Identifying Meibomian Gland Dysfunction Biomarkers in a Cohort of Patients Affected by DM Type II

 , ,
, ,  ,
,
Abstract
1. Introduction
2. Material and Methods
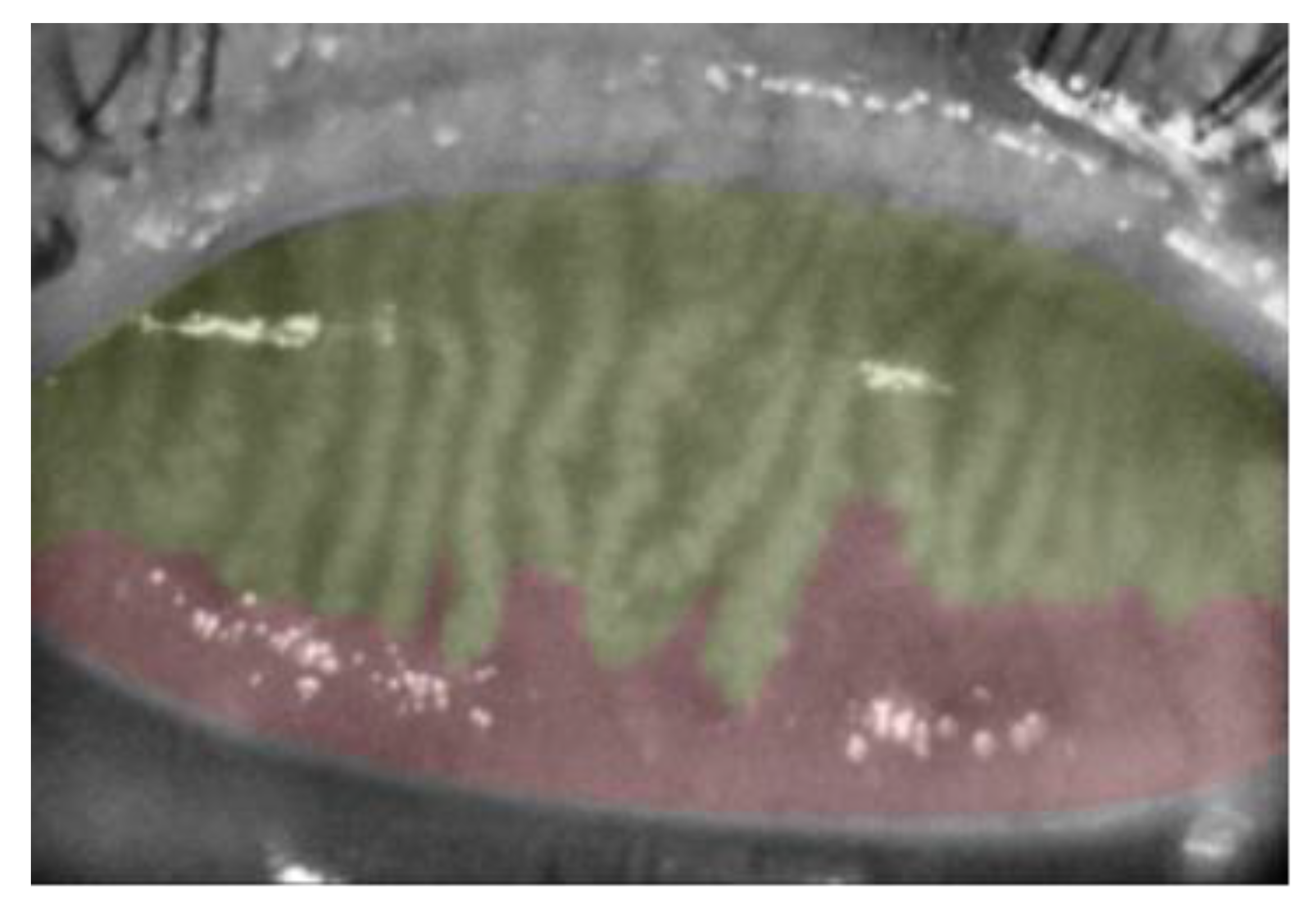
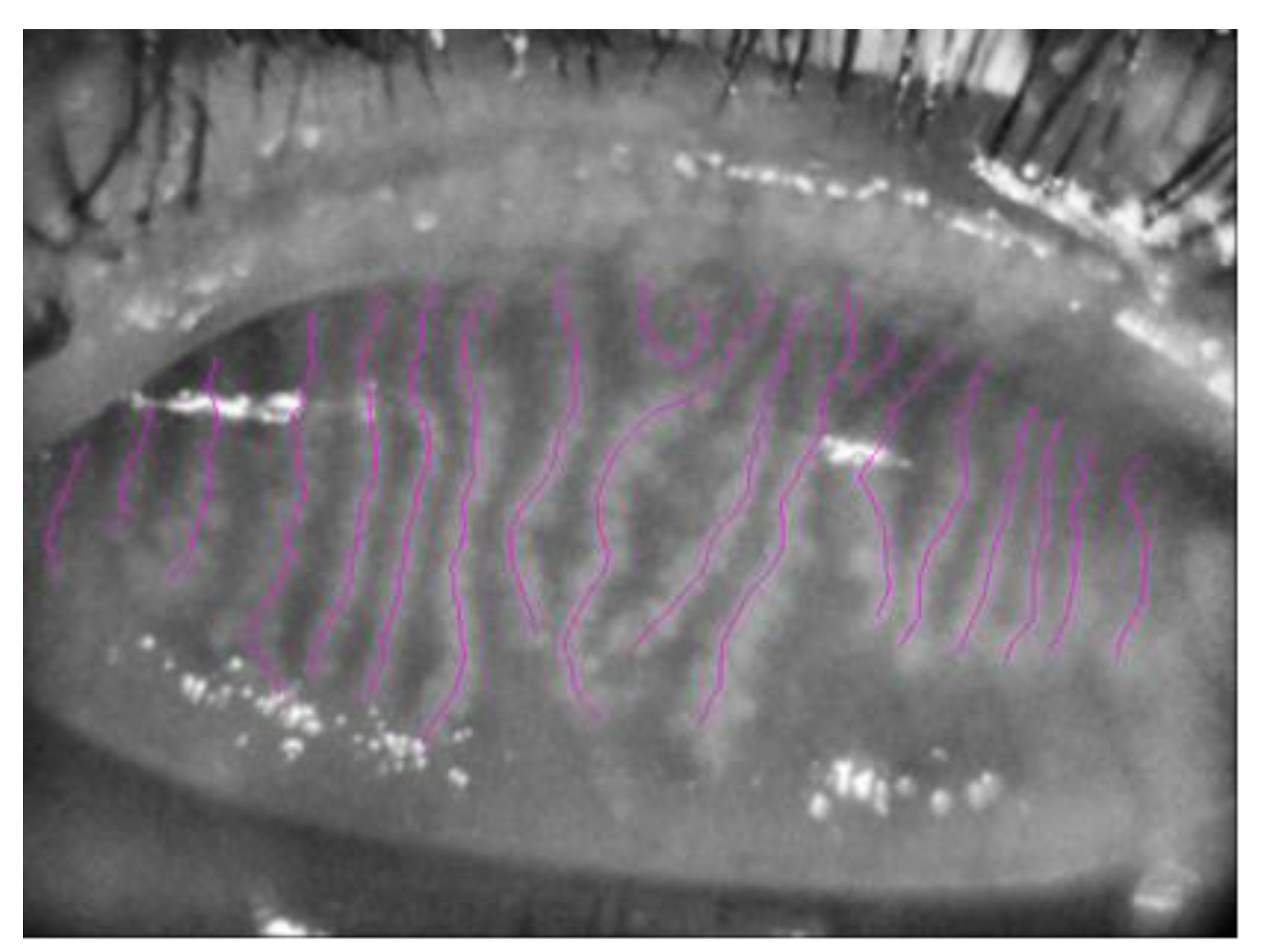
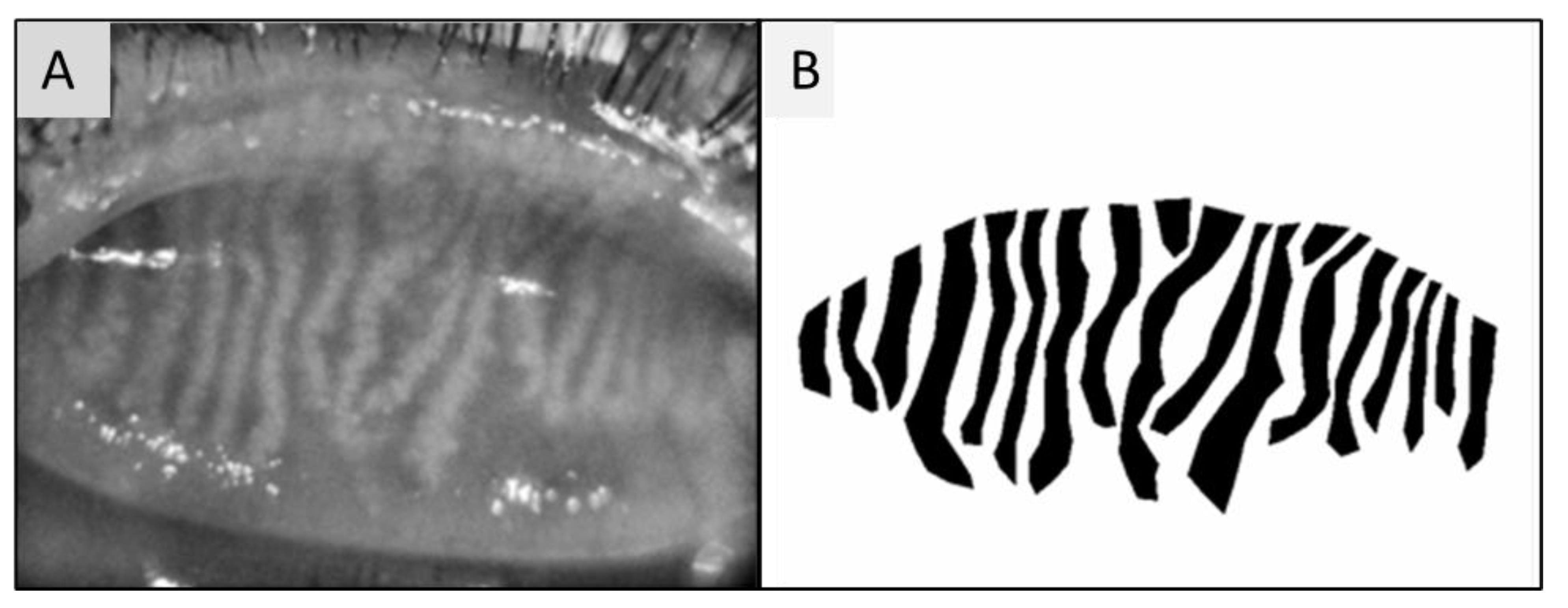
2.1. Image Analysis
2.2. Statistical Analysis
3. Results
3.1. Blood Biomarkers
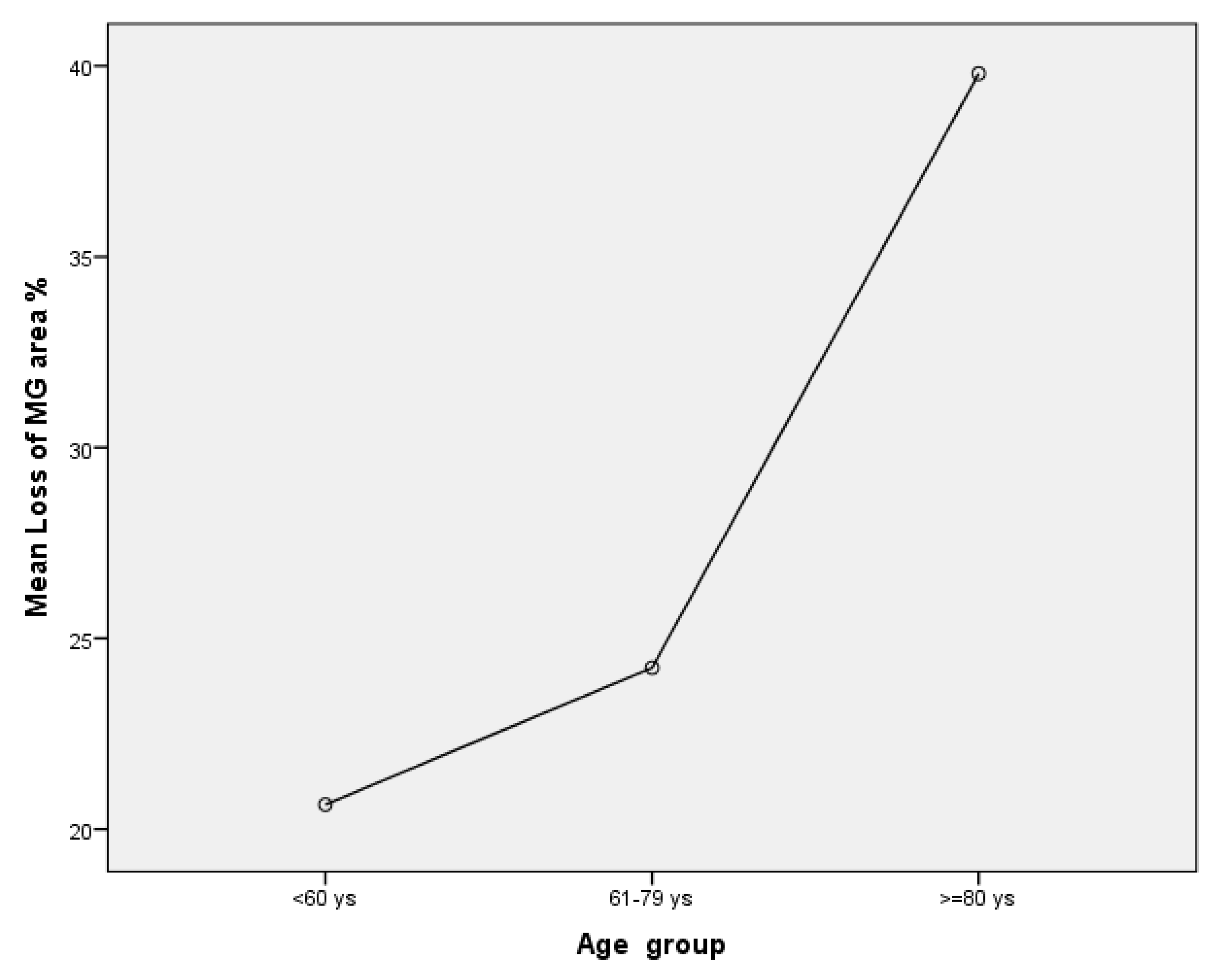
3.2. Meibography Analysis
4. Discussion and Conclusions
4.1. Role of Age and Diabetes
4.2. Hormones Role
4.3. Blood Lipid Levels BMI and Role
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tiffany, J.M. Physiological Functions of the Meibomian Glands. Prog Retinal Eye Res. 1995, 14, 47–74. [Google Scholar] [CrossRef]
- Rolando, M.; Merayo-Lloves, J. Management Strategies for Evaporative Dry Eye Disease and Future Perspective. Curr. Eye Res. 2022, 47, 813–823. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, D.A.; Sullivan, B.D.; Evans, J.E.; Schirra, F.; Yamagami, H.; Liu, M.; Richards, S.M.; Suzuki, T.; Schaumberg, D.A.; Sullivan, R.M.; et al. Androgen Deficiency, Meibomian Gland Dysfunction, and Evaporative Dry Eye. Ann. N. Y. Acad. Sci. 2002, 966, 211–222. [Google Scholar] [CrossRef]
- Bu, J.; Wu, Y.; Cai, X.; Jiang, N.; Jeyalatha, M.V.; Yu, J.; He, X.; He, H.; Guo, Y.; Zhang, M.; et al. Hyperlipidemia induces meibomian gland dysfunction. Ocul. Surf. 2019, 17, 777–786. [Google Scholar] [CrossRef] [PubMed]
- Ding, J.; Liu, Y.; A Sullivan, D. Effects of Insulin and High Glucose on Human Meibomian Gland Epithelial Cells. Investig. Opthalmology Vis. Sci. 2015, 56, 7814–7820. [Google Scholar] [CrossRef] [PubMed]
- Yoo, T.K.; Oh, E. Diabetes mellitus is associated with dry eye syndrome: A meta-analysis. Int. Ophthalmol. 2019, 39, 2611–2620. [Google Scholar] [CrossRef]
