
Effects of Self-Myofascial Release on Athletes’ Physical Performance: A Systematic Review

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection
2.2.1. Inclusion
2.2.2. Exclusion
2.3. Quality Assessment
2.4. Data Extraction and Synthesis
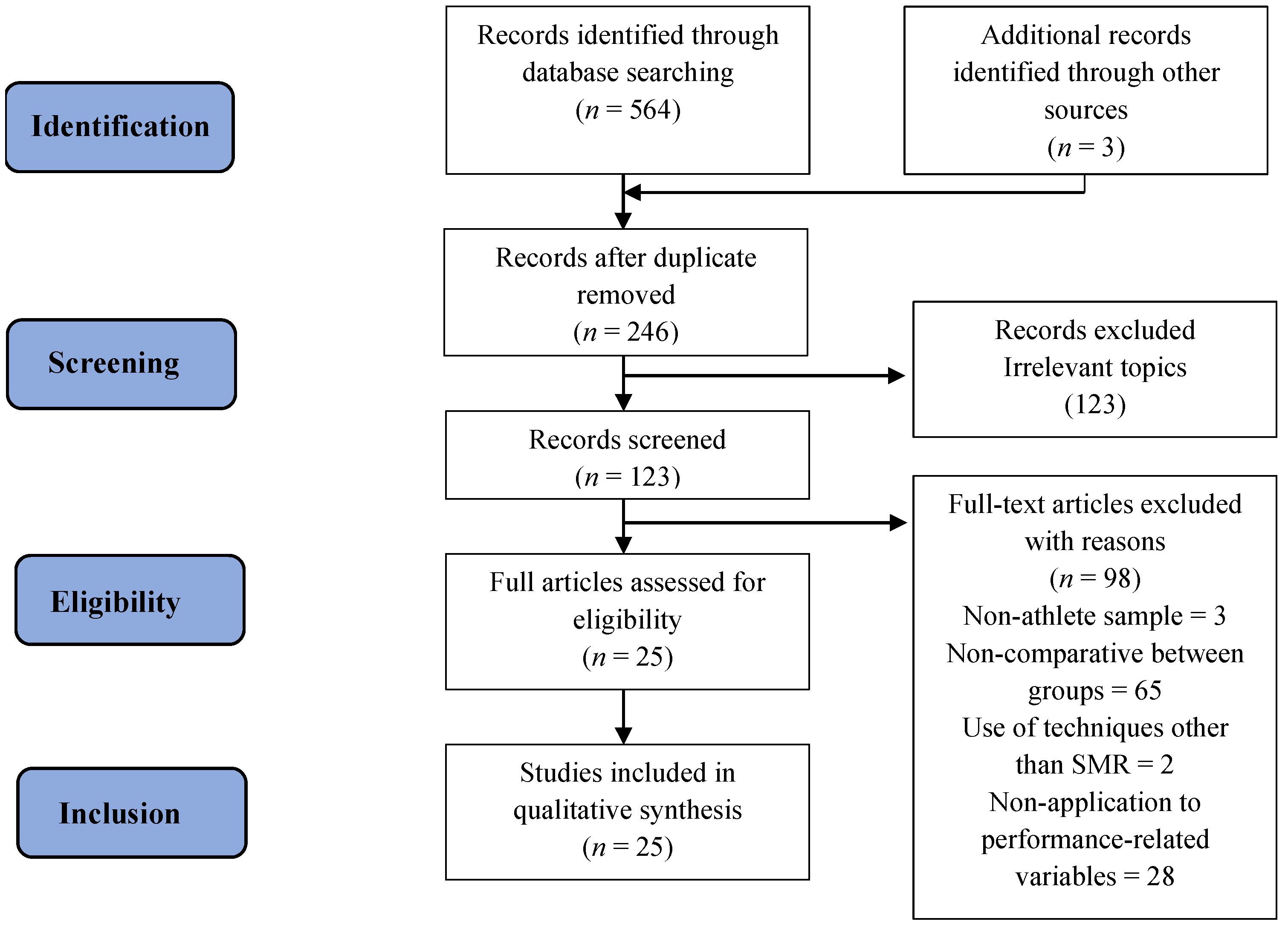
2.5. Search Summary
3. Results
3.1. Characteristics of Included Studies
3.2. Study Type
3.3. Main Results
3.3.1. Mobility Improvement
3.3.2. Strength Improvement
3.3.3. Speed Improvement
3.3.4. Agility Improvement
3.3.5. Influence on Subjects’ Recovery Capacity
4. Discussion
5. Conclusions
6. Brief Practical Applications
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Suarez-Rodriguez, V.; Fede, C.; Pirri, C.; Petrelli, L.; Loro-Ferrer, J.F.; Rodriguez-Ruiz, D.; De Caro, R.; Stecco, C. Fascial Innervation: A Systematic Review of the Literature. Int. J. Mol. Sci. 2022, 23, 5674. [Google Scholar] [CrossRef] [PubMed]
- Schleip, R. Fascial plasticity—A new neurobiological explanation: Part 2. J. Bodyw. Mov. Ther. 2003, 7, 105–116. [Google Scholar]
- Adstrum, S.; Hedley, G.; Schleip, R.; Stecco, C.; Yucesoy, C.A. Defining the fascial system. J. Bodyw. Mov. Ther. 2017, 21, 173–177. [Google Scholar] [CrossRef]
- Ferreira, R.M.; Martins, P.N.; Goncalves, R.S. Effects of Self-myofascial Release Instruments on Performance and Recovery: An Umbrella Review. Int. J. Exerc. Sci. 2022, 15, 861. [Google Scholar]
- Konrad, A.; Nakamura, M.; Tilp, M.; Donti, O.; Behm, D.G. Foam Rolling Training Effects on Range of Motion: A Systematic Review and Meta-Analysis. Sports Med. 2022, 52, 2523–2535. [Google Scholar] [CrossRef] [PubMed]
- Sulowska-Daszyk, I.; Skiba, A. The Influence of Self-Myofascial Release on Muscle Flexibility in Long-Distance Runners. Int. J. Environ. Res. Public Health 2022, 19, 457. [Google Scholar] [CrossRef] [PubMed]
- Pagaduan, J.C.; Chang, S.Y.; Chang, N.J. Chronic Effects of Foam Rolling on Flexibility and Performance: A Systematic Review of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2022, 19, 4315. [Google Scholar] [CrossRef]
- Amico, A.D.; Morin, C.; Release, M.; Performance, H. Effects of myofascial release on human performance a review of the literature. Myofascial Release Hum. Perform. 2013, 1, 1–45. [Google Scholar]
- Pernigoni, M.; Conte, D.; Calleja-González, J.; Boccia, G.; Romagnoli, M.; Ferioli, D. The Application of Recovery Strategies in Basketball: A Worldwide Survey. Front. Physiol. 2022, 13, 887507. [Google Scholar] [CrossRef]
- Cheatham, S.W.; Kolber, M.J.; Cain, M.; Lee, M. The effects of self-myofascial release using a foam roll or roller massager on joint range of motion, muscle recovery, and performance: A systematic review. Int. J. Sports Phys. Ther. 2015, 10, 827–838. [Google Scholar]
- Gabriel, A.; Konrad, A.; Roidl, A.; Queisser, J.; Schleip, R.; Horstmann, T.; Pohl, T. Myofascial Treatment Techniques on the Plantar Surface Influence Functional Performance in the Dorsal Kinetic Chain. J. Sports Sci. Med. 2022, 21, 13. [Google Scholar] [CrossRef] [PubMed]
- Beardsley, C.; Škarabot, J. Effects of self-myofascial release: A systematic review. J. Bodyw. Mov. Ther. 2015, 19, 747–758. [Google Scholar] [CrossRef] [PubMed]
- O’Connell, J.A. Bioelectric responsiveness of fascia: A model for understanding the effects of manipulation. Tech. Orthop. 2003, 18, 67–73. [Google Scholar] [CrossRef][Green Version]
- Tozzi, P. Selected fascial aspects of osteopathic practice. J. Bodyw. Mov. Ther. 2012, 16, 503–519. [Google Scholar] [CrossRef] [PubMed]
- Mauntel, T.C.; Clark, M.A.; Padua, D.A. Effectiveness of Myofascial Release Therapies on Physical Performance Measurements: A Systematic Review. Athl. Train Sport Health Care 2014, 6, 189–196. [Google Scholar] [CrossRef]
- Glänzel, M.H.; Rodrigues, D.R.; Petter, G.N.; Pozzobon, D.; Vaz, M.A.; Geremia, J.M. Foam Rolling Acute Effects on Myofascial Tissue Stiffness and Muscle Strength: A Systematic Review and Meta-Analysis. J. Strength Cond. Res. 2022, 10, 1519. [Google Scholar] [CrossRef]
- Borg-Stein, J.; Simons, D.G. Focused review: Myofascial pain. Arch. Phys. Med. Rehabil. 2002, 83, 40–47. [Google Scholar] [CrossRef]
- Thompson, W.R. Worldwide survey of fitness trends for 2018. ACSM Health Fit. J. 2017, 21, 10–19. [Google Scholar] [CrossRef]
- Weerapong, P.; Hume, P.A.; Kolt, G.S. The mechanisms of massage and effects on performance, muscle recovery and injury prevention. Sports Med. 2005, 35, 235–256. [Google Scholar] [CrossRef]
- Simmonds, N.; Miller, P.; Gemmell, H. A theoretical framework for the role of fascia in manual therapy. J. Bodyw. Mov. Ther. 2012, 16, 83–93. [Google Scholar] [CrossRef]
- Hedley, G. Notes on visceral adhesions as fascial pathology. J. Bodyw. Mov. Ther. 2010, 14, 255–261. [Google Scholar] [CrossRef]
- Martínez Rodríguez, R.; Galán del Río, F. Mechanistic basis of manual therapy in myofascial injuries. Sonoelastographic evolution control. J. Bodyw. Mov. Ther. 2013, 17, 221–234. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.S.; Ingber, D.E. Tensegrity and mechanoregulation: From skeleton to cytoskeleton. Osteoarthr. Cartil 1999, 7, 81–94. [Google Scholar] [CrossRef] [PubMed]
- Chaitow, L. Research in water and fascia. Micro-tornadoes, hydrogenated diamonds & nanocrystals. Massage Today 2009, 9, 1–3. [Google Scholar]
- Schleip, R.; Müller, D.G. Training principles for fascial connective tissues: Scientific foundation and suggested practical applications. J. Bodyw. Mov. Ther. 2013, 17, 103–115. [Google Scholar] [CrossRef] [PubMed]
- Bednar, D.A.; Orr, F.W.; Simon, G.T. Observations on the pathomorphology of the thoracolumbar fascia in chronic mechanical back pain: A microscopic study. Spine 1995, 20, 1161–1164. [Google Scholar] [CrossRef]
- Findley, T.; Chaudhry, H.; Stecco, A.; Roman, M. Fascia research—A narrative review. J. Bodyw. Mov. Ther. 2012, 16, 67–75. [Google Scholar] [CrossRef]
- Gerwin, R. Myofascial pain syndrome: Here we are, where must we go. J. Musculoskelet. Pain 2010, 18, 329–347. [Google Scholar] [CrossRef]
- Bron, C.; Dommerholt, J.D. Etiology of myofascial trigger points. Curr. Pain Headache Rep. 2012, 16, 439–444. [Google Scholar] [CrossRef]
- Chaudhry, H.; Schleip, R.; Ji, Z.; Bukiet, B.; Maney, M.; Findley, T. Threedimensional mathematical model for deformation of human fasciae in manual therapy. J. Am. Osteopath. Assoc. 2008, 108, 379–390. [Google Scholar]
- Queré, N.; Noël, E.; Lieutaud, A.; D’Alessio, P. Fasciatherapy combined with pulsology touch induces changes in blood turbulence potentially beneficial for vascular endothelium. J. Bodyw. Mov. Ther. 2009, 13, 239–245. [Google Scholar] [CrossRef]
- Okamoto, T.; Masuhara, M.; Ikuta, K. Acute effects of self-myofascial release using a foam roller on arterial function. J. Strength Cond. Res. 2014, 28, 69–73. [Google Scholar] [CrossRef] [PubMed]
