
Elastic Taping Application on the Neck: Immediate and Short-Term Impacts on Pain and Mobility of Cervical Spine

 ,
, 
 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
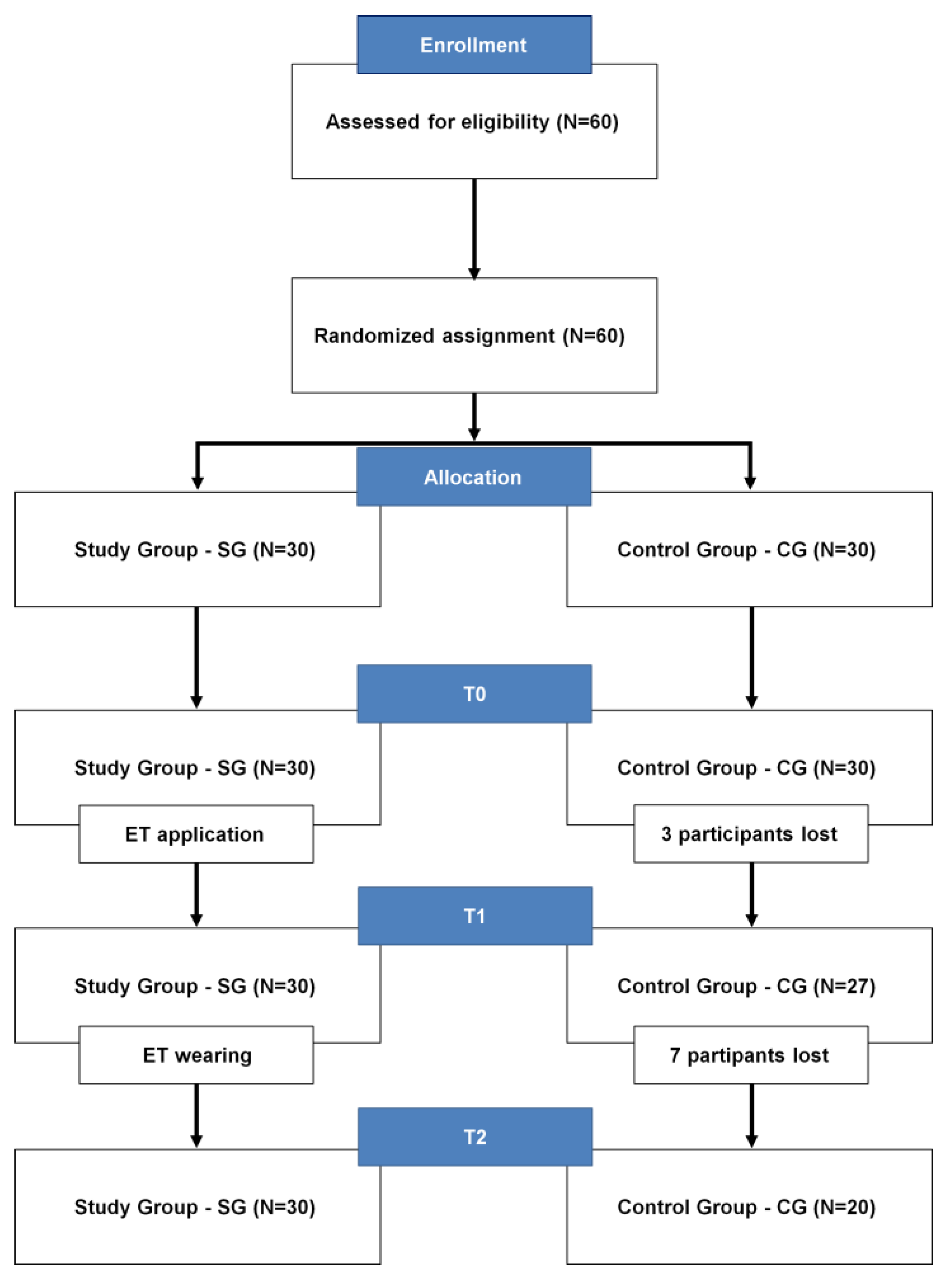
2.1. Design and Participants
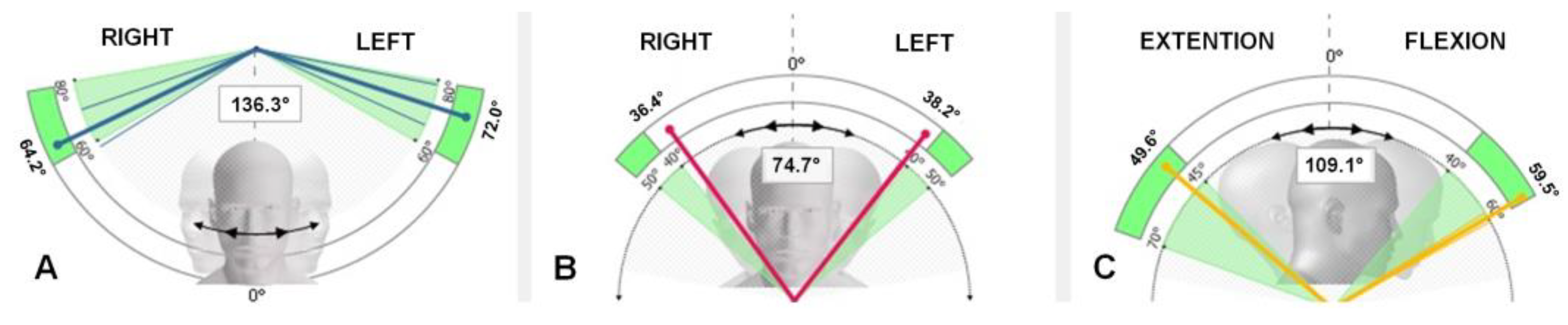
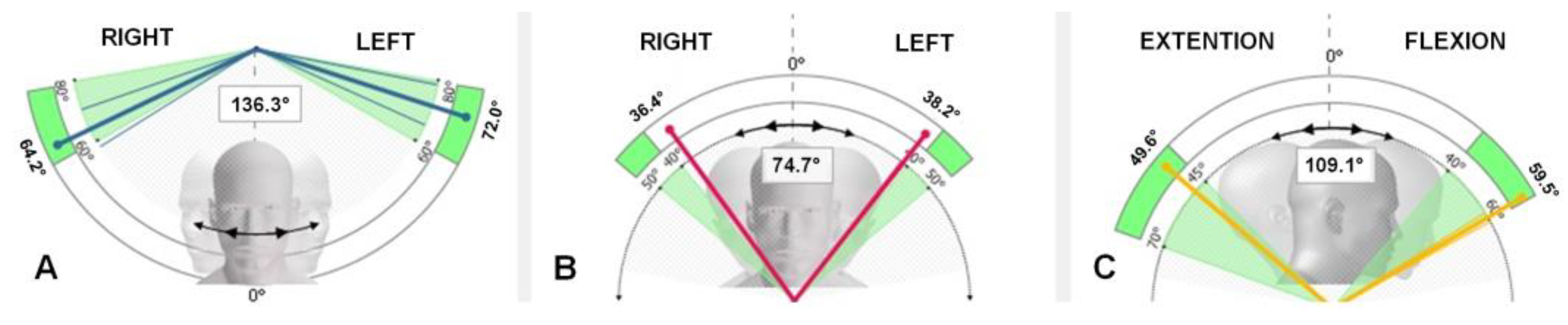
2.2. Instrumentation
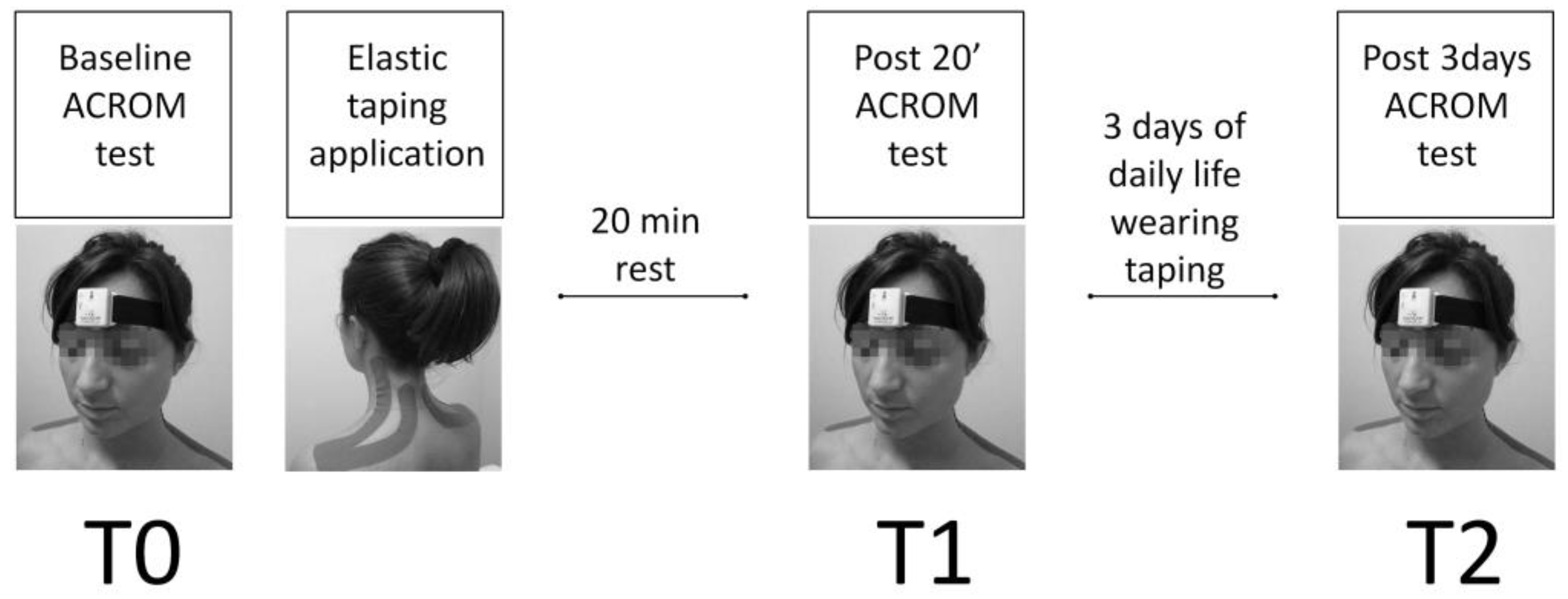
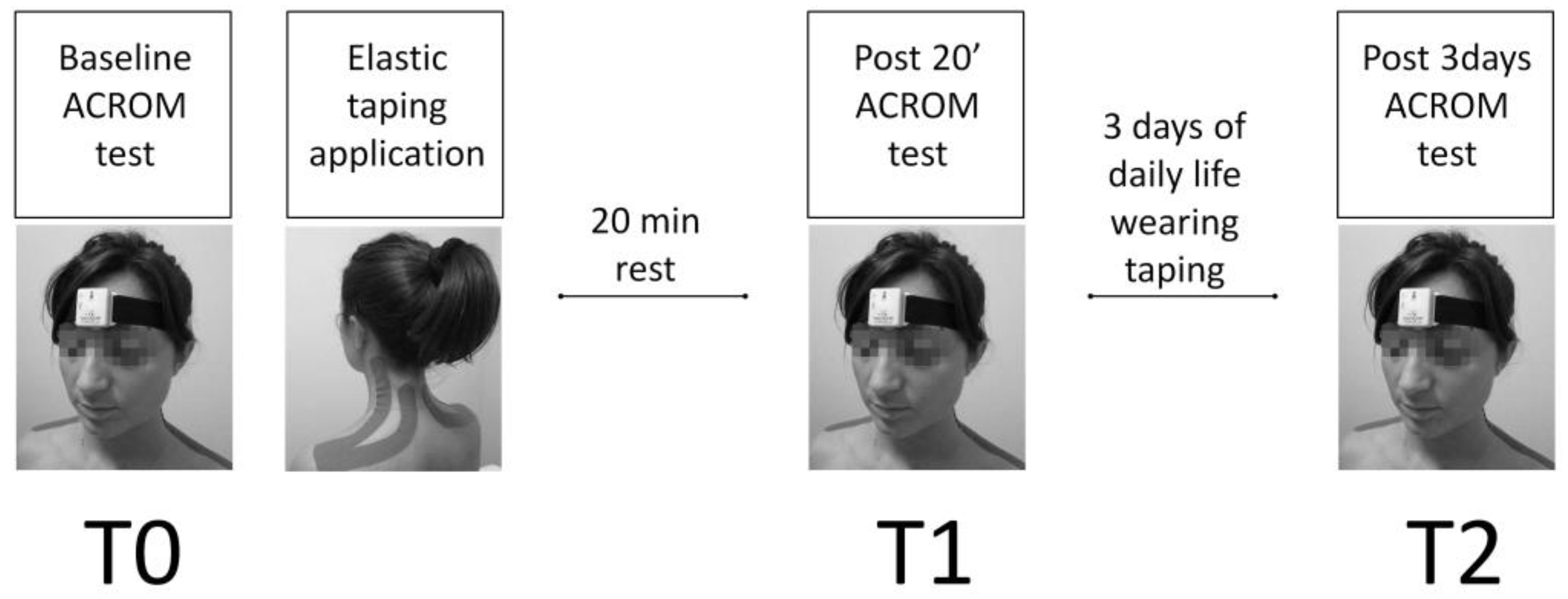
2.3. Procedure and Data Collection
2.4. Statistical Analysis
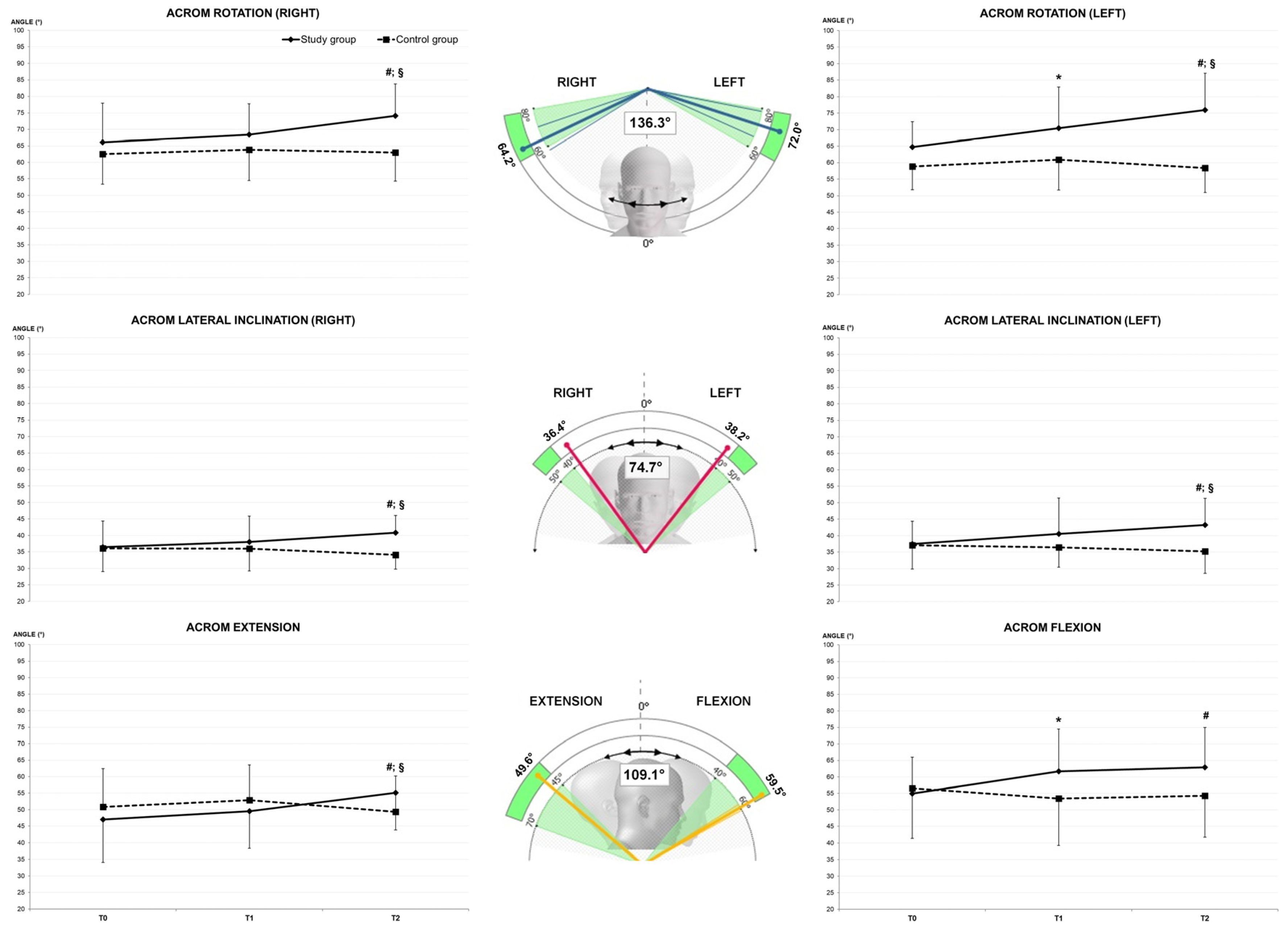
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Mean (SD) |
|---|---|
| Age (years) | 36.4 (7.3) |
| Body Height (cm) | 172.5 (7.8) |
| Body Mass (kg) | 73.3 (19.3) |
| Parameter | Inertial Sensor Mean (SD) | 3D Kinematics Mean (SD) | Z Score | p Value |
|---|---|---|---|---|
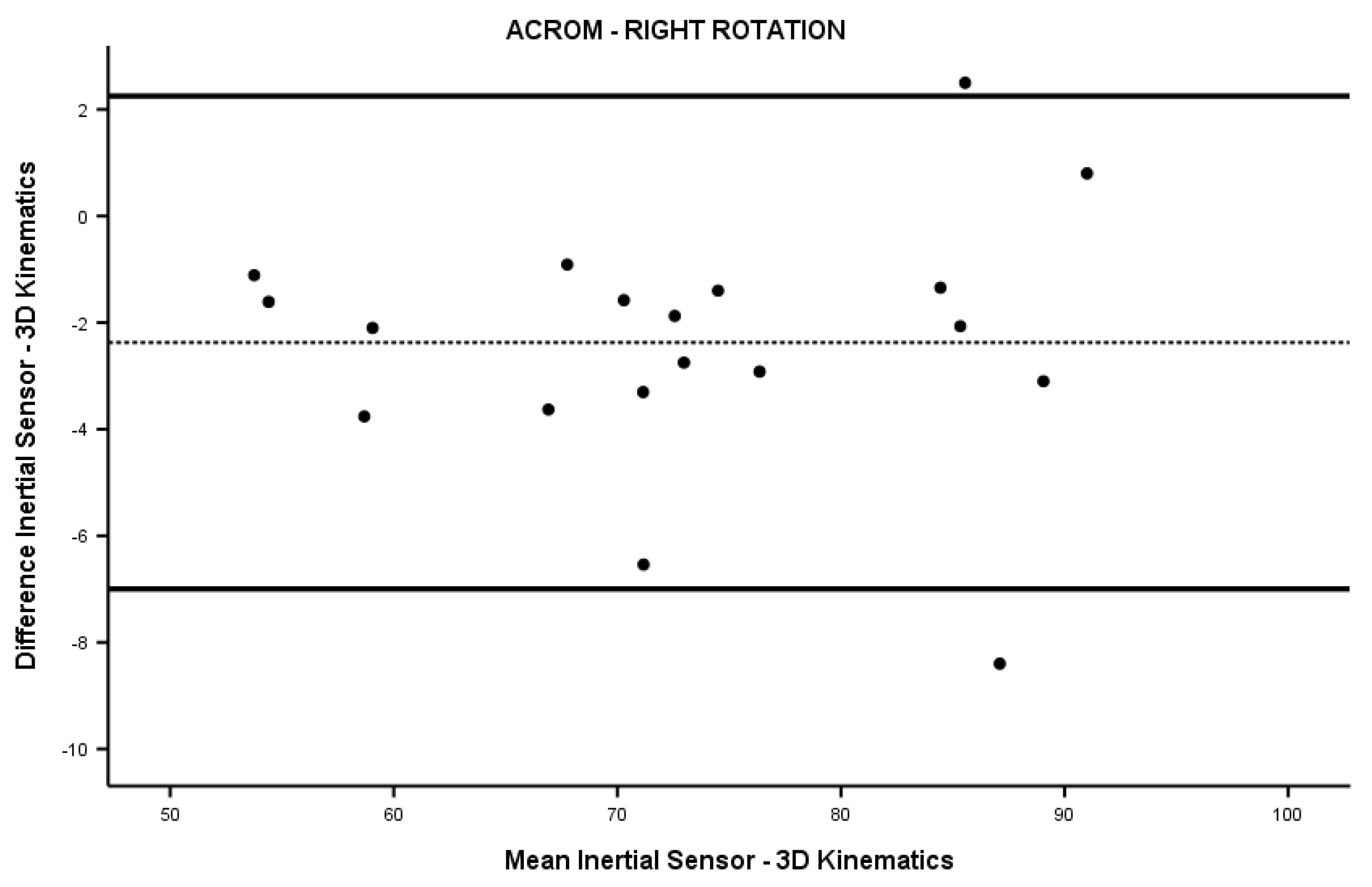
| Right rotation (°) | 72.1 (11.7) | 74.5 (11.6) | −0.818 | 0.414 |
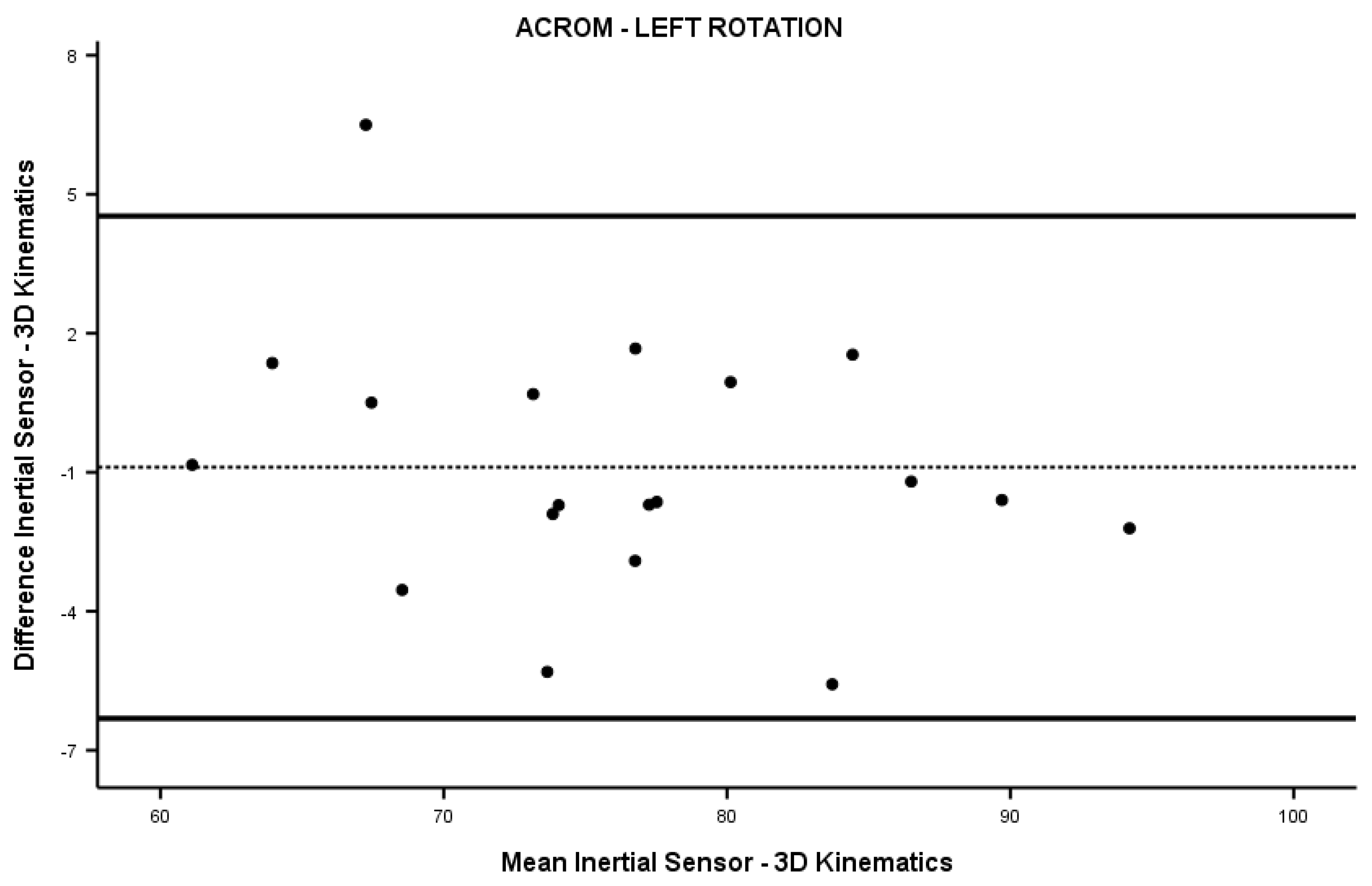
| Left rotation (°) | 75.9 (8.5) | 76.8 (9.2) | −0.336 | 0.737 |
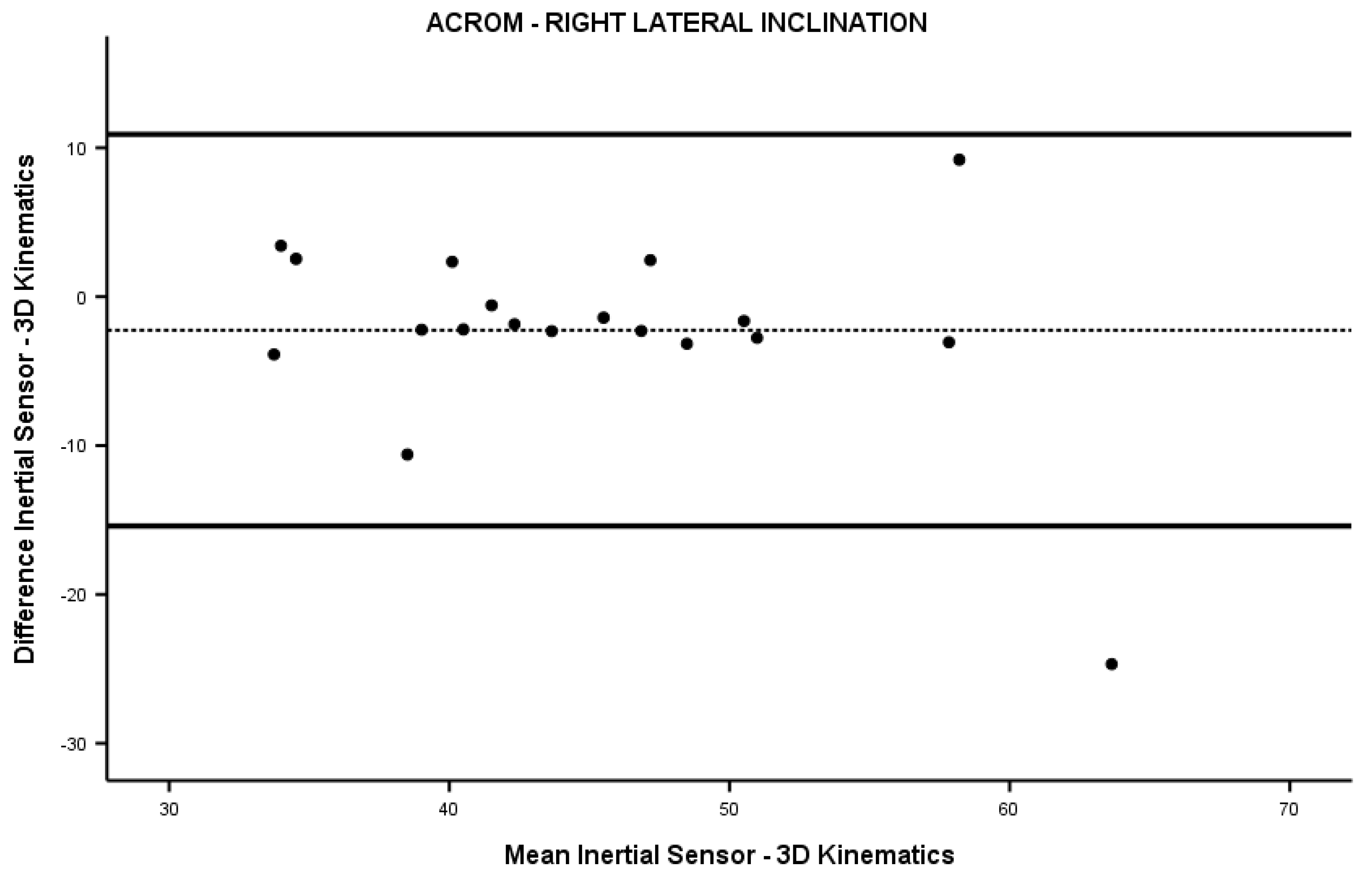
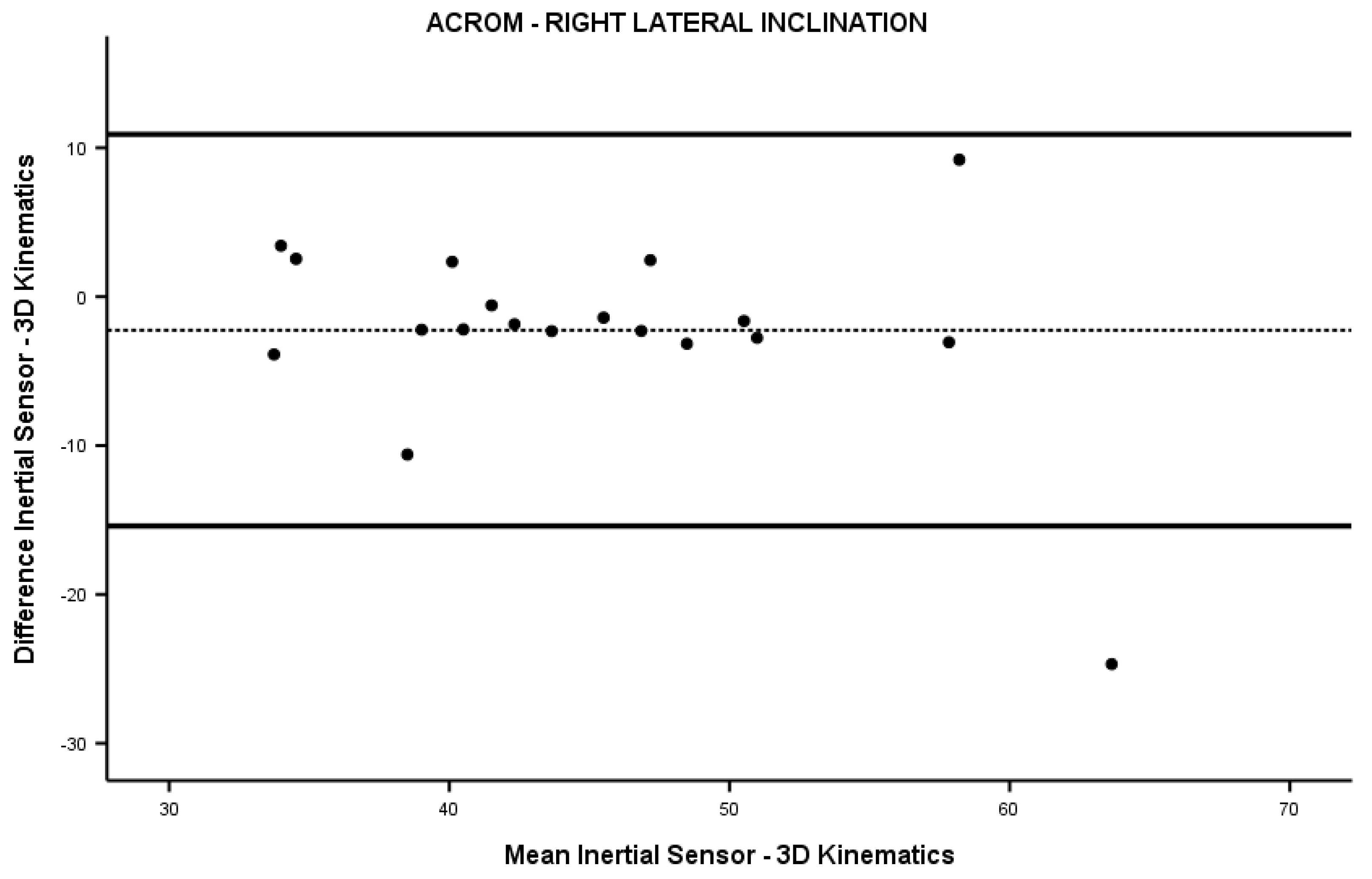
| Right lateral inclination (°) | 44.0 (7.9) | 46.2 (10.0) | −0.744 | 0.457 |
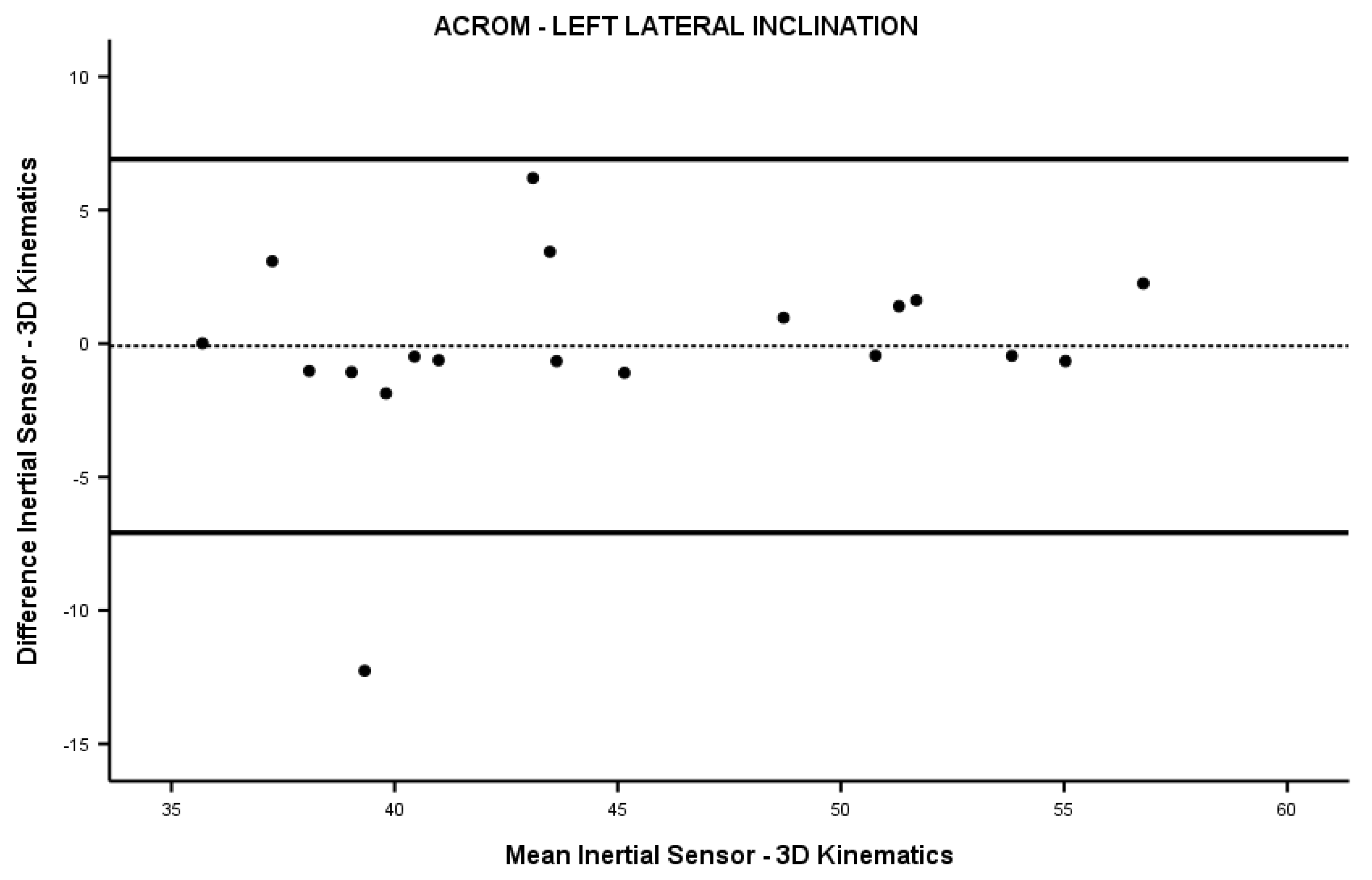
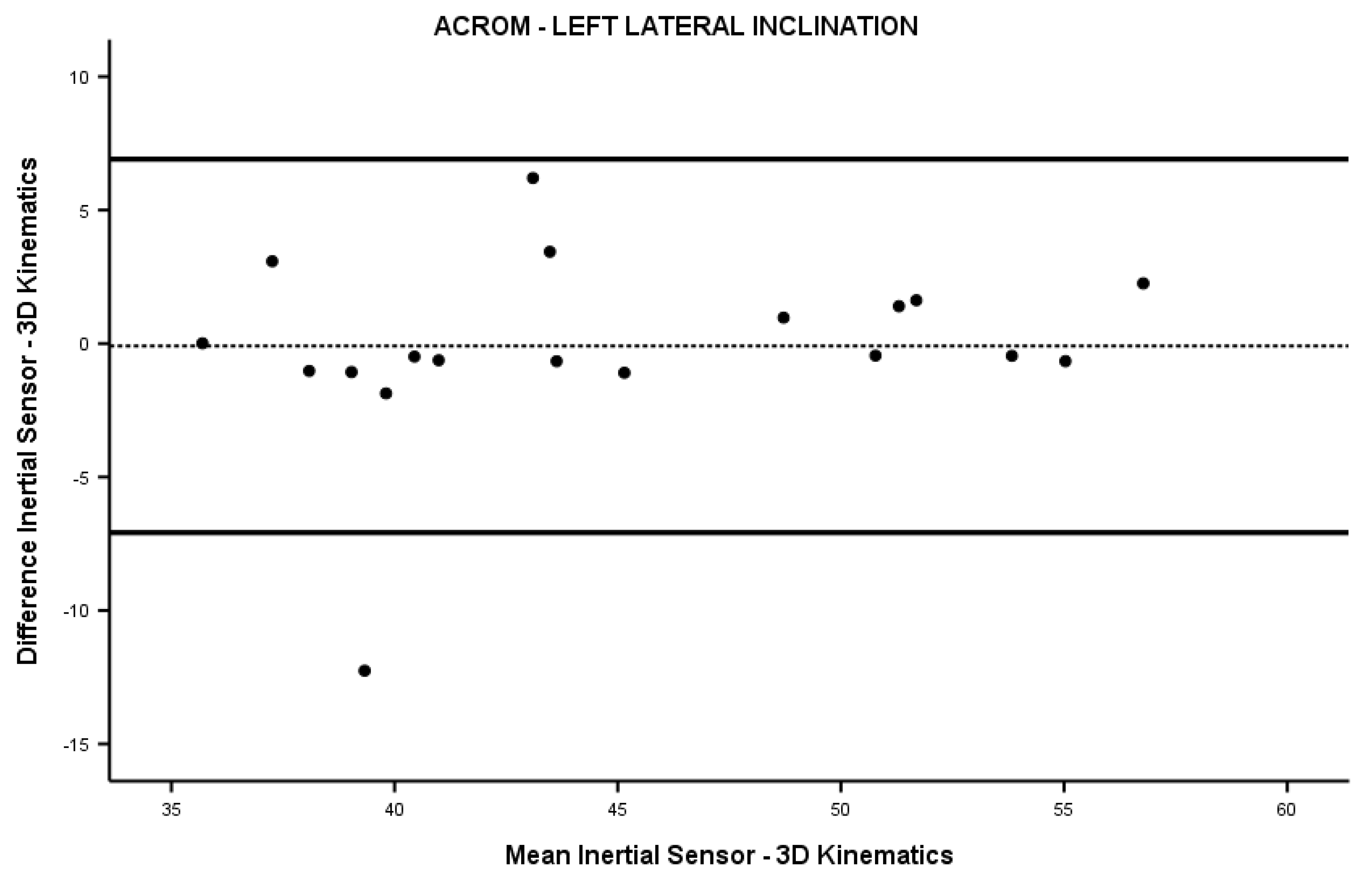
| Left lateral inclination (°) | 44.9 (7.2) | 45.0 (6.4) | −0.248 | 0.804 |
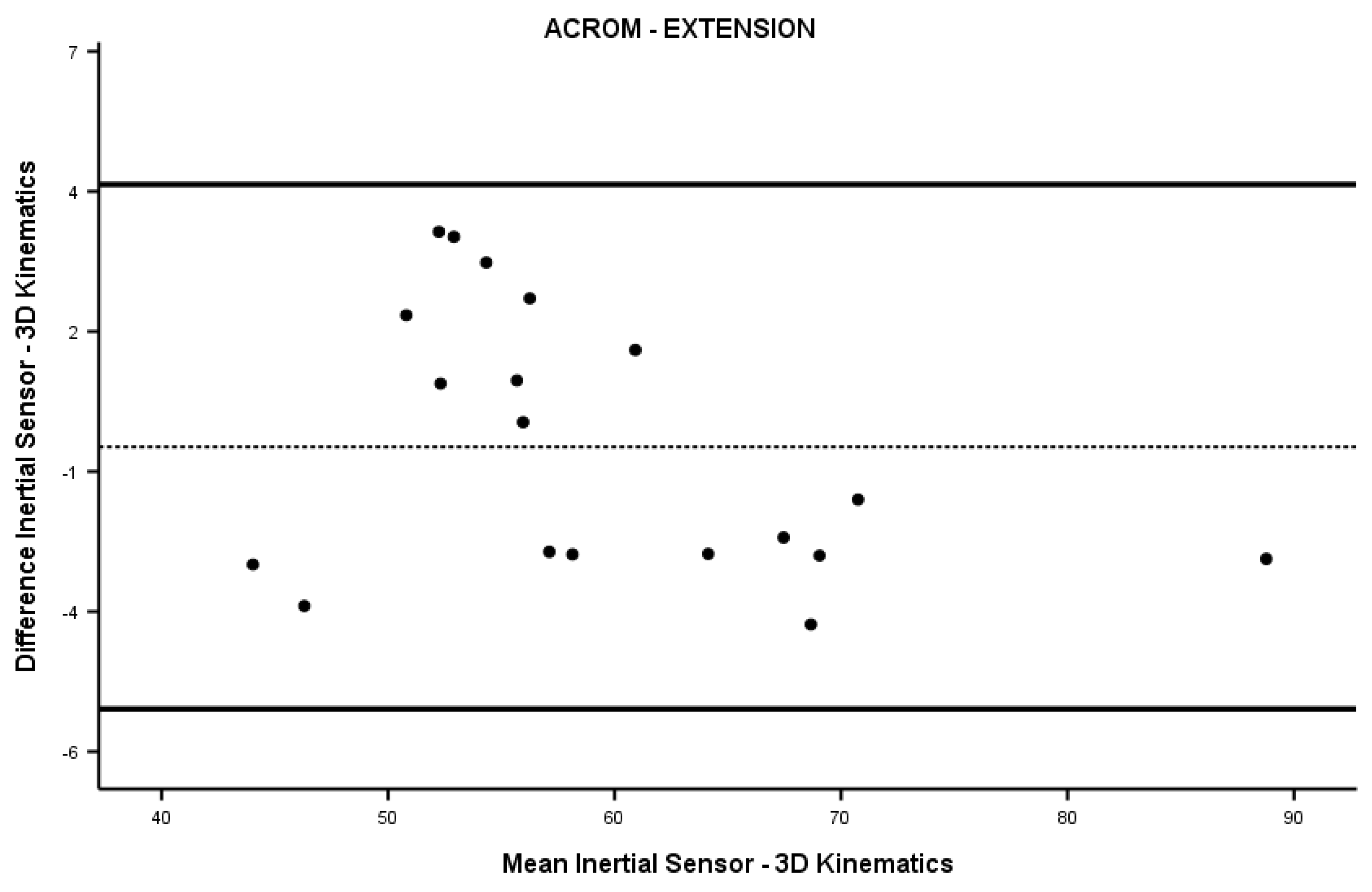
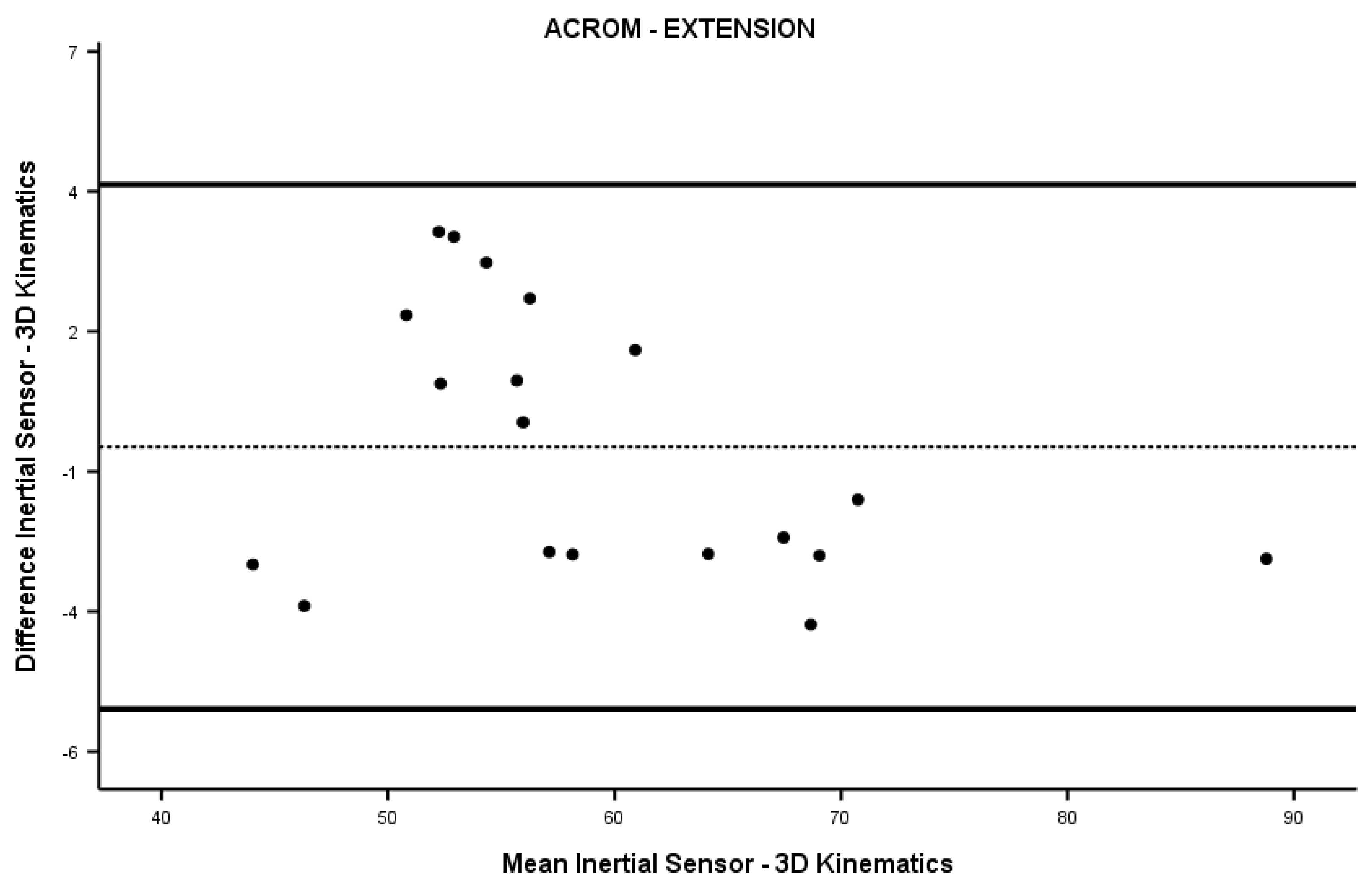
| Extension (°) | 59.0 (10.0) | 59.5 (10.9) | −0.044 | 0.965 |
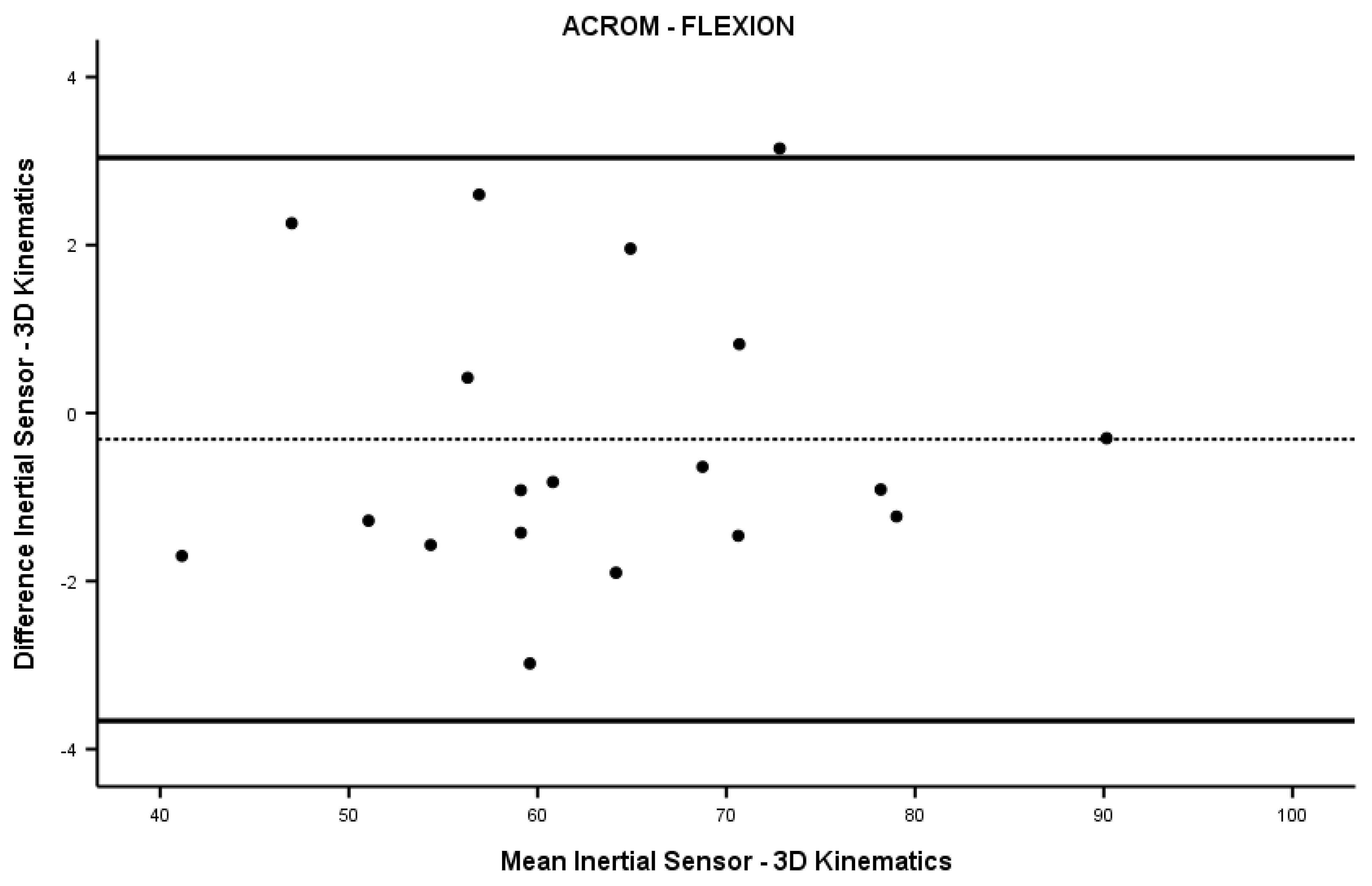
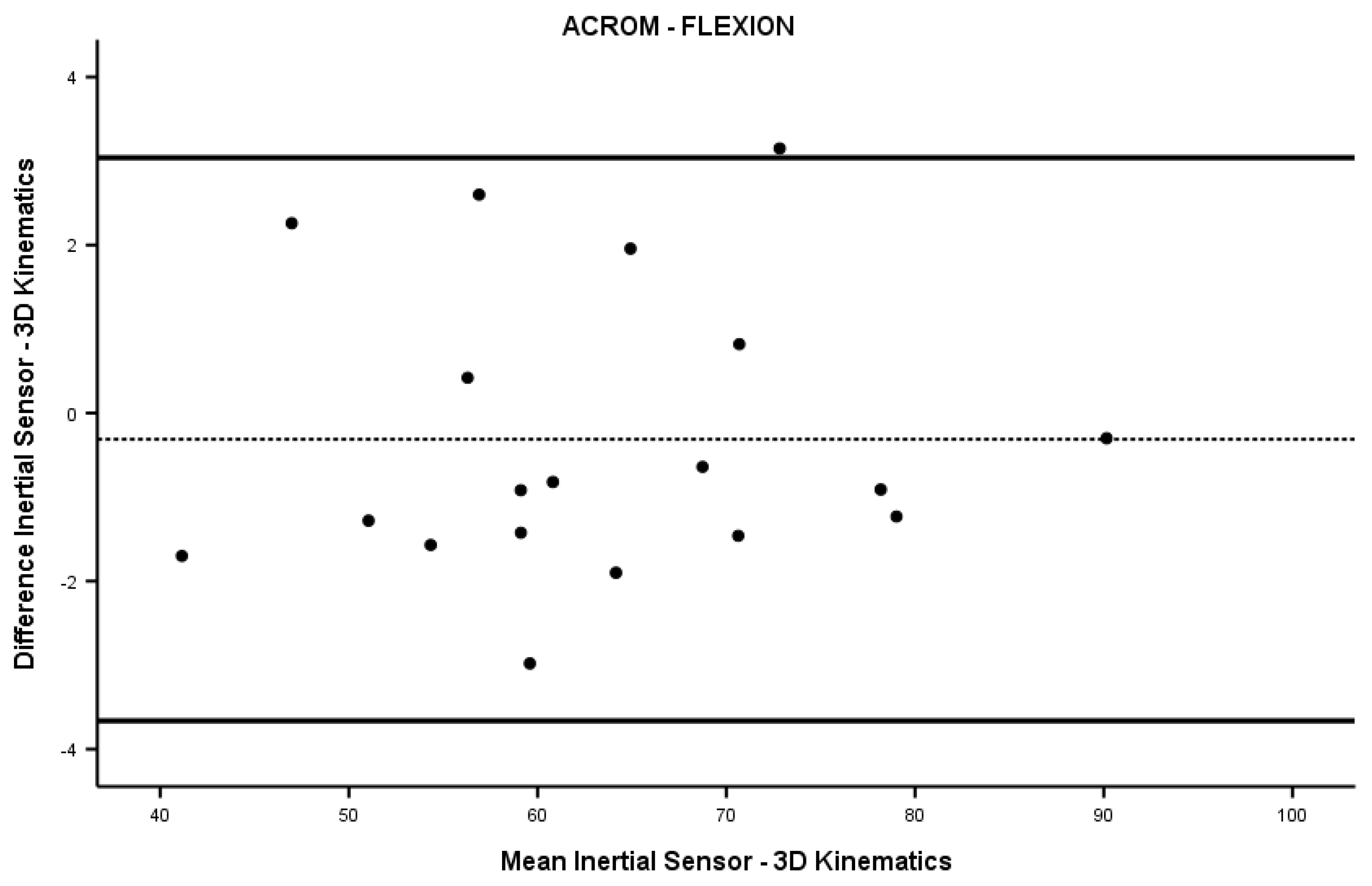
| Flexion (°) | 63.2 (12.0) | 63.6 (11.9) | −0.248 | 0.804 |


References
- Bogduk, N.; Mercer, S. Biomechanics of the Cervical Spine. I: Normal Kinematics. Clin. Biomech. 2000, 15, 633–648. [Google Scholar] [CrossRef]
