Vision Rehabilitation is Part of AMD Care

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
1.1. Patient-Centered Functional Priorities
- Reading—many patients express this as their foremost concern.
- Activities of Daily Living—even though reading may be the most prominent complaint, most people spend a larger part of their day performing a variety of other vision-dependent activities, such as self-care and home management.
- Safety—are people at risk for falls? How do they cross the street? Do they drive?
- Community participation—can the individual still participate in community events, including religious gatherings?
- Physical, cognitive and psychosocial well-being—since many patients with vision loss are elderly, these are important aspects that should not be overlooked. If cognitive problems exist, it may affect the recommendations to be made.
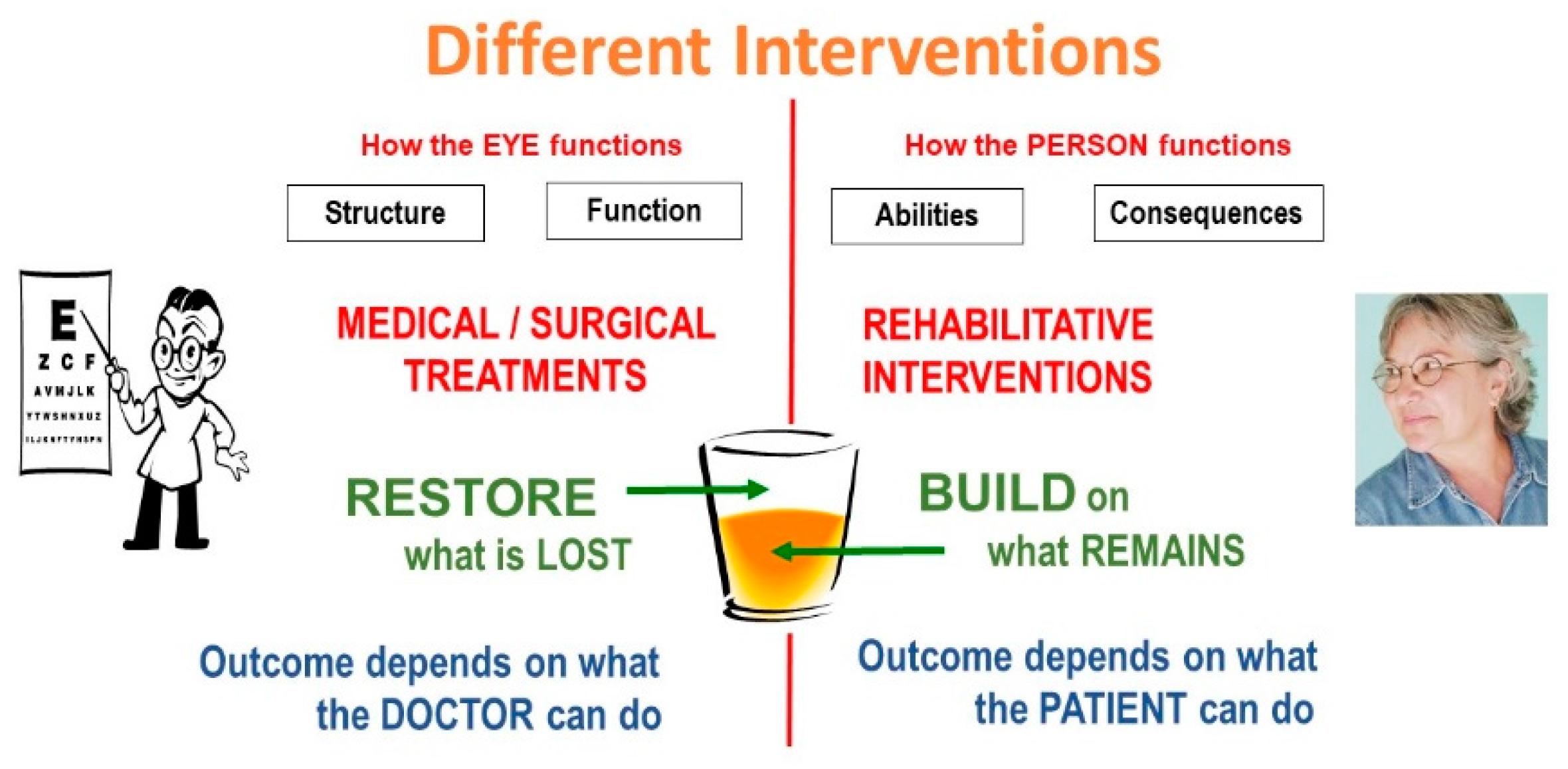
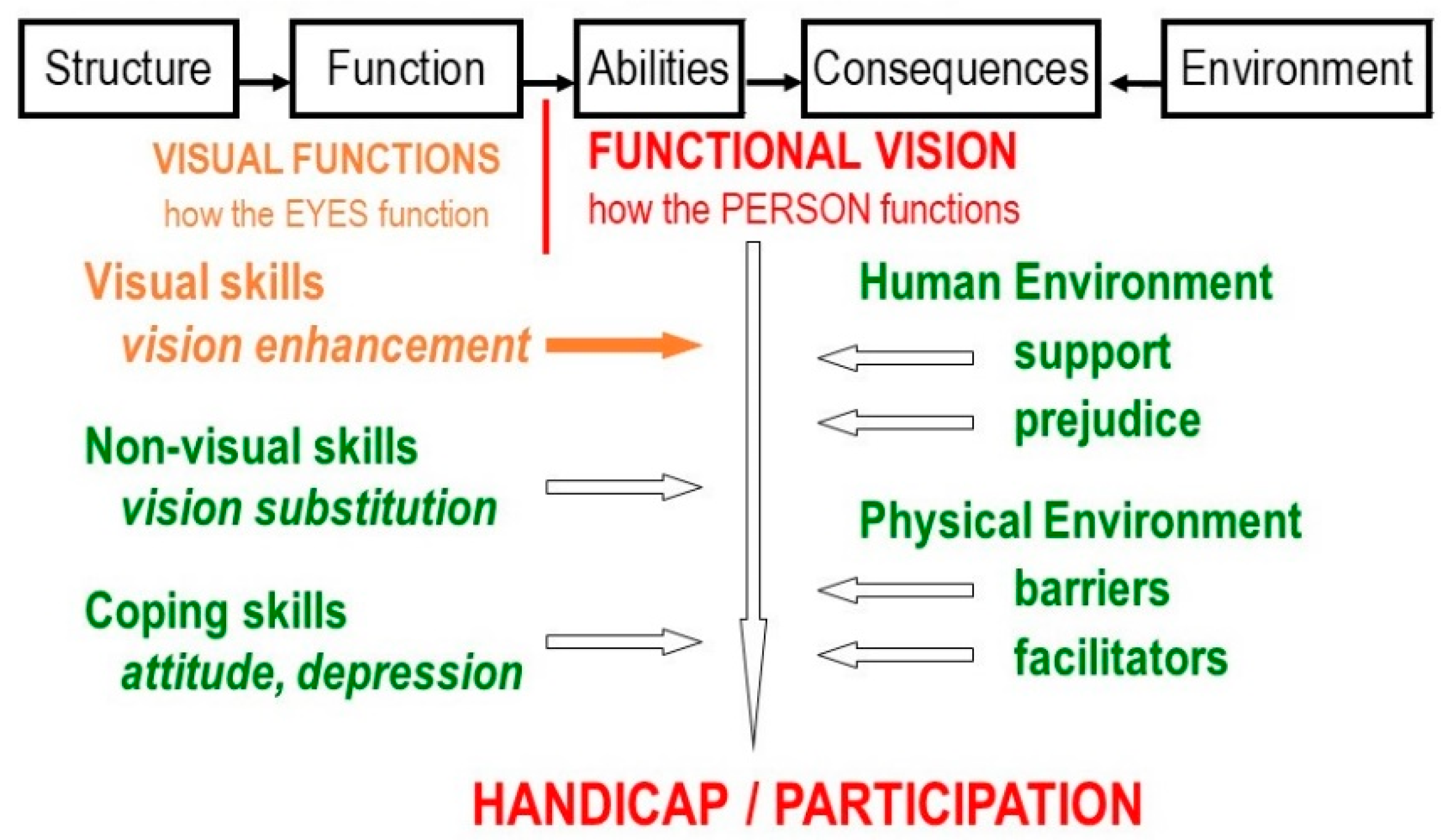
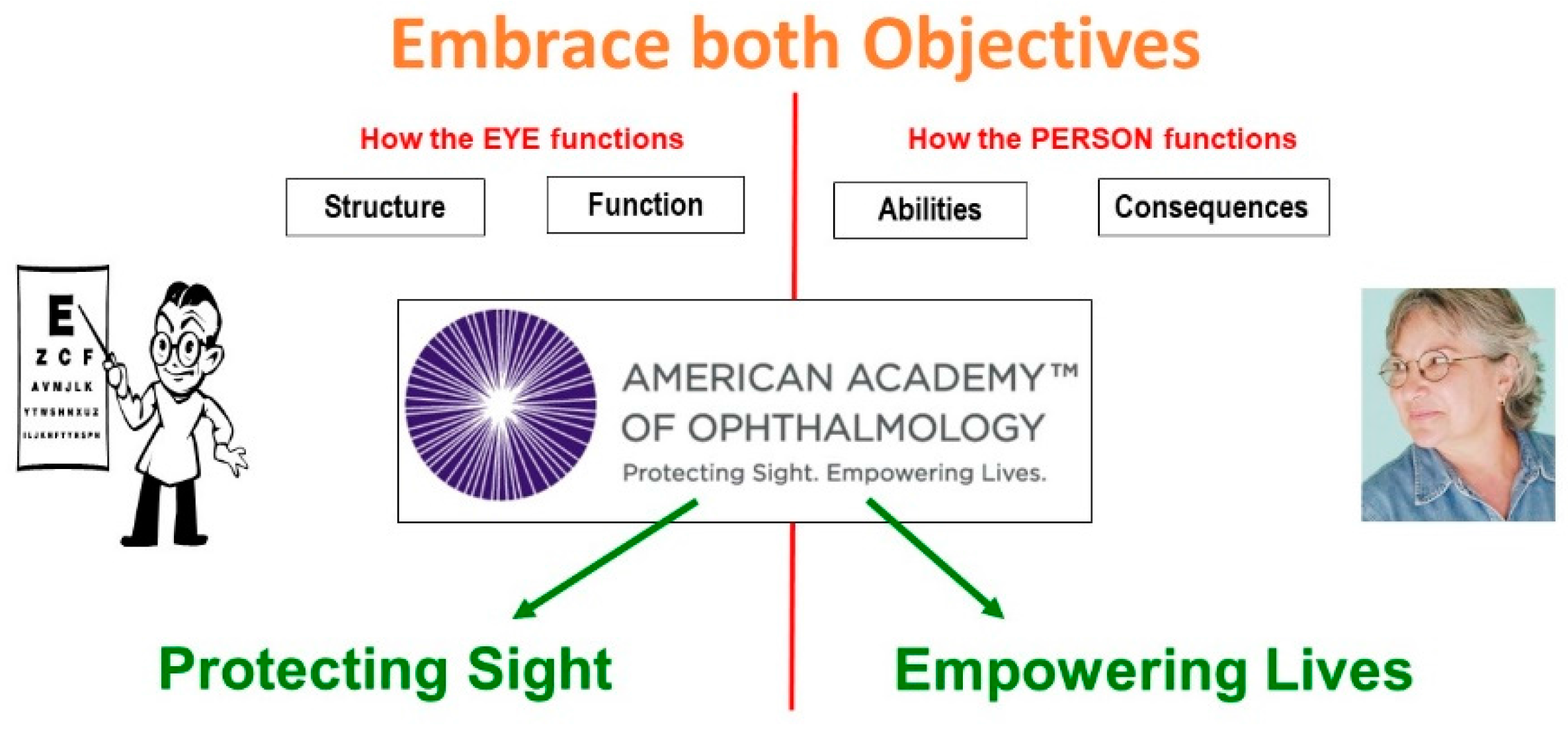
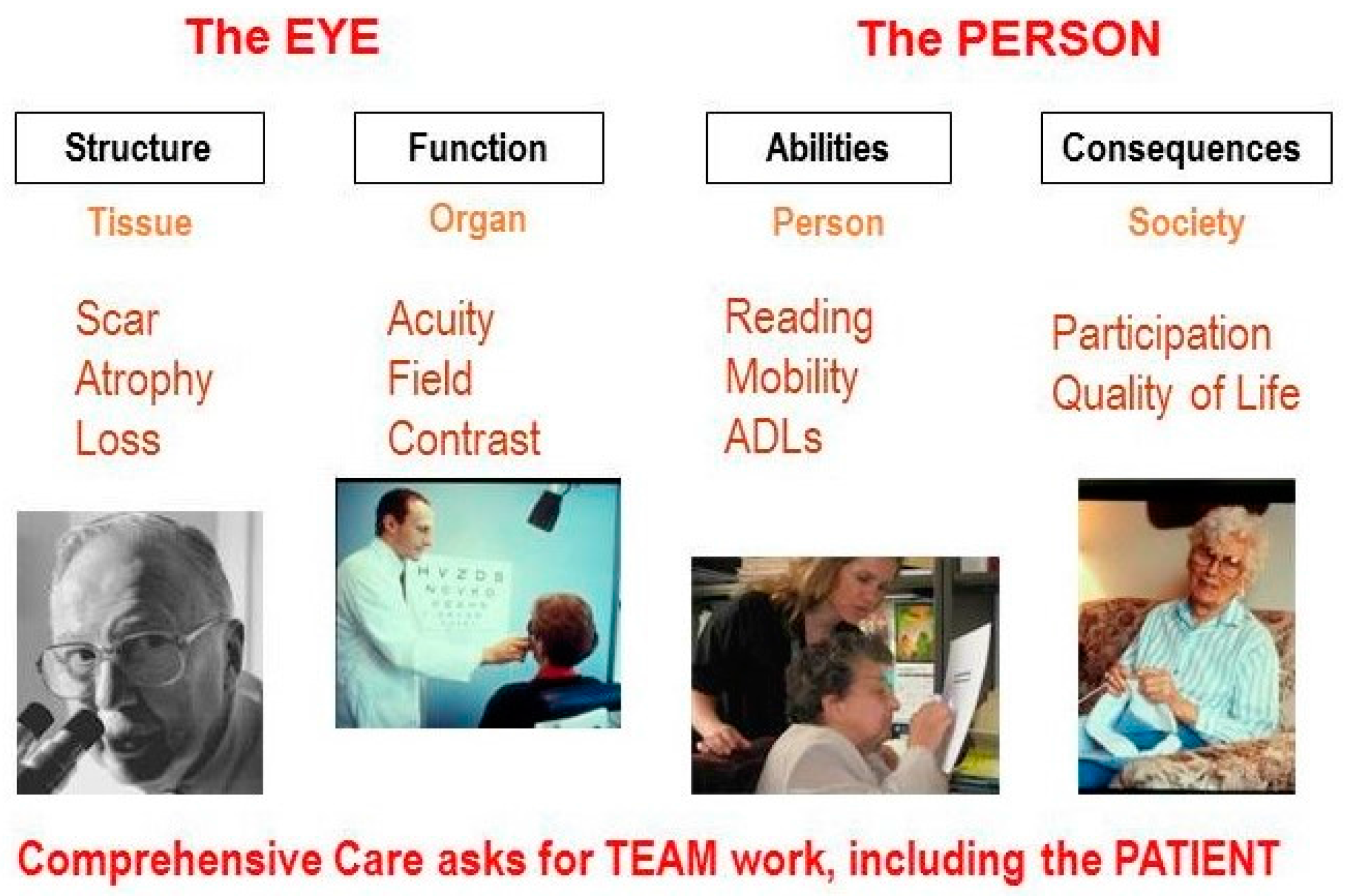
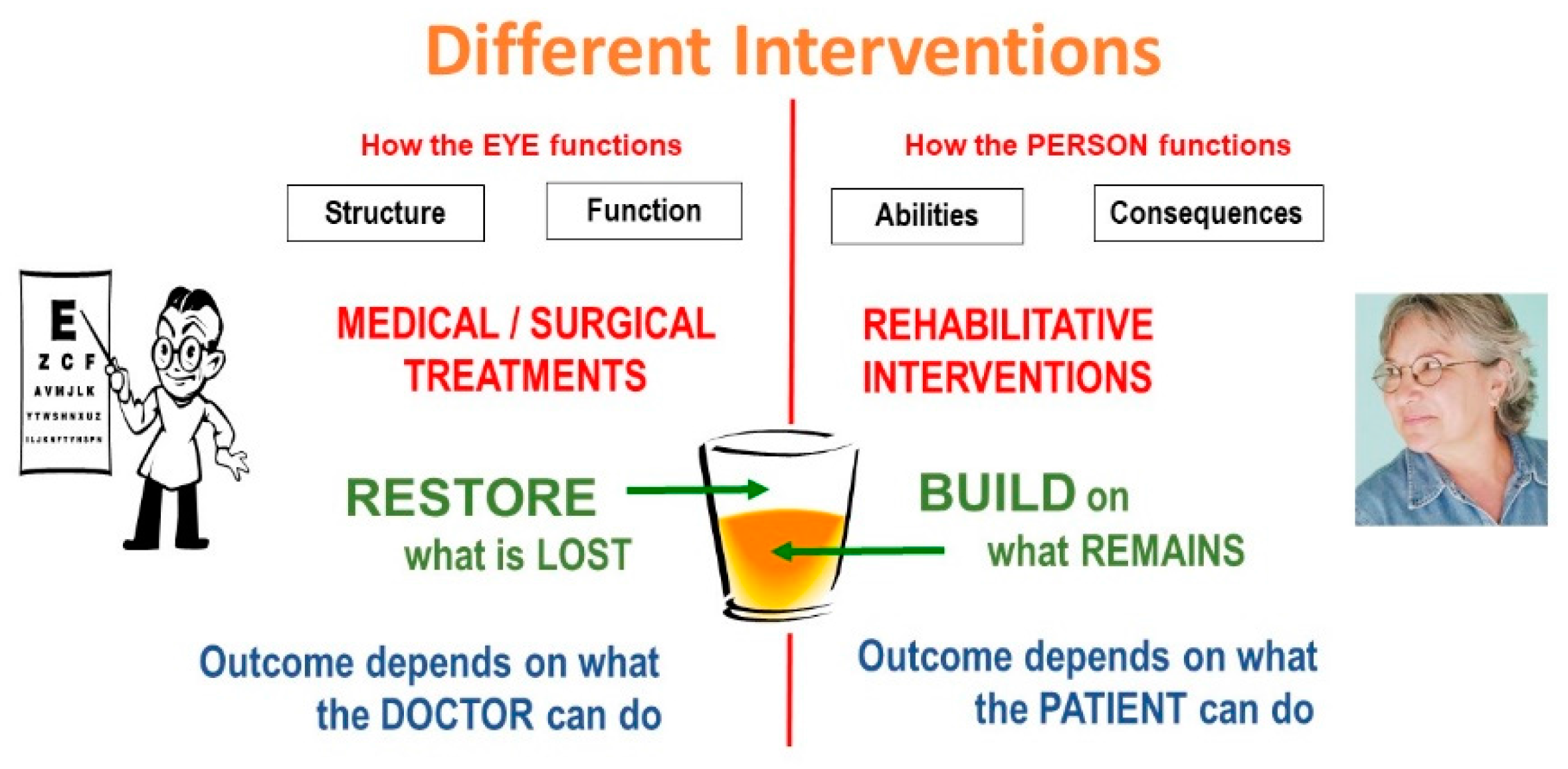
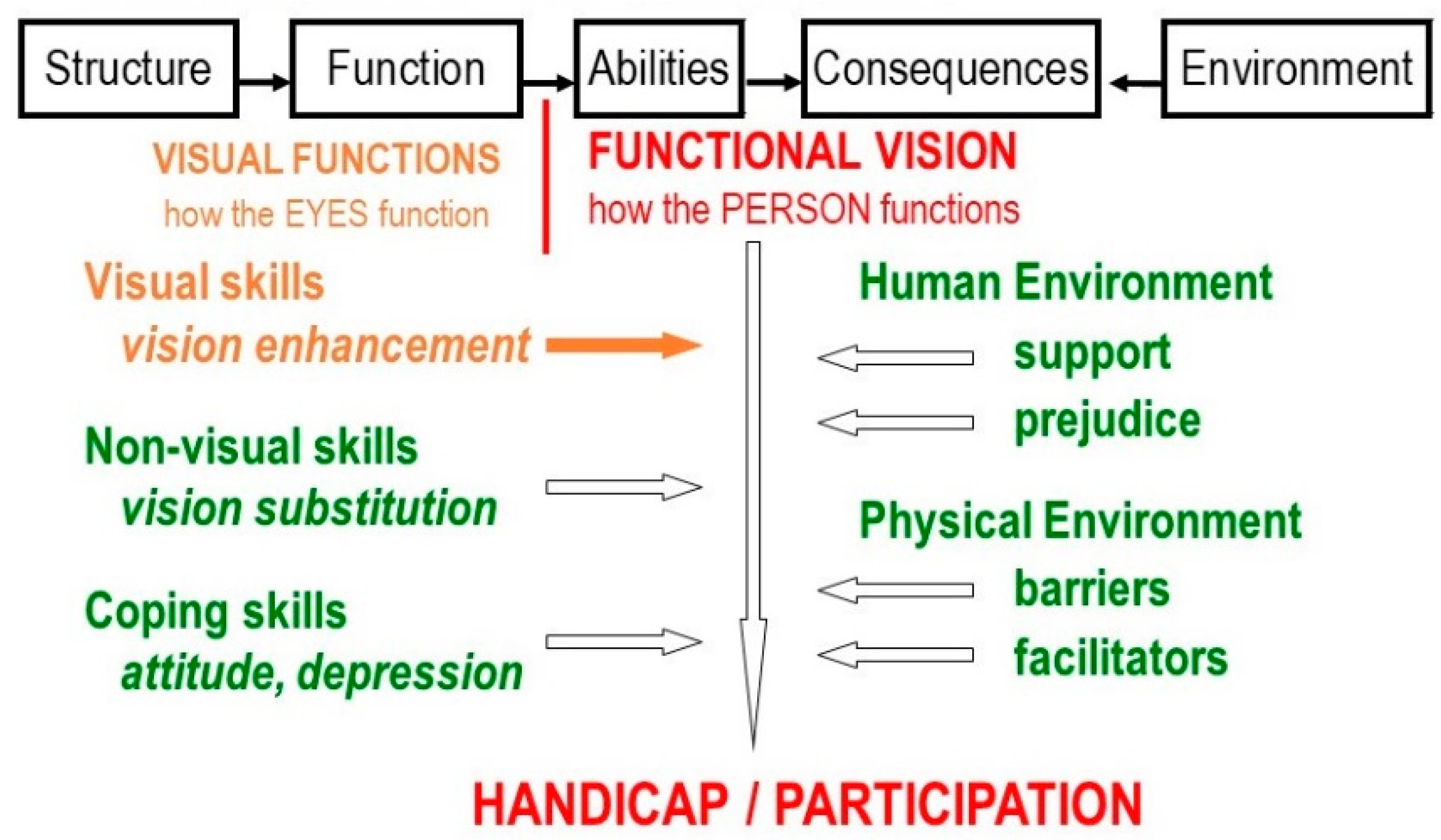
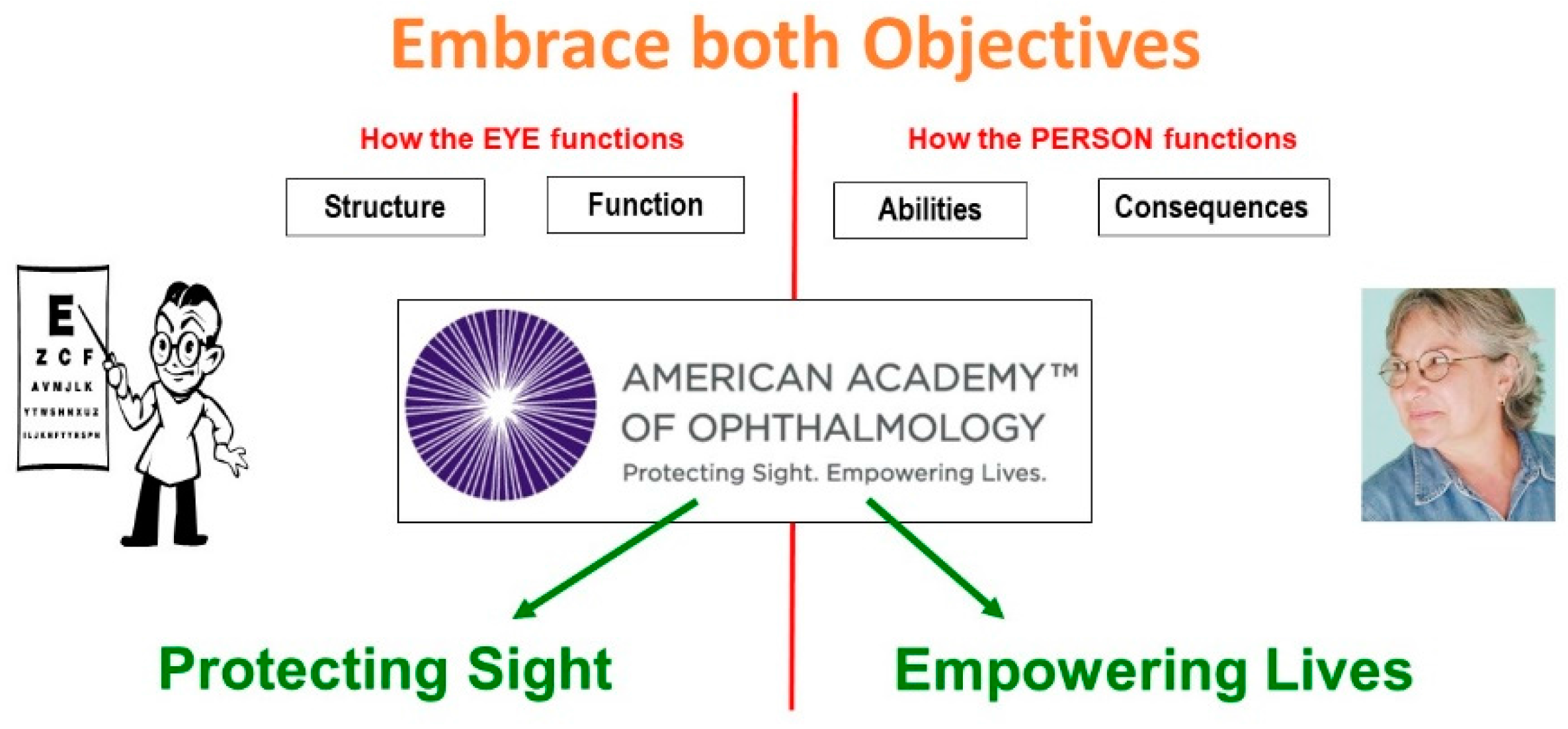
1.2. Four Aspects of Vision Loss