- Hong, C.Z.; Simons, D.G. Pathophysiologic and electrophysiologic mechanisms of myofascial trigger points. Arch. Phys. Med. Rehabil. 1998, 79, 863–872. [Google Scholar] [CrossRef]
- Myburgh, C.; Larsen, A.H.; Hartvigsen, J. A Systematic, Critical Review of Manual Palpation for Identifying Myofascial Trigger Points: Evidence and Clinical Significance. Arch. Phys. Med. Rehabil. 2008, 89, 1169–1176. [Google Scholar] [CrossRef] [PubMed]
- Jami, L. Golgi tendon organs in mammalian skeletal muscle: Functional properties and central actions. Physiol. Rev. 1992, 72, 623–666. [Google Scholar] [CrossRef]
- Stecco, C.; Gagey, O.; Belloni, A.N.; Pozzuoli, A.; Porzionato, A.; Macchi, V.; Aldegheri, R.; De Caro, R.; Delmas, V. Anatomy of the deep fascia of the upper limb. Second part: Study of innervation. Morphologie 2007, 91, 38–43. [Google Scholar] [CrossRef]
- Barnes, M.F. The basic science of myofascial release: Morphologic change in connective tissue. J. Bodyw. Move Ther. 1997, 1, 231–238. [Google Scholar] [CrossRef]
- Morelli, M.; Seaborne, D.E.; Sullivan, S.J. Changes in h-reflex amplitude during massage of triceps surae in healthy subjects. J. Orthop. Sports Phys. Ther. 1990, 12, 55–59. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Morelli, M.; Seaborne, D.E.; John Sullivan, S. H-reflex modulation during manual muscle massage of human triceps surae. Arch. Phys. Med. Rehabil. 1991, 72, 915–919. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, J.; Sullivan, S.J.; Seaborne, D.E. The effect of two intensities of massage on H-reflex amplitude. Phys. Ther. 1992, 72, 449–457. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, S.J.; Williams, L.R.T.; Seaborne, D.E.; Morelli, M. Effects of massage on alpha motoneuron excitability. Phys. Ther. 1991, 71, 555–560. [Google Scholar] [CrossRef]
- Morelli, M.; Chapman, C.E.; Sullivan, S.J. Do cutaneous receptors contribute to the changes in the amplitude of the H-reflex during massage? Electromyogr. Clin. Neurophysiol. 1999, 39, 441–447. [Google Scholar] [PubMed]
- Bradbury-Squires, D.J.; Noftall, J.C.; Sullivan, K.M.; Behm, D.G.; Power, K.E.; Button, D.C. Roller-massager application to the quadriceps and knee-joint range of motion and neuromuscular efficiency during a lunge. J. Athl. Train. 2015, 50, 133–140. [Google Scholar] [CrossRef]
- Wilke, J.; Schwiete, C.; Behringer, M. Effects of Maximal Eccentric Exercise on Deep Fascia Stiffness of the Knee Flexors: A Pilot Study using Shear-Wave Elastography. J. Sports Sci. Med. 2022, 21, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Schleip, R.; Naylor, I.L.; Ursu, D.; Melzer, W.; Zorn, A.; Wilke, H.J.; Lehmann-Horn, F.; Klingler, W. Passive muscle stiffness may be influenced by active contractility of intramuscular connective tissue. Med. Hypotheses 2006, 66, 66–71. [Google Scholar] [CrossRef]
- Collazo, M.A. Sistema de Capacidades Físicas. Fundamentos teóricos, Metodologicos y Cientificos que sustentan su Desarrollo en el Hombre; CENDA: Havana, Cuba, 2003. [Google Scholar]
- Schroeder, A.N.; Best, T.M. Is Self-Myofascial release an effective preexercise and recovery strategy? A literature review. Curr. Sports Med. Rep. 2015, 14, 200–208. [Google Scholar] [CrossRef]
- Wiewelhove, T.; Döweling, A.; Schneider, C.; Hottenrott, L.; Meyer, T.; Kellmann, M.; Pfeiffer, M.; Ferrauti, A. A Meta-Analysis of the Effects of Foam Rolling on Performance and Recovery. Front. Physiol. 2019, 10, 376. [Google Scholar] [CrossRef] [PubMed]
- Konrad, A.; Nakamura, M.; Behm, D.G. The Effects of Foam Rolling Training on Performance Parameters: A Systematic Review and Meta-Analysis including Controlled and Randomized Controlled Trials. Int. J. Environ. Res. Public Health. 2022, 19, 11638. [Google Scholar] [CrossRef]
- Alonso-Calvete, A.; Lorenzo-Martínez, M.; Padrón-Cabo, A.; Pérez-Ferreirós, A.; Kalén, A.; Abelairas-Gómez, C.; Rey, E. Does Vibration Foam Roller Influence Performance and Recovery? A Systematic Review and Meta-analysis. Sports Med. Open 2022, 8, 32. [Google Scholar] [CrossRef]
- Urrútia, G.; Bonfill, X. Declaración PRISMA: Una propuesta para mejorar la publicación de revisiones sistemáticas y metaanálisis. Med. Clin. 2010, 135, 507–511. [Google Scholar] [CrossRef] [PubMed]
- Mamédio, C.; Roberto, M.; Nobre, C. The Pico Strategy for the Research Question. Rev. Latino-Am. Enferm. 2007, 15, 508–511. [Google Scholar]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef] [PubMed]
- Kurt, C.; Gürol, B.; Nebioğlu, İ.Ö. Effects of traditional stretching versus self-myofascial release warm-up on physical performance in well-trained female athletes. J. Musculoskelet. Neuronal Interact. 2023, 23, 61. [Google Scholar]
- Barrenetxea-García, J.; Nuell, S.; Garai, S.; Murua-Ruiz, A.; Mielgo-Ayuso, J.; Calleja-González, J.; Sáez de Villarreal, E. Effect of Foam Roll recovery method on performance in water polo players: A randomized controlled trial. Physician Sportsmed. 2023; online ahead of print. [Google Scholar]
- Chen, C.H.; Chiu, C.H.; Tseng, W.C.; Wu, C.Y.; Su, H.H.; Chang, C.K.; Ye, X. Acute effects of combining dynamic stretching and vibration foam rolling warm-up on lower-limb muscle performance and functions in female handball players. J. Strength Cond. Res. 2023, 37, 1277–1283. [Google Scholar] [CrossRef]
- Kozlenia, D.; Domaradzki, J. Acute Effect of Short Intensive Self-Myofascial Release on Jump Performance in Amateur Athletes: A Randomized Cross-Over Study. Int. J. Environ. Res. Public Health. 2022, 19, 16816. [Google Scholar] [CrossRef]
- Michalski, T.; Król, T.; Michalik, P.; Rutkowska, M.; Dąbrowska-Galas, M.; Ziaja, D.; Kuszewski, M. Does the Self-Myofascial Release Affect the Activity of Selected Lower Limb Muscles of Soccer Players? J. Hum. Kinet. 2022, 83, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Zhang, Z.; Li, C.; Zhu, D.; Hu, Y.; Fu, H.; Zhai, H.; Wang, Y. Acute effects of vibration foam rolling and local vibration during warm-up on athletic performance in tennis players. PLoS ONE 2022, 17, e0268515. [Google Scholar] [CrossRef]
- Chen, A.H.; Chiu, C.H.; Hsu, C.H.; Wang, I.L.; Chou, K.M.; Tsai, Y.S.; Lin, Y.F.; Chen, C.H. Acute effects of vibration foam rolling warm-up on jump and flexibility asymmetry, agility and frequency speed of kick test performance in taekwondo athletes. Symmetry 2021, 13, 1664. [Google Scholar] [CrossRef]
- Lopez-Samanes, A.; Del Coso, J.; Hernández-Davó, J.L.; Moreno-Pérez, D.; Romero-Rodriguez, D.; Madruga-Parera, M.; Muñoz, A.; Moreno-Pérez, V. Acute effects of dynamic versus foam rolling warm-up strategies on physical performance in elite tennis players. Biol. Sport. 2021, 38, 595–601. [Google Scholar] [CrossRef]
- Rahimi, A.; Amani-Shalamzari, S.; Clemente, F.M. The effects of foam roll on perceptual and performance recovery during a futsal tournament. Physiol. Behav. 2020, 223, 112981. [Google Scholar] [CrossRef]
