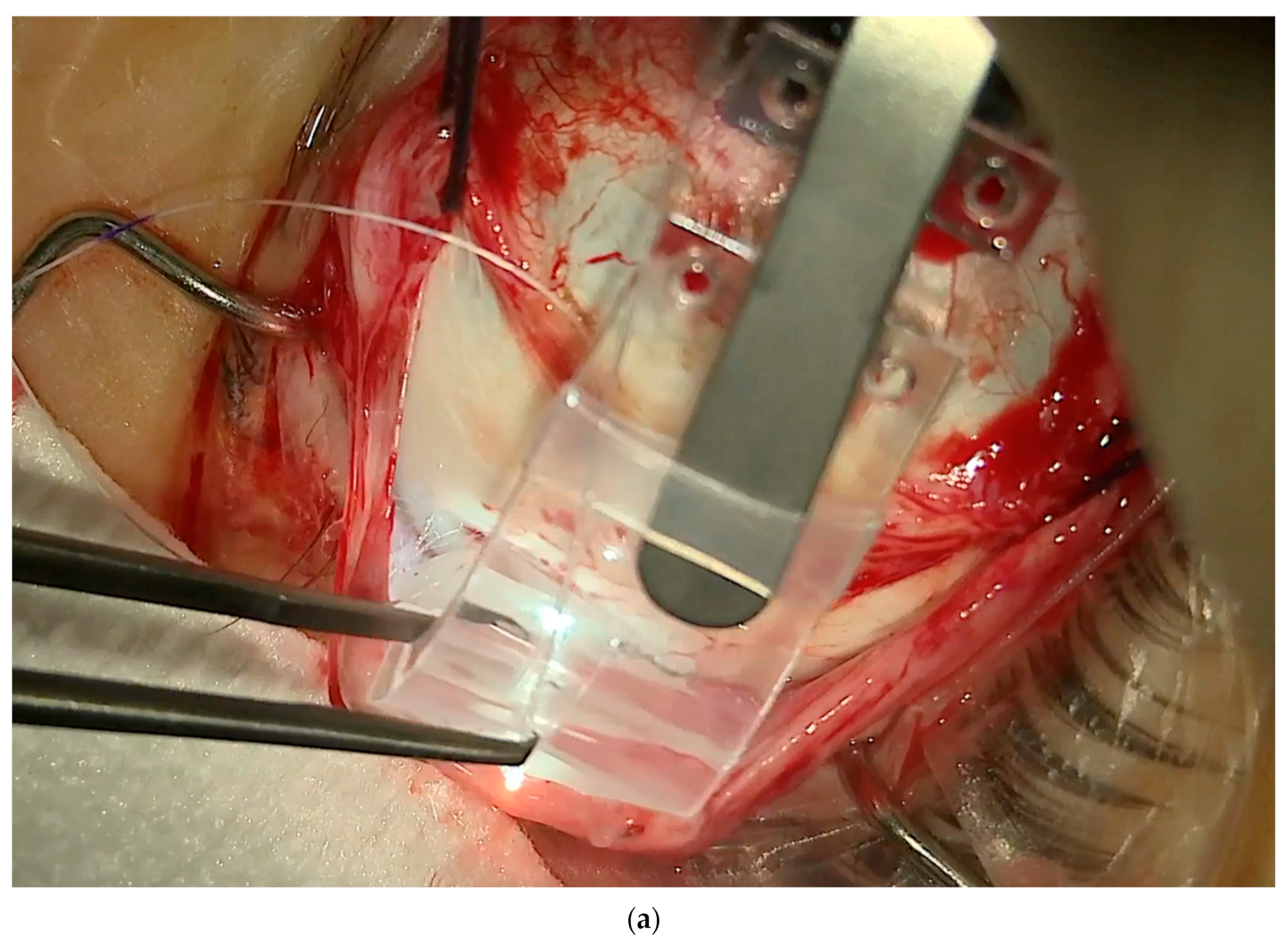
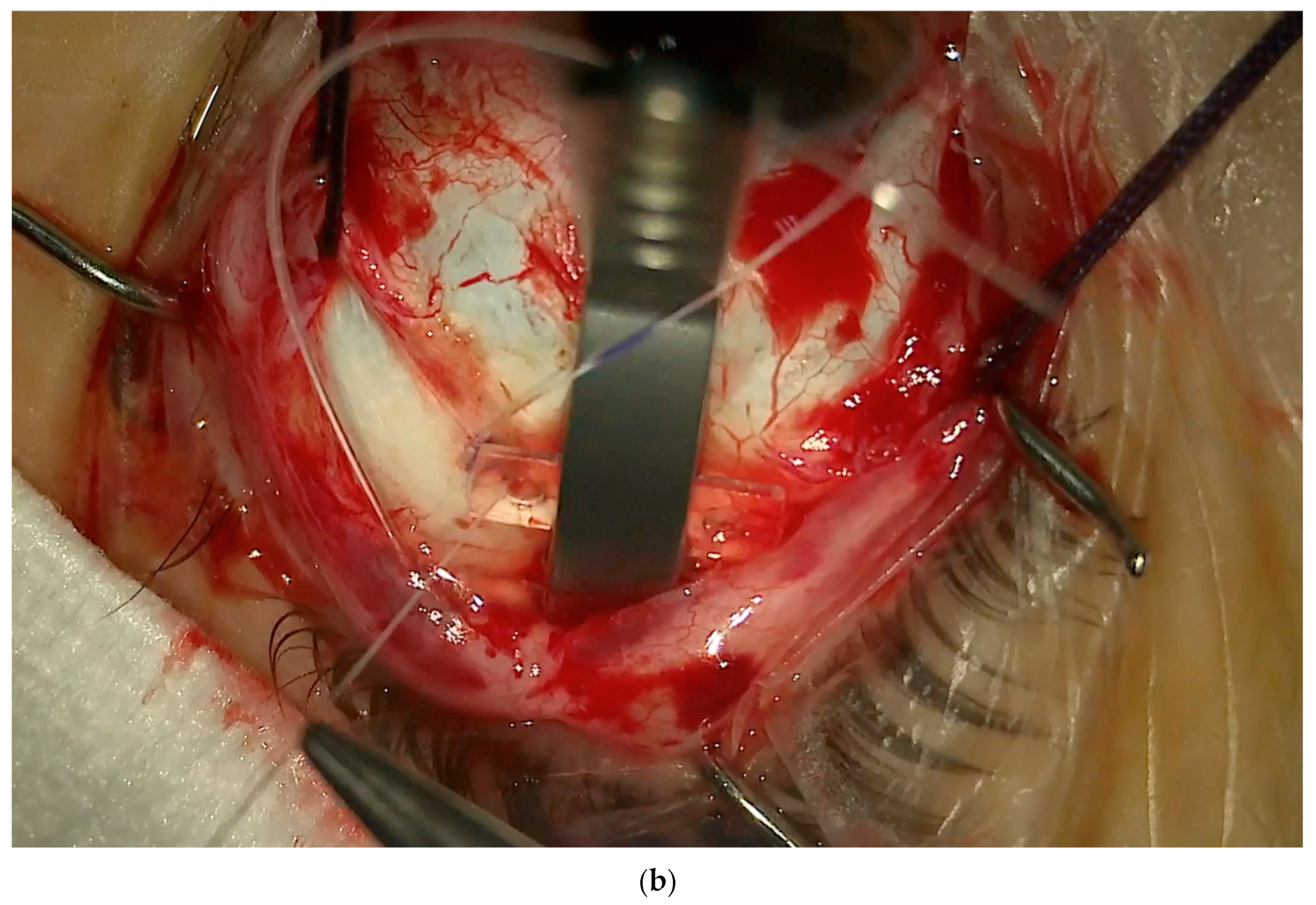
- Insertion of the NPB. The NPB is inserted into the superotemporal quadrant by gently sliding and pushing the head, with a rotational movement, first along the eyewall and finally toward and behind the posterior pole (Figure 8a,b). The head is placed under the macula.
- 6.