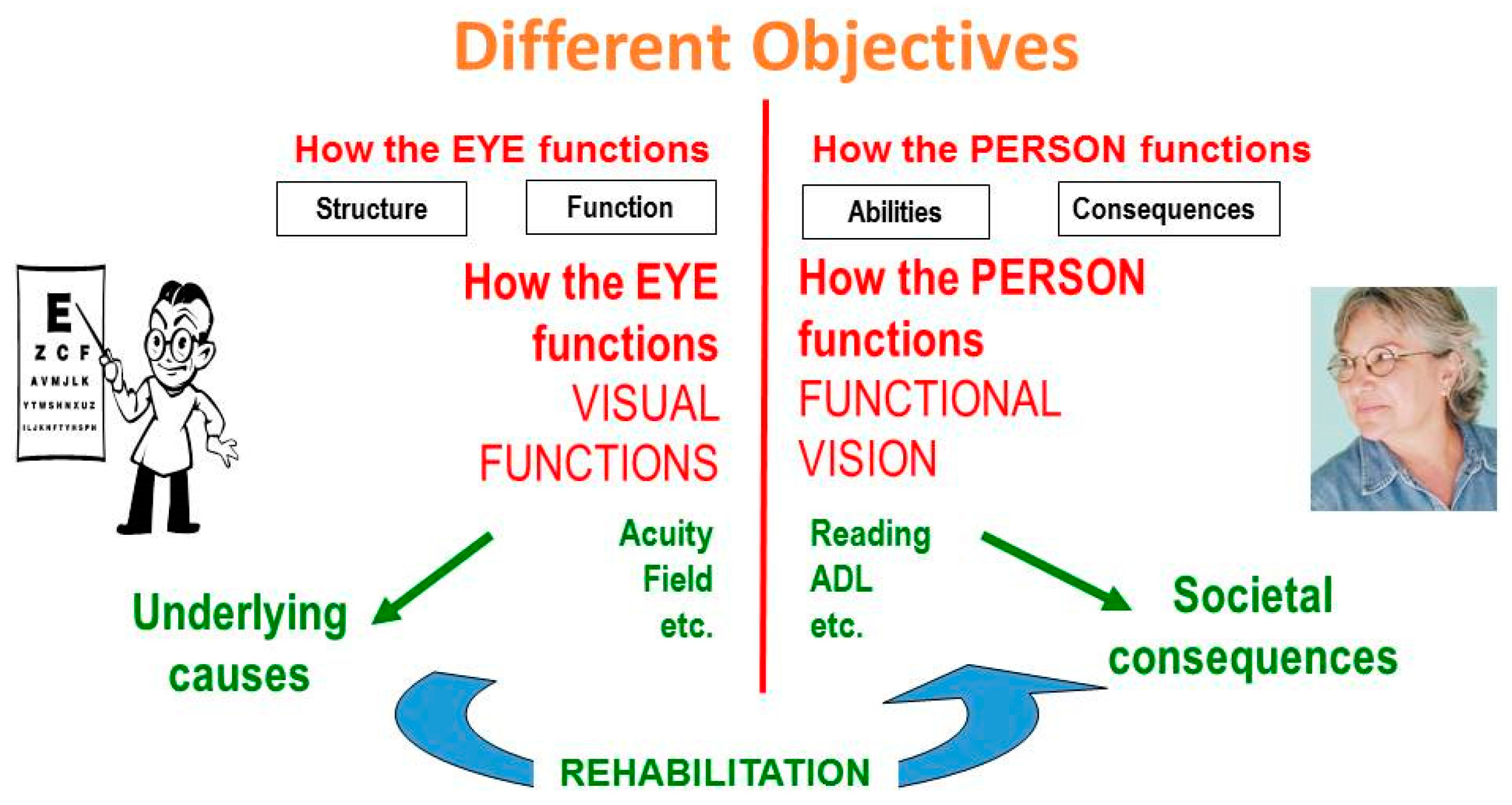
1.3. Vision Rehabilitation
1.4. Functional Assessment
- Detail vision—Usually measured as visual acuity.Letter chart acuity describes only the function of the central 1-degree area.
- Surround vision—Usually described as visual fieldSurround vision involves everything beyond the central 1-degree area.
- Contrast vision—Interacts with both acuity and field.Better illumination and better contrast can result in better acuity and a better field.
2. Detail Vision
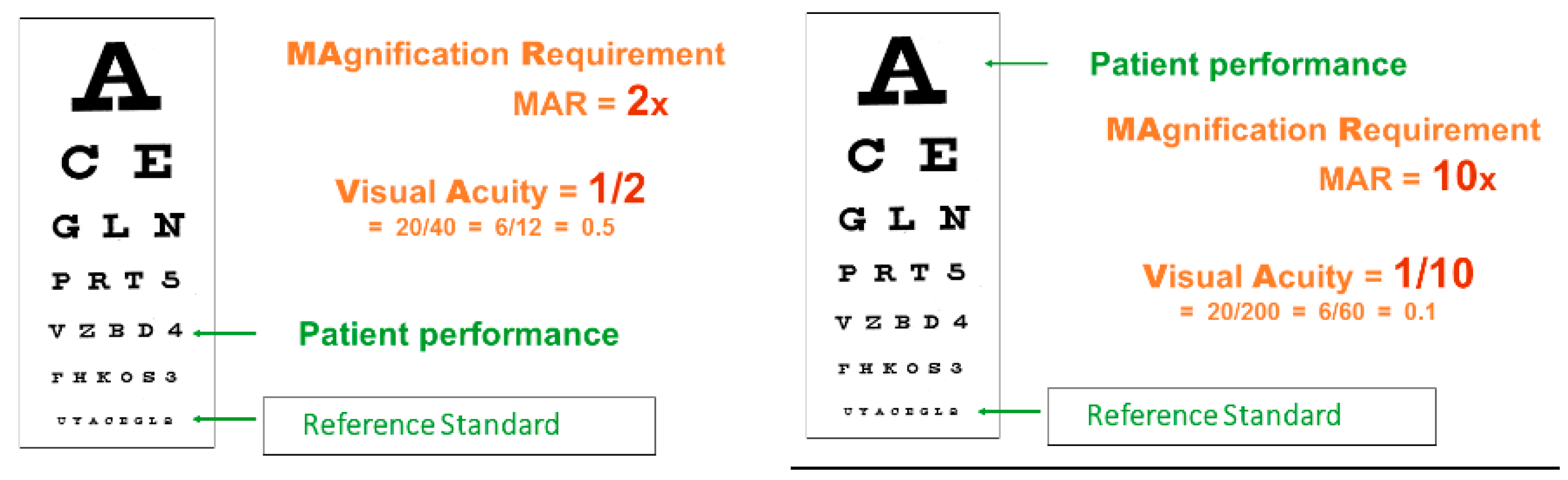
2.1. Recording Detail Vision