- Oranchuk, D.J.; Flattery, M.R.; Robinson, T.L. Superficial heat administration and foam rolling increase hamstring flexibility acutely; with amplifying effects. Phys. Ther. Sport. 2019, 40, 213–217. [Google Scholar] [CrossRef] [PubMed]
- Romero-Franco, N.; Romero-Franco, J.; Jiménez-Reyes, P. Jogging and practical-duration foam-rolling exercises and range of motion, proprioception, and vertical jump in athletes. J. Athl. Train. 2019, 54, 1171–1178. [Google Scholar] [PubMed]
- Guillot, A.; Kerautret, Y.; Queyrel, F.; Schobb, W.; Di Rienzo, F. Foam Rolling and Joint Distraction with Elastic Band Training Performed for 5–7 Weeks Respectively Improve Lower Limb Flexibility. J. Sports Sci. Med. 2019, 18, 160–171. [Google Scholar]
- Aune, A.A.; Bishop, C.; Turner, A.N.; Papadopoulos, K.; Budd, S.; Richardson, M.; Maloney, S.J. Acute and chronic effects of foam rolling vs eccentric exercise on ROM and force output of the plantar flexors. J. Sports Sci. 2019, 37, 138–145. [Google Scholar] [CrossRef] [PubMed]
- Giovanelli, N.; Vaccari, F.; Floreani, M.; Rejc, E.; Copetti, J.; Garra, M.; Biasutti, L.; Lazzer, S. Short-term effects of rolling massage on energy cost of running and power of the lower limbs. Int. J. Sports Physiol. Perform. 2018, 13, 1337–1343. [Google Scholar] [CrossRef] [PubMed]
- Stroiney, D.A.; Mokris, R.; Hanna, G.R.; Ranney, J.D. Examination of self-myofascial release vs. Instrument-assisted soft-tissue mobilization techniques on vertical and horizontal power in recreational athletes. J. Strength Cond. Res. 2020, 34, 79–88. [Google Scholar] [CrossRef] [PubMed]
- Richman, E.D.; Tyo Acrn, B.M. Combined effects of self-myofascial release and dynamic stretching on range of motion, jump, sprint, and agility performance. J. Strength Cond. Res. 2018, 33, 1795–1803. [Google Scholar] [CrossRef]
- Sağiroğlu, I.; Kurt, C.; Pekünlü, E.; Özsu, I. Residual effects of static stretching and self-myofascial-release exercises on flexibility and lower body explosive strength in well-trained combat athletes. Isokinet. Exerc. Sci. 2017, 25, 135–141. [Google Scholar] [CrossRef]
- D’Amico, A.; Paolone, V. The Effect of Foam Rolling on Recovery between Two Eight Hundred Metre Runs. J. Hum. Kinet. 2017, 57, 97–105. [Google Scholar]
- Fairall, R.R.; Cabell, L.; Boergers, R.J.; Battaglia, F. Acute effects of self-myofascial release and stretching in overhead athletes with GIRD. J. Bodyw. Mov. Ther. 2017, 21, 648–652. [Google Scholar] [CrossRef]
- Rey, E.; Padrón-Cabo, A.; Costa, P.B.; Barcala-Furelos, R. The Effects of Foam Rolling as a Recovery Tool in Professional Soccer Players. J. Strength Cond. Res. 2019, 33, 2194–2201. [Google Scholar] [CrossRef] [PubMed]
- Behara, B.; Jacobson, B.H. Acute Effects of Deep Tissue Foam Rolling and Dynamic Stretching on Muscular Strength, Power, and Flexibility in Division i Linemen. J. Strength Cond. Res. 2017, 31, 888–892. [Google Scholar] [CrossRef] [PubMed]
- Murray, A.M.; Jones, T.W.; Horobeanu, C.; Turner, A.P.; Sproule, J. Sixty seconds of foam rolling does not affect functional flexibility or change muscle temperature in adolescent athletes. Int. J. Sports Phys. Ther. 2016, 11, 765–776. [Google Scholar] [PubMed]
- Škarabot, J.; Beardsley, C.; Štirn, I. Comparing the effects of self-myofascial release with static stretching on ankle range-of-motion in adolescent athletes. Int. J. Sports Phys. Ther. 2015, 10, 203–212. [Google Scholar] [PubMed]
- Markovic, G. Acute effects of instrument assisted soft tissue mobilization vs. Foam rolling on knee and hip range of motion in soccer players. J. Bodyw. Mov. Ther. 2015, 19, 690–696. [Google Scholar] [CrossRef] [PubMed]
- Peacock, C.A.; Krein, D.D.; Silver, T.A.; Sanders, G.J.; von Carlowitz, K.P.A. An acute bout of self-myofascial release in the form of foam rolling improves performance testing. Int. J. Exerc. Sci. 2014, 7, 202–211. [Google Scholar] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, 2700. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef]
- McKenney, K.; Elder, A.S.; Elder, C.; Hutchins, A. Myofascial release as a treatment for orthopaedic conditions: A systematic review. J. Athl. Train. 2013, 48, 522–527. [Google Scholar] [CrossRef]
- MacDonald, G.Z.; Penney, M.D.; Mullaley, M.E.; Cuconato, A.L.; Drake, C.D.; Behm, D.G.; Button, D.C. An acute bout of self-myofascial release increases range of motion without a subsequent decrease in muscle activation or force. J. Strength Condit. Res. 2013, 27, 812–821. [Google Scholar] [CrossRef]
- Bushell, J.E.; Dawson, S.M.; Webster, M.M. Clinical relevance of foam rolling on hip extension angle in a functional lunge position. J. Strength Cond. Res. 2015, 29, 2397–2403. [Google Scholar] [CrossRef] [PubMed]
- Halperin, I.; Aboodarda, S.J.; Button, D.C.; Andersen, L.L.; Behm, D.G. Roller massager improves range of motion of plantar flexor muscles without subsequent decreases in force parameters. Int. J. Sports Phys. Ther. 2014, 9, 92–102. [Google Scholar] [PubMed]
- Sullivan, K.M.; Silvey, D.B.J.; Button, D.; Behm, D.G. Roller massage application to the hamstring increases sit and reach range of motion within five to ten section without performance impairments. Int. J. Sports Phys. Ther. 2013, 8, 228–236. [Google Scholar]
- Spellman, J.; Eldredge, R.; Nelson, M.; Ostrowski, J.; Concannon, J. Is Myofascial Decompression Effective at Increasing Hamstring Flexibility in the Athletic Population? A Critically Appraised Topic. J. Sport. Rehabil. 2022, 31, 1100–1104. [Google Scholar] [CrossRef]
- Pérez-Bellmunt, A.; Casasayas-Cos, O.; Ragazzi, P.; Rodríguez-Sanz, J.; Hidalgo-García, C.; Canet-Vintró, M.; Caballero-Martínez, I.; Pacheco, L.; López-de-Celis, C. Foam Rolling vs. Proprioceptive Neuromuscular Facilitation Stretching in the Hamstring Flexibility of Amateur Athletes: Control Trials. Int. J. Environ. Res. Public Health. 2023, 20, 1439. [Google Scholar] [CrossRef]
- Junker, D.H.; Stöggl, T.L. The Foam Roll as a Tool to Improve Hamstring Flexibility. J. Strength Cond. Res. 2015, 29, 3480–3485. [Google Scholar] [CrossRef]
- Pilat, A. Myofascial induction approaches. In Fascia: The Tensional Network of the Human Body; Elsevier: Edinburgh, UK, 2012; pp. 311–317. [Google Scholar]
- Purslow, P.P.; Delage, J.P. General anatomy of the muscle fasciae. In Fascia: The Tensional Network of the Human Body; Elsevier: Edinburgh, UK, 2012; pp. 5–11. [Google Scholar]
- Shah, S.; Bhalara, A. Myofascial release. Int. J. Health Sci. Res. 2012, 2, 69–77. [Google Scholar]
- Birbaumer, N.; Schmidt, R.F. Biologische Psychologie, 7th ed.; Springer: Berlin/Heidelberg, Germany, 2010. [Google Scholar]
- Freiwald, J. Optimales Dehnen. Sport—Prevention—Rehabilitation; Spitta: Balingen, Germany, 2013. [Google Scholar]