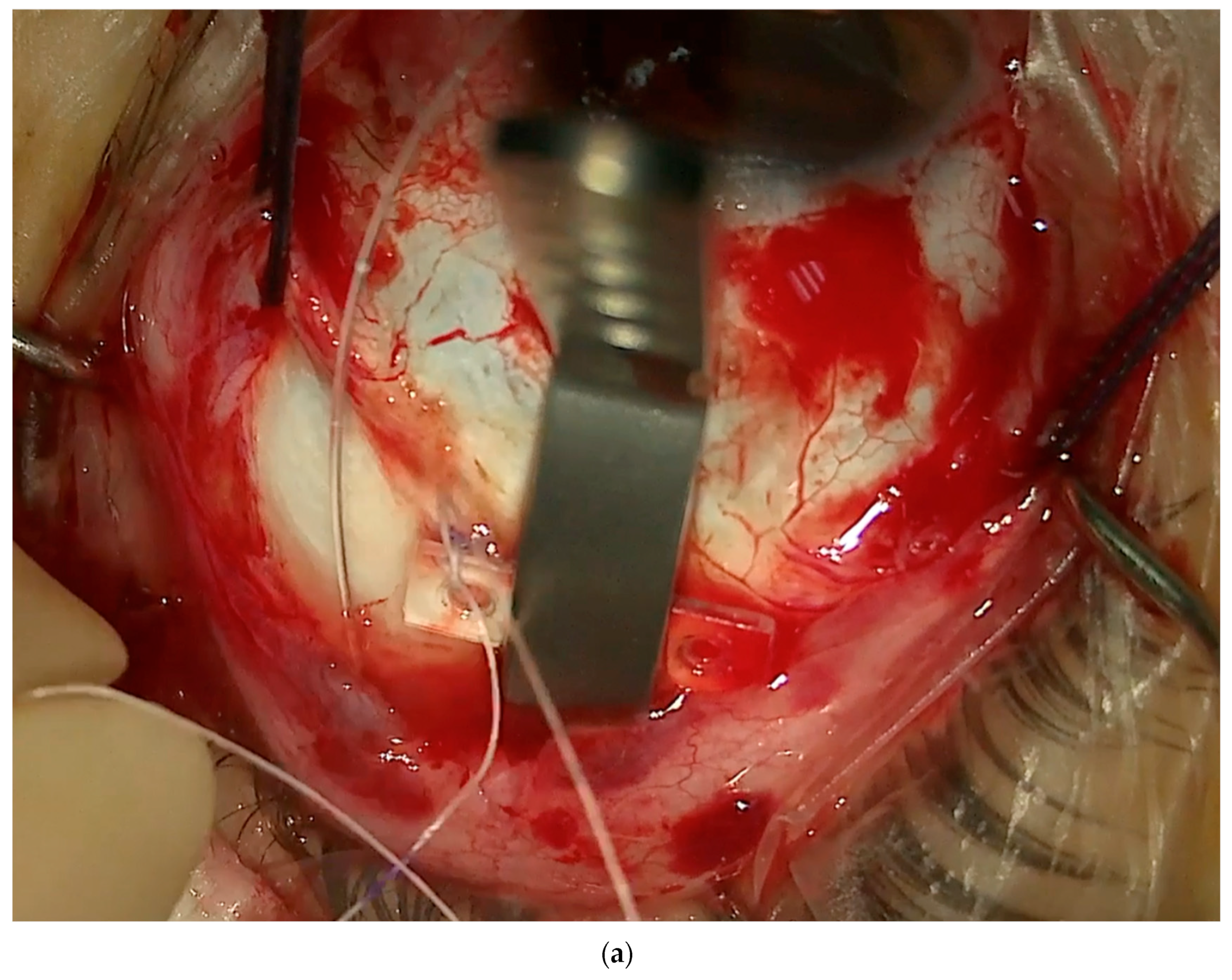
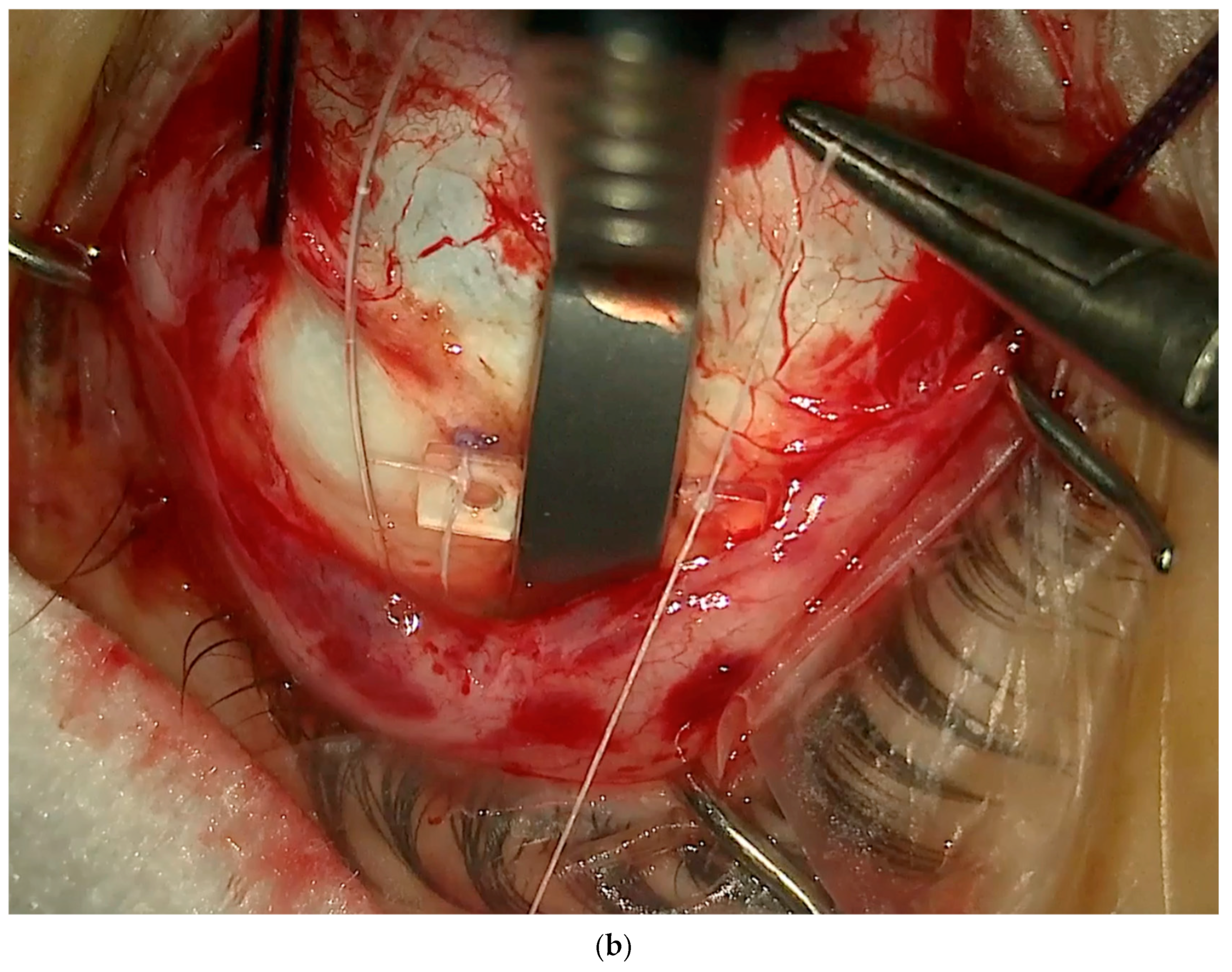
- Superior and Temporal Suture. The sutures are secured into the anterior holes of the NPB arm (Figure 9a,b).