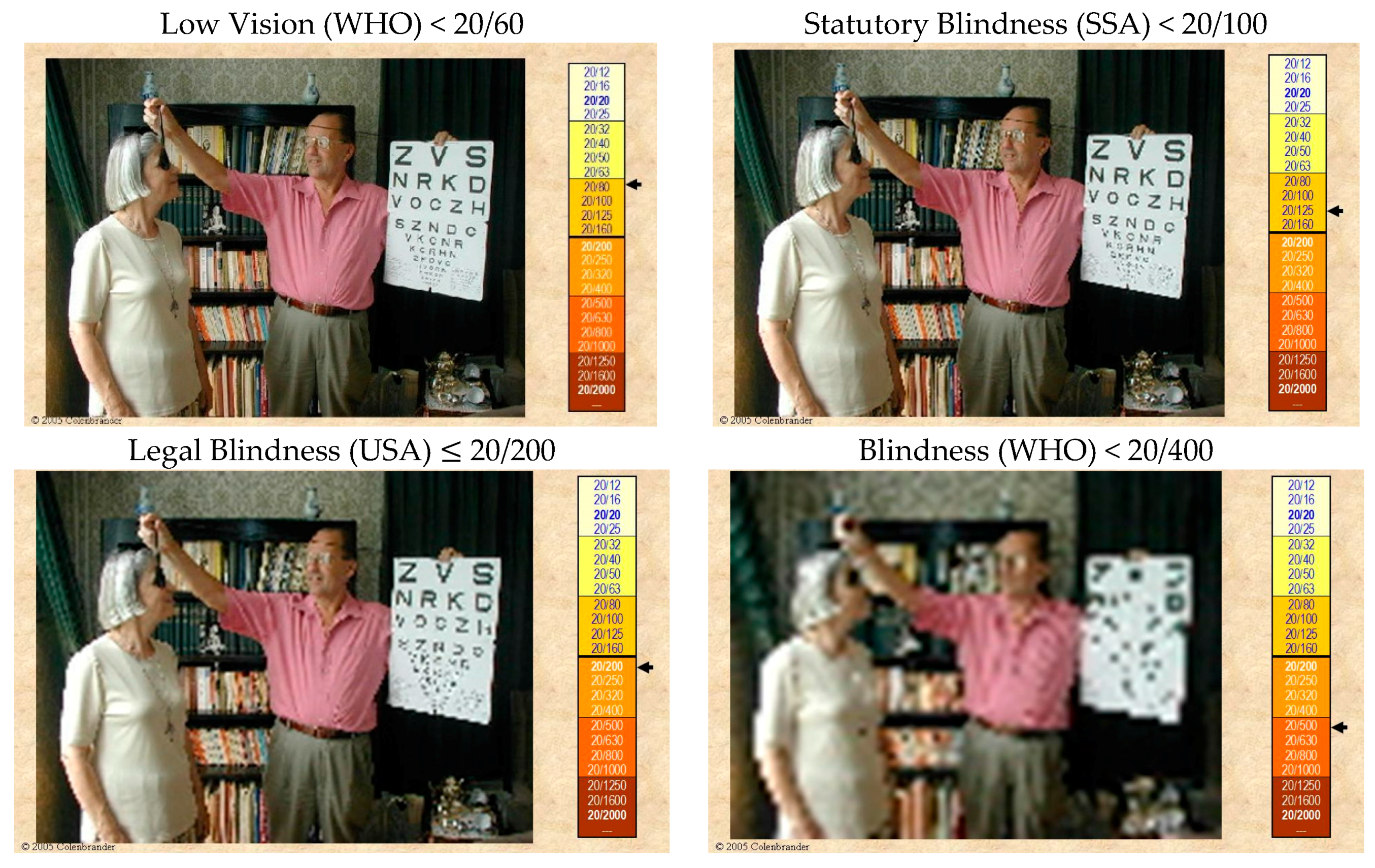
2.2. Labels for Detail Vision
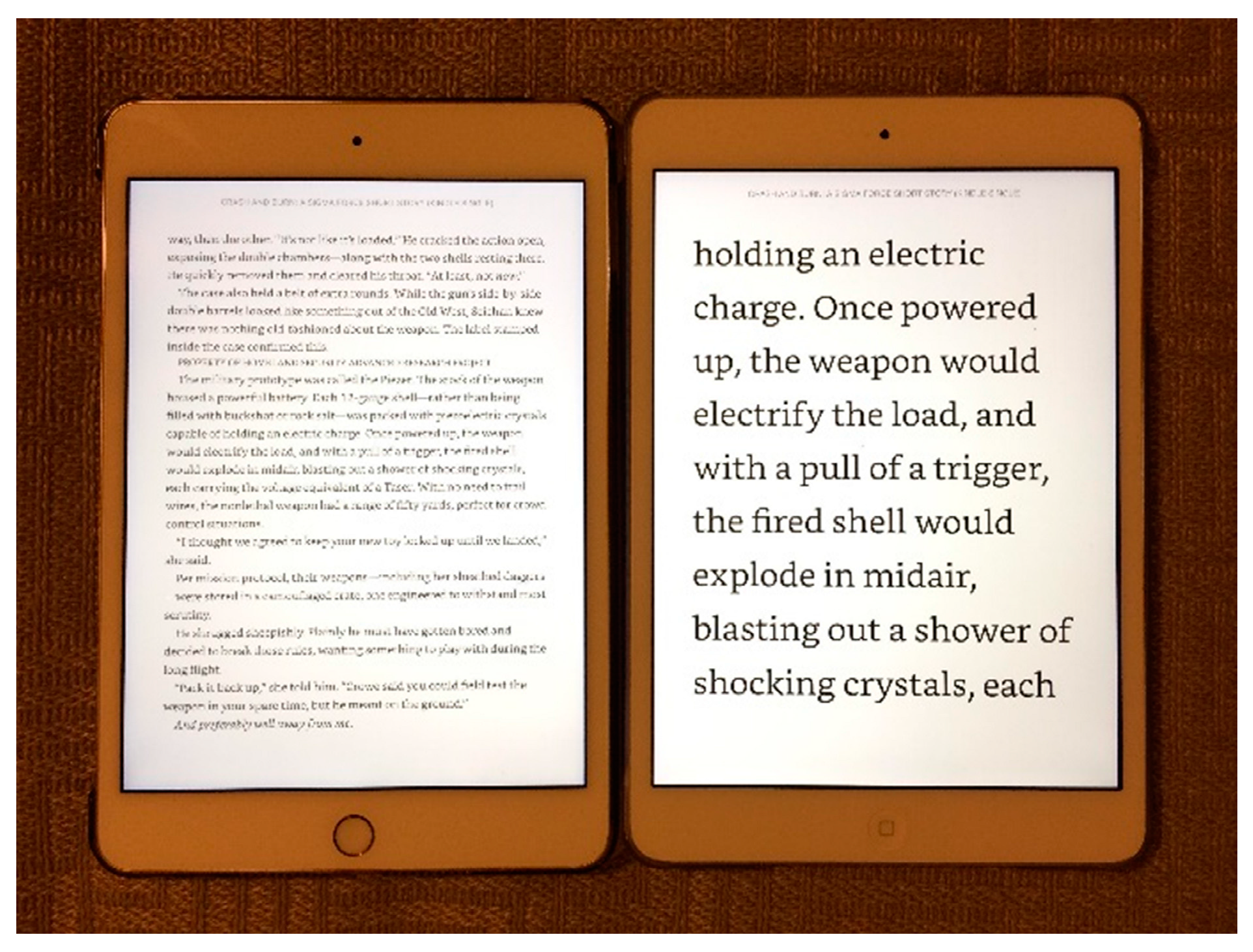
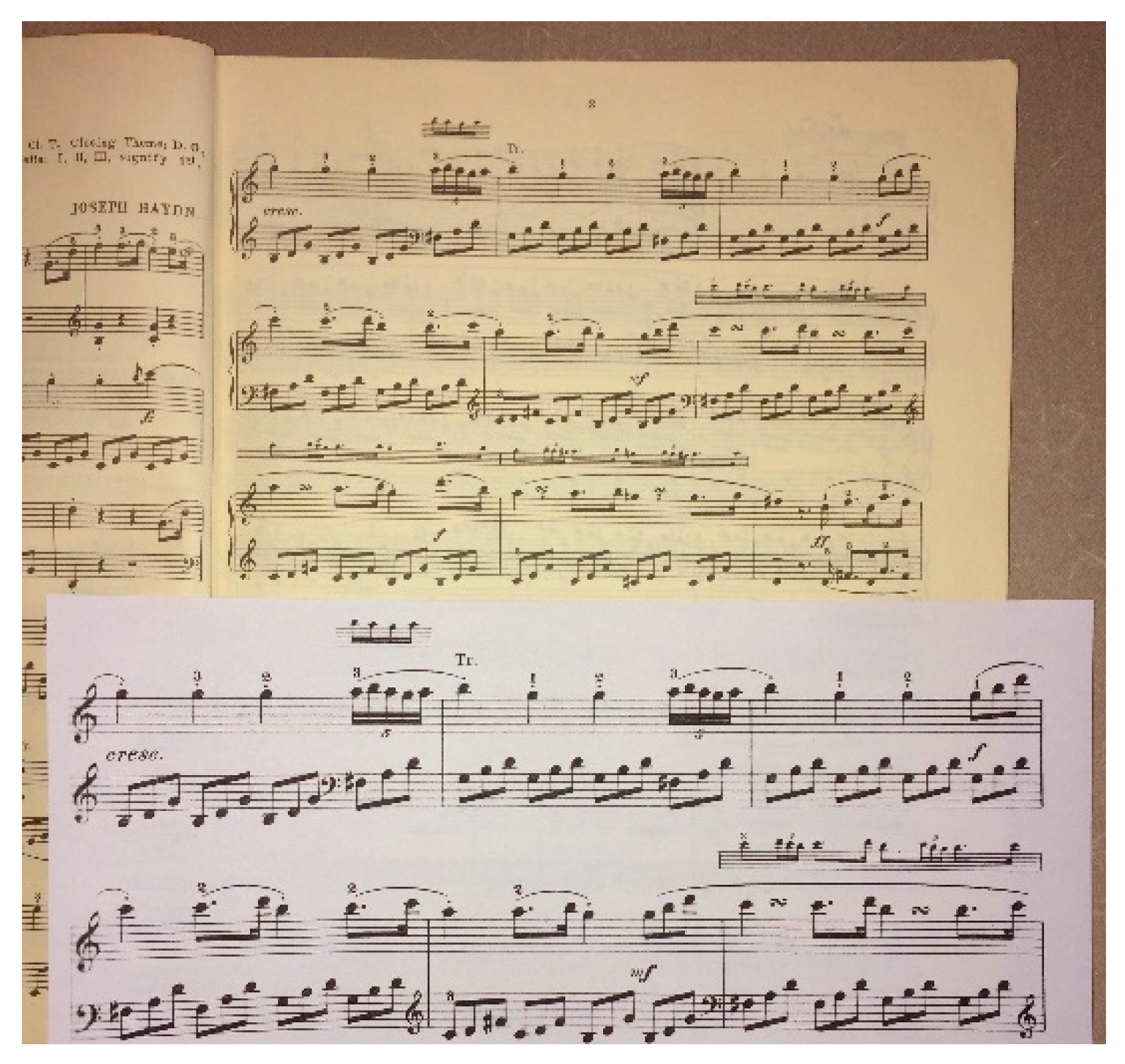
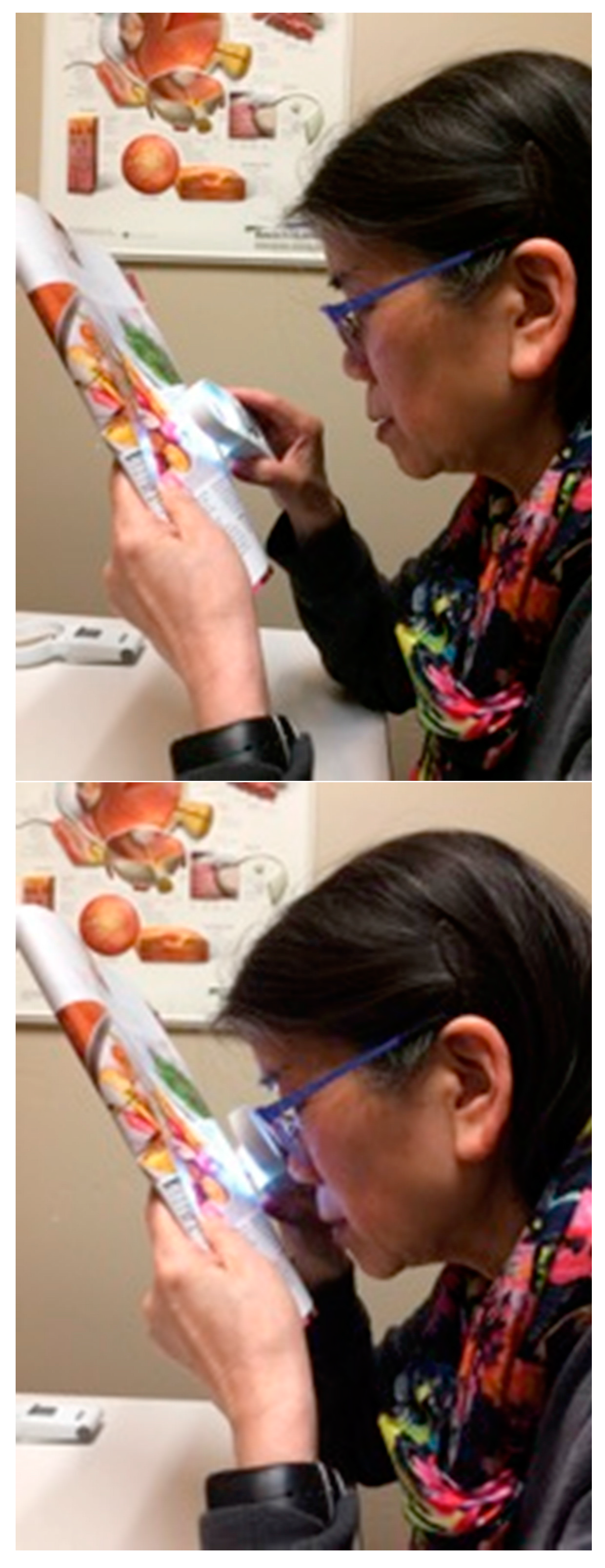
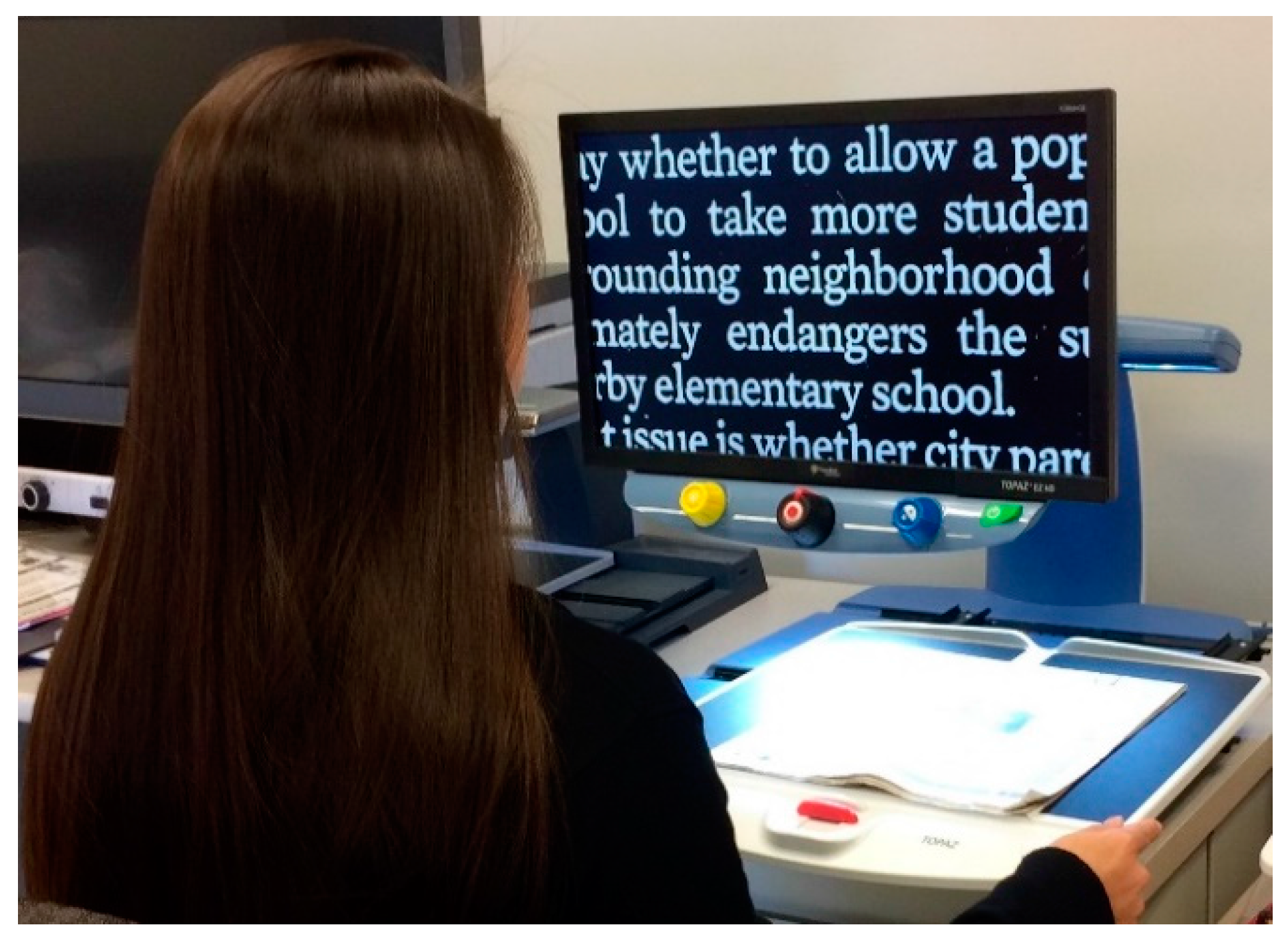
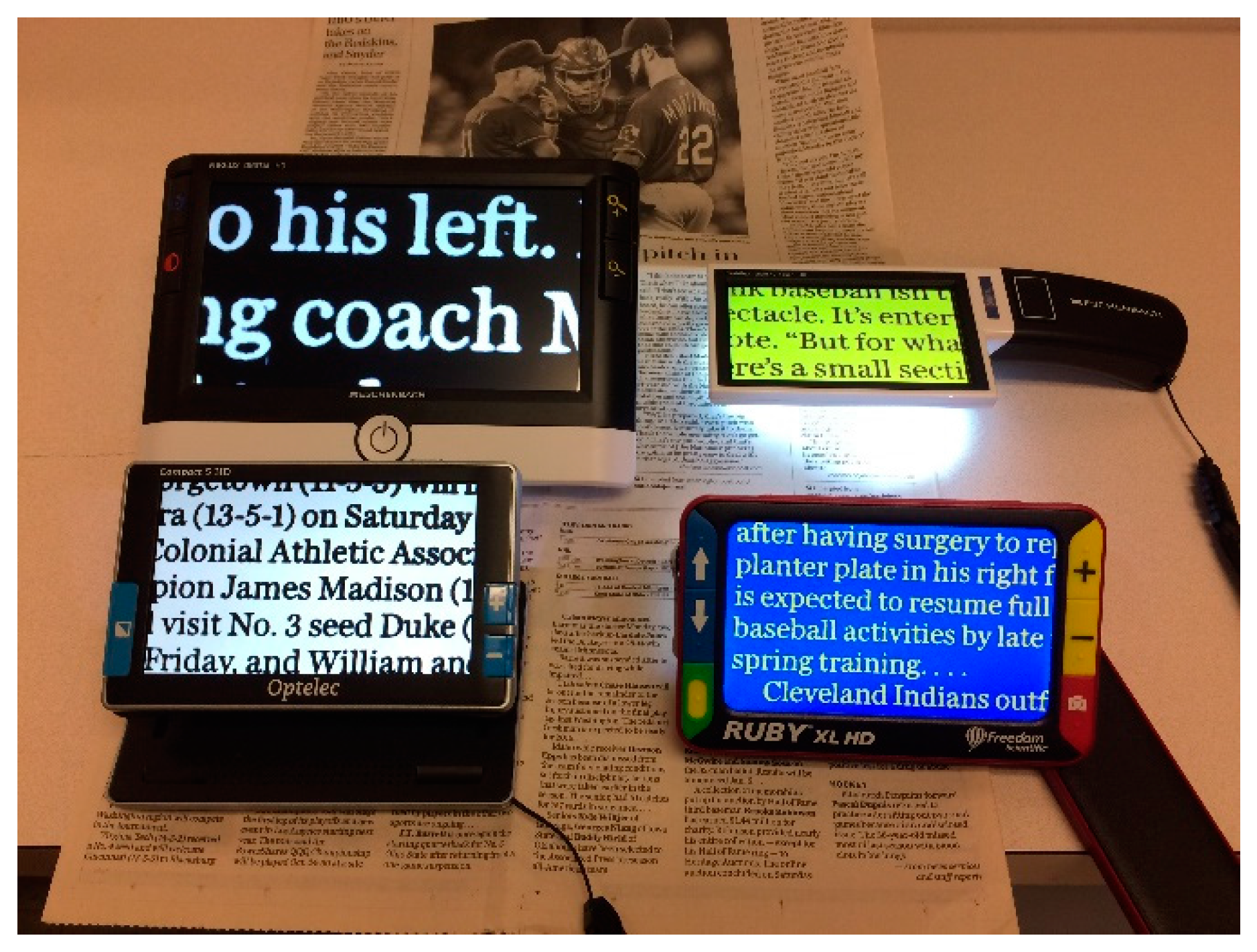
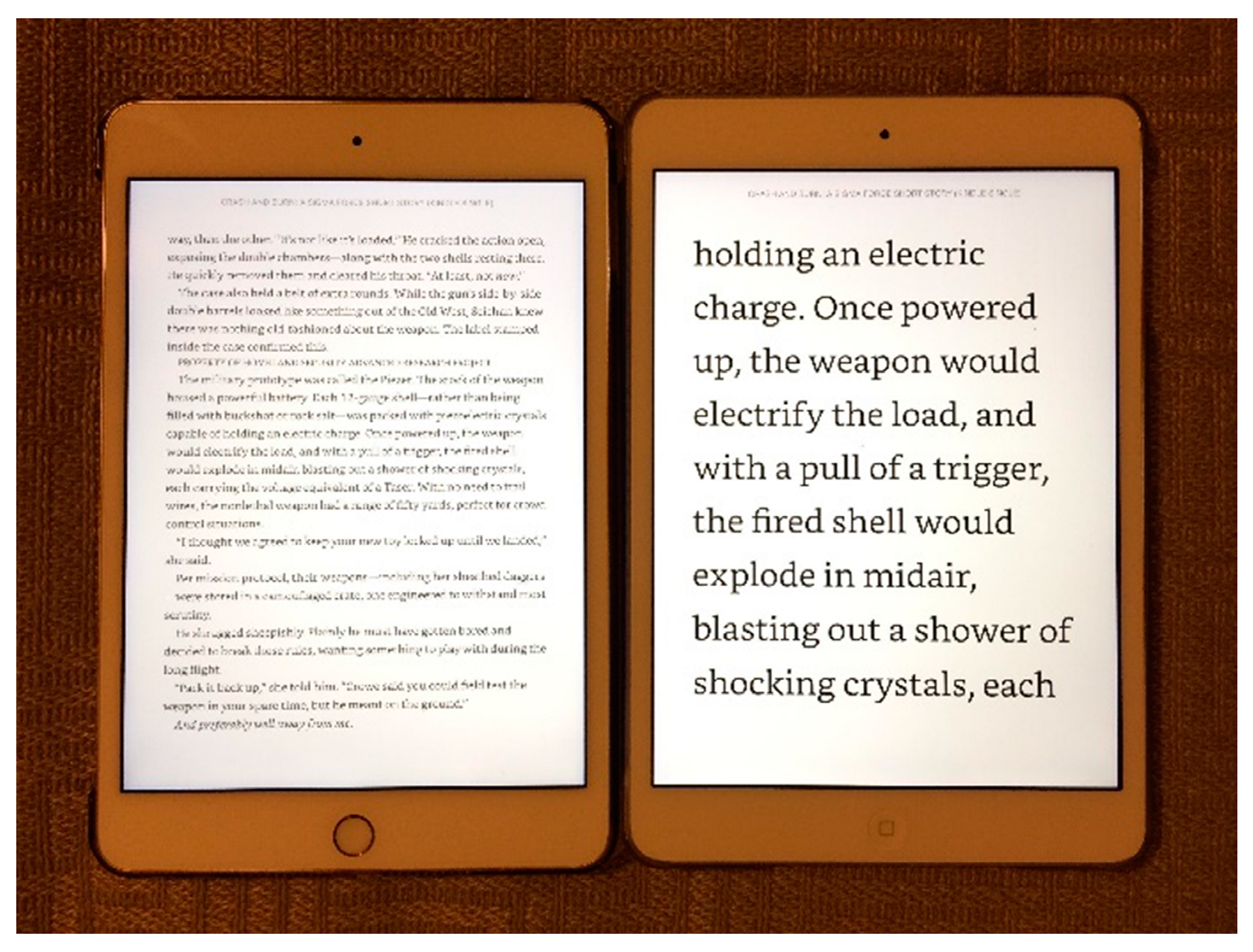
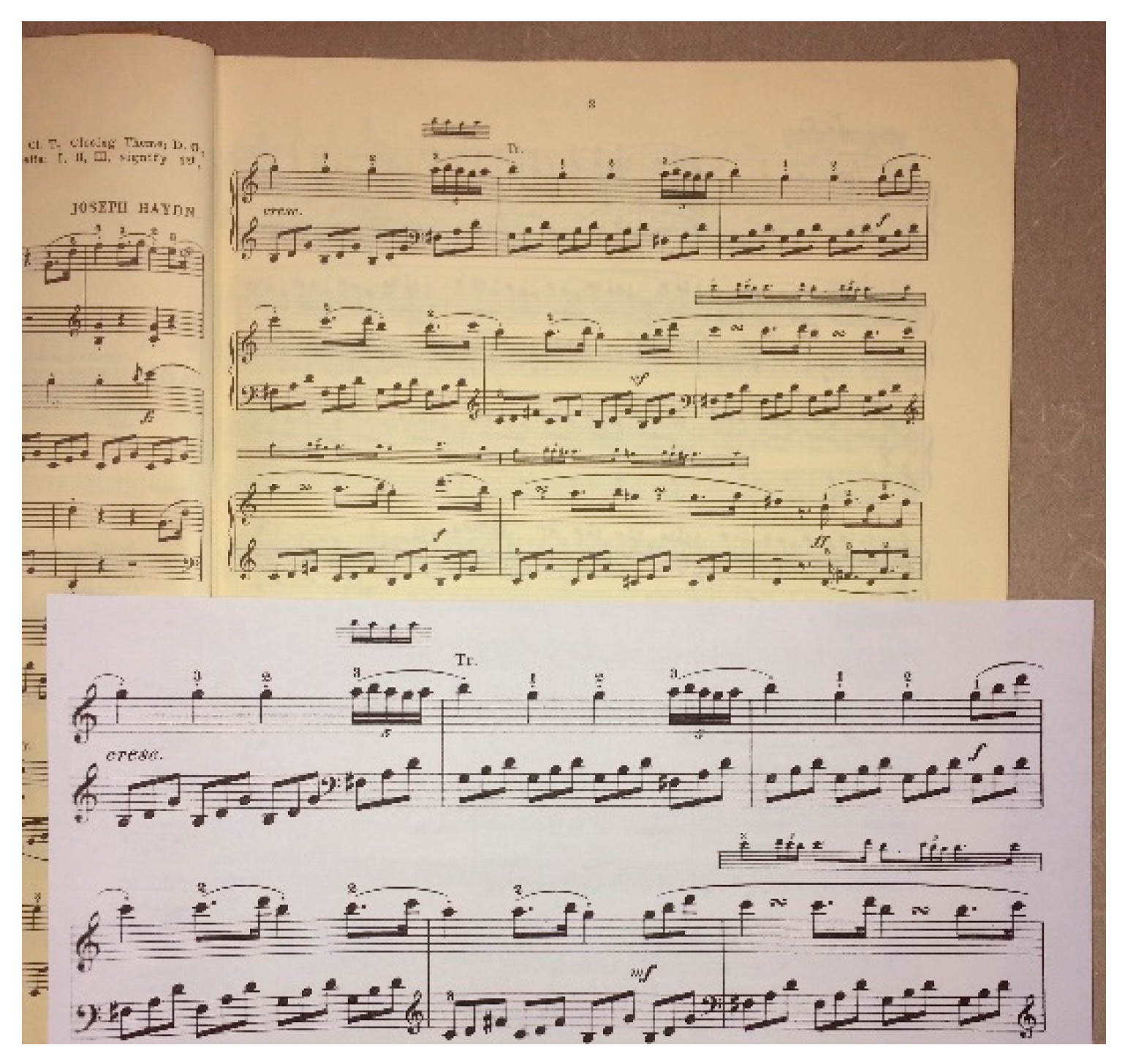
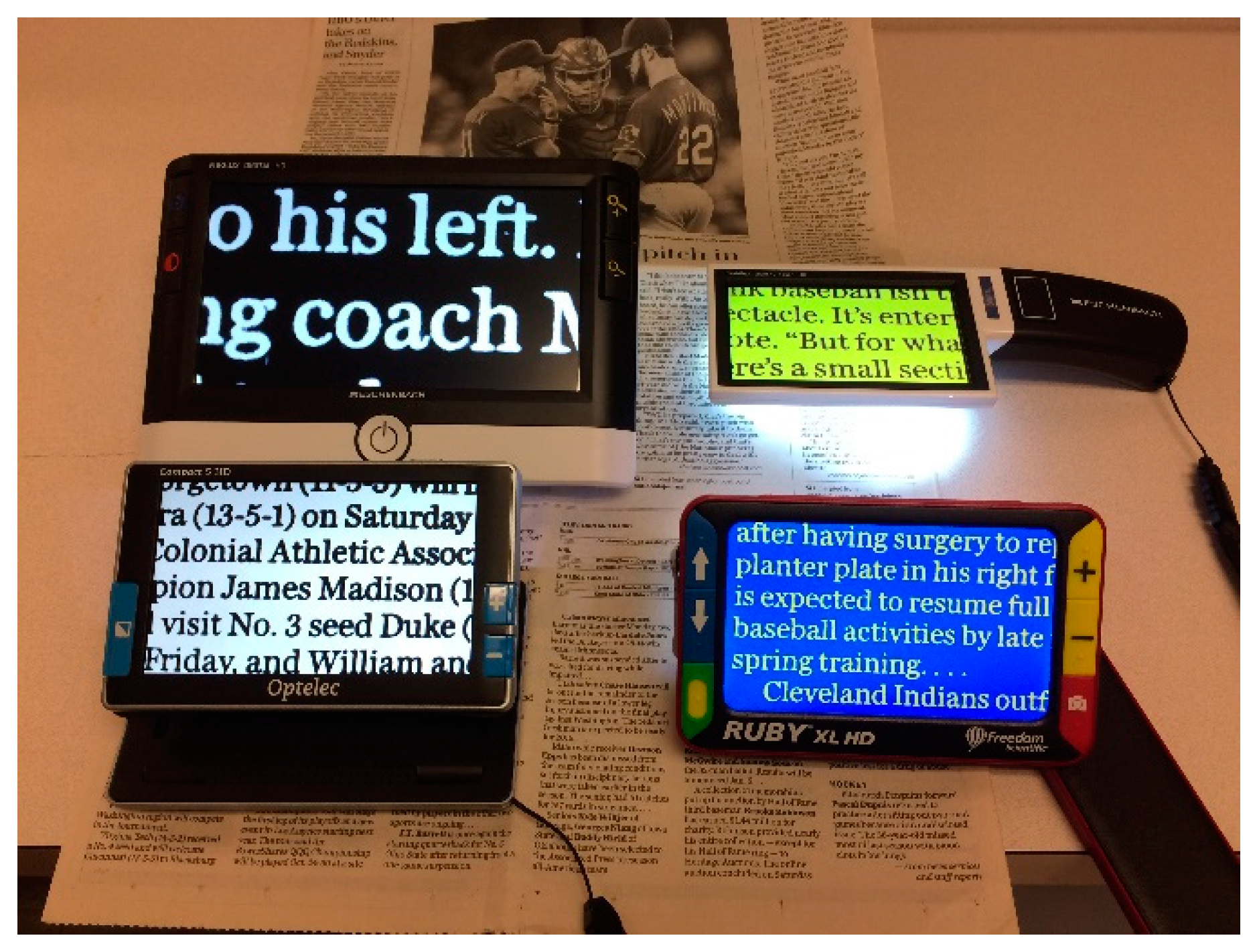
2.3. Remediation for Loss of Detail Vision
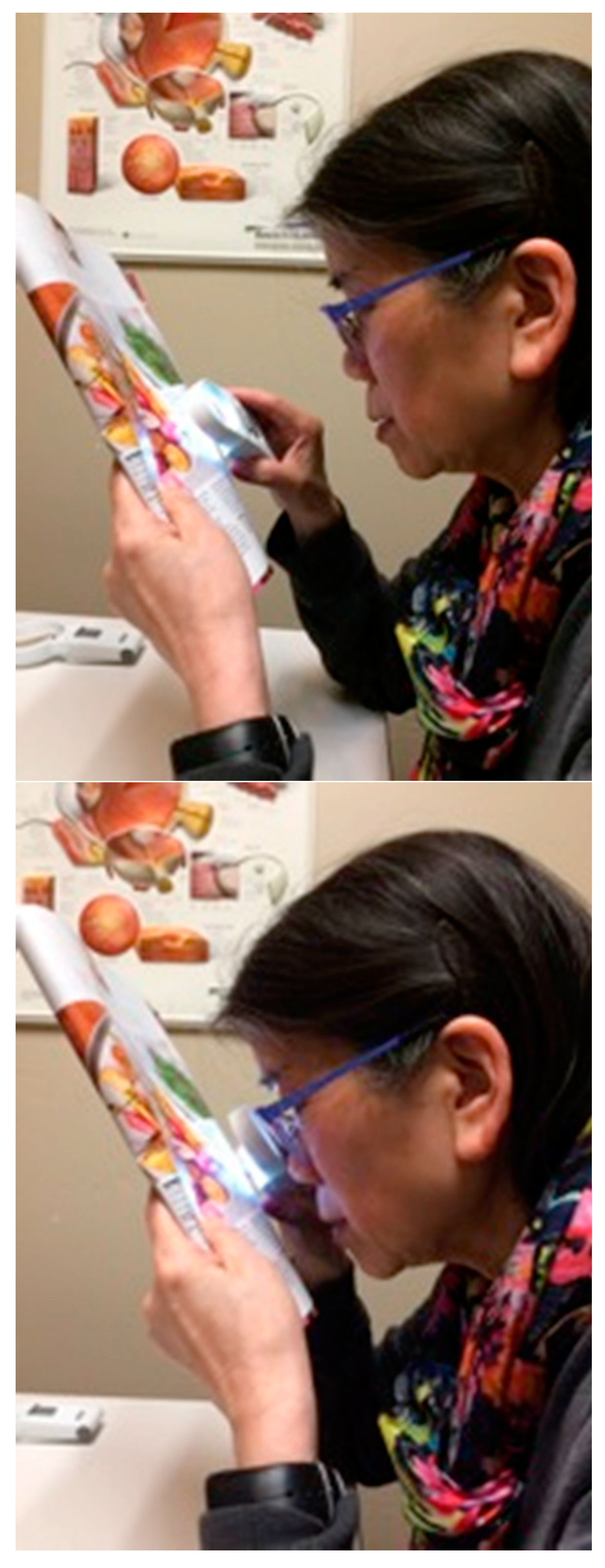
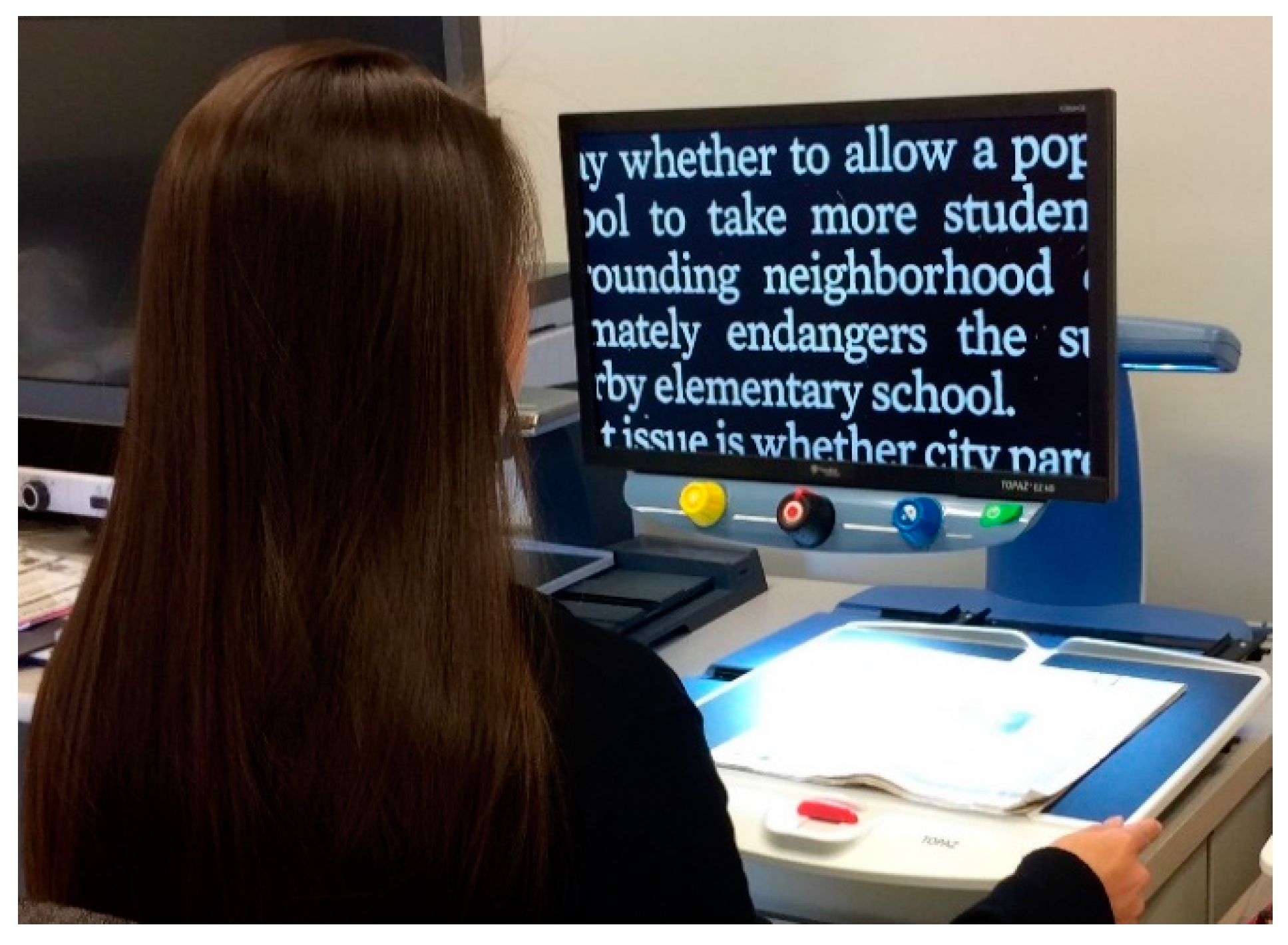
2.4. Vision Substitution
3. Surround Vision
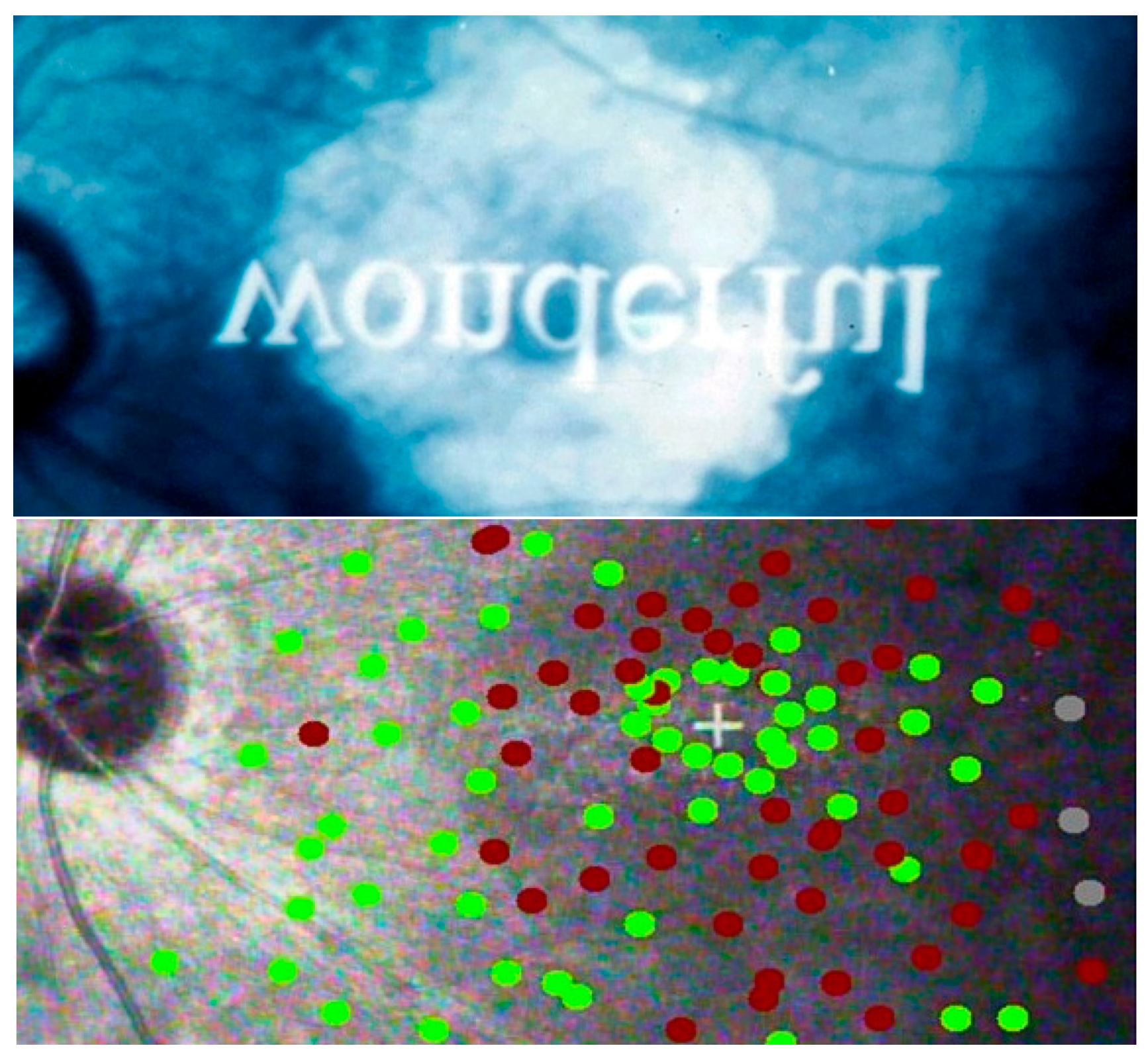