- Botion, L.M.; Green, A. Long-term regulation of lipolysis and hormone-sensitive lipase by insulin and glucose. Diabetes 1999, 48, 1691–1697. [Google Scholar] [CrossRef]
- Wei, Y.; Asbell, P.A. The Core Mechanism of Dry Eye Disease Is Inflammation. Eye Contact Lens: Sci. Clin. Pr. 2014, 40, 248–256. [Google Scholar] [CrossRef]
- Kang, M.H.; Kim, M.K.; Lee, H.J.; Lee, H.I.; Wee, W.R.; Lee, J.H. Interleukin-17 in Various Ocular Surface Inflammatory Diseases. J. Korean Med Sci. 2011, 26, 938–944. [Google Scholar] [CrossRef]
- Acera, A.; Rocha, G.; Vecino, E.; Lema, I.; Durán, J.A. Inflammatory Markers in the Tears of Patients with Ocular Surface Disease. Ophthalmic Res. 2008, 40, 315–321. [Google Scholar] [CrossRef]
- Schiffman, R.M.; Christianson, M.D.; Jacobsen, G.; Hirsch, J.D.; Reis, B.L. Reliability and Validity of the Ocular Surface Disease Index. Arch. Ophthalmol. 2000, 118, 615–621. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, M.; Kutsuna, M.; Uno, T.; Zheng, X.; Kodama, T.; Ohashi, Y. Marx Line: Fluorescein Staining Line on the Inner Lid as Indicator of Meibomian Gland Function. Am. J. Ophthalmol. 2006, 141, 669–669.e8. [Google Scholar] [CrossRef] [PubMed]
- van Bijsterveld, O.P. Diagnostic Tests in the Sicca Syndrome. Arch. Ophthalmol. 1969, 82, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Yanoff, M.; Duker, J.S. (Eds.) Ophthalmology: ExpertConsult.Com, 4th ed.; Elsevier Saunders: Philadelphia, PA, USA, 2014; ISBN 978-1-4557-3984-4. [Google Scholar]
- Pult, H.; Riede-Pult, B. Comparison of subjective grading and objective assessment in meibography. Contact Lens Anterior Eye 2013, 36, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Müller, R.T.; Abedi, F.; Cruzat, A.; Witkin, D.; Baniasadi, N.; Cavalcanti, B.; Jamali, A.; Chodosh, J.; Dana, R.; Pavan-Langston, D.; et al. Degeneration and Regeneration of Subbasal Corneal Nerves after Infectious Keratitis. Ophthalmology 2015, 122, 2200–2209. [Google Scholar] [CrossRef]