- 7.
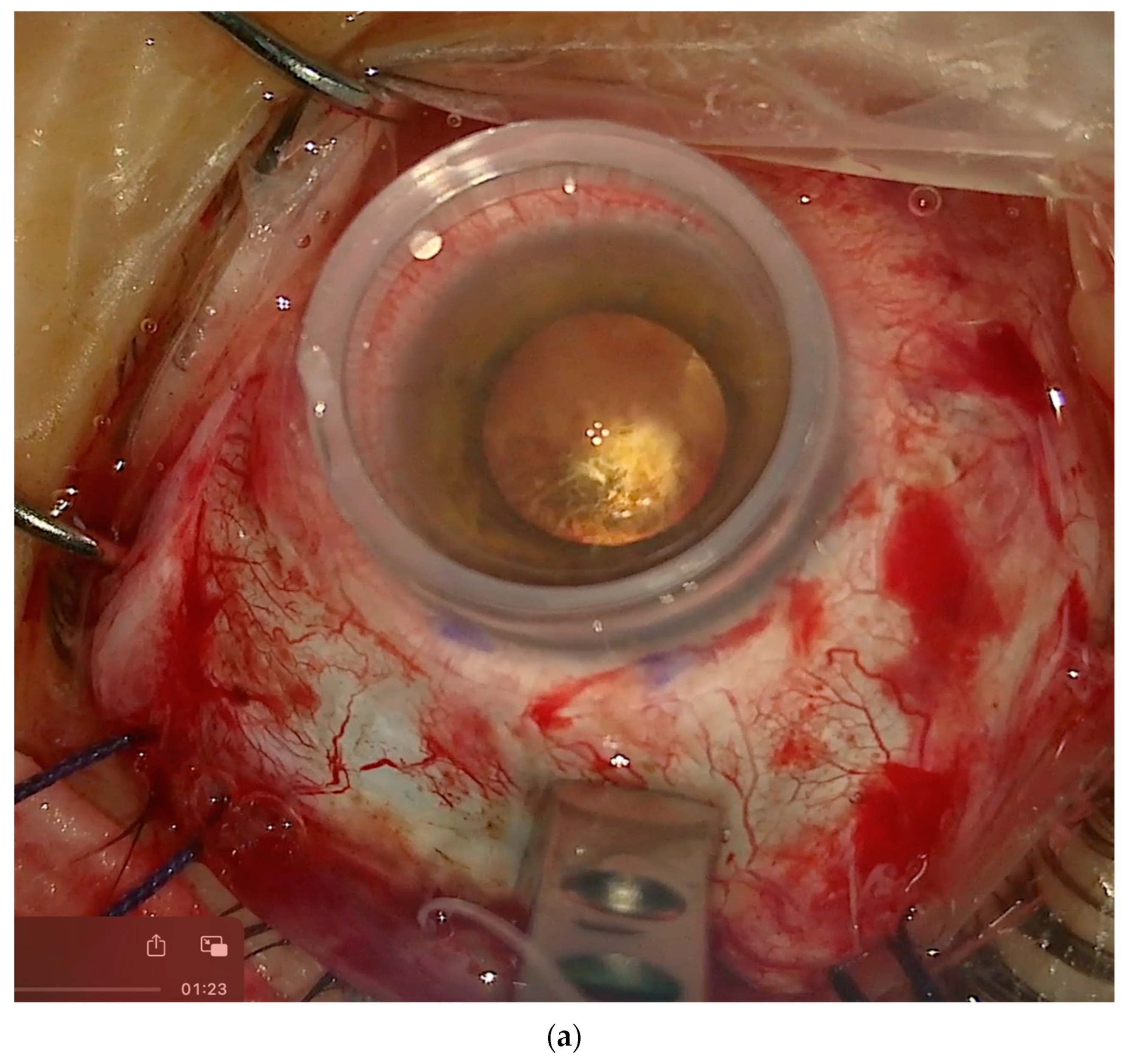
- Position Check. The position of the NPB is checked through the microscope by moving the NPB with the NPB loading device or with strong forceps (Figure 10a,b). If the location is correct, the surgeon can go to step 8; otherwise, the sutures should be adjusted until the buckle is well centered.
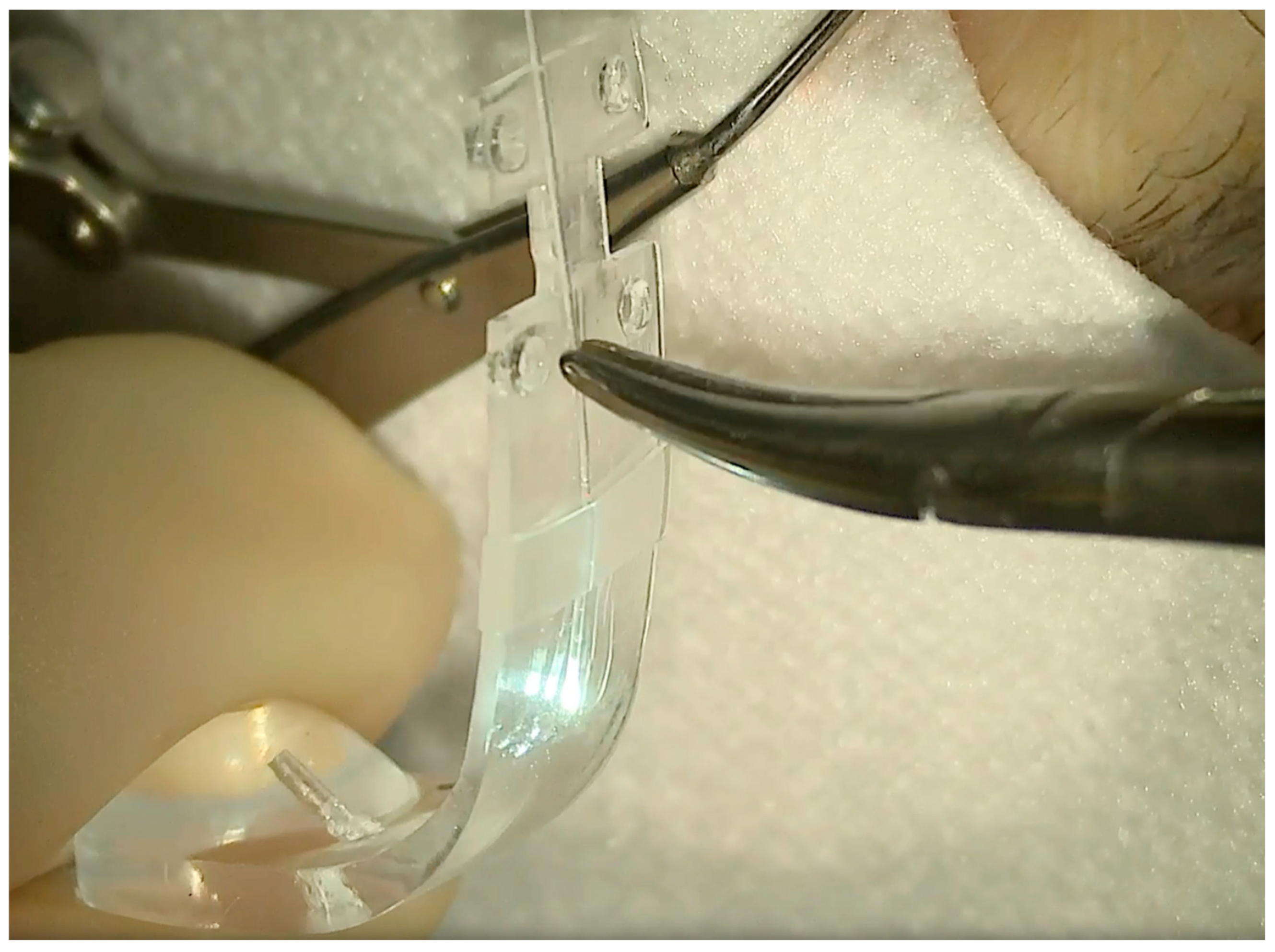
- 8.