- Shugg, J.A.J.; Jackson, C.D.; Dickey, J.P. Cervical Spine Rotation and Range of Motion: Pilot Measurements during Driving. Traffic Inj. Prev. 2011, 12, 82–87. [Google Scholar] [CrossRef] [PubMed]
- Thoomes-de Graaf, M.; Thoomes, E.; Fernández-de-las-Peñas, C.; Plaza-Manzano, G.; Cleland, J.A. Normative Values of Cervical Range of Motion for Both Children and Adults: A Systematic Review. Musculoskelet. Sci. Pract. 2020, 49, 102182. [Google Scholar] [CrossRef]
- Dowdell, J.; Kim, J.; Overley, S.; Hecht, A. Biomechanics and Common Mechanisms of Injury of the Cervical Spine. Handb. Clin. Neurol. 2018, 158, 337–344. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.J.; Han, H.Y.; Cheon, S.H.; Park, S.H.; Yong, M.S. The Effect of Forward Head Posture on Muscle Activity during Neck Protraction and Retraction. J. Phys. Ther. Sci. 2015, 27, 977–979. [Google Scholar] [CrossRef] [PubMed]
- Cheon, S.H.; Park, S.H. Changes in Neck and Upper Trunk Muscle Activities According to the Angle of Movement of the Neck in Subjects with Forward Head Posture. J. Phys. Ther. Sci. 2017, 29, 191–193. [Google Scholar] [CrossRef]
- Gareiss, L.; Krumm, A.; Otte, A. On Biomechanics of the Cervical Spine When Using a Smartphone. MMW Fortschr. Med. 2020, 162, 10–14. [Google Scholar] [CrossRef]
- Johnston, V.; Jull, G.; Souvlis, T.; Jimmieson, N.L. Neck Movement and Muscle Activity Characteristics in Female Office Workers with Neck Pain. Spine 2008, 33, 555–563. [Google Scholar] [CrossRef]
- Hagen, K.B.; Harms-Ringdahl, K.; Enger, N.O.; Hedenstad, R.; Morten, H. Relationship between Subjective Neck Disorders and Cervical Spine Mobility and Motion-Related Pain in Male Machine Operators. Spine 1997, 22, 1501–1507. [Google Scholar] [CrossRef]