- Setu, A.K.; Horstmann, J.; Schmidt, S.; Stern, M.E.; Steven, P. Deep learning-based automatic meibomian gland segmentation and morphology assessment in infrared meibography. Sci. Rep. 2021, 11, 7649. [Google Scholar] [CrossRef]
- Den, S.; Shimizu, K.; Ikeda, T.; Tsubota, K.; Shimmura, S.; Shimazaki, J. Association Between Meibomian Gland Changes and Aging, Sex, or Tear Function. Cornea 2006, 25, 651–655. [Google Scholar] [CrossRef]
- Nien, C.J.; Massei, S.; Lin, G.; Nabavi, C.; Tao, J.; Brown, D.J.; Paugh, J.R.; Jester, J.V. Effects of age and dysfunction on human meibomian glands. JAMA Ophthalmol 2011, 129, 462–469. [Google Scholar] [CrossRef]
- Hashemi, H.; Asharlous, A.; Aghamirsalim, M.; Yekta, A.; Pourmatin, R.; Sajjadi, M.; Pakbin, M.; Asadollahi, M.; Khabazkhoob, M. Meibomian gland dysfunction in geriatric population: Tehran geriatric eye study. Int. Ophthalmol. 2021, 41, 2539–2546. [Google Scholar] [CrossRef]
- Hykin, P.G.; Bron, A.J. Age-Related Morphological Changes in Lid Margin and Meibomian Gland Anatomy. Cornea 1992, 11, 334–342. [Google Scholar] [CrossRef]
- Yu, T.; Shi, W.-Y.; Song, A.-P.; Gao, Y.; Dang, G.-F.; Ding, G. Changes of meibomian glands in patients with type 2 diabetes mellitus. Int. J. Ophthalmol. 2016, 9, 1740–1744. [Google Scholar] [CrossRef] [PubMed]
- Fan, F.; Li, X.; Li, K.; Jia, Z. To Find Out the Relationship Between Levels of Glycosylated Hemoglobin with Meibomian Gland Dysfunction in Patients with Type 2 Diabetes. Ther. Clin. Risk Manag. 2021, 17, 797–807. [Google Scholar] [CrossRef]