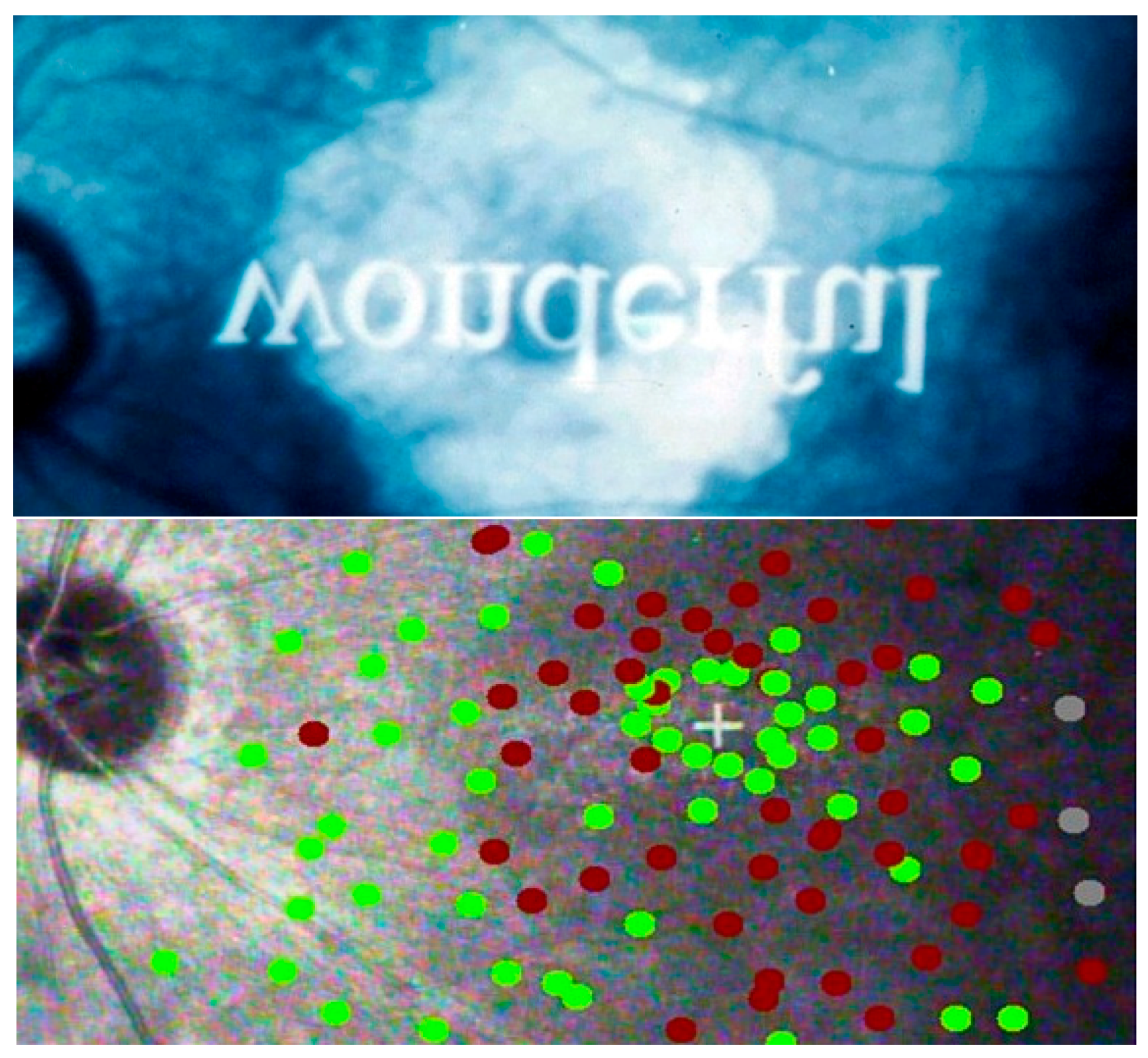
3.1. The Nature of Surround Vision
3.2. Remediation for Surround Vision Loss
4. Contrast Vision and Illumination
4.1. The nature of contrast vision
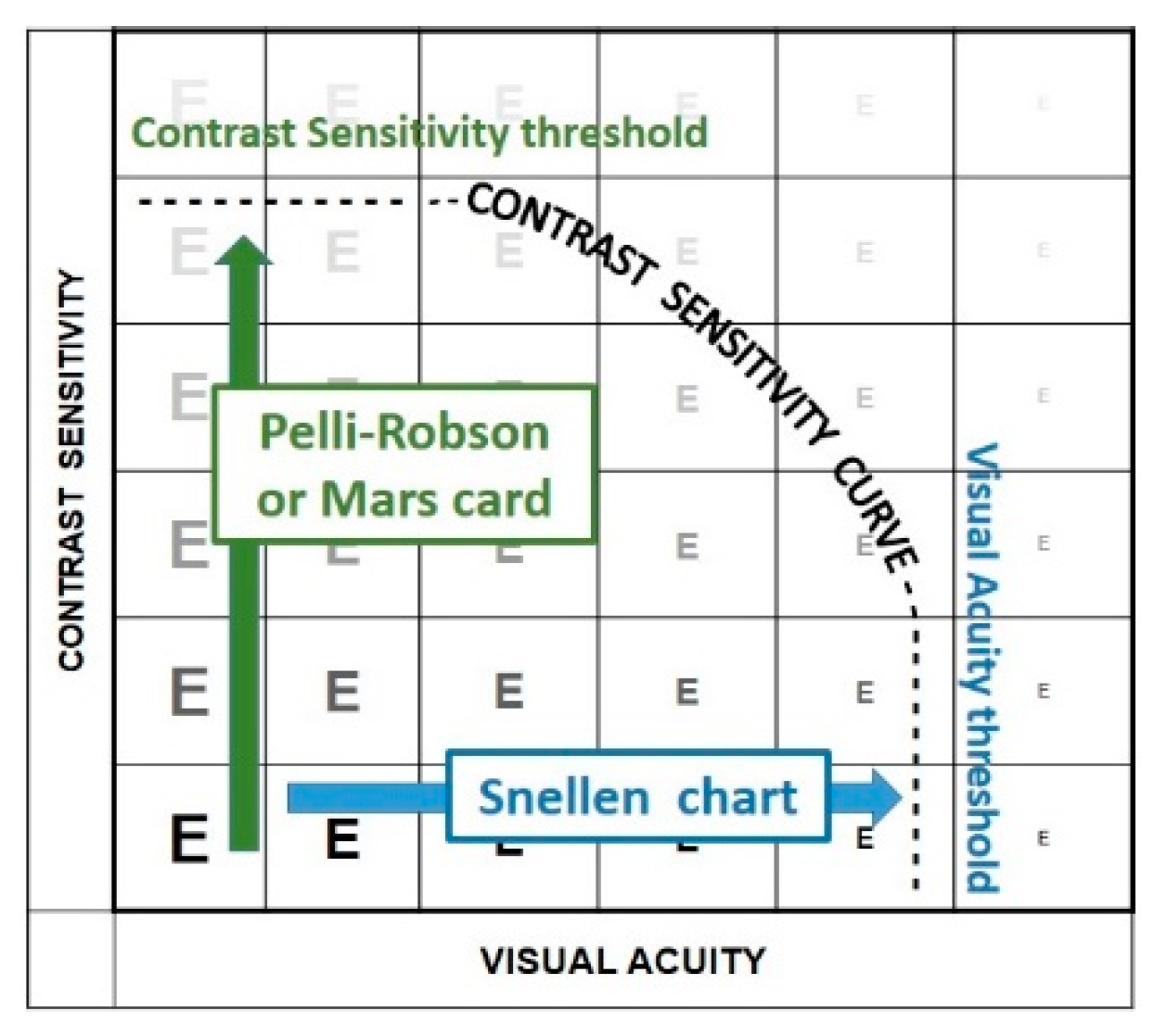
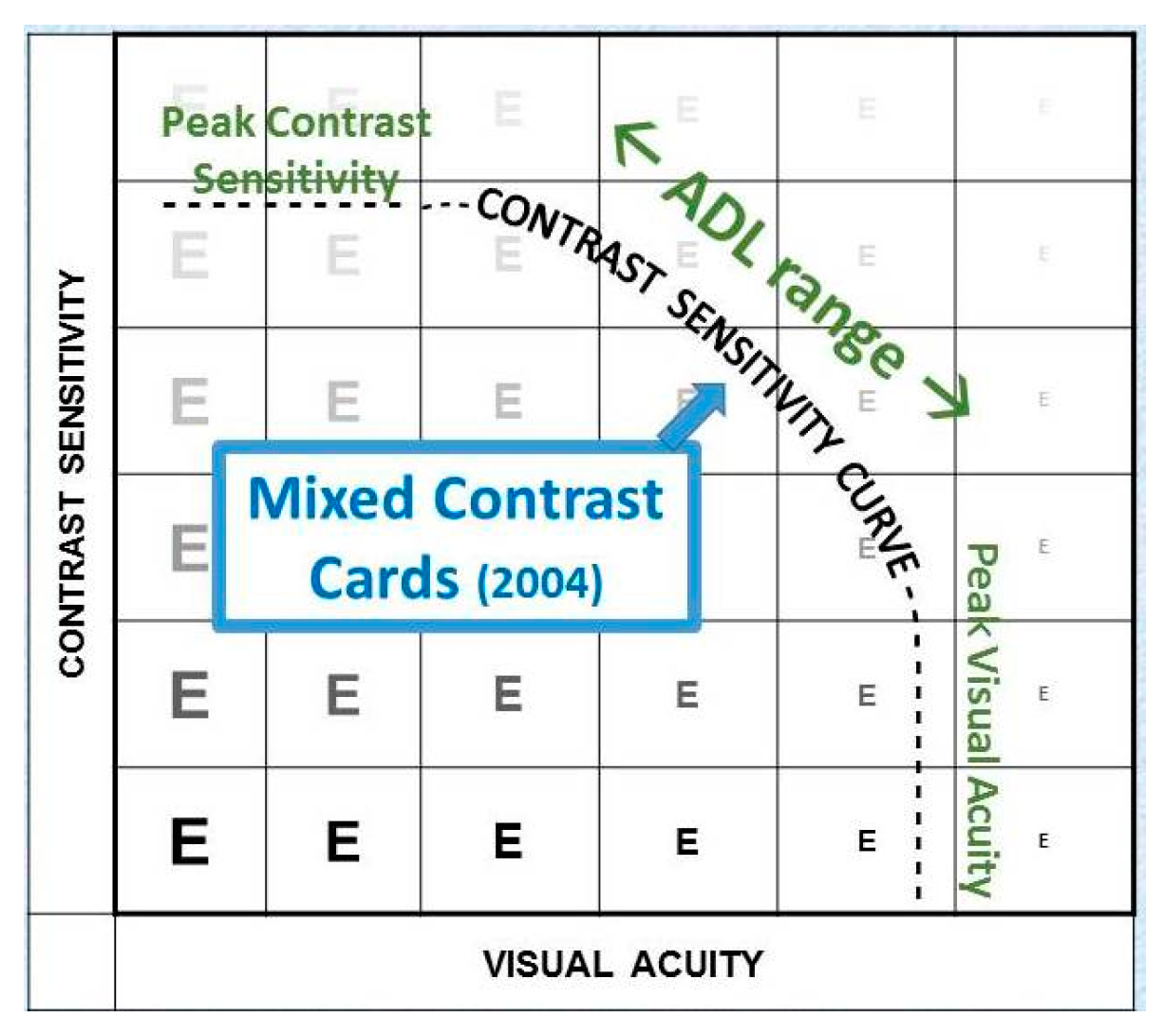
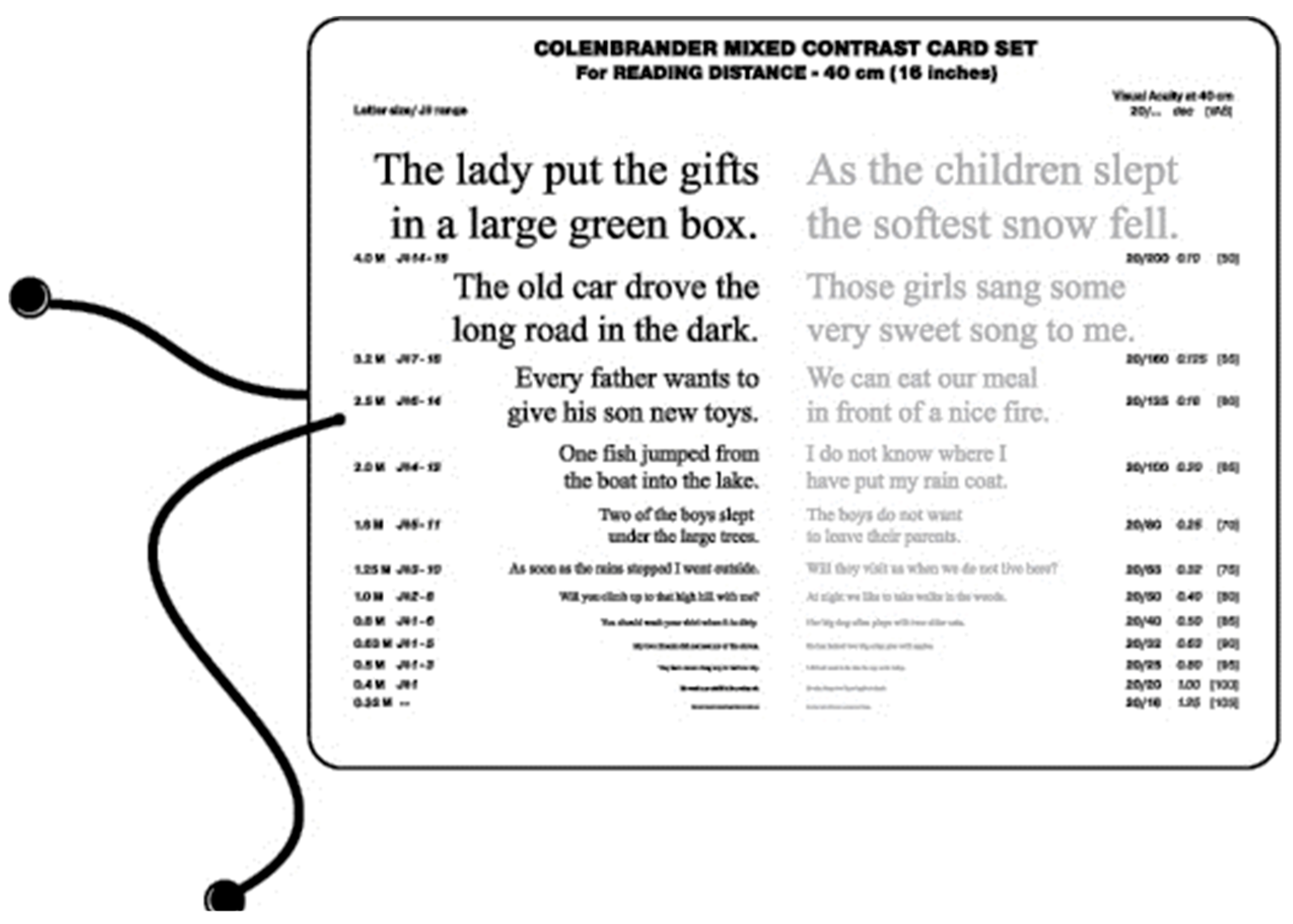
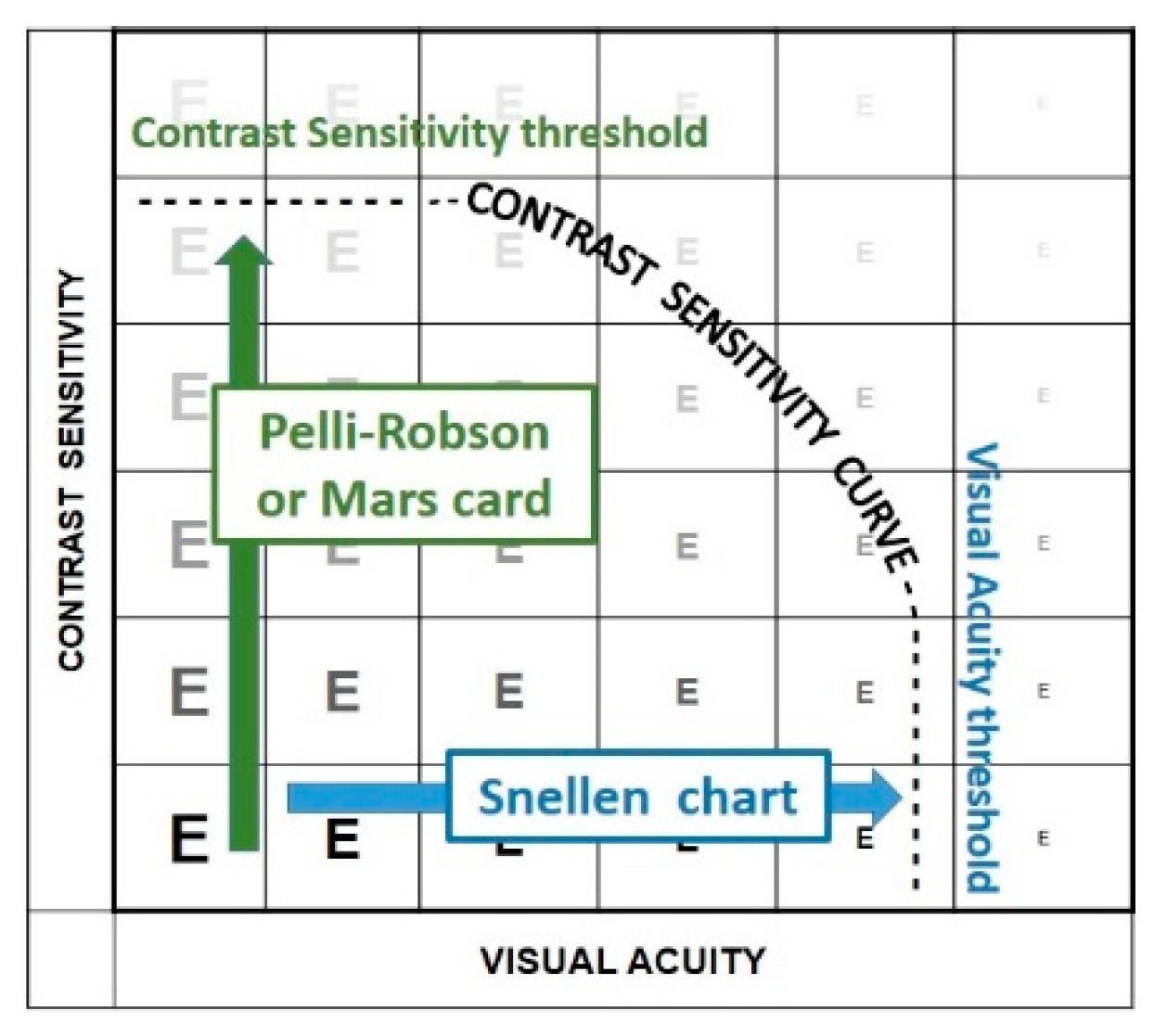
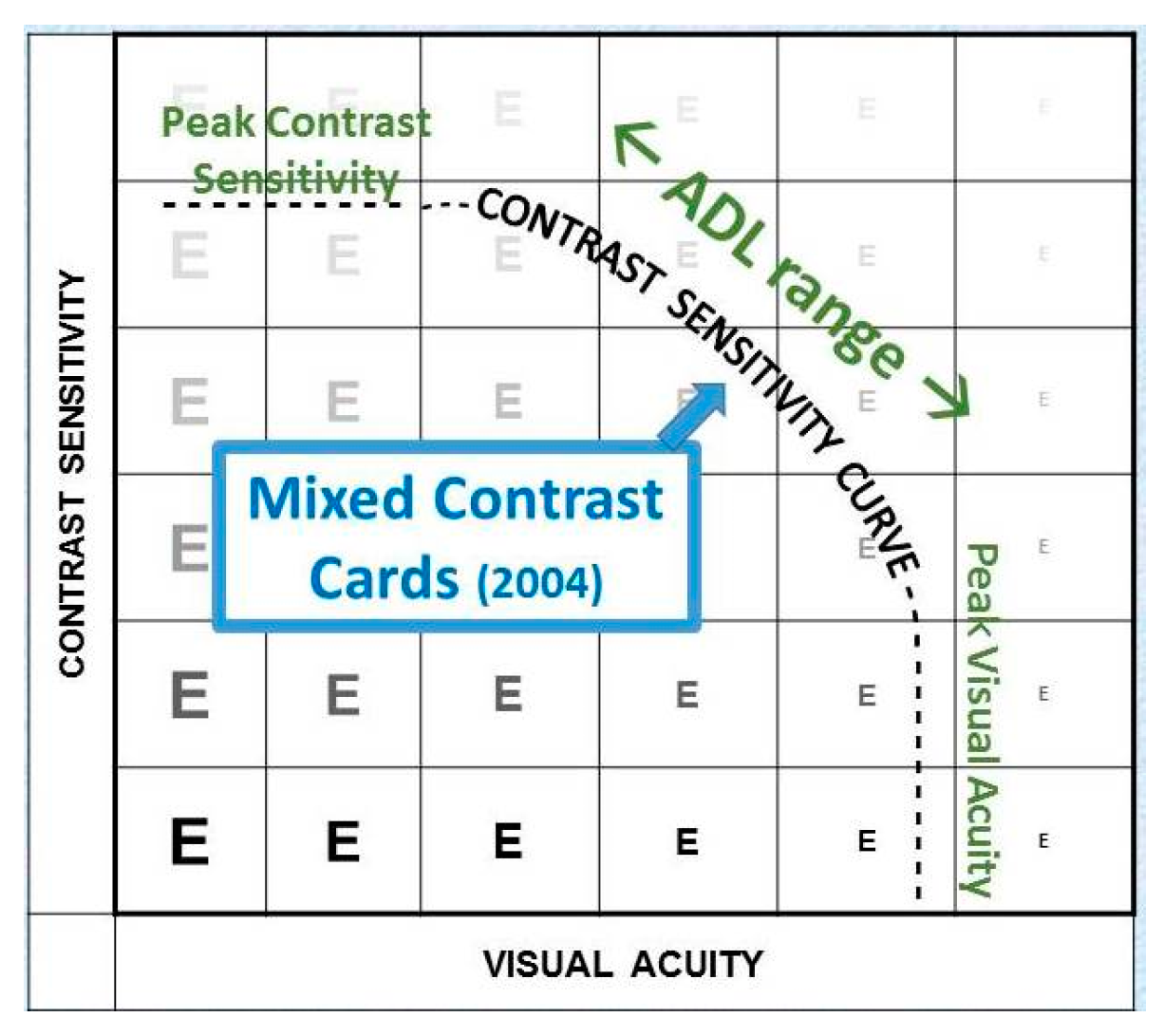
4.2. Assessment of Contrast Vision
4.3. Remediation of Reduced Contrast Vision
5. Conclusions
- Detail vision—Consider possible rehabilitation needs of anyone with <20/40 [1].