- Jordan, A.; Mehlsen, J.; Ostergaard, K. A comparison of physical characteristics between patients seeking treatment for neck pain and age-matched healthy people. J. Manip. Physiol. Ther. 1997, 20, 468–475. [Google Scholar]
- Woodhouse, A.; Vasseljen, O. Altered Motor Control Patterns in Whiplash and Chronic Neck Pain. BMC Musculoskelet. Disord. 2008, 9, 90. [Google Scholar] [CrossRef]
- Stenneberg, M.S.; Rood, M.; de Bie, R.; Schmitt, M.A.; Cattrysse, E.; Scholten-Peeters, G.G. To What Degree Does Active Cervical Range of Motion Differ Between Patients With Neck Pain, Patients With Whiplash, and Those Without Neck Pain? A Systematic Review and Meta-Analysis. Arch. Phys. Med. Rehabil. 2017, 98, 1407–1434. [Google Scholar] [CrossRef]
- Lee, H.; Nicholson, L.L.; Adams, R.D. Neck Muscle Endurance, Self-Report, and Range of Motion Data from Subjects with Treated and Untreated Neck Pain. J. Manip. Physiol. Ther. 2005, 28, 25–32. [Google Scholar] [CrossRef]
- Williams, M.A.; McCarthy, C.J.; Chorti, A.; Cooke, M.W.; Gates, S. A Systematic Review of Reliability and Validity Studies of Methods for Measuring Active and Passive Cervical Range of Motion. J. Manip. Physiol. Ther. 2010, 33, 138–155. [Google Scholar] [CrossRef]
- Jull, G.A.; O’Leary, S.P.; Falla, D.L. Clinical Assessment of the Deep Cervical Flexor Muscles: The Craniocervical Flexion Test. J. Manip. Physiol. Ther. 2008, 31, 525–533. [Google Scholar] [CrossRef]
- Belli, G.; Toselli, S.; Mauro, M.; Maietta Latessa, P.; Russo, L. Relation between Photogrammetry and Spinal Mouse for Sagittal Imbalance Assessment in Adolescents with Thoracic Kyphosis. J. Funct. Morphol. Kinesiol. 2023, 8, 68. [Google Scholar] [CrossRef] [PubMed]