- Abu, E.K.; O Ofori, A.; Boadi-Kusi, S.B.; Ocansey, S.; Yankah, R.K.; Kyei, S.; Awuku, A.Y. Dry eye disease and meibomian gland dysfunction among a clinical sample of type 2 diabetes patients in Ghana. Afr. Heal. Sci. 2022, 22, 293–302. [Google Scholar] [CrossRef] [PubMed]
- Lin, X.; Xu, B.; Zheng, Y.; Coursey, T.G.; Zhao, Y.; Li, J.; Fu, Y.; Chen, X.; Zhao, Y.-E. Meibomian Gland Dysfunction in Type 2 Diabetic Patients. J. Ophthalmol. 2017, 2017, 3047867. [Google Scholar] [CrossRef] [PubMed]
- Yu, T.; Han, X.-G.; Gao, Y.; Song, A.-P.; Dang, G.-F. Morphological and cytological changes of meibomian glands in patients with type 2 diabetes mellitus. Int. J. Ophthalmol. 2019, 12, 1415–1419. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Fang, X.; Luo, S.; Shang, X.; Xie, Z.; Dong, N.; Xiao, X.; Lin, Z.; Liu, Z. Meibomian Glands and Tear Film Findings in Type 2 Diabetic Patients: A Cross-Sectional Study. Front. Med. 2022, 9, 762493. [Google Scholar] [CrossRef]
- Arunachalam, C.; Shamsheer, R. A clinical study of meibomian gland dysfunction in patients with diabetes. Middle East Afr. J. Ophthalmol. 2015, 22, 462–466. [Google Scholar] [CrossRef]
- A Sullivan, D.; Sullivan, B.D.; Ullman, M.D.; Rocha, E.; Krenzer, K.L.; Cermak, J.M.; Toda, I.; Doane, M.G.; E Evans, J.; A Wickham, L. Androgen influence on the meibomian gland. Investig. Opthalmology Vis. Sci. 2000, 41, 3732–3742. [Google Scholar]
- Imperato-McGinley, J.; Gautier, T.; Cai, L.Q.; Yee, B.; Epstein, J.; Pochi, P. The androgen control of sebum production. Studies of subjects with dihydrotestosterone deficiency and complete androgen insensitivity. J. Clin. Endocrinol. Metab. 1993, 76, 524–528. [Google Scholar] [CrossRef]