- Surround vision—Requires patient education, rather than devices.
- Contrast vision—Requires patient education and environmental modifications.
Conflicts of Interest
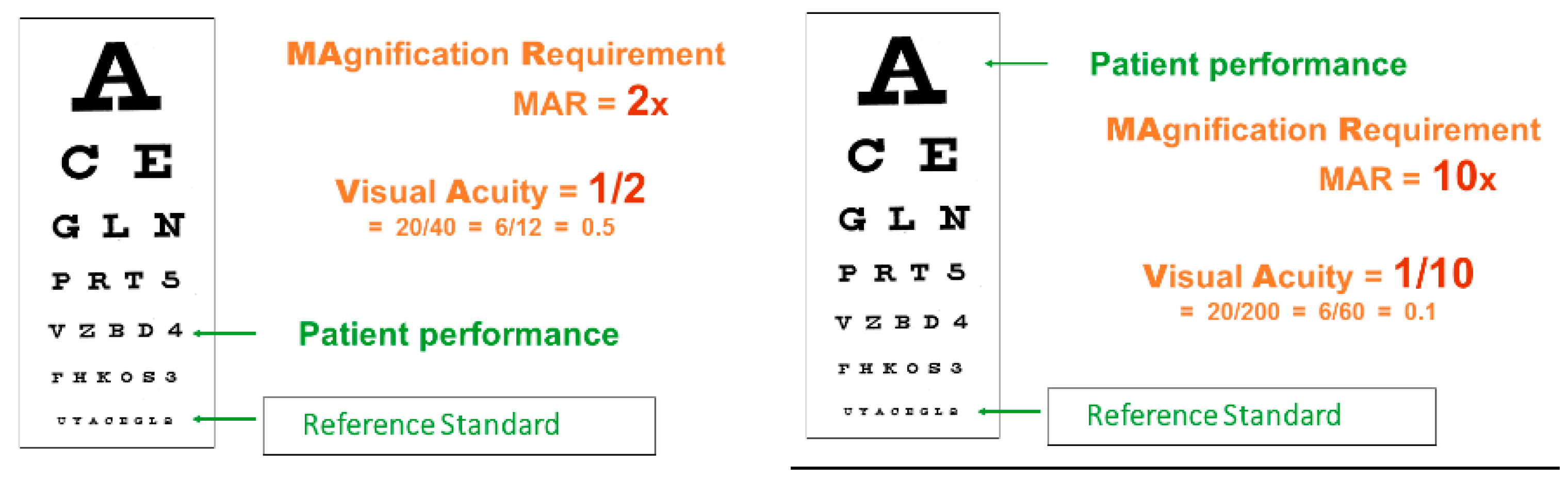
Appendix A. Measuring Detail Vision
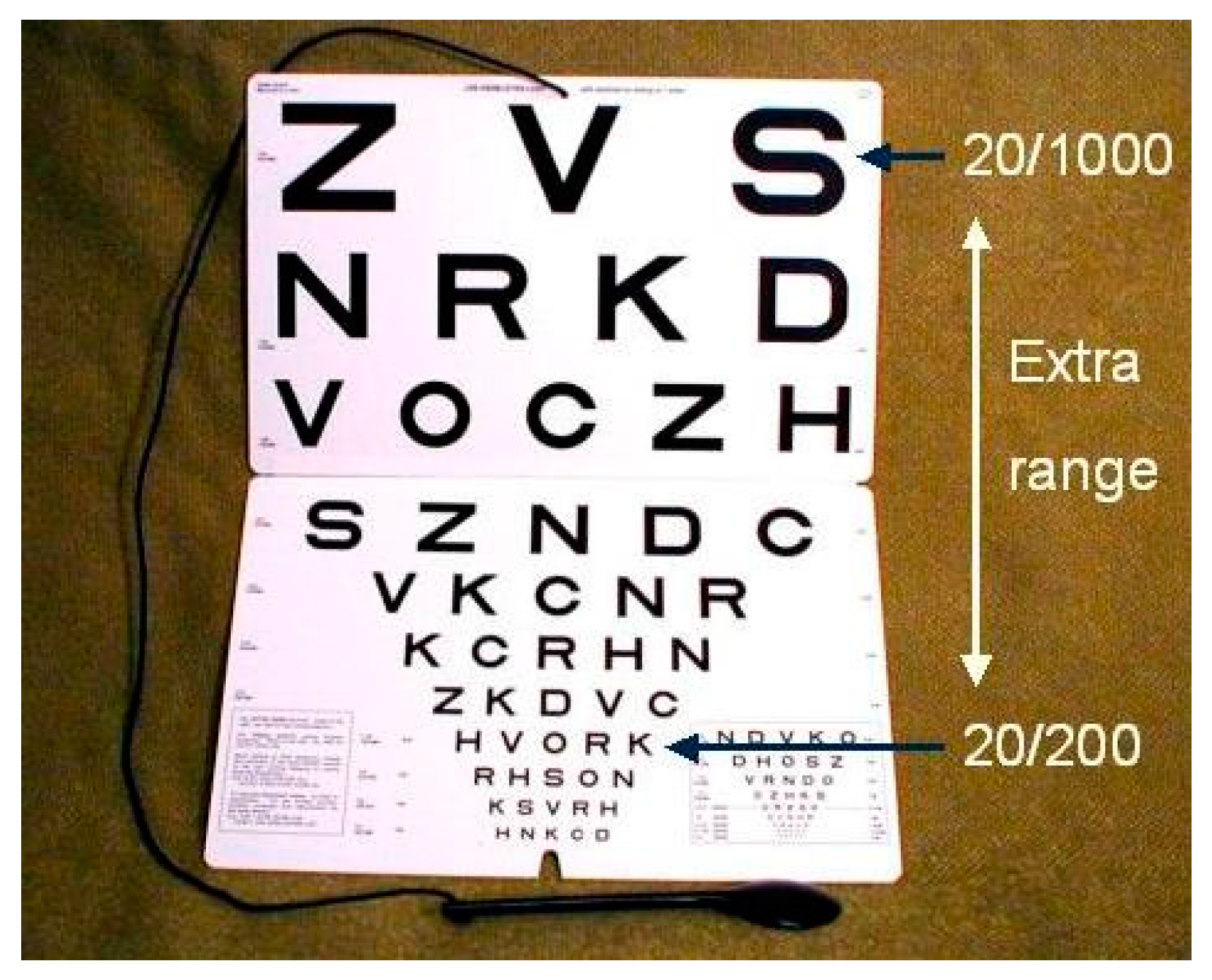
Appendix A.1. Letter Chart Acuity
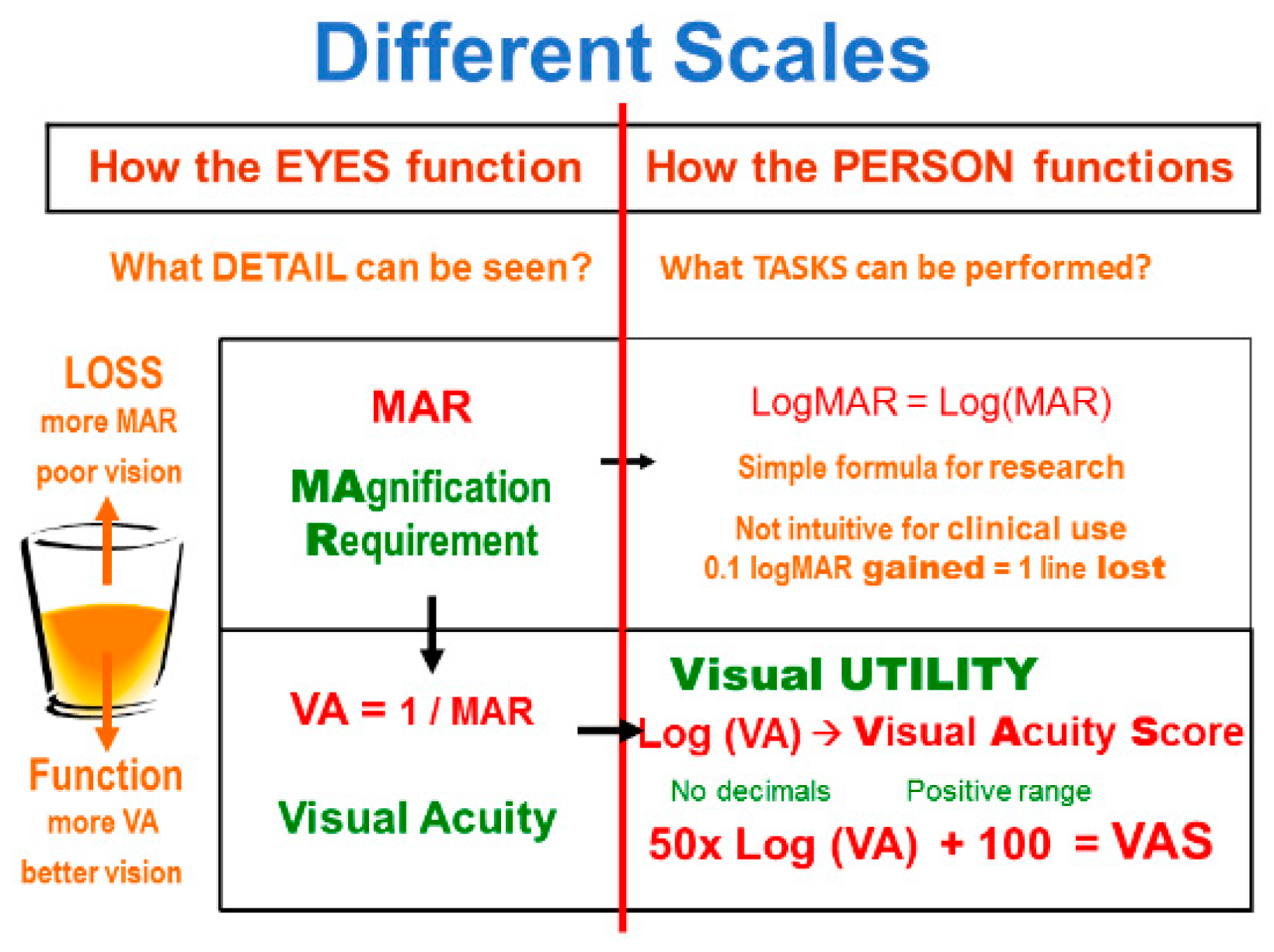
Appendix A.2. Measurement Scales
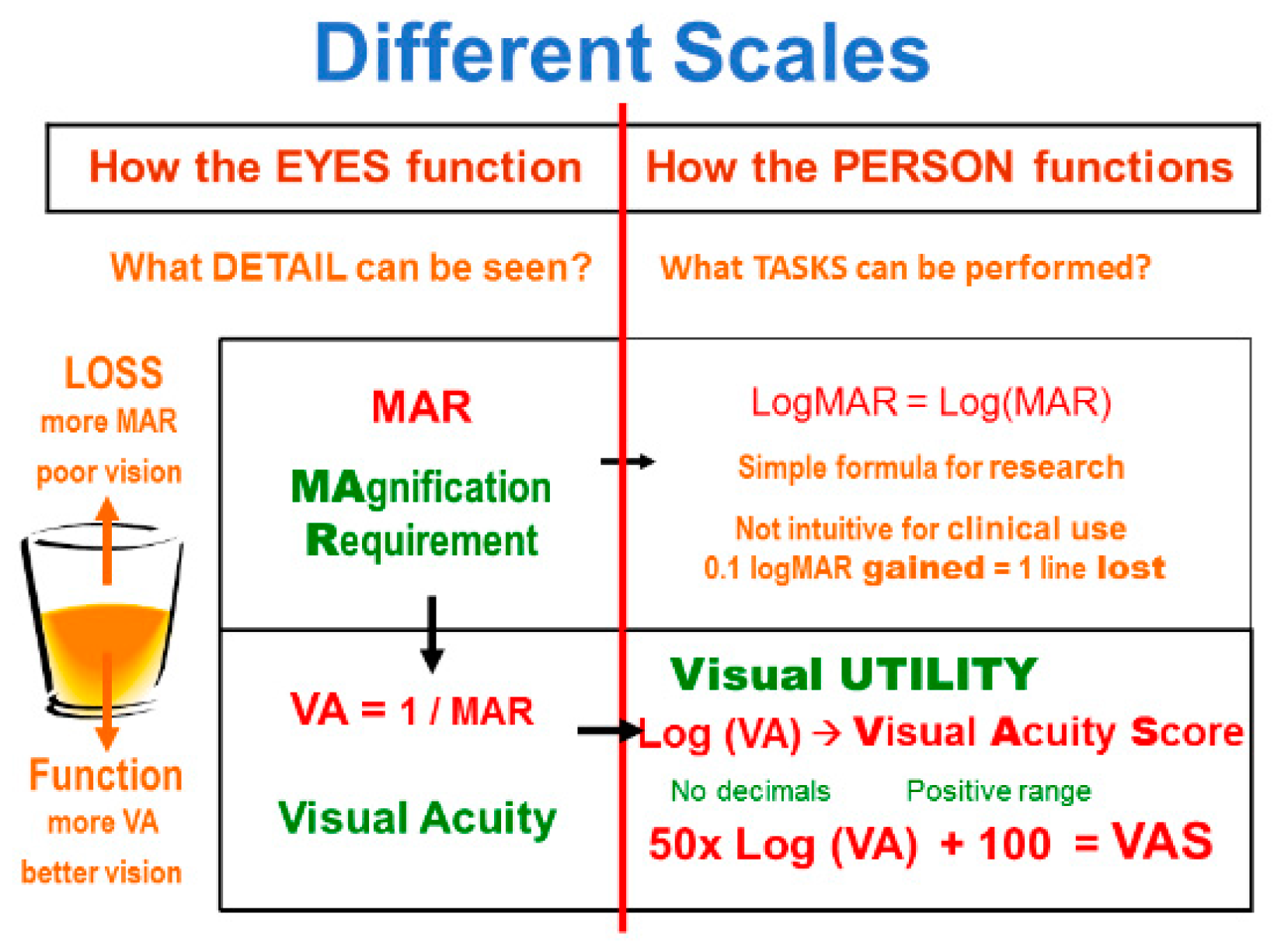
Appendix A.3. Logarithmic Progression
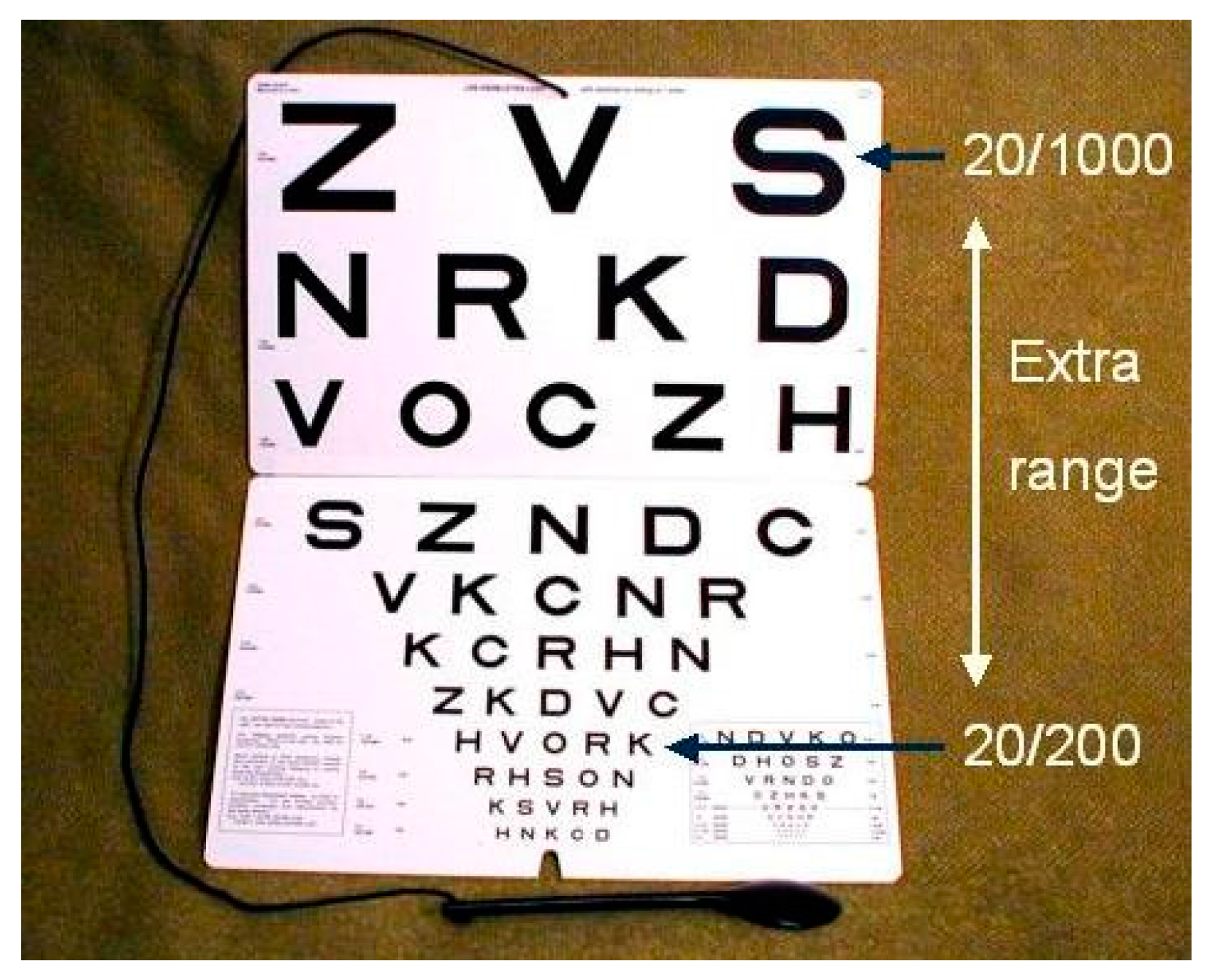
Appendix A.4. 1-m Chart
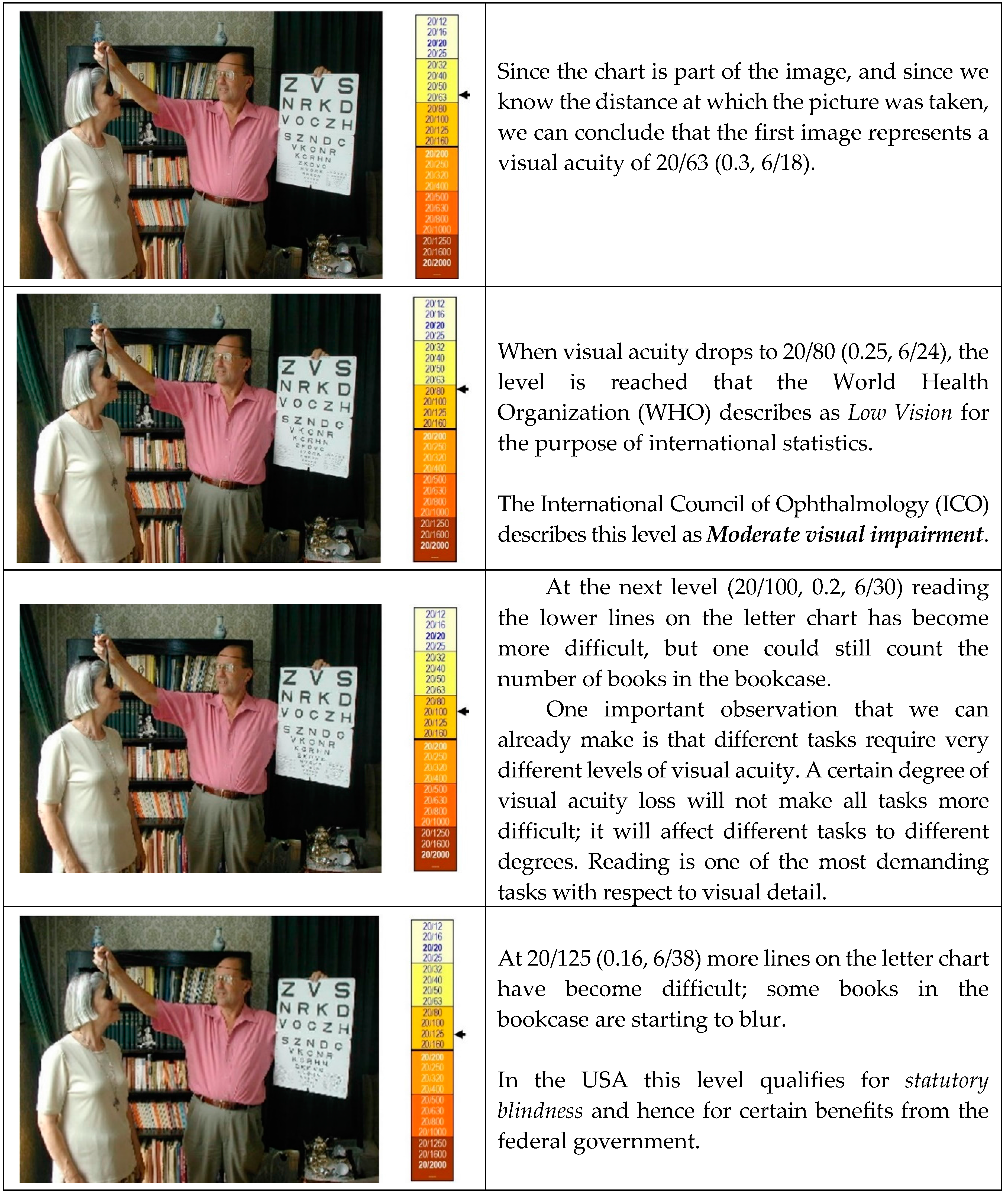
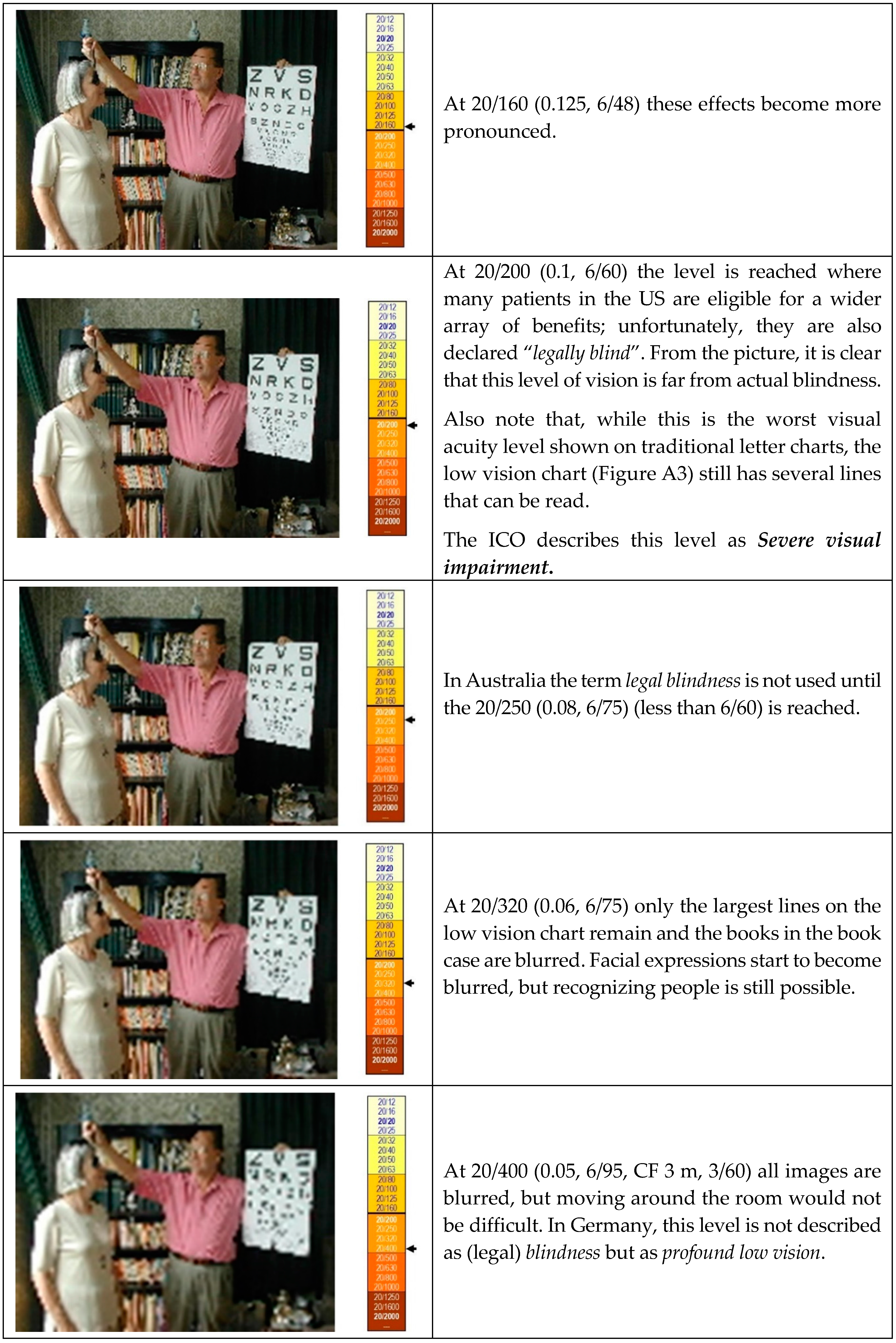
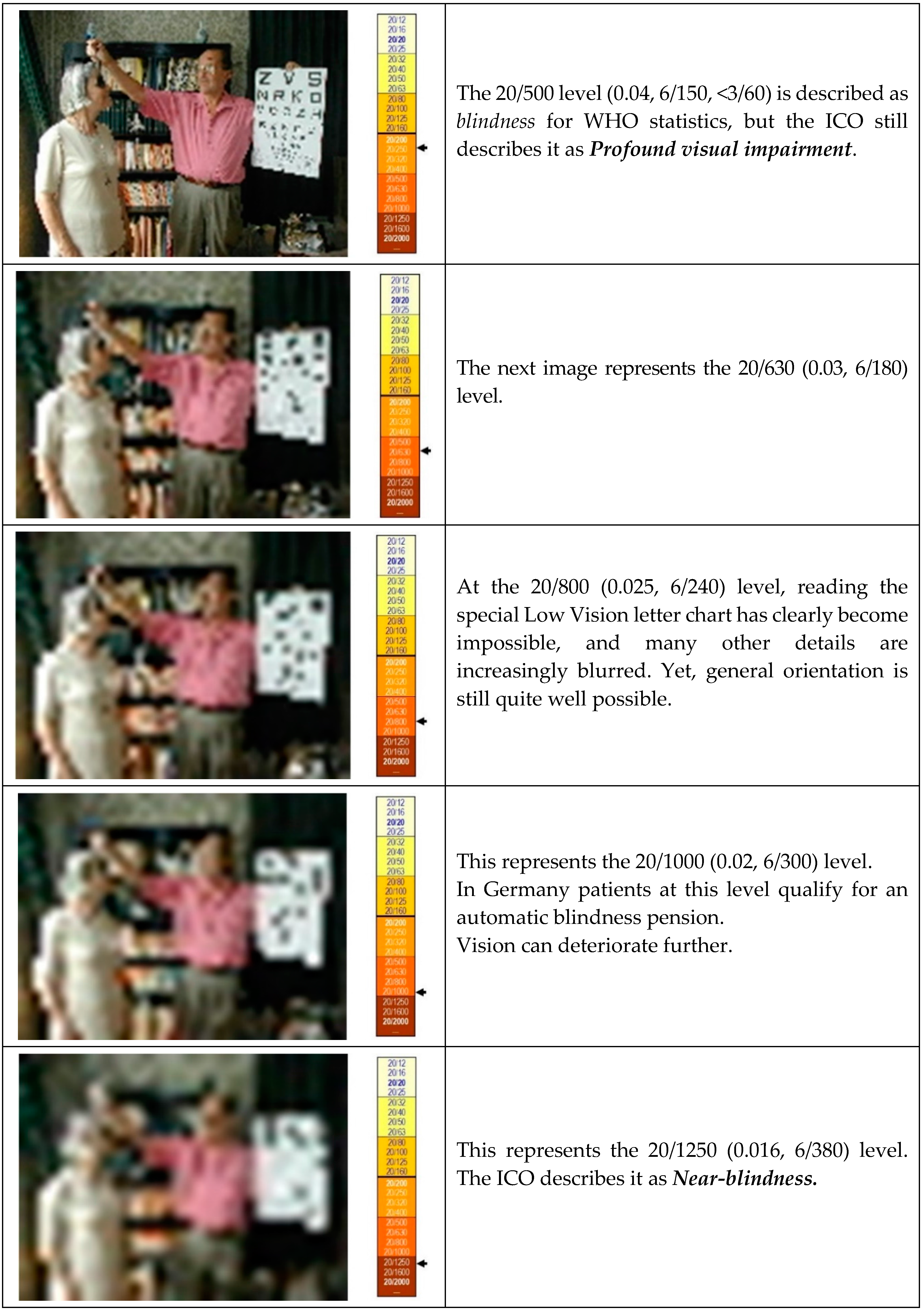
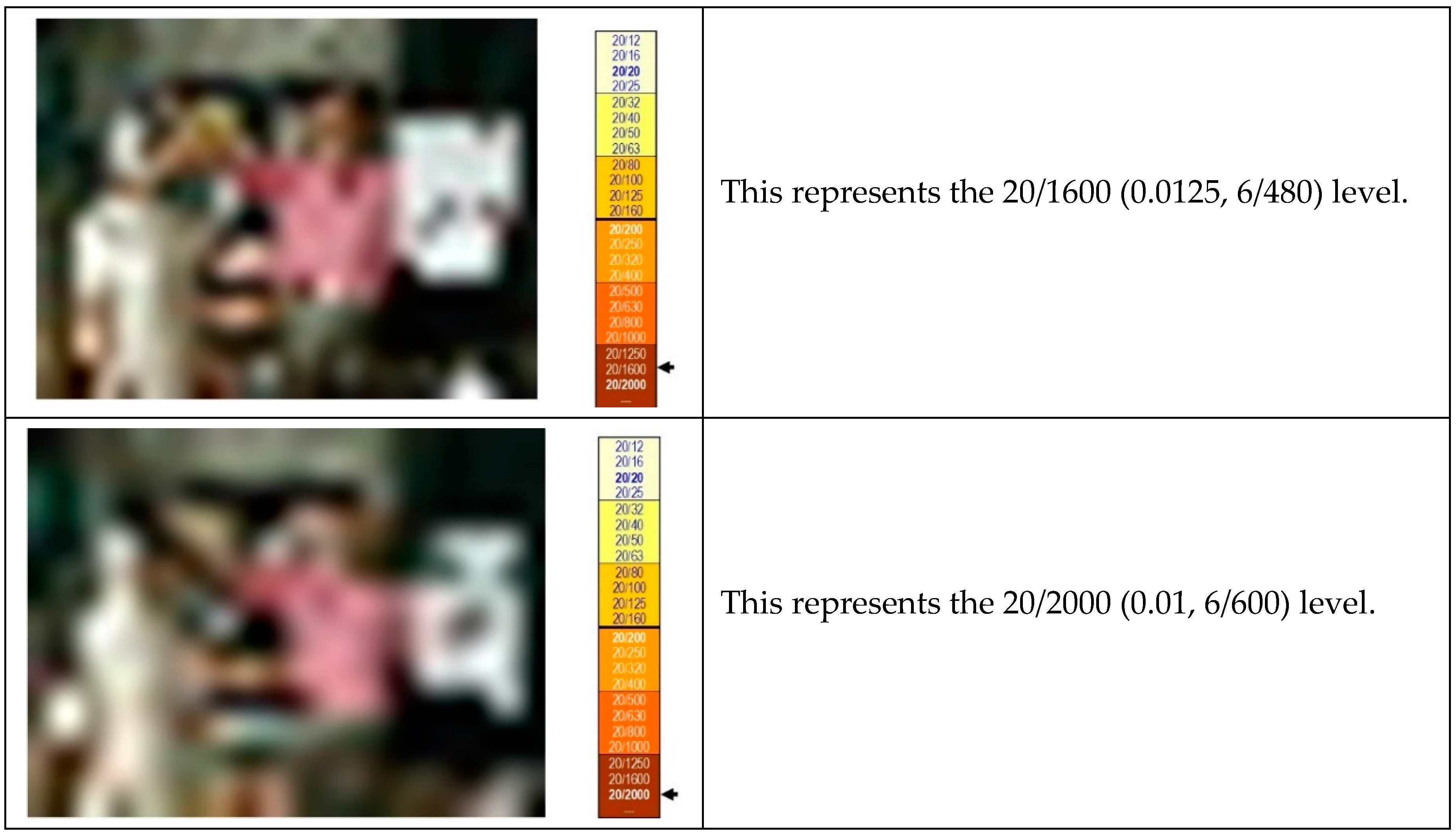
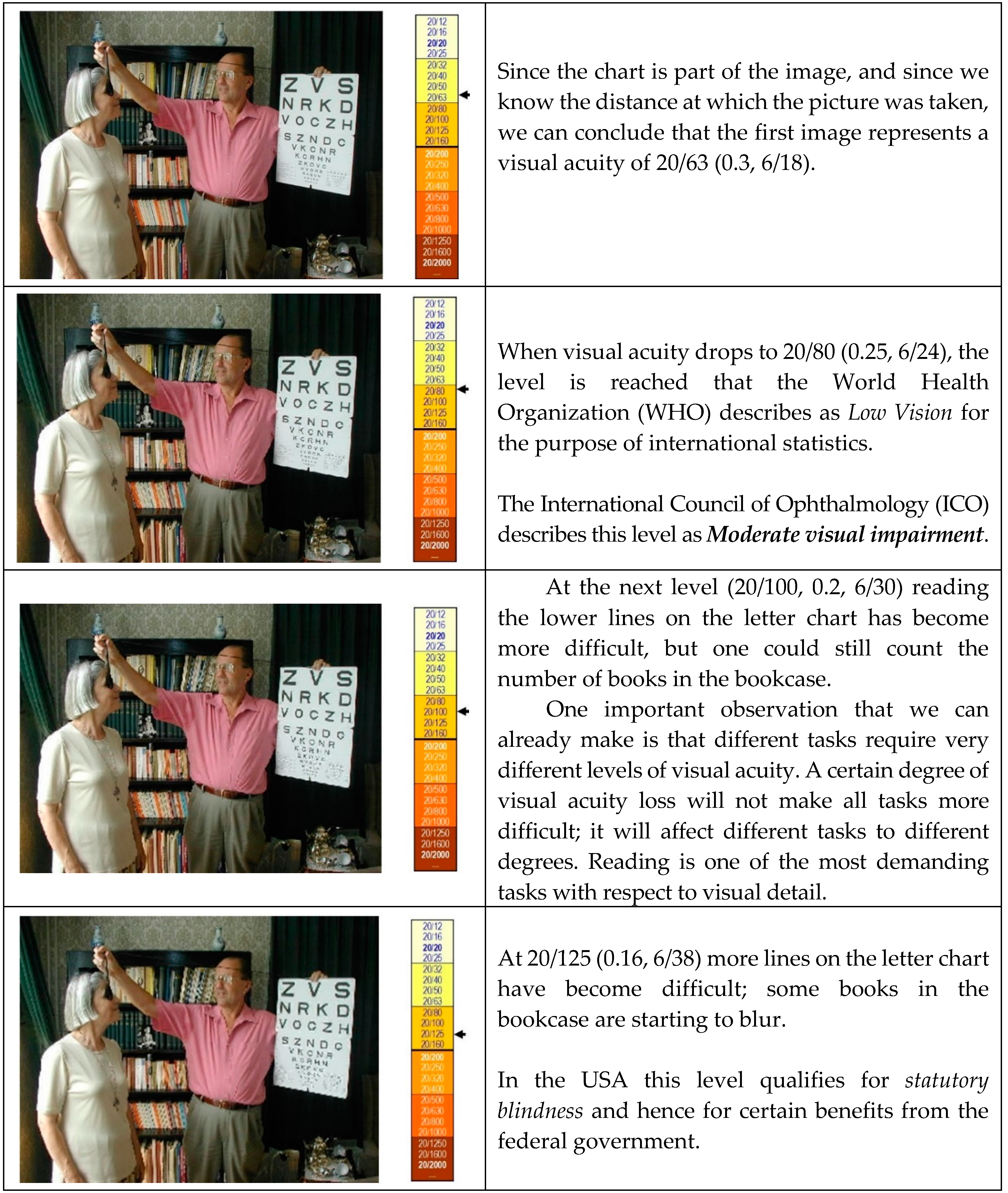
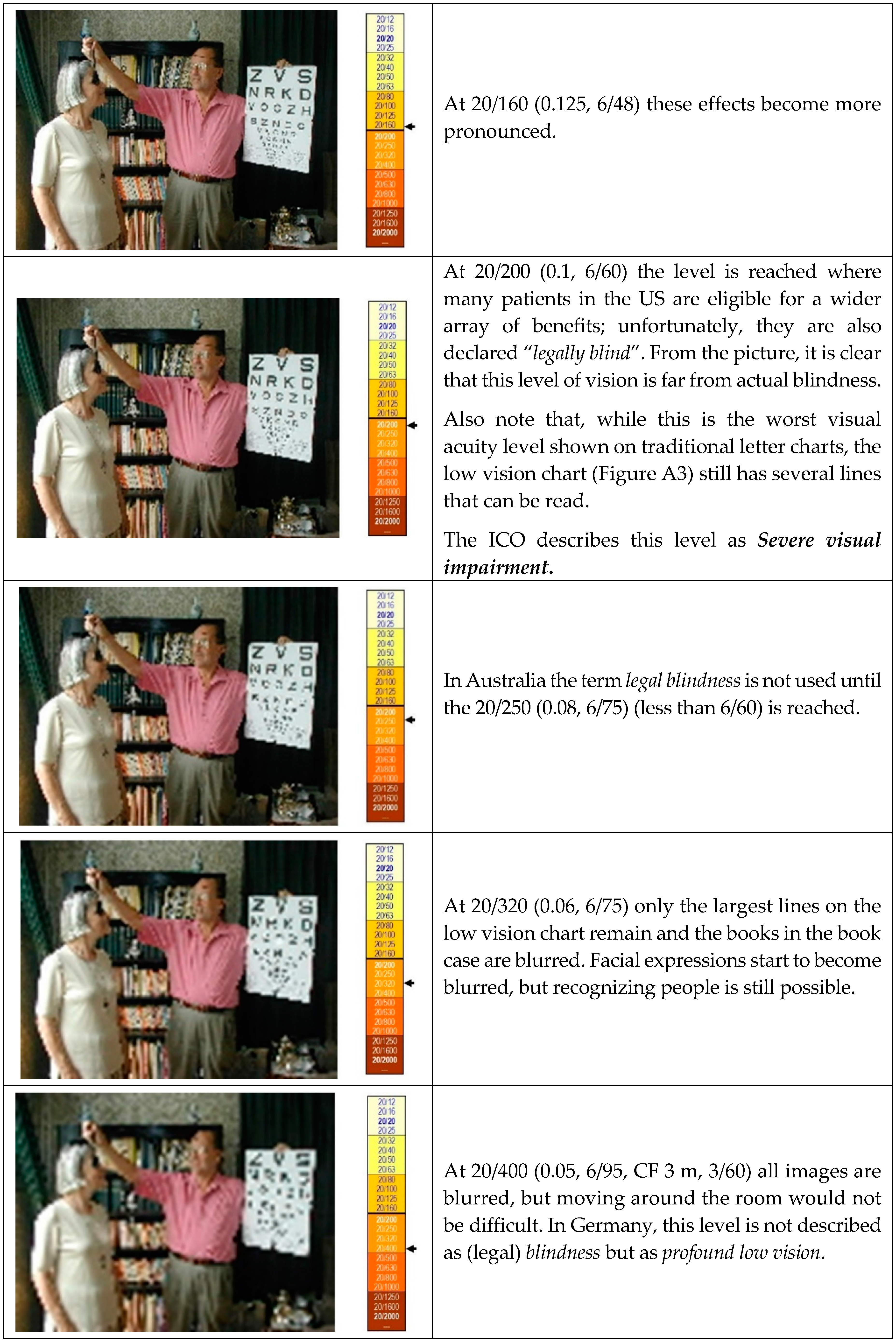
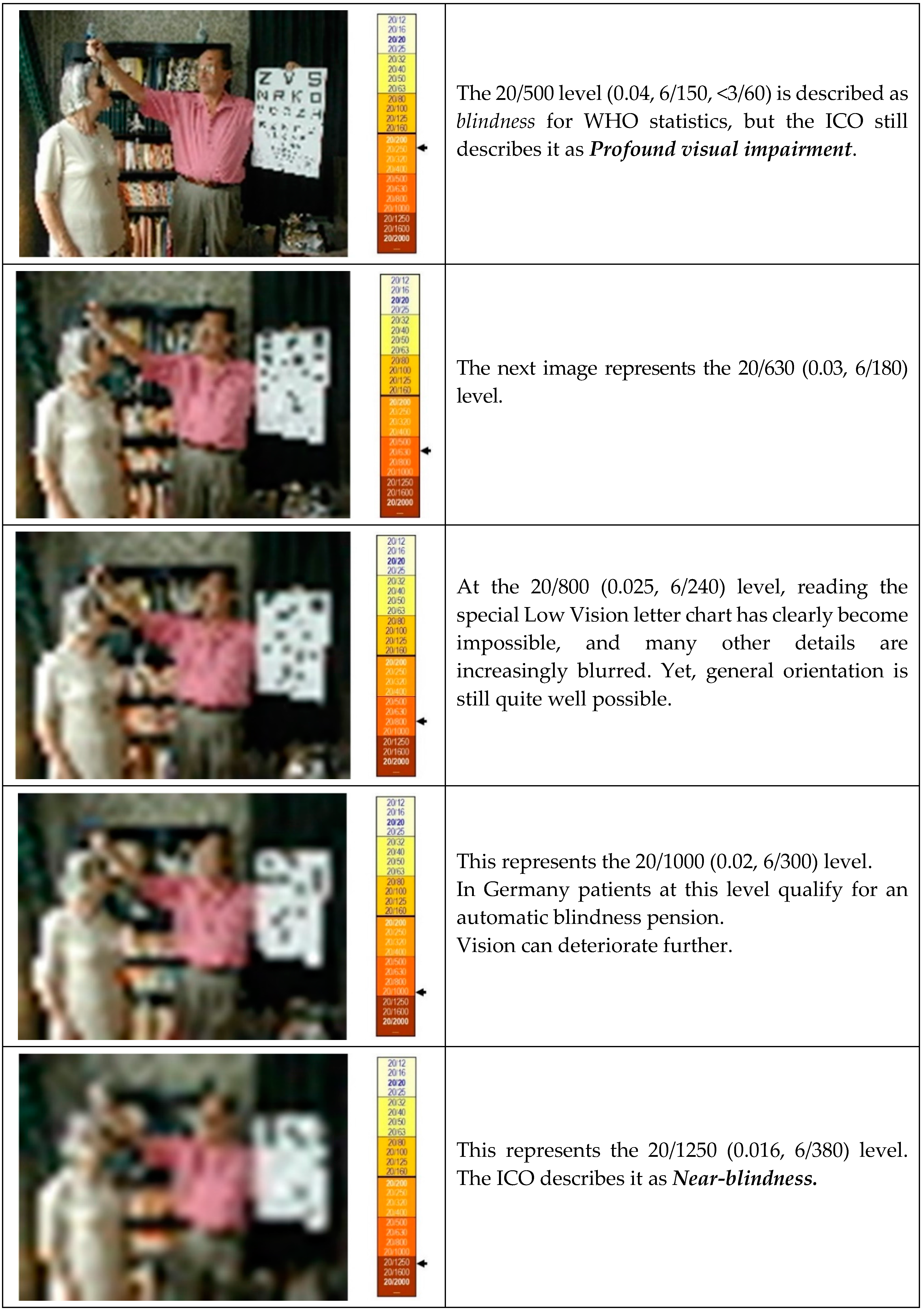
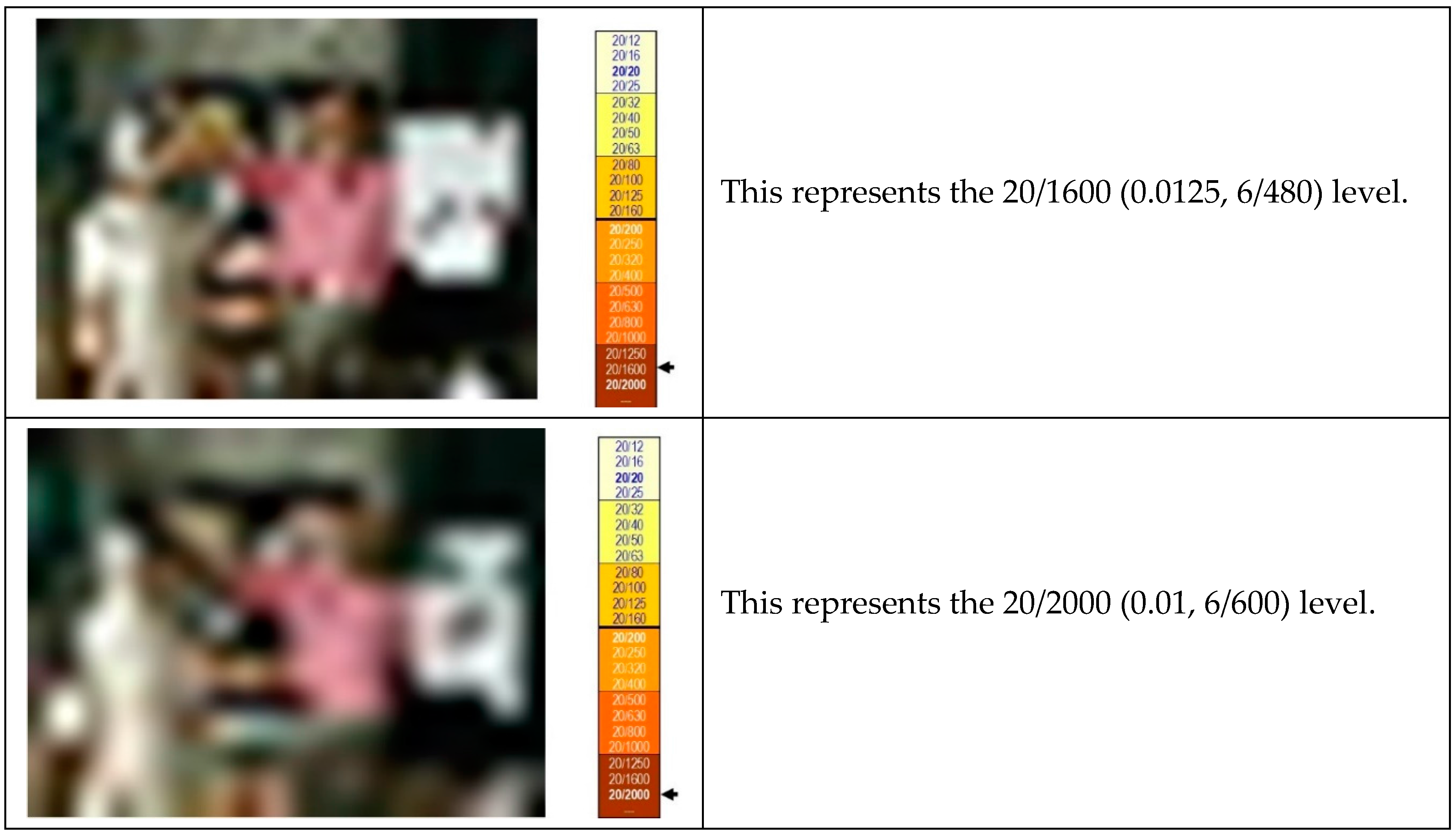
Appendix B. Samples of Detail Vision
References
- American Academy of Ophthalmology. Preferred Practice Pattern (PPP) for Vision Rehabilitation. 2017. Available online: https://www.aao.org/preferred-practice-pattern/vision-rehabilitation-ppp-2017 (accessed on 22 January 2018).
- Colenbrander, A. Assesment and Rehabilitation of Functional Vision. Report for ICO and ISLRR. Acta Ophthalmol. 2010, 88, 161–162. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Ophthalmology. The Academy’s Initiative in Vision Rehabilitation. Available online: https://www.aao.org/low-vision-and-vision-rehab (accessed on 22 January 2018).