- Russo, L.; Belli, G.; Di Blasio, A.; Lupu, E.; Larion, A.; Fischetti, F.; Montagnani, E.; Di Biase Arrivabene, P.; De Angelis, M. The Impact of Nordic Walking Pole Length on Gait Kinematic Parameters. J. Funct. Morphol. Kinesiol. 2023, 8, 50. [Google Scholar] [CrossRef] [PubMed]
- Di Giminiani, R.; Di Lorenzo, D.; La Greca, S.; Russo, L.; Masedu, F.; Totaro, R.; Padua, E. Angle-Angle Diagrams in the Assessment of Locomotion in Persons with Multiple Sclerosis: A Preliminary Study. Appl. Sci. 2022, 12, 7223. [Google Scholar] [CrossRef]
- Raya, R.; Garcia-Carmona, R.; Sanchez, C.; Urendes, E.; Ramirez, O.; Martin, A.; Otero, A. An Inexpensive and Easy to Use Cervical Range of Motion Measurement Solution Using Inertial Sensors. Sensors 2018, 18, 2582. [Google Scholar] [CrossRef]
- Elizagaray-García, I.; Gil-Martínez, A.; Navarro-Fernández, G.; Navarro-Moreno, A.R.; Sánchez-De-toro-hernández, J.; Díaz-De-terán, J.; Lerma-Lara, S. Inter, Intra-Examiner Reliability and Validity of Inertial Sensors to Measure the Active Cervical Range of Motion in Patients with Primary Headache. EXCLI J. 2021, 20, 879–893. [Google Scholar] [CrossRef]
- Russo, L.; Giustino, V.; Toscano, R.E.; Secolo, G.; Secolo, I.; Iovane, A.; Messina, G. Can Tongue Position and Cervical ROM Affect Postural Oscillations? A Pilot and Preliminary Study. J. Hum. Sport Exerc. 2020, 15, S840–S847. [Google Scholar] [CrossRef]
- Theobald, P.S.; Jones, M.D.; Williams, J.M. Do Inertial Sensors Represent a Viable Method to Reliably Measure Cervical Spine Range of Motion? Man Ther. 2012, 17, 92–96. [Google Scholar] [CrossRef] [PubMed]
- Wood, S.; Fryer, G.; Tan, L.L.F.; Cleary, C. Dry Cupping for Musculoskeletal Pain and Range of Motion: A Systematic Review and Meta-Analysis. J. Bodyw. Mov. Ther. 2020, 24, 503–518. [Google Scholar] [CrossRef] [PubMed]