- Wang, L.-X. Androgen and meibomian gland dysfunction: From basic molecular biology to clinical applications. Int. J. Ophthalmol. 2021, 14, 915–922. [Google Scholar] [CrossRef]
- Thody, A.J.; Shuster, S. Control and function of sebaceous glands. Physiol. Rev. 1989, 69, 383–416. [Google Scholar] [CrossRef]
- Krenzer, K.L.; Dana, M.R.; Ullman, M.D.; Cermak, J.M.; Tolls, D.B.; Evans, J.E.; Sullivan, D.A. Effect of Androgen Deficiency on the Human Meibomian Gland and Ocular Surface. J. Clin. Endocrinol. Metab. 2000, 85, 4874–4882. [Google Scholar] [CrossRef]
- Sullivan, B.D.; Evans, J.E.; Dana, M.R.; A Sullivan, D. Influence of Aging on the Polar and Neutral Lipid Profiles in Human Meibomian Gland Secretions. Arch. Ophthalmol. 2006, 124, 1286–1292. [Google Scholar] [CrossRef]
- Sullivan, B.D.; Evans, J.E.; Krenzer, K.L.; Dana, M.R.; Sullivan, D.A. Impact of Antiandrogen Treatment on the Fatty Acid Profile of Neutral Lipids in Human Meibomian Gland Secretions. J. Clin. Endocrinol. Metab. 2000, 85, 4866–4873. [Google Scholar] [CrossRef]
- Straub, R.H.; Konecna, L.; Hrach, S.; Rothe, G.; Kreutz, M.; Schölmerich, J.; Falk, W.; Lang, B. Serum Dehydroepiandrosterone (DHEA) and DHEA Sulfate Are Negatively Correlated with Serum Interleukin-6 (IL-6), and DHEA Inhibits IL-6 Secretion from Mononuclear Cells in Man in Vitro: Possible Link between Endocrinosenescence and Immunosenescence. J. Clin. Endocrinol. Metab. 1998, 83, 2012–2017. [Google Scholar] [CrossRef]
- Tsai, M.-H.; Huang, H.-C.; Peng, Y.-S.; Chen, Y.-C.; Tian, Y.-C.; Yang, C.-W.; Lien, J.-M.; Fang, J.-T.; Wu, C.-S.; Hsieh, S.-Y.; et al. Dehydroepiandrosterone sulfate and dehydroepiandrosterone sulfate/cortisol ratio in cirrhotic patients with septic shock: Another sign of hepatoadrenal syndrome? Crit. Care 2017, 21, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Kuriakose, R.K.; Braich, P.S. Dyslipidemia and its Association with Meibomian Gland Dysfunction: A Systematic Review. Int. Ophthalmol. 2018, 38, 1809–1816. [Google Scholar] [CrossRef] [PubMed]