- Colenbrander, A. The Historical Evolution of Visual Acuity Measurement. Vis. Impair. Res. 2008, 10, 57–66. [Google Scholar] [CrossRef]
- Snellen, H. Optotypi Ad Visum Determinandum, Dutch Edition ed; Weyers: Utrecht, The Netherlands, 1862; Multiple subsequent editions in many languages, Snellen’s text is still used today in the Netherlands. [Google Scholar]
- Seiple, W.; Szlyk, J.P.; McMahon, T.; Pulido, J.; Fishman, G.A. Eye-movement training for reading in patients with age-related macular degeneration. Investig. Ophthalmol. Vis. Sci. 2005, 46, 2886–2896. [Google Scholar] [CrossRef] [PubMed]
- Schoessow, K.A.; Fletcher, D.C.; Schuchard, R.A. Preferred Retinal Loci Relationship to Macular Scotomas: A 10 Year Comparison. J. Vis. Impair. Blind. 2012, 106, 745–750. [Google Scholar]
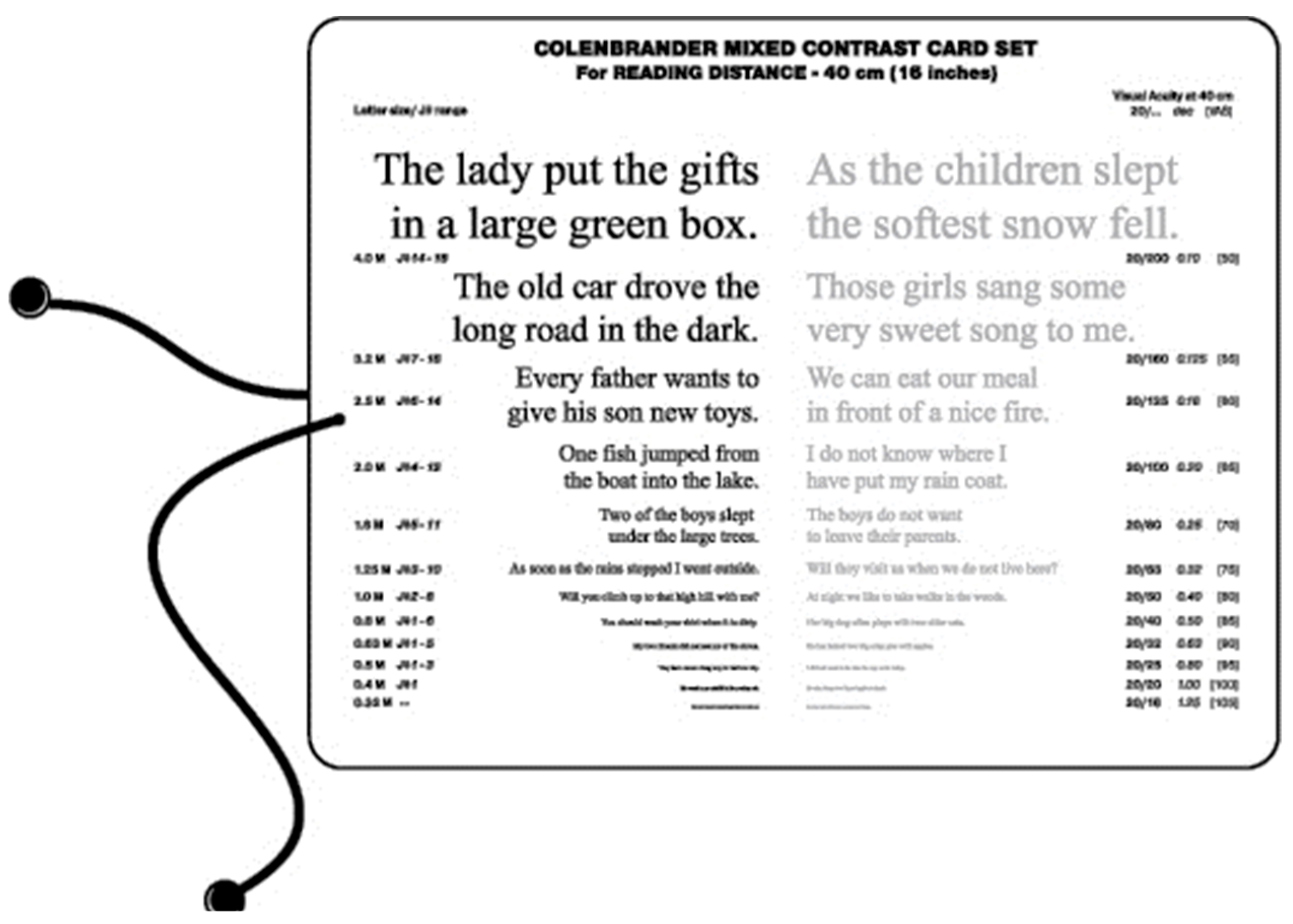
- Colenbrander, A.; Fletcher, D.C. The Mixed Contrast Reading Card, a new Screening Test for Contrast Sensitivity. In Proceedings of the International Congress Conference (Vision 2005), London, UK, 4–7 April 2005; Available online: https://www.dropbox.com/s/7daoyxdqltqecbc/V-2005%20-%20Mixed%20Contrast%20Card.pdf?dl=0 (accessed on 22 January 2018).
- Monoyer, F. Echelle typographique décimale pour mesurer l’acuité visuelle. Acad. Des Sc. Compt. Rend. 1875, 80, 1137–1138. [Google Scholar]
- International Council of Ophthalmology (ICO). Visual Standards, Aspects and Ranges of Vision Loss with emphasis on Population Surveys. April 2002. Available online: http://www.icoph.org/resources/10/Visual-Standards---Aspects-and-Ranges-of-Vision-Loss.html (accessed on 22 January 2018).