- Disconnecting the NPB Loading Device From the NPB. If the NPB loading device was used, at the end of the procedure, it must be carefully disconnected from the NPB. We advise to keep the NPB’s most anterior wing steady with non-toothed forceps and to gently elevate it by 1mm and pull the NPB loading device out.
- 9.
- Ending the Procedure. The traction sutures around the muscles are removed, and the Tenon is dried and placed over the buckle, suturing one spot in the inferotemporal quadrant. Then, the conjunctiva is dried and placed with care over the buckle and the Tenon and sutured with reabsorbable sutures (Vycril 7/0). Ideally, one suture is placed at the level of the superonasal peritomy and three sutures are placed at the inferoteporal radial peritomy.
3. Viewing the Maneuvers
4. Nomogram
4.1. Further Notes on The Technique
4.2. Complications of Macular Buckle and How to Avoid Them
- Superficial extrusion of the lateral arm of the macular buckle (5%), which manifests as a late complication, from 6 months to years postoperatively.
- ○
- Tips to avoid it: Keep an ideal position of the DLN of 11 mm or more by calculating the correct length of the NPB based on the axial length.
- Diplopia (5%), mostly in the form of hypotropia.
- ○
- Tips to avoid it: Advise the patient to move the eye in every direction while keeping the head still multiple times in the next two weeks after surgery. This helps to avoid fibrosis around the buckle in the orbit. Smaller NPBs are under study.
- Peripheral choroidal hemorrhage (0.5%), but only 0.05% were submacular.
- ○
- Tips to avoid it: Keep the IOP stable during surgery, avoiding paracentesis or opening of the vitreous chamber. Try to avoid multiple maneuvers over the sclera to insert the buckle. This will help to not stress the vortex veins with scleral massage.
5. Conclusions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Panozzo, G.; Mercanti, A. Optical coherence tomography findings in myopic traction maculopathy. Arch. Ophthalmol. 2004, 122, 1455–1460. [Google Scholar] [CrossRef] [PubMed]
- Baba, T.; Ohno-Matsui, K.; Futagami, S.; Yoshida, T.; Yasuzumi, K.; Kojima, A.; Tokoro, T.; Mochizuki, M. Prevalence and characteristics of foveal retinal detachment without macular hole in high myopia. Am. J. Ophthalmol. 2003, 135, 338–342. Available online: http://www.ncbi.nlm.nih.gov/pubmed/12614751 (accessed on 5 April 2015). [CrossRef] [PubMed]
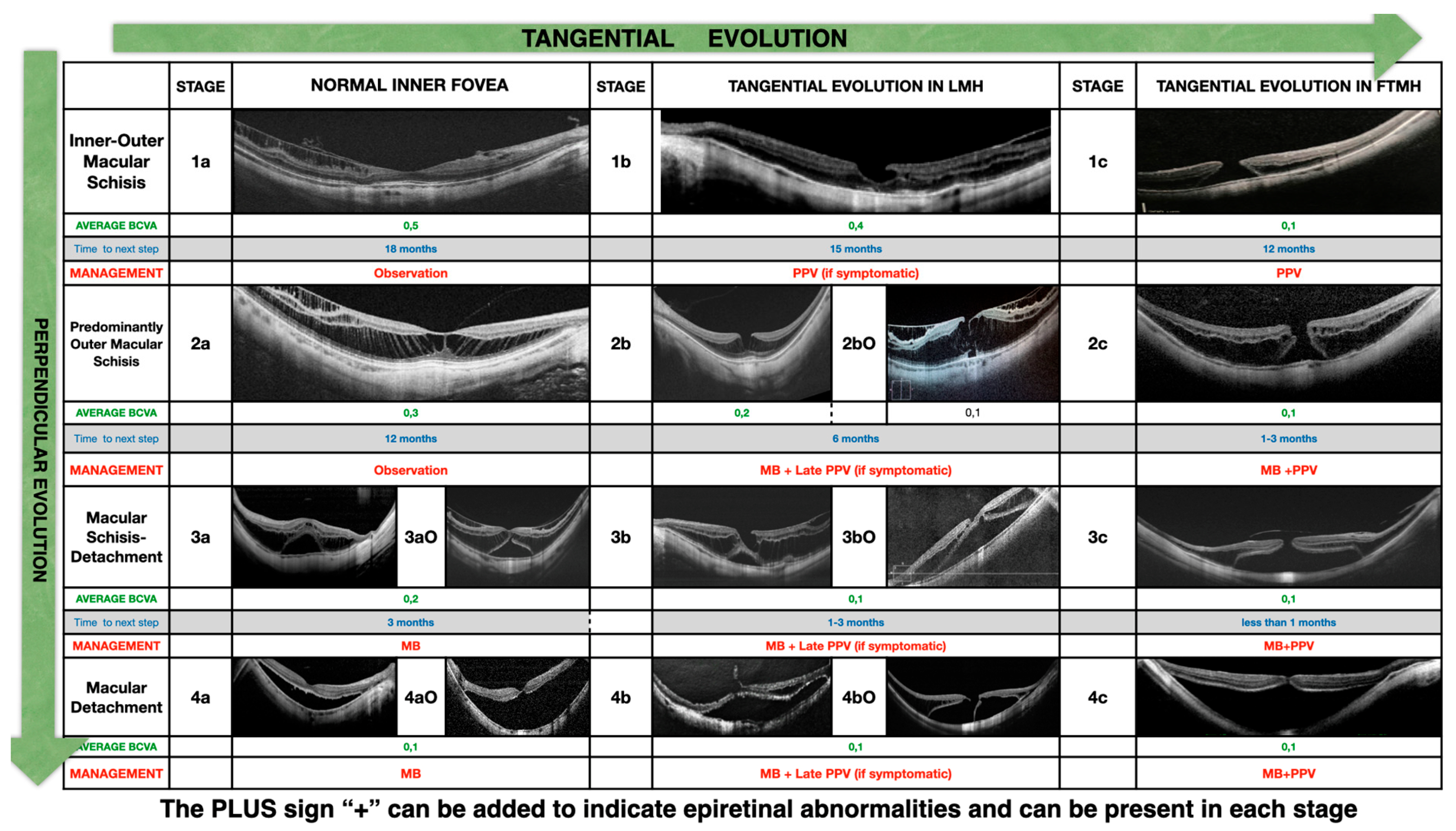
