
The Influence of Ankle Mobility and Foot Stability on Jumping Ability and Landing Mechanics: A Cross-Sectional Study

 ,
,  ,
,  ,
,  ,
,  ,
,  ,
,  ,
,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
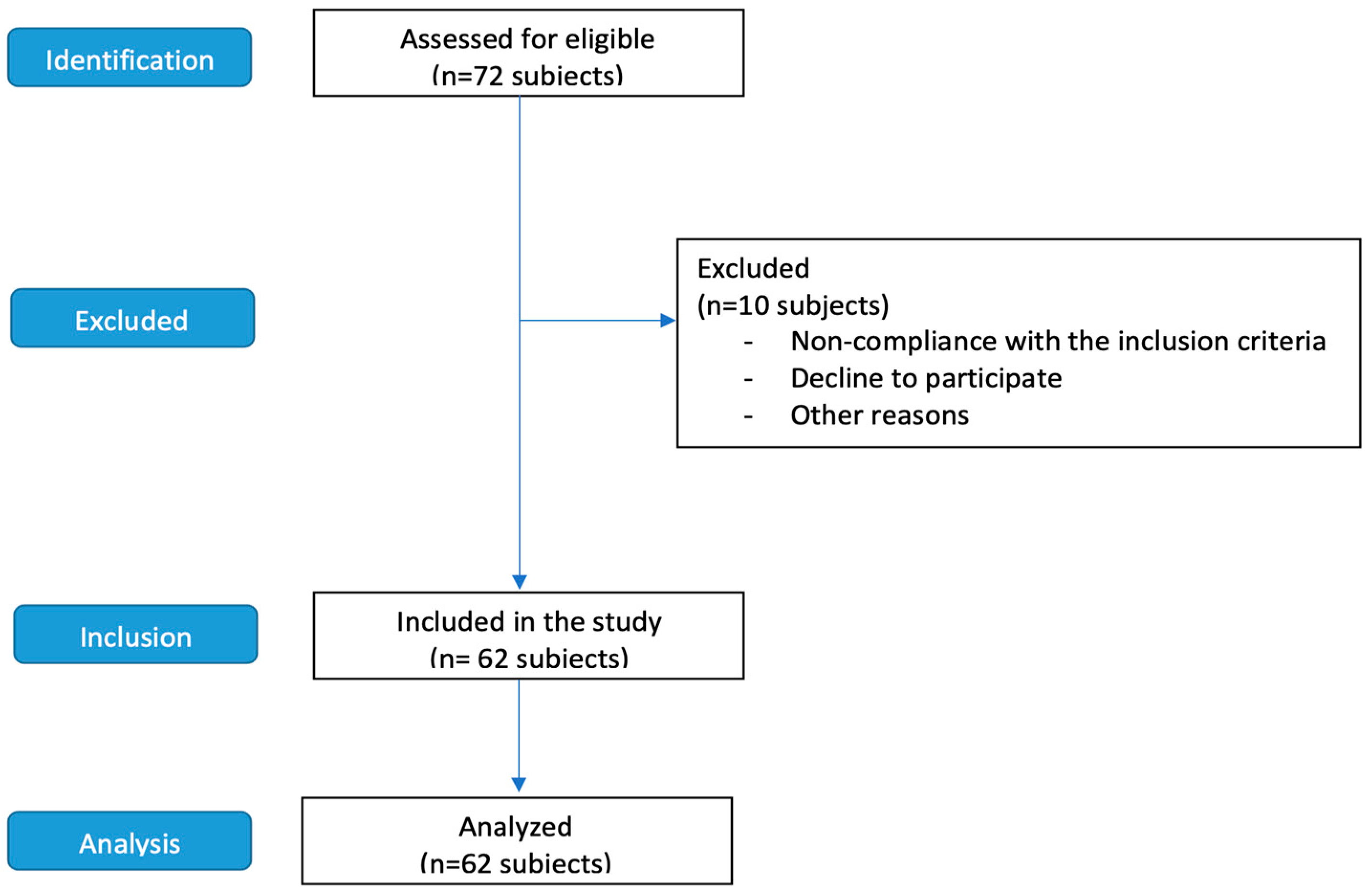
2.2. Subjects
- (a)
- Participants had no leg injuries in the past six months.
- (b)
- All participants had been playing and exercising regularly for at least six months.
- (c)
- There were no post-surgical subjects.
2.3. Procedures
2.3.1. The Measure of the Ankle Range of Motion
- -
- Range of motion (ROM°): It represents the angular excursion carried out by the segment that rotates from its starting point to its arrival point.
- -
- Angular speed (°/s): It represents the average angular velocity over the entire range of motion.
- -
- Fluency Index: An index ranging from 0 to 1 indicates the movement’s quality. The closer it is to 1, the smoother the movement. The dorsiflexion, plantar flexion, eversion, and inversion of both feet of all the subjects analyzed were evaluated on these three parameters (Figure 2).