- American Medical Association. Guides to the Evaluation of Permanent Impairment, 5th ed.; Cochiarella, L., Ed.; AMA Press: Chicago, IL, USA, 2001. [Google Scholar]
- American Medical Association. Guides to the Evaluation of Permanent Impairment, 6th ed.; Rondinelli, R., Ed.; AMA Press: Chicago, IL, USA, 2007. [Google Scholar]
- Green, J. On a new series of test-letters for determining the acuteness of vision. Transact. Am. Opthalmol. Soc. 1868, 1, 68–71. [Google Scholar]
- Ferris, F.L., III; Kassoff, A.; Bresnick, G.H.; Bailey, I. New Visual Acuity Charts for Clinical Research. Am. J. Ophthalmol. 1982, 94, 91–96. [Google Scholar] [CrossRef]
- Bailey, I.L.; Lovie, J.E. New Design Principles for Visual Acuity Letter Charts. Am. J. Optom. Physiol. Opt. 1976, 53, 740–745. [Google Scholar] [CrossRef] [PubMed]




© 2018 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Colenbrander, A. Vision Rehabilitation is Part of AMD Care. Vision 2018, 2, 4. https://doi.org/10.3390/vision2010004
Colenbrander A. Vision Rehabilitation is Part of AMD Care. Vision. 2018; 2(1):4. https://doi.org/10.3390/vision2010004
Chicago/Turabian StyleColenbrander, August. 2018. "Vision Rehabilitation is Part of AMD Care" Vision 2, no. 1: 4. https://doi.org/10.3390/vision2010004
APA StyleColenbrander, A. (2018). Vision Rehabilitation is Part of AMD Care. Vision, 2(1), 4. https://doi.org/10.3390/vision2010004