- Jay, K.; Sundstrup, E.; Søndergaard, S.D.; Behm, D.; Brandt, M.; Særvoll, C.A.; Jakobsen, M.D.; Andersen, L. Specific and cross over effects of massage for muscle soreness: Randomized controlled trial. Int. J. Sports Phys. Ther. 2014, 9, 82–91. [Google Scholar]
- Ciccone, W.J.; Bratton, D.R.; Weinstein, D.M.; Elias, J.J. Viscoelasticity and temperature variations decrease tension and stiffness of hamstring tendon grafts following anterior cruciate ligament reconstruction. J. Bone Jt. Surg. 2006, 88, 1071–1078. [Google Scholar] [CrossRef]
- Hamada, Y.; Akasaka, K.; Otsudo, T.; Sawada, Y.; Hattori, H.; Hasebe, Y.; Kikuchi, Y.; Hall, T. Immediate Effects of Foam Roller and Stretching to the Lead Hip on Golfers Swing: A Randomized Crossover Trial. Healthcare 2023, 11, 2001. [Google Scholar] [CrossRef]
- Warneke, K.; Aragão-Santos, J.C.; Alizadeh, S.; Bahrami, M.; Anvar, S.H.; Konrad, A.; Behm, D.G. Are Acute Effects of Foam-Rolling Attributed to Dynamic Warm Up Effects? A Comparative Study. J. Sports Sci. Med. 2023, 22, 180–188. [Google Scholar] [CrossRef] [PubMed]
- Holfiel, T.; Swoboda, B.; Krinner, S.; Grim, C.; Engelhardt, M.; Uder, M.; Heiss, R. Acute effects of lateral thigh foam rolling on arterial tissue perfusion determined by spectral Doppler and power Doppler ultrasound. J. Strength Cond. Res. 2017, 31, 893–900. [Google Scholar] [CrossRef]
- Mikesky, A.E.; Bahamonde, R.E.; Stanton, K.; Alvey, T.; Fitton, T. Acute effects of the stick-on strength, power, and flexibility. J. Strength Condit. Res. 2002, 16, 446–450. [Google Scholar]
- Healey, K.C.; Hatfield, D.L.; Blanpied, P.; Dorfman, L.R.; Riebe, D. The effects of myofascial release with foam rolling on performance. J. Strength Cond. Res. 2014, 28, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, I.M. The effects of precompetition massage on the kinematic parameters of 10-M sprint performance. J. Strength Cond. Res. 2010, 24, 1179–1183. [Google Scholar] [CrossRef] [PubMed]
- Goodwin, J.E.; Glaister, M.; Howaston, G.; Lockey, R.A.; McInnes, G. Effect of preperformance lower-limb massage on thirty-meter sprint running. J. Strength Cond. Res. 2007, 21, 1028–1031. [Google Scholar]
- Alegre, L.M.; Lara, A.J.; Elvira, J.L.L.; Aguado, X. Muscle morphology and jump performance: Gender and intermuscular variability. J. Sports Med. Phys. Fit. 2009, 49, 30–33. [Google Scholar]
- Taber, C.B.; Colter, R.J.; Davis, J.J.; Seweje, P.A.; Wilson, D.P.; Foster, J.Z.; Merrigan, J.J. The Effects of Body Tempering on Force Production, Flexibility and Muscle Soreness in Collegiate Football Athletes. J. Funct. Morphol. 2022, 7, 9. [Google Scholar] [CrossRef]
- Asker, M.; Brooke, H.L.; Waldén, M.; Tranaeus, U.; Johansson, F.; Skillgate, E.; Holm, L.W. Risk factors for, and prevention of, shoulder injuries in overhead sports: A systematic review with best-evidence synthesis. Br. J. Sports Med. 2018, 52, 1312–1319. [Google Scholar] [CrossRef]
- Ricci, V.; Mezian, K.; Chang, K.V.; Tarantino, D.; Güvener, O.; Gervasoni, F.; Naňka, O.; Özçakar, L. Ultrasound Imaging and Guidance for Cervical Myofascial Pain: A Narrative Review. Int. J. Environ. Res. Public Health 2023, 20, 3838. [Google Scholar] [CrossRef]


{kind=link}
| Studies | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | S |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Kurt, 2023 [54] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 |
| Barrenetxea-García, 2023 [55] | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 8 |
| Chen, 2023 [56] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 |
| Kozlenia 2022 [57] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 |
| Michalski, 2022 [58] | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6 |
| Wang, 2022 [59] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 |
| Chen, 2021 [60] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 |
| Lopez-Samanes, 2021 [61] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 |
| Rahimi, 2020 [62] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 |
| Ornachuk, 2019 [63] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 |
| Romero-Franco, 2019 [64] | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 9 |
| Guillot, 2019 [65] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 |
| Aune, 2018 [66] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 |
| Giovanelli, 2018 [67] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 |
| Stroiney, 2018 [68] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 |
| Richman, 2018 [69] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 8 |
| Sağiroğlu, 2017 [70] | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6 |
| D’Amico, 2017 [71] | 1 | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 7 |
| Fairall, 2017 [72] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 8 |
| Rey, 2017 [73] | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 9 |
| Behara, 2017 [74] | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 9 |
| Murray, 2016 [75] | 1 | 1 | 0 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 8 |
| Škarabot, 2015 [76] | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 9 |
| Markovic, 2015 [77] | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 8 |
| Peacock, 2014 [78] | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6 |
| Intervention | ||||||
|---|---|---|---|---|---|---|
| Study (1st Author and Year) | Design | Subjects (Age) | Sports Experience | Muscle Groups | Duration | N° Sessions |
| Kurt, 2023 [54] | RCD | 23 w (21.8 ± 1.73) | Turkey Women’s Handball Super League and regional league (9.57 ± 2.54 years of experience) | Quadriceps, hamstrings, hips | Three warm-up protocols in a randomised order: SS, DS, SMR All protocols start with 5 min cycling SS: 9 min of SS, 3 exercises 3 × 30 s both sides DS: 9 min of DS, 8 exercises 2 × 20 s both sides SMR: 9 min of SMP, 3 × 30 s each muscle group both sides | 3 (1 per condition) |
| Barrenetxea-García, 2023 [55] | RCT | 14 m and 16 w (20 ± 3.84) | Male First Regional League and Female Second National league in Waterpolo (more than 9 years of experience) | Gluteus medius, tensor fasciae latae, adductor, lumbar region, upper back, back of the shoulder and pectoral | FRG: 1 set of 60 s for each muscle group, 10 min in total (7-weeks, 28 sessions) CG: no intervention (passive, not using FR technique) | 28 |
| Chen, 2023 [56] | RCD | 10 w (21 ± 1) | Taiwanese handball collegiate national champion team (Training more than 15 h per week) | Quadriceps and hamstrings | Three warm-up protocols in a randomized order: GW, DS and DS + VR All protocols start with 5 min jogging GW continues with 8 min of SS and 8 min of DS DS continues with 4 sets of exercises (8 min) DS + VR continues with 4 sets of DS exercises (8 min) and 4 sets of VR—30 s at a rate of 30 rolls per min (1 s up, 1 s down) in each muscle for both legs | 3 (1 per condition) |