2.3.2. Counter-Movement Jump (CMJ)
2.3.3. Specific Jump-Landing Task
2.4. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bere, T.; Kruczynski, J.; Veintimilla, N.; Hamu, Y.; Bahr, R. Injury risk is low among world-class volleyball players: 4-year data from the FIVB Injury Surveillance System. Br. J. Sports Med. 2015, 49, 1132–1137. [Google Scholar] [CrossRef] [PubMed]
- Bahr, R.; Karlsen, R.; Lian, O.; Ovrebo, R.V. Incidence and mechanisms of acute ankle inversion injuries in volleyball. A retrospective cohort study. Am. J. Sports Med. 1994, 22, 595–600. [Google Scholar] [CrossRef] [PubMed]
- Bahr, R.; Bahr, I.A. Incidence of acute volleyball injuries: A prospective cohort study of injury mechanisms and risk factors. Scand. J. Med. Sci. Sports 1997, 7, 166–171. [Google Scholar] [CrossRef]
- Akbari, H.; Shimokochi, Y.; Sheikhi, B. Ankle dorsiflexion range of motion and landing postures during a soccer-specific task. PLoS ONE 2023, 18, e0283150. [Google Scholar] [CrossRef] [PubMed]
- Ungureanu, A.N.; Beratto, L.; Daga, F.A.; Boccia, G.; Lupo, C.; Brustio, P.R. Changes in anthropometric and fitness profile of Italian regional academy rugby union players. Biol. Sport 2022, 39, 621–628. [Google Scholar] [CrossRef] [PubMed]
- Asperti, A.M.; Fernandes, T.L.; Pedrinelli, A.; Hernandez, A.J. Sports Injuries among Amateur Athletes at a Brazilian University. Acta Ortop. Bras. 2017, 25, 93–98. [Google Scholar] [CrossRef]
- Indriethadottir, M.H.; Sveinsson, T.; Magnusson, K.; Arngrimsson, S.A.; Johannsson, E. Prevalence of sport injuries, sport participation and drop out due to injury in young adults. Laeknabladid 2015, 101, 451–456. [Google Scholar] [CrossRef]
- Boden, B.P.; Torg, J.S.; Knowles, S.B.; Hewett, T.E. Video analysis of anterior cruciate ligament injury: Abnormalities in hip and ankle kinematics. Am. J. Sports Med. 2009, 37, 252–259. [Google Scholar] [CrossRef]
- Carlson, V.R.; Sheehan, F.T.; Boden, B.P. Video Analysis of Anterior Cruciate Ligament (ACL) Injuries: A Systematic Review. JBJS Rev. 2016, 4, e5. [Google Scholar] [CrossRef]
- Sahin, N.; Bianco, A.; Patti, A.; Paoli, A.; Palma, A.; Ersoz, G. Evaluation of knee joint proprioception and balance of young female volleyball players: A pilot study. J. Phys. Ther. Sci. 2015, 27, 437–440. [Google Scholar] [CrossRef]
- Cejudo, A. Lower Extremity Flexibility Profile in Basketball Players: Gender Differences and Injury Risk Identification. Int. J. Environ. Res. Public Health 2021, 18, 11956. [Google Scholar] [CrossRef] [PubMed]
- Malloy, P.; Morgan, A.; Meinerz, C.; Geiser, C.; Kipp, K. The association of dorsiflexion flexibility on knee kinematics and kinetics during a drop vertical jump in healthy female athletes. Knee Surg. Sports Traumatol. Arthrosc. 2015, 23, 3550–3555. [Google Scholar] [CrossRef] [PubMed]
- Hagins, M.; Pappas, E.; Kremenic, I.; Orishimo, K.F.; Rundle, A. The effect of an inclined landing surface on biomechanical variables during a jumping task. Clin. Biomech. 2007, 22, 1030–1036. [Google Scholar] [CrossRef] [PubMed]
- Taylor, J.B.; Wright, E.S.; Waxman, J.P.; Schmitz, R.J.; Groves, J.D.; Shultz, S.J. Ankle Dorsiflexion Affects Hip and Knee Biomechanics During Landing. Sports Health 2022, 14, 328–335. [Google Scholar] [CrossRef]
- Stacoff, A.; Steger, J.; Stussi, E.; Reinschmidt, C. Lateral stability in sideward cutting movements. Med. Sci. Sports Exerc. 1996, 28, 350–358. [Google Scholar] [CrossRef]
- Braun, B.L. Effects of ankle sprain in a general clinic population 6 to 18 months after medical evaluation. Arch. Fam. Med. 1999, 8, 143–148. [Google Scholar] [CrossRef]
- Simpson, J.D.; Stewart, E.M.; Macias, D.M.; Chander, H.; Knight, A.C. Individuals with chronic ankle instability exhibit dynamic postural stability deficits and altered unilateral landing biomechanics: A systematic review. Phys. Ther. Sport 2019, 37, 210–219. [Google Scholar] [CrossRef]
- Driller, M.W.; Overmayer, R.G. The effects of tissue flossing on ankle range of motion and jump performance. Phys. Ther. Sport 2017, 25, 20–24. [Google Scholar] [CrossRef]
- Rabin, A.; Einstein, O.; Kozol, Z. The association of visually-assessed quality of movement during jump-landing with ankle dorsiflexion range-of-motion and hip abductor muscle strength among healthy female athletes. Phys. Ther. Sport 2018, 31, 35–41. [Google Scholar] [CrossRef]