- Saavedra-Hernández, M.; Castro-Sánchez, A.M.; Arroyo-Morales, M.; Cleland, J.A.; Lara-Palomo, I.C.; Fernández-De-Las-Peñas, C. Short-Term Effects of Kinesio Taping versus Cervical Thrust Manipulation in Patients with Mechanical Neck Pain: A Randomized Clinical Trial. J. Orthop. Sports Phys. Ther. 2012, 42, 724–730. [Google Scholar] [CrossRef]
- Xiong, J.; Zhang, Z.; Zhang, Z.; Ma, Y.; Li, Z.; Chen, Y.; Liu, Q.; Liao, W. Short-Term Effects of Kinesio Taping Combined with Cervical Muscles Multi-Angle Isometric Training in Patients with Cervical Spondylosis. BMC Musculoskelet. Disord. 2023, 24, 38. [Google Scholar] [CrossRef]
- Šiško, P.K.; Videmšek, M.; Karpljuk, D. The Effect of a Corporate Chair Massage Program on Musculoskeletal Discomfort and Joint Range of Motion in Office Workers. J. Altern. Complement. Med. 2011, 17, 617–622. [Google Scholar] [CrossRef]
- Tsauo, J.Y.; Lee, H.Y.; Hsu, J.H.; Chen, C.Y.; Chen, C.J. Physical Exercise and Health Education for Neck and Shoulder Complaints among Sedentary Workers. J. Rehabil. Med. 2004, 36, 253–257. [Google Scholar] [CrossRef]
- Williams, S.; Whatman, C.; Hume, P.A.; Sheerin, K. Kinesio Taping in Treatment and Prevention of Sports Injuries: A Meta-Analysis of the Evidence for Its Effectiveness. Sports Med. 2012, 42, 153–164. [Google Scholar] [CrossRef]
- Russo, L.; Bartolucci, P.; Ardigò, L.P.; Padulo, J.; Pausic, J.; Iacono, A. Dello An Exploratory Study on the Acute Effects of Proprioceptive Exercise and/or Neuromuscular Taping on Balance Performance. Asian J. Sports Med. 2018, 9, 63020. [Google Scholar] [CrossRef]
- Erdoğanoğlu, Y.; Bayraklı, B. Short-Term Changes in Chronic Neck Pain After the Use of Elastic Adhesive Tape. J. Chiropr. Med. 2021, 20, 70–76. [Google Scholar] [CrossRef]