| Kozlenia 2022 [57] | RCD | 14 m and 16 w (21.8 ± 1.15) | University amateur athletes (soccer, handball, basketball, volleyball and extreme conditioning program training) (3.76 ± 1.73 training sessions per week; 104.83 ± 26.01 single training session duration in min; 6.48 ± 3.12 weekly training volume in hours/week) | Calves, hamstrings, glutes, and thighs | Group A: 10 min GW (5 min jogging, 15 reps—air squats. 15 reps—high knees, 15 reps—lunges, and submaximal trials of the jump to be tested) + SI-SMR Group B: Only GW SI-SMR protocol: Each muscle group treated for 15 s with an intensity of 20 reps/15 s × leg, maintaining high pressure on the foam roller during application, 7–8 on the pain numbering rating scale | 2 (1 per condition) |
| Michalski, 2022 [58] | RCT | 40 m (A = 20 m, 25.5 ± 5.2; B = 20 m, 26.3 ± 1.3) (17 FP and 3 GK) | Soccer players of the regional soccer league; high level of physical fitness (soccer training a minimum of 3 times per week) | Hamstring muscles (FR application), assessing biceps femoris and gluteus maximus | Group A = hamstring group; protocol of 210 s applying FR technique; application rhythm per repetition: 4 s (2 s in one direction and 2 s in the opposite one) Group B = rest | 1 |
| Wang, 2022 [59] | RCD | 27 m (20.4 ± 1.3) | Tennis players; 10 ± 0.7 years of experience | Lower back, gluteus, quadriceps, lateral thigh muscles, hamstrings, calf muscle groups | VFR = 5 min jogging + 1 set × 30 s (40 beats per min) each muscle group (7 min in total); PVPD = 5 min jogging + PVPD 1 set × 30 s each muscle group (7 min in total); CG = 5 min jogging | Only 1, (every subject performed only 1 condition) |
| Chen, 2021 [60] | RCD | 15 m (20.63 ± 1.18) | Elite taekwondo athletes; 9.79 ± 2.77 years of experience | Quadriceps and hamstrings | Three warm-up protocols in a randomised order: GW, GW + VR, and GW with double VR for the weaker leg Three (GW + VR) or six sets (GW + double VR) × 30 s at a rate of 30 rolls per min (1 s up, 1 s down) in each muscle for both legs | 3 (1 per condition) |
| Lopez Samanes, 2021 [61] | RCD | 11 m (20.64 ± 3.56) | High-performance tennis players (ATP players among 300 best national tennis players in Spain) | Quadriceps, hamstrings, gluteus, gastrocnemius | Rolling for 8 min on each lower extremity unilaterally (two different warm-up protocols: dynamic vs. Self-Myofascial Release with foam rolling) | 2 (1 per condition) |
| Rahimi, 2020 [62] | RCT | 16 m (19.1 ± 1.3) | Elite futsal players (training hours per week = 9) | Anterior thigh, hamstrings, gluteus, and gastrocnemius | Five reps × 40 s with 20 s rest between repetitions (two groups: (i) passive recovery (PR); and (ii) FR recovery) | Three matches in five days |
| Oranchuk, 2019 [63] | RCD | 26 w (19.4 ± 1.7) | NCAA Division II lacrosse (13) and soccer players (13) Years of experience: 6.9 ± 4.1 | Hamstrings | SH, FR, SH + FR in combination, and control groups taken into consideration Three sets × 1 min with 30 s passive rest between sets (FR protocol) | 4 (1 per condition) |
| Romero-Franco, 2019 [64] | RCT | 18 m and 12 w (24.1 ± 4.2) | Collegiate competitive athletes (several disciplines) | Anterior thigh, hamstrings, calf | Experimental (8 min jogging and FR exercises) and control group (8 min jogging) For 45 s in each muscle of both legs + 15 s of rest between legs (the entire FR protocol lasted about 6 min) | 1 |
| Guillot, 2019 [65] | RCT | 30 m (18.85 ± 1.10); | Professional rugby players | Right and left sides, separately (hip extensors, hip adductors, knee extensors, knee flexors and plantar flexors) | Participants from the FR 20 s and FR 40 s groups, respectively, performed a 7-week (15-session) foam rolling training programme involving between 7 and 14 back-and-forth movements per session; each back-and-forth movement did not exceed 3 s. CG with neutral task (cycling) | 15 |
| Aune, 2018 [66] | RCT | 23 (18 ± 1). (11 w; 12 m) | Top-division Norwegian soccer club | Gastrocnemius | Participants were allocated to an FR or eccentric exercise intervention group, both designed to improve dorsiflexion ROM. Three bouts of 60 s of foam rolling. Bouts were separated by 30 s. Participants completed three separate testing sessions on day 1 (baseline and 30 min post), day 2 (24 h post), and day 28 (4 weeks post) | 3 |
| Giovanelli, 2018 [67] | RCD | 13 m (26.3 ± 5.3) | Soccer, track and field, trail running, parkour; hours per week: 9.9 ± 3.5 | Plantar fascia, gastrocnemius, tibialis anterior, anterior thigh with extended knee, anterior thigh with flexed knee, posterior thigh, gluteus, fasciae latae | SMR protocol in experimental condition, while in the control condition testing session, the same measurements are performed without undergoing the SMR protocol Protocol: 1 min × muscle group, with 10 s per change; The application frequency was about 0.5 Hz (e.g., each rolling cycle lasted about 2 s) | 2 (1 per condition) |
| Stroiney, 2018 [68] | RCT | 49 (20.35 ± 2.56). (21 w), (28 m). | Various sports; average days per week: 5.13 ± 1.16; average minutes per session: 83.34 ± 34.60 | Sural triceps, hamstrings, quadriceps | SMR and IASTM groups SMR protocol: 90 s × muscle group | 1 (each subject performed only one condition) |
| Richman, 2018 [69] | RCD | 14 w (19.8 ± 1.3) | NCAA DII Volleyball and Basketball | Hip flexors, quadriceps, adductors, fascia lata tensors, plantar flexors and extensors | 6-min per session. Group 1: Light walking; Group 2: SMR 30 s × muscle group × leg | 2 (1 per condition) |
| Sağiroğlu, 2017 [70] | RCD | 16 m (23.9 ± 3.6) | MMA (Judo, Karate, Tae Kwon Do, Muay Thai); years of experience: 12.9 ± 5.2 | Hamstrings, quadriceps, gastrocnemius, soleus, glutes | SS and SMR groups SS = 4 stretching exercises; two sets × 30 s with 10 s passive recovery on each extremity; SMR = five back-and-forth FR movements × 30 s pressure with highest tolerable level. Two sets × 20 s with 10 s passive recovery × muscle × leg. Rest for 30 s between exercises | 3 (1 per condition) |
| D’Amico, 2017 [71] | RCD | 16 m (20.5 ± 0.5) | Track, 800 m flat | Glutes, hip flexors, quadriceps, iliotibial bands, adductors | The subjects complete two 800 m runs on a treadmill, separated by a 30 min rest, during which time a foam rolling protocol or passive rest period is performed FR protocol: Six back-and-forth FR movements on each side, adding up to a total of 30 s since each rolling movement lasts on whichever side for 5 s; 10 min per session | 2 (1 per condition) |
| Fairall, 2017 [72] | RCD | 12 m (36.92 ± 11.17) | Amateur baseball and softball; years of playing time: 28.42 ± 10.93 | Infraspinatus and deltoids | SMR, SS, and the combination of both (SMR + SS) Protocol: Two sets of SMR × 60 s, 30 s rest per set; SS for 30 s × three sets + 30 s rest between sets; and combining SMR and SS | 3 (1 per condition) |