- Grabow, L.; Young, J.D.; Byrne, J.M.; Granacher, U.; Behm, D.G. Unilateral Rolling of the Foot did not Affect Non-Local Range of Motion or Balance. J. Sports Sci. Med. 2017, 16, 209–218. [Google Scholar]
- Cuschieri, S. The STROBE guidelines. Saudi J. Anaesth. 2019, 13, S31–S34. [Google Scholar] [CrossRef] [PubMed]
- Bianco, A.; Patti, A.; Bellafiore, M.; Battaglia, G.; Sahin, F.N.; Paoli, A.; Cataldo, M.C.; Mammina, C.; Palma, A. Group fitness activities for the elderly: An innovative approach to reduce falls and injuries. Aging Clin. Exp. Res. 2014, 26, 147–152. [Google Scholar] [CrossRef]
- Kroger, I.; Mussig, J.; Brand, A.; Patzold, R.; Wackerle, H.; Klopfer-Kramer, I.; Augat, P. Recovery of gait and function during the first six months after tibial shaft fractures. Gait Posture 2022, 91, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Hespanhol Junior, L.C.; de Carvalho, A.C.; Costa, L.O.; Lopes, A.D. Lower limb alignment characteristics are not associated with running injuries in runners: Prospective cohort study. Eur. J. Sport Sci. 2016, 16, 1137–1144. [Google Scholar] [CrossRef]
- Baldazzi, A.; Molinaro, L.; Taborri, J.; Margheritini, F.; Rossi, S.; Bergamini, E. Reliability of wearable sensors-based parameters for the assessment of knee stability. PLoS ONE 2022, 17, e0274817. [Google Scholar] [CrossRef]
- Ahmadian, N.; Nazarahari, M.; Whittaker, J.L.; Rouhani, H. Quantification of Triple Single-Leg Hop Test Temporospatial Parameters: A Validated Method using Body-Worn Sensors for Functional Evaluation after Knee Injury. Sensors 2020, 20, 3464. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.C.; Washell, B.R.; Aini, M.F.; Brown, S.; Hall, M.C. Effects of Static Stretching and Foam Rolling on Ankle Dorsiflexion Range of Motion. Med. Sci. Sports Exerc. 2019, 51, 1752–1758. [Google Scholar] [CrossRef]
- Montalvo, S.; Gonzalez, M.P.; Dietze-Hermosa, M.S.; Eggleston, J.D.; Dorgo, S. Common Vertical Jump and Reactive Strength Index Measuring Devices: A Validity and Reliability Analysis. J. Strength Cond. Res. 2021, 35, 1234–1243. [Google Scholar] [CrossRef]
- Glatthorn, J.F.; Gouge, S.; Nussbaumer, S.; Stauffacher, S.; Impellizzeri, F.M.; Maffiuletti, N.A. Validity and reliability of Optojump photoelectric cells for estimating vertical jump height. J. Strength Cond. Res. 2011, 25, 556–560. [Google Scholar] [CrossRef]
- Patti, A.; Giustino, V.; Hirose, N.; Messina, G.; Cataldi, S.; Grigoli, G.; Marchese, A.; Mule, G.; Drid, P.; Palma, A.; et al. Effects of an experimental short-time high-intensity warm-up on explosive muscle strength performance in soccer players: A pilot study. Front. Physiol. 2022, 13, 984305. [Google Scholar] [CrossRef]
- Butler, R.J.; Russell, M.E.; Queen, R. Effect of soccer footwear on landing mechanics. Scand. J. Med. Sci. Sports 2014, 24, 129–135. [Google Scholar] [CrossRef]
- Watabe, T.; Takabayashi, T.; Tokunaga, Y.; Kubo, M. Copers adopt an altered dynamic postural control compared to individuals with chronic ankle instability and controls in unanticipated single-leg landing. Gait Posture 2022, 92, 378–382. [Google Scholar] [CrossRef]
- Fransz, D.P.; Huurnink, A.; de Boode, V.A.; Kingma, I.; van Dieen, J.H. Time to stabilization in single leg drop jump landings: An examination of calculation methods and assessment of differences in sample rate, filter settings and trial length on outcome values. Gait Posture 2015, 41, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Patti, A.; Bianco, A.; Messina, G.; Iovane, A.; Alesi, M.; Pepi, A.; Palma, A. Evaluation of podalic support and monitoring of balance control in children with and without dyslexia: A pilot study. Sustainability 2020, 12, 1191. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Taylor and Francis: Hoboken, NJ, USA, 2013. [Google Scholar]
- Donovan, L.; Hertel, J. A new paradigm for rehabilitation of patients with chronic ankle instability. Physician Sportsmed. 2012, 40, 41–51. [Google Scholar] [CrossRef]
- Patti, A.; Bianco, A.; Sahin, N.; Sekulic, D.; Paoli, A.; Iovane, A.; Messina, G.; Gagey, P.M.; Palma, A. Postural control and balance in a cohort of healthy people living in Europe: An observational study. Medicine 2018, 97, e13835. [Google Scholar] [CrossRef] [PubMed]