- Alahmari, K.A.; Reddy, R.S.; Tedla, J.S.; Samuel, P.S.; Kakaraparthi, V.N.; Rengaramanujam, K.; Ahmed, I. The Effect of Kinesio Taping on Cervical Proprioception in Athletes with Mechanical Neck Pain-a Placebo-Controlled Trial. BMC Musculoskelet. Disord. 2020, 21, 648. [Google Scholar] [CrossRef]
- Ay, S.; Konak, H.E.; Evcik, D.; Kibar, S. The Effectiveness of Kinesio Taping on Pain and Disability in Cervical Myofascial Pain Syndrome. Rev. Bras. Reumatol. 2017, 57, 93–99. [Google Scholar] [CrossRef]
- Russo, L.; Montagnani, E.; Pietrantuono, D.; D’Angona, F.; Fratini, T.; Di Giminiani, R.; Palermi, S.; Ceccarini, F.; Migliaccio, G.M.; Lupu, E.; et al. Self-Myofascial Release of the Foot Plantar Surface: The Effects of a Single Exercise Session on the Posterior Muscular Chain Flexibility after One Hour. Int. J. Environ. Res. Public Health 2023, 20, 974. [Google Scholar] [CrossRef] [PubMed]
- Russo, L.; Bartolucci, P. Taping Elastico® Applicazioni in Chinesiologia; ATS—Giacomo Catalani Editore: Arezzo, Italy, 2018. [Google Scholar]
- Richardson, J.T.E. Eta squared and partial eta squared as measures of effect size in educational research. Educ. Res. Rev. 2011, 6, 135–147. [Google Scholar] [CrossRef]
- Lakens, D. Calculating and reporting effect sizes to facilitate cumulative science: A practical primer for t-tests and ANOVAs. Front. Psychol. 2013, 4, 63. [Google Scholar] [CrossRef] [PubMed]
- Korthals-de Bos, I.B.C.; Hoving, J.L.; Van Tulder, M.W.; Rutten-van Mölken, M.P.M.H.; Adèr, H.J.; De Vet, H.C.W.; Koes, B.W.; Vondeling, H.; Bouter, L.M. Cost Effectiveness of Physiotherapy, Manual Therapy, and General Practitioner Care for Neck Pain: Economic Evaluation alongside a Randomised Controlled Trial. BMJ 2003, 326, 911–914. [Google Scholar] [CrossRef] [PubMed]