| Rey, 2017 [73] | RCT | 18 m (26.6 ± 3.3) | Professional soccer players; years of systematic soccer training: 14.8 ± 2.6 | Quadriceps, hamstrings, adductors, glutes, gastrocnemius | FR recovery group and passive recovery group Protocol: 3 min after training session. Five FR exercises at a 50-pulse cadence per min. Both legs for 45 s each, with 15 s rest. The total FR time is 20 min | 1 (each subject performed only one condition) |
| Behara, 2017 [74] | RCT | 14 m (≥18) | NCAA DI American Football with >6 years of experience | Hamstrings, quadriceps, gluteus maximus, gastrocnemius | (a) no treatment, (b) deep tissue foam rolling, and (c) dynamic stretching FR protocol: 1 min on each muscle and extremity; 8 min in total | 3 (1 per condition) |
| Murray, 2016 [75] | RCD | 12 m (14.2 ± 1.4) | Elite squash sports academy | Hip flexors and quadriceps | FR and FAT groups (10 subjects each) FAT is a new form of IASTM For 60 s per muscle group, with 30 back-and-forth FR movements (15 in each direction) | 2 (1 per condition) |
| Skarabot, 2015 [76] | RCD | 11 (5 w), (6 m); (15.3 ± 1.0) | Trained endurance swimmers | Soleus, gastrocnemius | SS and FR groups: Each comprises three sets of 30 s of the intervention with 10 s of inter-set rest. FR + SS comprises the protocol from the FR condition followed by the protocol from the SS condition in sequence | 3 (1 per condition) |
| Markovic, 2015 [77] | RCT | 20 m (19 ± 2) | Competitive soccer | Quadriceps and hamstrings | FR group; FAT group (a new form of IASTM) Two sets × 1 min of FR per muscle group | 2 (1 per condition) |
| Peacock, 2014 [78] | RCD | 11 m (22.18 ± 2.18) | NCAA DI and DII competitive American football, soccer, track and field athletes | Thoracolumbar region, glutes, hamstrings, gastrocnemius, quadriceps, pectoral | The two warm-up routines compared: a total-body dynamic warm-up (DYN) and a total-body dynamic warm-up paired with SMR FR protocol: Five back-and-forth FR movements on each muscle group, taking 30 s × each back-and-forth movement; applied on both sides | 2 (1 per condition) |
| Study | n | Measurement | Results | |||
|---|---|---|---|---|---|---|
| Group | M | SD | p | |||
| Kurt, 2023 [54] | 23 | Sit-and-reach test (cm) | SS | 36.4 | 5.7 | p = 0.01 * (SS-DS); p = 0.001 * (DS-SMR) |
| DS | 38.3 | 6.2 | ||||
| SMR | 36.9 | 5.9 | ||||
| Chen, 2023 [56] | 10 | Knee flexion (degrees) | GW | 69.3 | 9.6 | p < 0.05 * |
| DS + VFR | 79.4 | 7.7 | ||||
| Knee extension (degrees) | GW | 130.5 | 6 | p > 0.05 | ||
| DS + VFR | 133.5 | 5.1 | ||||
| Wang, 2022 [59] | 27 | Y balance test—Left | VFR | 0.879 | 0.081 | p > 0.05 |
| Percussion devices | 0.849 | 0.074 | ||||
| CG | 0.872 | 0.036 | ||||
| Y balance test—Right | VFR | 0.876 | 0.123 | |||
| Percussion devices | 0.867 | 0.085 | ||||
| CG | 0.878 | 0.064 | ||||
| Chen, 2021 [60] | 15 | Active knee flexion—Stronger leg (degrees) | GW | 127.9 | 5.3 | p = 0.87 |
| GW + VFR | 128.9 | 5.3 | ||||
| Active knee flexion—Weaker leg (degrees) | GW | 129.1 | 4.9 | p = 0.70 | ||
| GW + VFR | 128.7 | 4.9 | ||||
| Modified sit-and-reach test—Stronger leg (degrees) | GW | 59.8 | 9.9 | p = 0.92 | ||
| GW + VFR | 60.6 | 8.4 | ||||
| Modified sit-and-reach test—Weaker leg (degrees) | GW | 57.1 | 11.1 | p = 0.8 | ||
| GW + VFR | 59.6 | 8.8 | ||||
| Lopez Samanes, 2021 [61] | 11 | Passive straight leg raise test—Dominant leg (degrees) | DS pre | 76.55 | 6.07 | p > 0.05 |
| DS post | 78.18 | 6.23 | ||||
| SMR pre | 77.27 | 5.75 | ||||
| SMR post | 79.09 | 4.13 | ||||
| Passive straight leg raise test—No dominant leg (degrees) | DS pre | 75.64 | 5.78 | p > 0.05 | ||
| DS post | 76.36 | 5.71 | ||||
| SMR pre | 77.09 | 5.47 | ||||
| SMR post | 78.36 | 4.97 | ||||
| Modified version of the Thomas test—Dominant leg | DS pre | 0.91 | 3.39 | p > 0.05 | ||
| DS post | 1.82 | 3.52 | ||||
| SMR pre | 0 | 2.69 | ||||
| SMR post | 0.36 | 2.8 | ||||
| Modified version of the Thomas test—No dominant leg | DS pre | 2.18 | 3.16 | p > 0.05 | ||
| DS post | 2.55 | 3.24 | ||||
| SMR pre | 0.73 | 2.24 | ||||
| SMR post | 1.09 | 3.02 | ||||
| Oranchuk, 2019 [63] | 13 | Passive straight leg raise (degrees) | CG | +1.9° | p > 0.05 | |
| FR | +5.4° | p < 0.001 * | ||||
| FR + heat | +9.5° | p < 0.001 * | ||||
| Romero-Franco, 2019 [64] | 30 | Thomas hip extension (degrees) | CG | −3.3–4.1° | Intra p < 0.05 * | Inter p > 0.05 |
| FR | −4.7–5.5° | Intra p < 0.05 * | ||||
| Thomas knee flexion (degrees) | CG | +1.6° | Intra p > 0.05 | Inter p < 0.05 * | ||
| FR | −2.4° | Intra p < 0.05 * | ||||
| Popliteal angle test (degrees) | CG | +1.8° | p > 0.05 intra and inter group | |||
| FR | −5.6° | |||||
| Ankle dorsiflexion (degrees) | CG | +1.5° | Intra p > 0.05 | Inter p > 0.05 | ||
| FR | +6.3° | Intra p < 0.05 * | ||||
| Guillot, 2019 [65] | 30 | Side split (degrees) | CG | +1.8° | p = 0.67 | |
| FR20 | +17.7° | p = 0.002 * | ||||
| FR40 | +18° | p = 0.005 * | ||||
| Active straight leg raise—Right side (degrees) | CG | +0.6° | p = 0.84 | |||
| FR20 | +14° | p = 0.004 * | ||||
| FR40 | +6.2° | p = 0.002 * | ||||
| Active straight leg raise—Left side (degrees) | CG | +0.1° | p = 0.98 | |||
| FR20 | +9.2° | p = 0.060 | ||||
| FR40 | +15.7° | p = 0.003 * | ||||
| Active flexed leg raise—Right side (degrees) | CG | +1.8° | p = 0.73 | |||
| FR20 | +14.2° | p = 0.004 * | ||||
| FR40 | +16.9° | p = 0.001 * | ||||
| Active flexed leg raise—Left side (degrees) | CG | −0.1° | p = 0.98 | |||
| FR20 | +11.5° | p = 0.01 * | ||||
| FR40 | +16.4° | p < 0.001 * | ||||
| Hip extension—Right side (degrees) | CG | +0.9 | p = 0.76 | |||
| FR20 | +17.1° | p < 0.001 * | ||||
| FR40 | +15.4° | p < 0.001 * | ||||
| Hip extension—Left side (degrees) | CG | +0.7 | p = 0.82 | |||
| FR20 | +15.5° | p < 0.001 * | ||||
| FR40 | +13.5° | p < 0.001 * | ||||
| Aune, 2018 [66] | 23 | Dorsiflexion ROM (degrees) | Eccentric | +7% | p < 0.001 * pre–post (whole sample) Inter p > 0.05 | |
| FR | +9% | |||||
| Richman, 2018 [69] | 14 | Sit and reach/flexibility (cm) | Light walking + DS pre | 37.6 | 4.2 | p < 0.05 * |
| Light walking + DS post | 39.9 | 3.9 | ||||
| FR + DS pre | 36.3 | 4.8 | p < 0.05 * | |||
| FR + DS post | 38.5 | 4.4 | ||||
| Rey, 2017 [73] | 18 | Sit and reach (cm) | CG pre | 25.27 | 8.8 | p > 0.05 |
| CG post | 24.94 | 7.24 | ||||
| FR pre | 20.79 | 9.18 | ||||
| FR post | 23.17 | 7.61 | ||||
| Fairall, 2017 [72] | 12 | Glenohumeral internal rotation ROM (degrees) | SMR | 24.15 | 4.66 | Intra-group p < 0.000 * Inter-group p = 0.55 |
| SS | 28.62 | 6.79 | ||||
| SMR + SS | 30.36 | 7.21 | ||||
| D’Amico, 2017 [71] | 16 | ROM hip extension (degrees) | Passive | Not specified | p > 0.05 | |
| FR | ||||||
| Stride length (cm) | Passive | Not specified | p > 0.05 | |||