- Butovich, I.A.; Suzuki, T. Delineating a novel metabolic high triglycerides-low waxes syndrome that affects lipid homeostasis in meibomian and sebaceous glands. Exp. Eye Res. 2020, 199, 108189. [Google Scholar] [CrossRef] [PubMed]
- Gupta, P.K.; Venkateswaran, N.; Heinke, J.; Stinnett, S.S. Association of meibomian gland architecture and body mass index in a pediatric population. Ocul. Surf. 2020, 18, 657–662. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.Y.; Liao, Y.; Huang, C.H.; Wang, S.; Liu, Z.G. Association between meibomian gland dysfunction and body mass index in Chinese adults. Zhonghua Yi Xue Za Zhi 2021, 101, 2514–2518. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Grade | Lower Lid Examination after Fluorescin Staining |
|---|---|
| 0 | ML runs along the conjunctival side of the Mos |
| 1 | Parts of the ML touch the Mos |
| 2 | ML runs through the Mos |
| 3 | ML runs along the skin side of the Mos |
| Number of patients/eyes | 18 |
| Age (years) | 67.76 ± 12.39 (32–81) |
| BMI (kg/m2) | 29.05 ± 4.52 (21–36) |
| Tear break-up time (s) | 2.94 ± 1.89 (0–7) |
| Schirmer test I (mm/5 min) | 7.94 ± 5.97 (0–18) |
| Schirmer test II (mm/5 min) | 5.29 ± 3.84 (0–14) |
| Marx line score | 3.8 ± 2.7 (0–9) |
| Vbs score | 1.29 ± 0.98 (0–3) |
| OSDI | 32.55 ± 28.57 (0–90) |
| β | T | p Value | |
|---|---|---|---|
| Glicemia (mg/dL) VS | |||
| Meibobian length (mm/mm2) | −0.043 | −0.087 | 0.933 |
| Meibomian area (mm2) | 0.097 | 0.254 | 0.805 |
| Meibomian width top (mm/mm2) | −0.218 | −0.309 | 0.764 |
| Meibomian width centre (mm/mm2) | 0.373 | 0.476 | 0.644 |