- Driessen, M.T.; Lin, C.W.C.; Van Tulder, M.W. Cost-Effectiveness of Conservative Treatments for Neck Pain: A Systematic Review on Economic Evaluations. Eur. Spine J. 2012, 21, 1441–1450. [Google Scholar] [CrossRef]
- Aboagye, E.; Lilje, S.; Bengtsson, C.; Peterson, A.; Persson, U.; Skillgate, E. Manual Therapy versus Advice to Stay Active for Nonspecific Back and/or Neck Pain: A Cost-Effectiveness Analysis. Chiropr. Man Therap. 2022, 30, 27. [Google Scholar] [CrossRef]
- Hoy, D.; March, L.; Woolf, A.; Blyth, F.; Brooks, P.; Smith, E.; Vos, T.; Jan, B.; Blore, J.; Murray, C.; et al. The Global Burden of Neck Pain: Estimates from the Global Burden of Disease 2010 Study. Ann. Rheum. Dis. 2014, 73, 1309–1315. [Google Scholar] [CrossRef]
- Yang, J.M.; Lee, J.H. Is Kinesio Taping to Generate Skin Convolutions Effective for Increasing Local Blood Circulation? Med. Sci. Monit. 2018, 24, 288–293. [Google Scholar] [CrossRef]
- Craighead, D.H.; Shank, S.W.; Volz, K.M.; Alexander, L.M. Kinesiology Tape Modestly Increases Skin Blood Flow Regardless of Tape Application Technique. JPHR J. Perform. Health Res. 2017, 1, 72–78. [Google Scholar] [CrossRef]
- Banerjee, G.; Briggs, M.; Johnson, M.I. The Immediate Effects of Kinesiology Taping on Cutaneous Blood Flow in Healthy Humans under Resting Conditions: A Randomised Controlled Repeated-Measures Laboratory Study. PLoS ONE 2020, 15, e0229386. [Google Scholar] [CrossRef]
- Parreira, P.D.C.S.; Costa, L.D.C.M.; Takahashi, R.; Junior, L.C.H.; da Luz Junior, M.A.; da Silva, T.M.; Costa, L.O.P. Kinesio Taping to Generate Skin Convolutions Is Not Better than Sham Taping for People with Chronic Non-Specific Low Back Pain: A Randomised Trial. J. Physiother. 2014, 60, 90–96. [Google Scholar] [CrossRef] [PubMed]