| FR | ||||||
| Sağiroğlu, 2017 [70] | 16 | Sit-and-reach (cm) peak improvement during recovery (time) | Aerobic running | MIP = +2.13 cm (min 30:30) | Inter-group p < 0.05 * (aerobic running + SMR with better results in short term <10 min) | |
| Aerobic running + SS | MIP = +1.69 cm (min 15:30) | |||||
| Aerobic running + SMR | MIP = +2.03 cm (min 10:30) | |||||
| Behara, 2017 [74] | ROM hip flexion (degrees) | Baseline | 94.17 | 21.1 | p < 0.000 * | |
| FR | 108.92 | 15.51 | ||||
| DS | 111.77 | 13.44 | ||||
| Murray, 2016 [75] | 12 | ROM hip flexors and quadriceps (degrees) | FR + 2.4° than CG for overall flexibility changes | p = 0.03 * | ||
| Markovic, 2015 [77] | 20 | Passive straight leg raise (degrees) | FAT | +13.7° hip | p = 0.039 * | |
| FR | +6.6° hip | |||||
| Passive knee flexion test (degrees) | FAT | +15.2° | p = 0.06 | |||
| FR | +7° | |||||
| Škarabot, 2015 [76] | 11 | ROM ankle dorsiflexion (degrees) | SS | +0.9 | 0.67 | p < 0.05 * |
| FR | +0.4 | 0.67 | ||||
| SS + FR | +1.3 | 0.65 | ||||
| Peacock, 2014 [78] | 11 | Sit and reach (cm) | DYN | 34.12 | 5.21 | p = 0.83 |
| SMR + DYN | 34.32 | 5.7 | ||||
| Study | n | Measurement | Results | |||
|---|---|---|---|---|---|---|
| Group | M | SD | p | |||
| Kurt, 2023 [54] | 23 | CMJ height (cm) | SS | 22.3 | 3 | p < 0.05 * |
| DS | 25 | 3.7 | ||||
| SMR | 23.8 | 0 | ||||
| CMJ reactive index | SS | 0.528 | 2.275 | p > 0.05 | ||
| DS | 0.50 | 0.27 | ||||
| SMR | 0.57 | 0.33 | ||||
| Stiffness (kN/m) | SS | 6.92 | 6.4 | p > 0.05 | ||
| DS | 6.50 | 6.81 | ||||
| SMR | 7.07 | 7.1 | ||||
| Isokinetic peak torque—right knee extensor at 60° (Nm) | SS | 132.4 | 28.9 | p = 0.038 * | ||
| DS | 140.4 | 25.6 | ||||
| SMR | 138 | 24.6 | ||||
| Isokinetic peak torque—left knee extensor at 60° (Nm) | SS | 125 | 24 | p = 0.086 | ||
| DS | 130.7 | 21.9 | ||||
| SMR | 131.9 | 22.7 | ||||
| Isokinetic peak torque—right knee flexor at 60° (Nm) | SS | 90 | 15.5 | p = 0.006 * | ||
| DS | 94.9 | 18.5 | ||||
| SMR | 94.7 | 17.1 | ||||
| Isokinetic peak torque—left knee flexor at 60° (Nm) | SS | 88.3 | 13.5 | p = 0.603 | ||
| DS | 89.7 | 12.9 | ||||
| SMR | 91 | 15 | ||||
| Barrenetxea-García, 2023 [55] | 30 | In-water boost (jump, cm) | CG | 116.04 | 6.82 | p > 0.05 |
| FR | 114.51 | 6.96 | ||||
| Throwing speed test (m.s−1) | CG | 56.97 | 7 | p > 0.05 | ||
| FR | 58.08 | 7.88 | ||||
| Chen, 2023 [56] | 10 | Hamstring stiffness (Nm−1) | GW | 292.89 | 24.28 | p = 0.01 * |
| DS + VFR | 253.33 | 36.2 | ||||
| Quadricep stiffness (Nm−1) | GW | 254 | 23.78 | p > 0.05 | ||
| DS + VFR | 257.09 | 12.5 | ||||
| Hamstring isokinetic strength at 60° (Nm) | GW | 51.52 | 8.89 | p > 0.05 | ||
| DS + VFR | 51.39 | 12.28 | ||||
| Quadricep isokinetic strength at 60° (Nm) | GW | 107.47 | 14.29 | p > 0.05 | ||
| DS + VFR | 100.16 | 21.76 | ||||
| Wang, 2022 [59] | 27 | CMJ (cm) | VFR | 53.18 | 4.49 | p = 0.03 * |
| Percussion devices | 50.08 | 3.97 | ||||
| CG | 47.92 | 3.82 | ||||
| Drop jump (reactive strength index) | VFR | 2.01 | 0.11 | p = 0.012 * | ||
| Percussion devices | 1.99 | 0.11 | ||||
| CG | 1.86 | 0.05 | ||||
| Kozlenia, 2022 [57] | 30 | SJ (Jump height, relative force and power) | A vs. B | No SI-SMR vs. SI-SMR Diff.= 0.5–1.70 (A) vs. 0.11–0.16 (B) (depending on the variable) | p > 0.05 | |
| CMJ (Jump height, relative force and power) | A vs. B | Diff. = 0.23–0.89 (A) vs. −0.18–0.41 (B) (depending on the variable) | p > 0.05 | |||
| CMJ Height (Eccentric utilisation ratio) | A vs. B | Diff.= 0.01 (A) vs. 0.03 (B) | p > 0.05 | |||
| DJ (Jump height, relative force and power, reactive strength index and stiffness) | A vs. B | Diff.= −0.03–3.31 (A) vs. −1.71–0.46 (B) (depending on the variable) | p > 0.05 | |||
| Chen, 2021 [60] | 15 | CMJ (cm) | GW | 34.6 | 4.1 | p = 0.61 |
| GW + VFR | 35.1 | 4.7 | ||||
| Lopez Samanes, 2021 [61] | 11 | CMJ (cm) | DS pre | 34.78 | 5.13 | p > 0.05 |
| DS post | 35.59 | 5.19 | ||||
| SMR pre | 34.24 | 6.77 | ||||
| SMR post | 34.42 | 7.07 | ||||
| Rahimi, 2020 [62] | 17 | Sergeant jump (cm) | Passive pre | 44.9 | 7 | p > 0.05 |
| Passive post | 43.8 | 6.7 | ||||
| FR pre | 45.4 | 3 | ||||
| FR post | 44.5 | 4.5 | ||||
| Romero-Franco, 2019 [64] | 30 | CMJ (cm) | CG | +1.9 | Intra p < 0.05 * | Inter p > 0.05 |
| FR | +4 | Intra p < 0.05 * | ||||
| Aune, 2018 [66] | 23 | Drop jump—Reactive strength index | Significant chronic increase through the intervention (whole group, FR + eccentric) | Inter p = 0.932 | ||
| Plantar flexion torque (Nm) | Slightly better acute response for eccentric group, but no significant | p = 0.402 | ||||
| Richman, 2019 [69] | 14 | Drop jump (cm) | Light walk + DS | 42.45 | 6.35 | p = 0.351 |
| FR + DS | 43.18 | 7.01 | ||||
| Squat jump (cm) | Light walk + DS | 36.01 | 8.16 | p = 0.022 * | ||
| FR + DS | 37.73 | 7.75 | ||||
| CMJ (cm) | Light walk + DS | 40.91 | 7.66 | p = 0.021 * | ||
| FR + DS | 43.54 | 7.26 | ||||
| Stroiney, 2018 [68] | 49 | Sergeant jump—Men (cm) | SMR pre | 59.41 | 6.48 | p inter-group < 0.05 * |
| SMR post | 61.95 | 9.68 | ||||
| Assisted soft tissue mobilisation, pre | 59.15 | 13.36 | ||||
| Assisted soft tissue mobilisation, post | 60.22 | 11.07 | ||||
| Sergeant jump—Women (cm) | SMR pre | 45.11 | 4.78 | |||
| SMR post | 46.3 | 6.68 | ||||
| Assisted soft tissue mobilisation, pre | 47.55 | 7.26 | ||||
| Assisted soft tissue mobilisation, post | 43.26 | 8.1 | ||||
| Giovanelli, 2018 [67] | 13 | Maximal power—Lower limbs (W/kg) | CG | 62.1 | 11.1 | p = 0.251 |
| FR | 58.9 | 15.7 | ||||
| CMJ/RFD (N) | FR pre | 1819 | 362 | p = 0.024 * | ||
| FR post | 1972 | 461 | ||||
| Rey, 2017 [73] | 18 | CMJ (cm) | CG pre | 32.33 | 5.43 | p > 0.05 |
| CG post | 30.36 | 4.53 | ||||
| FR pre | 31.32 | 4.28 | ||||
| FR post | 30.26 | 3.34 | ||||
| Sağiroğlu, 2017 [70] | 16 | CMJ (cm) peak loss during recovery (time) | Aerobic running | −1.69 (min 30:00) | p inter-group > 0.05 | |
| Aerobic running + SS | −2.62 (min 30:00) | |||||
| Aerobic running + SMR | −2.19 (min 30:30) | |||||
| Behara, 2017 [74] | 14 | Vertical jump—Power peak (Watts) | Baseline | 4282.91 | 487.81 | p = 0.45 |
| FR | 4372.46 | 474.57 | ||||
| DS | 4318.73 | 418.52 | ||||
| Vertical jump—Velocity peak (m.s−1) | Baseline | 3.18 | 0.32 | p = 0.25 | ||
| FR | 3.27 | 0.28 | ||||
| DS | 3.22 | 0.27 | ||||
| Leg extension isometric force (Nm) | Baseline | 221.63 | 40.15 | p = 0.63 | ||
| FR | 214.01 | 49.85 | ||||
| DS | 208.44 | 60.25 | ||||
| Leg flexion isometric force (Nm) | Baseline | 134 | 25.06 | p = 0.63 | ||
| FR | 125.13 | 17.53 | ||||
| DS | 126.11 | 21.83 | ||||
| Peacock, 2014 [78] | 11 | Vertical jump (cm) | DYN | 67.66 | 9.79 | p = 0.012 * |
| SMR + DYN | 72.97 | 10.6 | ||||
| Horizontal jump (cm) | DYN | 228.6 | 25.25 | p = 0.007 * | ||
| SMR + DYN | 237.84 | 25.45 | ||||