| Meibomian width low (mm/mm2) | 0.148 | 0.316 | 0.758 |
| Testosterone (nmol/L) VS | |||
| Meibomian length (mm/mm2) | −0.085 | −0.178 | 0.863 |
| Meibomian area (mm2) | 0.342 | 0.861 | 0.410 |
| Meibomian width top (mm/mm2) | −0.011 | −0.019 | 0.985 |
| Meibomian width centre (mm/mm2) | −0.137 | −0.219 | 0.831 |
| Meibomian width low (mm/mm2) | −0.051 | −0.117 | 0.909 |
| Trygliceridis (mg/dL) VS | |||
| Meibomian length (mm/mm2) | 0.078 | 0.242 | 0.813 |
| Meibomian area (mm2) | 0.264 | 1.002 | 0.336 |
| Meibomian width top (mm/mm2) | −1.100 | −2.420 | 0.277 |
| Meibomian width centre (mm/mm2) | 1.487 | 2.504 | 0.288 |
| Meibomian width low (mm/mm2) | −0.705 | −2.005 | 0.682 |
| Total Cholesterol (mg/dL) VS | |||
| Meibomian length (mm/mm2) | 0.639 | 1.634 | 0.133 |
| Meibomian area (mm2) | 0.337 | 1.119 | 0.289 |
| Meibomian width top (mm/mm2) | −1.024 | −1.834 | 0.097 |
| Meibomian width centre (mm/mm2) | 1.558 | 2.512 | 0.204 |
| Meibomian width low (mm/mm2) | −0.938 | −2.536 | 0.115 |
| HDL cholesterol (mg/dL) vs | |||
| Meibomian length (mm/mm2) | 0.529 | 1.350 | 0.207 |
| Meibomian area (mm2) | −0.516 | −1.709 | 0.118 |
| Meibomian width top (mm/mm2) | −0.686 | −1.227 | 0.248 |
| Meibomian width centre (mm/mm2) | 0.048 | 0.078 | 0.940 |
| Meibomian width low (mm/mm2) | 0.606 | 1.636 | 0.133 |
| LDL Cholesterol (mg/dL) vs | |||
| Meibomian length (mm/mm2) | 0.388 | 0.737 | 0.494 |
| Meibomian area (mm2) | 0.105 | 0.246 | 0.815 |
| Meibomian width top (mm/mm2) | 0.170 | 0.215 | 0.838 |
| Meibomian width centre (mm/mm2) | 0.658 | 0.828 | 0.445 |
| Meibomian width low (mm/mm2) | −0.347 | −0.742 | 0.491 |
| DHEAS (µg/dL) VS | |||
| Meibomian length (mm/mm2) | −0.512 | −1.520 | 0.154 |
| Meibomian area (mm2) | 0.050 | 0.183 | 0.858 |