- Scoppa, F.; Capra, R.; Gallamini, M.; Shiffer, R. Clinical stabilometry standardization: Basic definitions—acquisition interval—sampling frequency. Gait Posture 2013, 37, 290–292. [Google Scholar] [CrossRef]
- Brown, C.; Padua, D.; Marshall, S.W.; Guskiewicz, K. Individuals with mechanical ankle instability exhibit different motion patterns than those with functional ankle instability and ankle sprain copers. Clin. Biomech. 2008, 23, 822–831. [Google Scholar] [CrossRef]
- Han, S.; Lee, H.; Son, S.J.; Hopkins, J.T. Effect of varied dorsiflexion range of motion on landing biomechanics in chronic ankle instability. Scand. J. Med. Sci. Sports 2023, 33, 1125–1134. [Google Scholar] [CrossRef]
- Caulfield, B.M.; Garrett, M. Functional instability of the ankle: Differences in patterns of ankle and knee movement prior to and post landing in a single leg jump. Int. J. Sports Med. 2002, 23, 64–68. [Google Scholar] [CrossRef]
- Doherty, C.; Bleakley, C.; Hertel, J.; Caulfield, B.; Ryan, J.; Delahunt, E. Single-leg drop landing movement strategies in participants with chronic ankle instability compared with lateral ankle sprain ‘copers’. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 1049–1059. [Google Scholar] [CrossRef] [PubMed]
- Monaghan, K.; Delahunt, E.; Caulfield, B. Ankle function during gait in patients with chronic ankle instability compared to controls. Clin. Biomech. 2006, 21, 168–174. [Google Scholar] [CrossRef] [PubMed]
- Panoutsakopoulos, V.; Kotzamanidou, M.C.; Papaiakovou, G.; Kollias, I.A. The Ankle Joint Range of Motion and Its Effect on Squat Jump Performance with and without Arm Swing in Adolescent Female Volleyball Players. J. Funct. Morphol. Kinesiol. 2021, 6, 14. [Google Scholar] [CrossRef]
- Taborri, J.; Molinaro, L.; Russo, L.; Palmerini, V.; Larion, A.; Rossi, S. Comparison of Machine Learning Algorithms Fed with Mobility-Related and Baropodometric Measurements to Identify Temporomandibular Disorders. Sensors 2024, 24, 3646. [Google Scholar] [CrossRef] [PubMed]
- Giustino, V.; Zangla, D.; Messina, G.; Pajaujiene, S.; Feka, K.; Battaglia, G.; Bianco, A.; Palma, A.; Patti, A. Kinematics of Cervical Spine during Rowing Ergometer at Different Stroke Rates in Young Rowers: A Pilot Study. Int. J. Environ. Res. Public Health 2022, 19, 7690. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Subjects (n) | Age (y) | Height (cm) | Weight (kg) | |
|---|---|---|---|---|
| Mean | F (37) | 16.0 | 161 | 55.9 |
| M (25) | 17.2 | 174 | 69.9 | |
| Standard deviation | F (37) | 4.78 | 8.57 | 11.7 |
| M (25) | 3.27 | 10.6 | 12.4 |
| Dorsiflexion of Foot | ||||||||
|---|---|---|---|---|---|---|---|---|
| Left Foot | Right Foot | |||||||
| Angular Speed (°/s) | Range of Motion (ROM°) | Fluency Index | Angular Speed (°/s) | Range of Motion (ROM°) | Fluency Index | |||
| Left foot | Dorsiflexion | Angular speed (°/s) | ||||||
| Range of motion (ROM°) | ||||||||
| Fluency Index | 0.400 ** | |||||||
| Plantarflexion | Angular speed (°/s) | 0.360 ** | 0.275 * | −0.281 * | ||||
| Range of motion (ROM°) | ||||||||
| Fluency Index | 0.540 *** | 0.487 *** | 0.356 ** | |||||
| Eversion | Angular speed (°/s) | 0.378 ** | 0.261 * | 0.443 *** | 0.293 * | |||
| Range of motion (ROM°) | 0.250 * | |||||||
| Fluency Index | 0.395 ** | 0.334 ** | ||||||
| Inversion | Angular speed (°/s) | 0.449 *** | 0.597 *** | 0.287 * | ||||
| Range of motion (ROM°) | ||||||||
| Fluency Index | 0.422 *** | |||||||
| Right foot | Dorsiflexion | Angular speed (°/s) | 0.334 ** | |||||
| Range of motion (ROM°) | 0.538 *** | |||||||
| Fluency Index | 0.355 ** | 0.403 ** | ||||||
| Plantarflexion | Angular speed (°/s) | 0.308 * | 0.585 *** | 0.345 ** | ||||
| Range of motion (ROM°) | 0.452 *** | |||||||
| Fluency Index | 0.321 * | 0.267 * | 0.312 * | −0.287 * | 0.262 * | |||
| Eversion | Angular speed (°/s) | 0.294 * | 0.280 * | 0.627 *** | 0.494 *** | |||
| Range of motion (ROM°) | 0.274 * | 0.322 * | 0.355 ** | |||||
| Fluency Index | 0.339 ** | 0.309* | 0.251 * | |||||
| Inversion | Angular speed (°/s) | 0.647 *** | 0.337 ** | |||||
| Range of motion (ROM°) | 0.381 ** | |||||||
| Fluency Index | 0.308 * | 0.267 * | 0.263 * | |||||