- Parolini, B.; Palmieri, M.; Finzi, A.; Besozzi, G.; Lucente, A.; Nava, U.; Pinackatt, S.; Adelman, R.; Frisina, R. The new Myopic Traction Maculopathy Staging System. Eur. J. Ophthalmol. 2021, 31, 1299–1312. [Google Scholar] [CrossRef] [PubMed]
- Parolini, B.; Arevalo, J.F.; Hassan, T.; Kaiser, P.; Rezaei, K.A.; Singh, R.; Sakamoto, T.; Rocha, J.; Frisina, R. International Validation of Myopic Traction Maculopathy Staging System. Ophthalmic Surg. Lasers Imaging Retin. 2023, 54, 153–157. [Google Scholar] [CrossRef] [PubMed]
- Parolini, B.; Palmieri, M.; Finzi, A.; Frisina, R. Proposal for the management of myopic traction maculopathy based on the new MTM staging system. Eur. J. Ophthalmol. 2021, 31, 3265–3276. [Google Scholar] [CrossRef] [PubMed]
- Parolini, B.; Frisina, R.; Pinackatt, S.; Mete, M. A New L-Shaped Design of Macular Buckle to Support a Posterior Staphyloma in High Myopia. Retina 2013, 33, 1466–1470. [Google Scholar] [CrossRef] [PubMed]
- Parolini, B.; Frisina, R.; Pinackatt, S.; Gasparotti, R.; Gatti, E.; Baldi, A.; Penzani, R.; Lucente, A.; Semeraro, F. Indications and results of a new l-shaped macular buckle to support a posterior staphyloma in high myopia. Retina 2015, 35, 2469–2482. [Google Scholar] [CrossRef] [PubMed]
- Mateo, C.; Burés-Jelstrup, A. Macular buckling with ANDO PLOMBE may increase choroidal thickness and mimic serous retinal detachment seen in the tilted disk syndrome. Retin. Cases Brief. Rep. 2016, 10, 327–330. [Google Scholar] [CrossRef] [PubMed]
- Alkabes, M.; Mateo, C. Macular buckle technique in myopic traction maculopathy: A 16-year review of the literature and a comparison with vitreous surgery. Graefe’s Arch. Clin. Exp. Ophthalmol. 2018, 256, 863–877. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, T.; Ando, F.U. Episcleral macular buckling by semirigid shaped-rod exoplant for recurrent retinal detachment with macular hole in highly myopic eyes. Retina 2005, 25, 147–151. [Google Scholar] [CrossRef] [PubMed]
- Stirpe, M.; Ripandelli, G.; Rossi, T.; Cacciamani, A.; Orciuolo, M. A new adjustable macular buckle designed for highly myopic eyes. Retina 2012, 32, 1424–1427. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.C.; Sheu, J.J.; Chen, Y.H.; Chen, Y.J.; Chen, C.H.; Lee, J.J.; Huang, C.L.; Chen, C.T.; Kuo, H.K. Gore-tex vascular graft for macular buckling in high myopia eyes. Retina 2017, 37, 1263–1269. [Google Scholar] [CrossRef] [PubMed]
- Ripa, M.; Motta, L.; Matello, V.; Frisina, R.; Parolini, B. Long-Term results of macular buckle for MTM stage 3–4 With maculoschisis and macular detachment without and with lamellar macular hole. Eur. J. Ophthalmol. 2024, 11206721241234958. [Google Scholar] [CrossRef] [PubMed]