| Meibomian width top (mm/mm2) | 1.377 | 2.884 | 0.921 |
| Meibomian width centre (mm/mm2) | −1.415 | −2.270 | 0.832 |
| Meibomian width low (mm/mm2) | −0.052 | −0.140 | 0.891 |
| ASD (ng/mL) VS | |||
| Meibomian length (mm/mm2) | 0.478 | 2.174 | 0.045 * |
| Meibomian area (mm2) | 0.051 | 0.166 | 0.871 |
| Meibomian width top (mm/mm2) | 0.505 | 0.950 | 0.361 |
| Meibomian width centre (mm/mm2) | −0.598 | −0.861 | 0.406 |
| Meibomian width low (mm/mm2) | −0.041 | −0.101 | 0.921 |
| Cortisol (µg/dL) vs | |||
| Meibomian length (mm/mm2) | 0.510 | 1.321 | 0.211 |
| Meibomian area (mm2) | −0.220 | −0.695 | 0.500 |
| Meibomian width top (mm/mm2) | −0.279 | −0.510 | 0.619 |
| Meibomian width centre (mm/mm2) | −0.024 | −0.034 | 0.974 |
| Meibomian width low (mm/mm2) | 0.419 | 0.990 | 0.342 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abbouda, A.; Florido, A.; Avogaro, F.; Bladen, J.; Vingolo, E.M. Identifying Meibomian Gland Dysfunction Biomarkers in a Cohort of Patients Affected by DM Type II. Vision 2023, 7, 28. https://doi.org/10.3390/vision7020028
Abbouda A, Florido A, Avogaro F, Bladen J, Vingolo EM. Identifying Meibomian Gland Dysfunction Biomarkers in a Cohort of Patients Affected by DM Type II. Vision. 2023; 7(2):28. https://doi.org/10.3390/vision7020028
Chicago/Turabian StyleAbbouda, Alessandro, Antonio Florido, Filippo Avogaro, John Bladen, and Enzo Maria Vingolo. 2023. "Identifying Meibomian Gland Dysfunction Biomarkers in a Cohort of Patients Affected by DM Type II" Vision 7, no. 2: 28. https://doi.org/10.3390/vision7020028
APA StyleAbbouda, A., Florido, A., Avogaro, F., Bladen, J., & Vingolo, E. M. (2023). Identifying Meibomian Gland Dysfunction Biomarkers in a Cohort of Patients Affected by DM Type II. Vision, 7(2), 28. https://doi.org/10.3390/vision7020028