| Left foot | One-legged landing after a forward jump | Ellipse Surface Area (mm2) | −0.315 * | −0.406 ** | ||||
| Maximum oscillation | ||||||||
| Average speed of movement (mm/s) | ||||||||
| X-mean (mm) | 0.363 ** | 0.308 * | 0.530 *** | |||||
| Y-mean (mm) | ||||||||
| Right foot | One-legged landing after a forward jump | Ellipse Surface Area (mm2) | −0.310 * | |||||
| Maximum oscillation | 0.254 * | |||||||
| Average speed of movement (mm/s) | ||||||||
| X-mean (mm) | 0.305 * | |||||||
| Y-mean (mm) | ||||||||
| Left foot | One-legged landing on a lateral jump | Ellipse Surface Area (mm2) | −0.352 ** | |||||
| Maximum oscillation | ||||||||
| Average speed of movement (mm/s) | ||||||||
| X-mean (mm) | 0.279 * | |||||||
| Y-mean (mm) | ||||||||
| Right foot | One-legged landing on a lateral jump | Ellipse Surface Area (mm2) | ||||||
| Maximum oscillation | ||||||||
| Average speed of movement (mm/s) | ||||||||
| X-mean (mm) | ||||||||
| Y-mean (mm) | ||||||||
| CMJ | 0.464 *** | 0.810 *** | ||||||
| Plantarflexion of Foot | ||||||||
|---|---|---|---|---|---|---|---|---|
| Left Foot | Right Foot | |||||||
| Angular Speed (°/s) | Range of Motion (ROM°) | Fluency Index | Angular Speed (°/s) | Range of Motion (ROM°) | Fluency Index | |||
| Left foot | Dorsiflexion | Angular speed (°/s) | ||||||
| Range of motion (ROM°) | ||||||||
| Fluency Index | ||||||||
| Plantarflexion | Angular speed (°/s) | |||||||
| Range of motion (ROM°) | ||||||||
| Fluency Index | 0.483 *** | |||||||
| Eversion | Angular speed (°/s) | 0.428 *** | 0.382 ** | |||||
| Range of motion (ROM°) | 0.399 ** | |||||||
| Fluency Index | 0.355 ** | 0.403 ** | ||||||
| Inversion | Angular speed (°/s) | 0.405 ** | 0.453 *** | |||||
| Range of motion (ROM°) | 0.499 *** | |||||||
| Fluency Index | 0.303 * | |||||||
| Right foot | Dorsiflexion | Angular speed (°/s) | ||||||
| Range of motion (ROM°) | ||||||||
| Fluency Index | ||||||||
| Plantarflexion | Angular speed (°/s) | 0.466 *** | 0.436 *** | |||||
| Range of motion (ROM°) | 0.585 *** | |||||||
| Fluency Index | 0.478 *** | 0.464 ** | 0.626 *** | |||||
| Eversion | Angular speed (°/s) | 0.379 ** | 0.280 * | 0.320 * | 0.715 *** | 0.380 ** | ||
| Range of motion (ROM°) | 0.303 * | 0.290 * | ||||||
| Fluency Index | 0.290* | 0.378 ** | 0.359 ** | |||||
| Inversion | Angular speed (°/s) | 0.252 * | 0.300* | 0.656 ** | 0.497 *** | |||
| Range of motion (ROM°) | 0.377 ** | 0.270 * | 0.309 * | |||||
| Fluency Index | 0.369 ** | 0.298 * | ||||||
| Left foot | One-legged landing after a forward jump | Ellipse Surface Area (mm2) | ||||||
| Maximum oscillation | ||||||||
| Average speed of movement (mm/s) | ||||||||
| X-mean (mm) | ||||||||
| Y-mean (mm) | ||||||||
| Right foot | One-legged landing after a forward jump | Ellipse Surface Area (mm2) | ||||||
| Maximum oscillation | ||||||||
| Average speed of movement (mm/s) | ||||||||
| X-mean (mm) | ||||||||
| Y-mean (mm) | ||||||||
| Left foot | One-legged landing on a lateral jump | Ellipse Surface Area (mm2) | ||||||
| Maximum oscillation | ||||||||
| Average speed of movement (mm/s) | ||||||||
| X-mean (mm) | ||||||||
| Y-mean (mm) | ||||||||
| Right foot | One-legged landing on a lateral jump | Ellipse Surface Area (mm2) | ||||||
| Maximum oscillation | ||||||||
| Average speed of movement (mm/s) | ||||||||
| X-mean (mm) | ||||||||
| Y-mean (mm) | ||||||||
| CMJ | ||||||||
| Eversion of Foot | ||||||||
|---|---|---|---|---|---|---|---|---|
| Left Foot | Right Foot | |||||||
| Angular Speed (°/s) | Range of Motion (ROM°) | Fluency Index | Angular Speed (°/s) | Range of Motion (ROM°) | Fluency Index | |||
| Left foot | Dorsiflexion | Angular speed (°/s) | ||||||
| Range of motion (ROM°) | ||||||||
| Fluency Index | ||||||||
| Plantarflexion | Angular speed (°/s) | |||||||
| Range of motion (ROM°) | ||||||||
| Fluency Index | ||||||||
| Eversion | Angular speed (°/s) | |||||||
| Range of motion (ROM°) | ||||||||
| Fluency Index | 0.579 *** | |||||||
| Inversion | Angular speed (°/s) | 0.684 *** | 0.352 ** | |||||
| Range of motion (ROM°) | 0.307 * | |||||||
| Fluency Index | 0.298 * | 0.255 * | ||||||
| Right foot | Dorsiflexion | Angular speed (°/s) | ||||||
| Range of motion (ROM°) | ||||||||
| Fluency Index | ||||||||