- Parolini, B.; Padrón, J.F.R.; Lopes, E.; Matello, V.; Crincoli, E. Evaluation of macular atrophy in patients treated with macular buckle for myopic traction maculopathy (MTM): Mid and long-term follow-up. Retina 2022, 44, 1180–1187. [Google Scholar] [CrossRef] [PubMed]
- Kortuem, F.C.; Ziemssen, F.; Neubauer, J.; Bartz-Schmidt, K.U.; Dimopoulos, S. Introducing a customized low-cost macular buckle. Retina 2022, 10–1097. [Google Scholar] [CrossRef] [PubMed]
- Akduman, L. A titanium macular buckle implant designed for an easy placement in myopic macular holes. Retin. Cases Brief Rep. 2024, 18, 173–176. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| AL Pre | Superior DLN | Temporal DLN |
|---|---|---|
| 28.06 | 11.00 | 9.00 |
| 28.61 | 10.00 | 9.00 |
| 29.02 | 11.50 | 9.00 |
| 29.23 | 12.00 | 8.00 |
| 29.37 | 9.50 | 9.00 |
| 29.6 | 9.50 | 9.00 |
| 29.78 | 10.00 | 10.00 |
| 30.03 | 12.00 | 9.00 |
| 30.09 | 11.50 | 10.00 |
| 30.36 | 12.00 | 11.00 |
| 30.62 | 10.00 | 8.50 |
| 30.78 | 11.50 | 9.00 |
| 30.85 | 11.50 | 10.50 |
| 31.03 | 11.00 | 10.50 |
| 31.17 | 12.00 | 10.00 |
| 31.49 | 12.00 | 11.00 |
| 31.52 | 11.50 | 11.50 |
| 31.55 | 12.50 | 12.00 |
| 31.50 | 12.50 | 11.00 |
| 31.62 | 11.50 | 11.50 |
| 31.81 | 12.00 | 10.00 |
| 31.90 | 13.00 | 12.50 |
| 31.18 | 13.50 | 12.00 |
| 32.81 | 13.00 | 13.00 |
| 32.91 | 13.50 | 13.00 |
| 33.89 | 14.50 | 14.00 |
| 34.31 | 14.00 | 14.00 |
| 34.49 | 15.00 | 14.00 |
| 34.51 | 14.00 | 14.00 |
| 34.85 | 14.00 | 12.50 |
| 35.39 | 15.00 | 14.00 |
| 35.65 | 16.50 | 15.00 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parolini, B. A New Model of a Macular Buckle and a Refined Surgical Technique for the Treatment of Myopic Traction Maculopathy. Vision 2024, 8, 42. https://doi.org/10.3390/vision8030042
Parolini B. A New Model of a Macular Buckle and a Refined Surgical Technique for the Treatment of Myopic Traction Maculopathy. Vision. 2024; 8(3):42. https://doi.org/10.3390/vision8030042
Chicago/Turabian StyleParolini, Barbara. 2024. "A New Model of a Macular Buckle and a Refined Surgical Technique for the Treatment of Myopic Traction Maculopathy" Vision 8, no. 3: 42. https://doi.org/10.3390/vision8030042
APA StyleParolini, B. (2024). A New Model of a Macular Buckle and a Refined Surgical Technique for the Treatment of Myopic Traction Maculopathy. Vision, 8(3), 42. https://doi.org/10.3390/vision8030042