| Indirect 1RM bench press (kg) | DYN | 99.92 | 19.56 | p = 0.024 * | ||
| SMR + DYN | 103.68 | 20.47 | ||||
| Study | n | Measurement | Results | |||
|---|---|---|---|---|---|---|
| Group | M | SD | p | |||
| Barrenetxea-García, 2023 [55] | 30 | 20 m sprint swim test (seconds) | CG | 12.23 | 0.75 | p > 0.05 |
| FR | 12.17 | 0.89 | ||||
| Wang, 2022 [59] | 27 | 2.5 m lateral acceleration test left (seconds) | VFR | 0.94 | 0.098 | p > 0.05 |
| Percussion devices | 1.004 | 0.138 | ||||
| CG | 0.951 | 0.09 | ||||
| 2.5 m lateral acceleration test (seconds) | VFR | 0.896 | 0.1 | |||
| Percussion devices | 0.967 | 0.107 | ||||
| CG | 0.954 | 0.122 | ||||
| Lopez Samanes, 2021 [61] | 11 | 10 m sprints (seconds) | DS pre | 2.22 | 0.11 | p > 0.05 |
| DS post | 2.2 | 0.12 | ||||
| SMR pre | 2.12 | 0.08 | ||||
| SMR post | 2.14 | 0.08 | ||||
| Rahimi, 2020 [62] | 17 | Repeated sprint ability (m) | Passive pre | 740.8 | 52.3 | p > 0.05 |
| Passive post | 727.6 | 65.3 | ||||
| FR pre | 723.5 | 41.9 | ||||
| FR post | 689.6 | 40.8 | ||||
| Stroiney, 2018 [68] | Sprint time—Men (seconds) | SMR pre | 5.4 | 0.47 | p > 0.05 | |
| SMR post | 5.47 | 0.52 | ||||
| Assisted soft tissue mobilisation, pre | 5.1 | 0.42 | ||||
| Assisted soft tissue mobilisation, post | 5.34 | 0.43 | ||||
| Sprint time—Women (seconds) | SMR pre | 5.7 | 0.27 | |||
| SMR post | 6.06 | 0.5 | ||||
| Assisted soft tissue mobilisation, pre | 5.8 | 0.49 | ||||
| Assisted soft tissue mobilisation, post | 5.94 | 0.47 | ||||
| Giovanelli, 2018 [67] | 13 | Running energy cost | CG pre vs. post | Not specified | ||
| FR pre vs. post | +6.2% | 8.3 | p = 0.052 | |||
| D’Amico, 2017 [71] | 16 | Running time (seconds) | Active recovery | 146.9 | 2.2 | p < 0.05 * |
| SMR | 145.2 | 1.8 | ||||
| Rey, 2017 [73] | 18 | 5 m sprints (seconds) | CG pre | 0.98 | 0.03 | p > 0.05 |
| CG post | 1 | 0.05 | ||||
| FR pre | 0.98 | 0.06 | ||||
| FR post | 1 | 0.06 | ||||
| 10 m sprints (seconds) | CG pre | 1.68 | 0.07 | p > 0.05 | ||
| CG post | 1.71 | 0.07 | ||||
| FR pre | 1.71 | 0.09 | ||||
| FR post | 1.72 | 0.05 | ||||
| Peacock, 2014 [78] | 11 | 37 m sprints (seconds) | DYN | 5.11 | 0.29 | p = 0.002 * |
| SMR + DYN | 4.95 | 0.21 | ||||
| Study | n | Measurement | Results | |||
|---|---|---|---|---|---|---|
| Group | M | SD | p | |||
| Wang, 2022 [59] | 27 | Hexagon test (seconds) | VFR | 10.73 | 0.4 | p = 0.03 * |
| Percussion devices | 11.02 | 0.45 | ||||
| CG | 11.39 | 0.73 | ||||
| Chen, 2021 [60] | 15 | Frequency speed of kick test | GW | 105.1 | 7.7 | p = 0.33 |
| GW + VFR | 109.5 | 9.9 | ||||
| Hexagon test (seconds) | GW | 12.8 | 1.6 | p = 0.03 * | ||
| GW + VFR | 11.6 | 1 | ||||
| 5-0-5 test (seconds) | GW | 2.6 | 0.2 | p = 0.37 | ||
| GW + VFR | 2.6 | 0.2 | ||||
| Lopez Samanes, 2021 [61] | 11 | 5-0-5 test (seconds) | DS pre | 2.86 | 0.14 | p > 0.05 |
| DS post | 2.79 | 0.13 | ||||
| SMR pre | 2.75 | 0.18 | ||||
| SMR post | 2.76 | 0.13 | ||||
| Rahimi, 2020 [62] | 17 | Pro-agility 5-10-5 test (seconds) | Passive pre | 5.2 | 0.3 | p > 0.05 |
| Passive post | 5.4 | 0.3 | ||||
| FR pre | 5.1 | 0.3 | ||||
| FR post | 5.2 | 0.3 | ||||
| Richman, 2018 [69] | 14 | Short sprint (seconds) | Light walk + DS | 2.05 | 0.17 | p = 0.222 |
| FR + DS | 2.02 | 0.13 | ||||
| t-test (seconds) | Light walk + DS | 12.22 | 0.77 | p = 0.577 | ||
| FR + DS | 12.18 | 0.08 | ||||
| Rey, 2017 [73] | 18 | t-test (seconds) | CG pre | 9.22 | 0.21 | p between groups < 0.05 * |
| CG post | 9.48 | 0.27 | ||||
| FR pre | 9.34 | 0.31 | ||||
| FR post | 9.36 | 0.34 | ||||
| Peacock, 2014 [78] | 11 | Pro-agility 18.3 m (seconds) | DYN | 4.97 | 0.24 | p = 0.001 * |
| SMR + DYN | 4.8 | 0.16 | ||||
| Study | n | Measurement | Results | ||||
|---|---|---|---|---|---|---|---|
| Group | M | SD | p | ||||
| Barrenetxea-García, 2023 [55] | 30 | sRPE | CG | min 580 max 750 | 145–181 res. | p > 0.05 | |
| FR | min 627 max 829 | 248–150 res. | |||||
| Michalski, 2022 [58] | 40 | %MVC GM | HR | 22.9 p0; 21.1 p1; 22.7 p2 | p < 0.001 (p1) | ||
| CG | 38.9 p0; 4.2 p1; 36.1 p2 | ||||||
| %MVC BF | HR | 21.7 p0; 20.7 p1; 23 p2 | p < 0.001 (p1); p < 0.01 (p2) | ||||
| CG | 27 p0; 41.8 p1; 40.2 p2 | ||||||
| sEMG GM | HR | 109.8 p0; 89.7 p1; 100 p2 | p < 0.001 (p1) | ||||
| CG | 143 p0; 153.7 p1; 131.3 p2 | ||||||
| sEMG BF | HR | 114.8 p0; 109.9 p1; 121.3 p2 | p < 0.0001 (p1); p < 0.001 (p2) | ||||
| CG | 113 p0; 237.7 p1; 228.4 p2 | ||||||
| Chen, 2021 [60] | 15 | Rate of perceived exertion | FR | 12.17 | 0.89 | p = 0.93 | |
| GW + VFR | 6.7 | 1.6 | |||||
| Rahimi, 2020 [62] | 17 | Hooper questionnaire | FR vs. PR Lower scores FR (2–3° md) FR vs. PR No difference FR vs. PR Differences at 3° md 4–6 vs. 5–8 | p < 0.05 * | |||
| Rate of perceived exertion | p > 0.05 | ||||||
| Blood lactate (mmol/L) | p < 0.05 * | ||||||
| Giovanelli, 2018 [67] | 13 | Rate of perceived exertion | CG pre | 2.7 | 1.2 | p = 0.586 | |
| CG post | 2.8 | 1.1 | |||||
| FR pre | 2.6 | 1.1 | p = 0.054 | ||||
| FR post | 2.2 | 0.9 | |||||
| Rey, 2017 [73] | 18 | Total quality recovery test | CG pre | 15.57 | 1.33 | p between groups < 0.05 * | |
| CG post | 12.67 | 1.66 | |||||
| FR pre | 15.11 | 1.54 | |||||
| FR post | 15.00 | 1.67 | |||||
| Visual analogue scale | CG pre | 4.05 | 0.06 | p between groups < 0.05 * | |||
| CG post | 5.6 | 1.19 | |||||
| FR pre | 4.81 | 0.85 | |||||
| FR post | 4.83 | 1.02 | |||||
| D’Amico, 2017 [71] | 16 | Blood lactate (mmol/L) | Passive | Not specified | p > 0.05 | ||
| FR | |||||||
| Murray, 2016 [75] | 12 | Tensiomyography | CG | No differences between protocols on any variables | p > 0.05 | ||
| FR | |||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-Aranda, L.M.; Sanz-Matesanz, M.; García-Mantilla, E.D.; González-Fernández, F.T. Effects of Self-Myofascial Release on Athletes’ Physical Performance: A Systematic Review. J. Funct. Morphol. Kinesiol. 2024, 9, 20. https://doi.org/10.3390/jfmk9010020
Martínez-Aranda LM, Sanz-Matesanz M, García-Mantilla ED, González-Fernández FT. Effects of Self-Myofascial Release on Athletes’ Physical Performance: A Systematic Review. Journal of Functional Morphology and Kinesiology. 2024; 9(1):20. https://doi.org/10.3390/jfmk9010020
Chicago/Turabian StyleMartínez-Aranda, Luis Manuel, Manuel Sanz-Matesanz, Ezequiel David García-Mantilla, and Francisco Tomás González-Fernández. 2024. "Effects of Self-Myofascial Release on Athletes’ Physical Performance: A Systematic Review" Journal of Functional Morphology and Kinesiology 9, no. 1: 20. https://doi.org/10.3390/jfmk9010020
APA StyleMartínez-Aranda, L. M., Sanz-Matesanz, M., García-Mantilla, E. D., & González-Fernández, F. T. (2024). Effects of Self-Myofascial Release on Athletes’ Physical Performance: A Systematic Review. Journal of Functional Morphology and Kinesiology, 9(1), 20. https://doi.org/10.3390/jfmk9010020