| Plantarflexion | Angular speed (°/s) | 0.671 *** | 0.585 *** | |||||
| Range of motion (ROM°) | 0.314 * | |||||||
| Fluency Index | 0.489 *** | 0.465 *** | ||||||
| Eversion | Angular speed (°/s) | 0.695 *** | 0.380 ** | |||||
| Range of motion (ROM°) | 0.629 *** | |||||||
| Fluency Index | 0.314 * | 0.480 *** | 0.464 *** | |||||
| Inversion | Angular speed (°/s) | 0.673 *** | 0.461 *** | 0.637 *** | 0.300 * | |||
| Range of motion (ROM°) | 0.347 ** | |||||||
| Fluency Index | 0.462 *** | 0.433 *** | 0.288 * | 0.459 *** | ||||
| Left foot | One-legged landing after a forward jump | Ellipse Surface Area (mm2) | ||||||
| Maximum oscillation | ||||||||
| Average speed of movement (mm/s) | ||||||||
| X-mean (mm) | ||||||||
| Y-mean (mm) | ||||||||
| Right foot | One-legged landing after a forward jump | Ellipse Surface Area (mm2) | ||||||
| Maximum oscillation | ||||||||
| Average speed of movement (mm/s) | ||||||||
| X-mean (mm) | ||||||||
| Y-mean (mm) | ||||||||
| Left foot | One-legged landing on a lateral jump | Ellipse Surface Area (mm2) | ||||||
| Maximum oscillation | ||||||||
| Average speed of movement (mm/s) | ||||||||
| X-mean (mm) | ||||||||
| Y-mean (mm) | ||||||||
| Right foot | One-legged landing on a lateral jump | Ellipse Surface Area (mm2) | ||||||
| Maximum oscillation | ||||||||
| Average speed of movement (mm/s) | ||||||||
| X-mean (mm) | ||||||||
| Y-mean (mm) | ||||||||
| CMJ | ||||||||
| Inversion of Foot | ||||||||
|---|---|---|---|---|---|---|---|---|
| Left Foot | Right Foot | |||||||
| Angular Speed (°/s) | Range of Motion (ROM°) | Fluency Index | Angular Speed (°/s) | Range of Motion (ROM°) | Fluency Index | |||
| Left foot | Dorsiflexion | Angular speed (°/s) | ||||||
| Range of motion (ROM°) | ||||||||
| Fluency Index | ||||||||
| Plantarflexion | Angular speed (°/s) | |||||||
| Range of motion (ROM°) | ||||||||
| Fluency Index | ||||||||
| Eversion | Angular speed (°/s) | |||||||
| Range of motion (ROM°) | ||||||||
| Fluency Index | ||||||||
| Inversion | Angular speed (°/s) | |||||||
| Range of motion (ROM°) | ||||||||
| Fluency Index | 0.382 ** | |||||||
| Right foot | Dorsiflexion | Angular speed (°/s) | ||||||
| Range of motion (ROM°) | ||||||||
| Fluency Index | ||||||||
| Plantarflexion | Angular speed (°/s) | 0.633 *** | 0.265 * | |||||
| Range of motion (ROM°) | 0.476 *** | |||||||
| Fluency Index | 0.413 *** | |||||||
| Eversion | Angular speed (°/s) | 0.684 *** | 0.290 * | |||||
| Range of motion (ROM°) | ||||||||
| Fluency Index | ||||||||
| Inversion | Angular speed (°/s) | 0.757 *** | ||||||
| Range of motion (ROM°) | 0.298 * | 0.657 *** | 0.288 * | |||||
| Fluency Index | 0.36 ** | |||||||
| Left foot | One-legged landing after a forward jump | Ellipse Surface Area (mm2) | ||||||
| Maximum oscillation | ||||||||
| Average speed of movement (mm/s) | ||||||||
| X-mean (mm) | ||||||||
| Y-mean (mm) | ||||||||
| Right foot | One-legged landing after a forward jump | Ellipse Surface Area (mm2) | ||||||
| Maximum oscillation | ||||||||
| Average speed of movement (mm/s) | ||||||||
| X-mean (mm) | ||||||||
| Y-mean (mm) | ||||||||
| Left foot | One-legged landing on a lateral jump | Ellipse Surface Area (mm2) | ||||||
| Maximum oscillation | ||||||||
| Average speed of movement (mm/s) | ||||||||
| X-mean (mm) | ||||||||
| Y-mean (mm) | ||||||||
| Right foot | One-legged landing on a lateral jump | Ellipse Surface Area (mm2) | ||||||
| Maximum oscillation | ||||||||
| Average speed of movement (mm/s) | ||||||||
| X-mean (mm) | ||||||||
| Y-mean (mm) | ||||||||
| CMJ | ||||||||
| Description | Gender | n | Mean | SD | p | Cohen’s d | ||
|---|---|---|---|---|---|---|---|---|
| Age | F | 37 | 16.027 | 4.775 | ns | |||
| M | 25 | 17.240 | 3.270 | |||||
| Height | F | 37 | 160.730 | 8.568 | <0.001 | −1.47 | ||
| M | 25 | 174.080 | 10.571 | |||||
| Weight | F | 37 | 55.946 | 11.723 | <0.001 | −1.16 | ||
| M | 25 | 69.880 | 12.364 | |||||
| Left foot | One-legged landing after a forward jump | * Ellipse Surface Area (mm2) | F | 37 | 67,044.45 | 36,620.1 | ns | |
| M | 25 | 82,007.7 | 66,993.9 | |||||
| * Sway path length (mm) | F | 37 | 845.427 | 281.710 | ns | |||
| M | 25 | 943.225 | 333.231 | |||||
| * Maximum oscillation | F | 37 | 42.056 | 63.484 | 0.007 | −0.61 | ||
| M | 25 | 99.247 | 125.736 | |||||
| * Average speed of movement (mm/s) | F | 37 | 42.774 | 14.492 | ns | |||
| M | 25 | 47.860 | 17.984 | |||||
| * X-mean | F | 37 | −31.809 | 13.256 | ns | |||
| M | 25 | −30.845 | 18.738 | |||||
| Y-mean | F | 37 | 9.493 | 14.314 | ns | |||
| M | 25 | 16.026 | 19.085 | |||||
| Right foot | One-legged landing after a forward jump | * Ellipse Surface Area (mm2) | F | 37 | 77,004.3 | 38,035.4 | ns | |
| M | 25 | 85,871.6 | 48,083.5 | |||||
| * Sway path length (mm) | F | 37 | 923.166 | 349.061 | ns | |||
| M | 25 | 876.222 | 284.824 | |||||
| * Maximum oscillation | F | 37 | 95.330 | 152.405 | ns | |||
| M | 25 | 72.798 | 132.586 | |||||
| * Average speed of movement (mm/s) | F | 37 | 46.846 | 17.650 | ns | |||
| M | 25 | 45.978 | 18.437 | |||||
| X-mean | F | 37 | −29.909 | 11.828 | ns | |||
| M | 25 | −28.670 | 12.373 | |||||
| Y-mean | F | 37 | 10.631 | 10.952 | ns | |||
| M | 25 | 12.533 | 16.041 | |||||
| Left foot | One-legged landing on a lateral jump | * Ellipse Surface Area (mm2) | F | 37 | 72,284.882 | 38,690.435 | ns | |
| M | 25 | 74,317.066 | 32,100.34 | |||||
| * Sway path length (mm) | F | 37 | 1090.288 | 442.459 | ns | |||
| M | 25 | 1007.506 | 284.450 | |||||
| * Maximum oscillation | F | 37 | 76.547 | 110.790 | ns | |||
| M | 25 | 75.708 | 120.193 | |||||
| * Average speed of movement (mm/s) | F | 37 | 55.658 | 23.406 | ns | |||
| M | 25 | 52.162 | 16.778 | |||||
| * X-mean | F | 37 | −32.728 | 25.125 | ns | |||
| M | 25 | −35.727 | 15.995 | |||||
| Y-mean | F | 37 | 5.659 | 17.210 | ns | |||
| M | 25 | 9.467 | 14.178 | |||||
| Right foot | One-legged landing on a lateral jump | * Ellipse Surface Area (mm2) | F | 37 | 69,621.044 | 37,242.685 | ns | |
| M | 25 | 79,571.328 | 77,463.133 | |||||
| Sway path length (mm) | F | 37 | 1034.607 | 331.264 | 0.027 | 0.58 | ||
| M | 25 | 868.578 | 186.447 | |||||
| * Maximum swing | F | 37 | 101.488 | 144.359 | ns | |||
| M | 25 | 51.333 | 60.789 | |||||
| * Average speed of movement (mm/s) | F | 37 | 52.636 | 175.341 | ns | |||
| M | 25 | 43.969 | 9.822 | |||||
| * X-mean | F | 37 | −27.628 | 17.750 | ns | |||
| M | 25 | −29.159 | 27.710 | |||||
| * Y-mean | F | 37 | 7.660 | 9.008 | ns | |||
| M | 25 | 10.980 | 21.543 | |||||
| Left foot | Dorsiflexion | * Angular speed (°/s) | F | 37 | 44.838 | 34.791 | ns | |
| M | 25 | 42.800 | 23.272 | |||||
| Range of motion (ROM°) | F | 37 | 29.754 | 5.913 | ns | |||
| M | 25 | 30.896 | 6.269 | |||||
| * Fluency Index | F | 37 | 0.86 | 0.156 | ns | |||
| M | 25 | 0.88 | 0.116 | |||||
| Left foot | Plantarflexion | * Angular speed (°/s) | F | 37 | 46.703 | 36.325 | ns | |
| M | 25 | 47.520 | 45.710 | |||||
| Range of motion (ROM°) | F | 37 | 44.935 | 9.012 | ns | |||
| M | 25 | 46.088 | 11.211 | |||||
| * Fluency Index | F | 37 | 0.83 | 0.142 | ns | |||
| M | 25 | 0.82 | 0.145 | |||||
| Left foot | Eversion | Angular speed (°/s) | F | 37 | 47.730 | 25.941 | ns | |
| M | 25 | 40.040 | 21.255 | |||||
| Range of motion (ROM°) | F | 37 | 32.205 | 9.936 | ns | |||
| M | 25 | 32.824 | 7.925 | |||||
| * Fluency Index | F | 37 | 0.866 | 0.141 | ns | |||
| M | 25 | 0.858 | 0.134 | |||||
| Left foot | Inversion | * Angular speed (°/s) | F | 37 | 54.757 | 22.869 | ns | |
| M | 25 | 47.920 | 19.455 | |||||
| Range of motion (ROM°) | F | 37 | 37.970 | 8.495 | ns | |||
| M | 25 | 39.092 | 11.572 | |||||
| * Fluency Index | F | 37 | 0.907 | 0.098 | ns | |||
| M | 24 | 0.838 | 0.206 | |||||
| Right foot | Dorsiflexion | * Angular speed (°/s) | F | 37 | 45.973 | 27.046 | ns | |
| M | 25 | 45.640 | 20.512 | |||||
| Range of motion (ROM°) | F | 37 | 29.827 | 6.193 | ns | |||
| M | 25 | 31.520 | 6.754 | |||||
| * Fluency Index | F | 37 | 0.860 | 0.120 | ns | |||
| M | 25 | 0.917 | 0.107 | |||||
| Right foot | Plantarflexion | * Angular speed (°/s) | F | 37 | 50.351 | 25.588 | ns | |
| M | 25 | 41.840 | 20.134 | |||||
| Range of motion (ROM°) | F | 37 | 43.543 | 8.861 | ns | |||
| M | 25 | 42.776 | 9.620 | |||||
| * Fluency Index | F | 37 | 0.843 | 0.116 | ns | |||
| M | 25 | 0.824 | 0.101 | |||||
| Right foot | Eversion | * Angular speed (°/s) | F | 37 | 51.054 | 27.993 | ns | |
| M | 25 | 48.640 | 28.110 | |||||
| Range of motion (ROM°) | F | 37 | 33.030 | 8.463 | ns | |||
| M | 25 | 34.380 | 12.373 | |||||
| * Fluency Index | F | 37 | 0.879 | 0.183 | ns | |||
| M | 25 | 0.863 | 0.125 | |||||
| Right foot | Inversion | * Angular speed (°/s) | F | 37 | 53 | 25.970 | ns | |
| M | 25 | 48 | 22.856 | |||||
| Range of motion (ROM°) | F | 37 | 37.924 | 8.3194 | ns | |||
| M | 25 | 42.056 | 13.204 | |||||
| * Fluency Index | F | 37 | 0.869 | 0.176 | ns | |||
| M | 25 | 0.901 | 0.105 | |||||
| CMJ | F | 37 | 18.735 | 4.805 | 0.001 | −0.89 | ||
| M | 25 | 23.324 | 5.609 | |||||
| Multiple Linear Regression—CMJ (cm) | ||||
|---|---|---|---|---|
| Predictor | Estimate | SE | t | p |
| Intercept | −24.694 | 6.143 | −4.019 | <0.001 |
| Right Dorsiflexion Range of Mov. ° | 0.674 | 0.057 | 11.672 | <0.001 |
| Foot size | 0.605 | 0.127 | 4.767 | <0.001 |
| Right sway path length (mm) | 0.017 | 0.006 | 2.890 | 0.005 |
| Right average speed of movement (mm/s) | −0.322 | 0.107 | −3.018 | 0.004 |
| Right Plantarflexion Range of Mov.° | −0.006 | 0.041 | −0.145 | 0.885 |
| Multiple Linear Regression—CMJ (cm) | ||||
|---|---|---|---|---|
| Predictor | Estimate | SE | t | p |
| Intercept | −16.919 | 9.644 | −1.754 | 0.085 |
| Left Dorsiflexion Range of Mov. ° | 0.489 | 0.108 | 4.545 | <0.001 |
| Foot size | 0.634 | 0.211 | 3.007 | 0.004 |
| Left sway path length (mm) | 0.002 | 0.017 | 0.102 | 0.919 |
| Left average speed of movement (mm/s) | −0.066 | 0.327 | −0.200 | 0.842 |
| Left Plantarflexion Range of Mov.° | −0.031 | 0.065 | −0.471 | 0.639 |
| Measurements | p | ||
|---|---|---|---|
| Left ellipse surface area (mm2) | vs. | Right ellipse surface area (mm2) | 0.147 |
| Left sway path length (mm) | vs. | Right sway path length (mm) | 0.603 |
| Left maximum oscillation | vs. | Right maximum swing | 0.363 |
| Left x-mean | vs. | Right x-mean | 0.305 |
| Left y-mean | vs. | Right y-mean | 0.655 |
| Left ellipse surface area (mm2) | vs. | (l)—Left ellipse surface area (mm2) | 0.997 |
| Left sway path length (mm) | vs. | (l)—Left sway path length (mm) | <0.001 |
| Left maximum oscillation | vs. | (l)—Left maximum oscillation | 0.589 |
| Left average speed of movement (mm/s) | vs. | (l)—Left average speed of movement (mm/s) | <0.001 |
| Left x-mean | vs. | (l)—Left x-mean | 0.420 |
| Left y-mean | vs. | (l)—Left y-mean | 0.014 |
| Right ellipse surface area (mm2) | vs. | (l)—Right ellipse surface area (mm2) | 0.313 |
| Right sway path length (mm) | vs. | (l)—Right sway path length (mm) | 0.154 |
| Right maximum swing | vs. | (l)—Right maximum oscillation | 0.839 |
| Right average speed of movement (mm/s) | vs. | (l)—Right average speed of movement (mm/s) | 0.288 |
| Right x-mean | vs. | (l)—Right x-mean | 0.671 |
| Right y-mean | vs. | (l)—Right y-mean | 0.146 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patti, A.; Gervasi, M.; Giustino, V.; Figlioli, F.; Canzone, A.; Drid, P.; Thomas, E.; Messina, G.; Vicari, D.S.S.; Palma, A.; et al. The Influence of Ankle Mobility and Foot Stability on Jumping Ability and Landing Mechanics: A Cross-Sectional Study. J. Funct. Morphol. Kinesiol. 2024, 9, 160. https://doi.org/10.3390/jfmk9030160
Patti A, Gervasi M, Giustino V, Figlioli F, Canzone A, Drid P, Thomas E, Messina G, Vicari DSS, Palma A, et al. The Influence of Ankle Mobility and Foot Stability on Jumping Ability and Landing Mechanics: A Cross-Sectional Study. Journal of Functional Morphology and Kinesiology. 2024; 9(3):160. https://doi.org/10.3390/jfmk9030160
Chicago/Turabian StylePatti, Antonino, Marco Gervasi, Valerio Giustino, Flavia Figlioli, Alberto Canzone, Patrik Drid, Ewan Thomas, Giuseppe Messina, Domenico Savio Salvatore Vicari, Antonio Palma, and et al. 2024. "The Influence of Ankle Mobility and Foot Stability on Jumping Ability and Landing Mechanics: A Cross-Sectional Study" Journal of Functional Morphology and Kinesiology 9, no. 3: 160. https://doi.org/10.3390/jfmk9030160
APA StylePatti, A., Gervasi, M., Giustino, V., Figlioli, F., Canzone, A., Drid, P., Thomas, E., Messina, G., Vicari, D. S. S., Palma, A., & Bianco, A. (2024). The Influence of Ankle Mobility and Foot Stability on Jumping Ability and Landing Mechanics: A Cross-Sectional Study. Journal of Functional Morphology and Kinesiology, 9(3), 160. https://doi.org/10.3390/jfmk9030160