- Araujo, A.C.; do Carmo Silva Parreira, P.; Junior, L.C.H.; da Silva, T.M.; da Luz Junior, M.A.; da Cunha Menezes Costa, L.; Pena Costa, L.O. Medium Term Effects of Kinesio Taping in Patients with Chronic Non-Specific Low Back Pain: A Randomized Controlled Trial. Physiotherapy 2018, 104, 149–151. [Google Scholar] [CrossRef] [PubMed]
- Vercelli, S.; Colombo, C.; Tolosa, F.; Moriondo, A.; Bravini, E.; Ferriero, G.; Francesco, S. The Effects of Kinesio Taping on the Color Intensity of Superficial Skin Hematomas: A Pilot Study. Phys. Ther. Sport 2017, 23, 156–161. [Google Scholar] [CrossRef] [PubMed]
- Pamuk, U.; Yucesoy, C.A. MRI Analyses Show That Kinesio Taping Affects Much More than Just the Targeted Superficial Tissues and Causes Heterogeneous Deformations within the Whole Limb. J. Biomech. 2015, 48, 4262–4270. [Google Scholar] [CrossRef]


| Parameter | F | p Value |
|---|---|---|
| ACROM right rotation (°) | 3.764 | 0.027 |
| ACROM left rotation (°) | 8.034 | 0.001 |
| ACROM right lateral inclination (°) | 10.400 | 0.000 |
| ACROM left lateral inclination (°) | 7.537 | 0.001 |
| ACROM extension (°) | 7.435 | 0.001 |
| ACROM flexion (°) | 5.708 | 0.005 |
| Pain (A.U.) | 113.111 | 0.000 |
| Parameter | T0 | T1 | T2 | p Value | ||
|---|---|---|---|---|---|---|
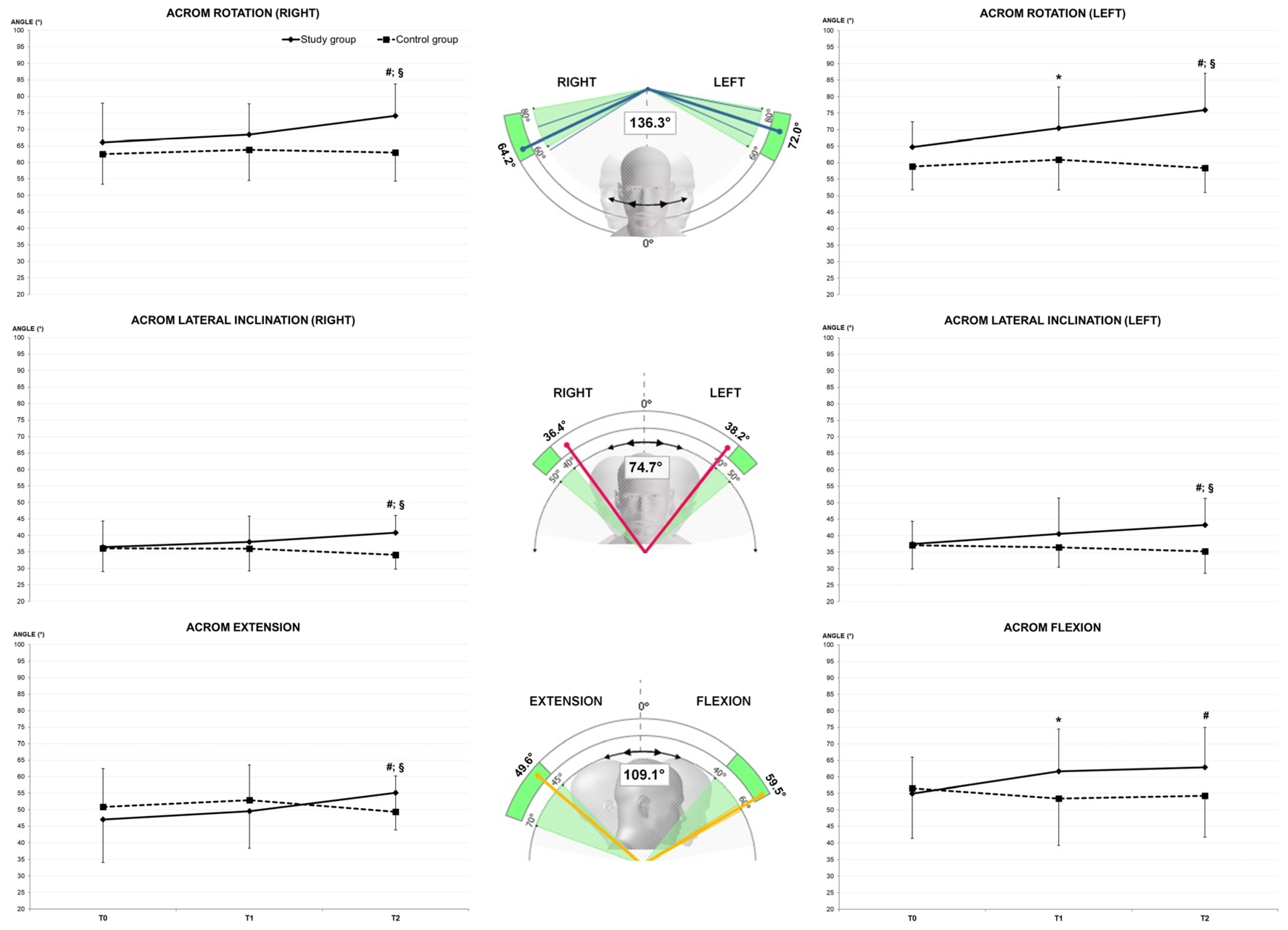
| Study Group (SG) | ACROM right rotation (°) | 66.0 ± 11.9 | 68.4 ± 9.3 | 74.2 ± 9.6 #§ | 0.432 | 0.000 |
| ACROM left rotation (°) | 64.8 ± 7.7 | 70.4 ± 12.5 * | 76.0 ± 11.1 #§ | 0.599 | 0.000 | |
| ACROM right lateral inclination (°) | 36.5 ± 7.9 | 38.0 ± 7.9 | 40.9 ± 5.2 #§ | 0.452 | 0.000 | |
| ACROM left lateral inclination (°) | 37.5 ± 6.9 | 40.6 ± 10.8 | 43.2 ± 8.0 #§ | 0.554 | 0.000 | |
| ACROM extension (°) | 47.0 ± 12.9 | 49.6 ± 11.3 | 55.1 ± 11.3 #§ | 0.360 | 0.000 | |
| ACROM flexion (°) | 55.0 ± 3.6 | 61.7 ± 12.8 * | 62.9 ± 12.0 # | 0.288 | 0.002 | |
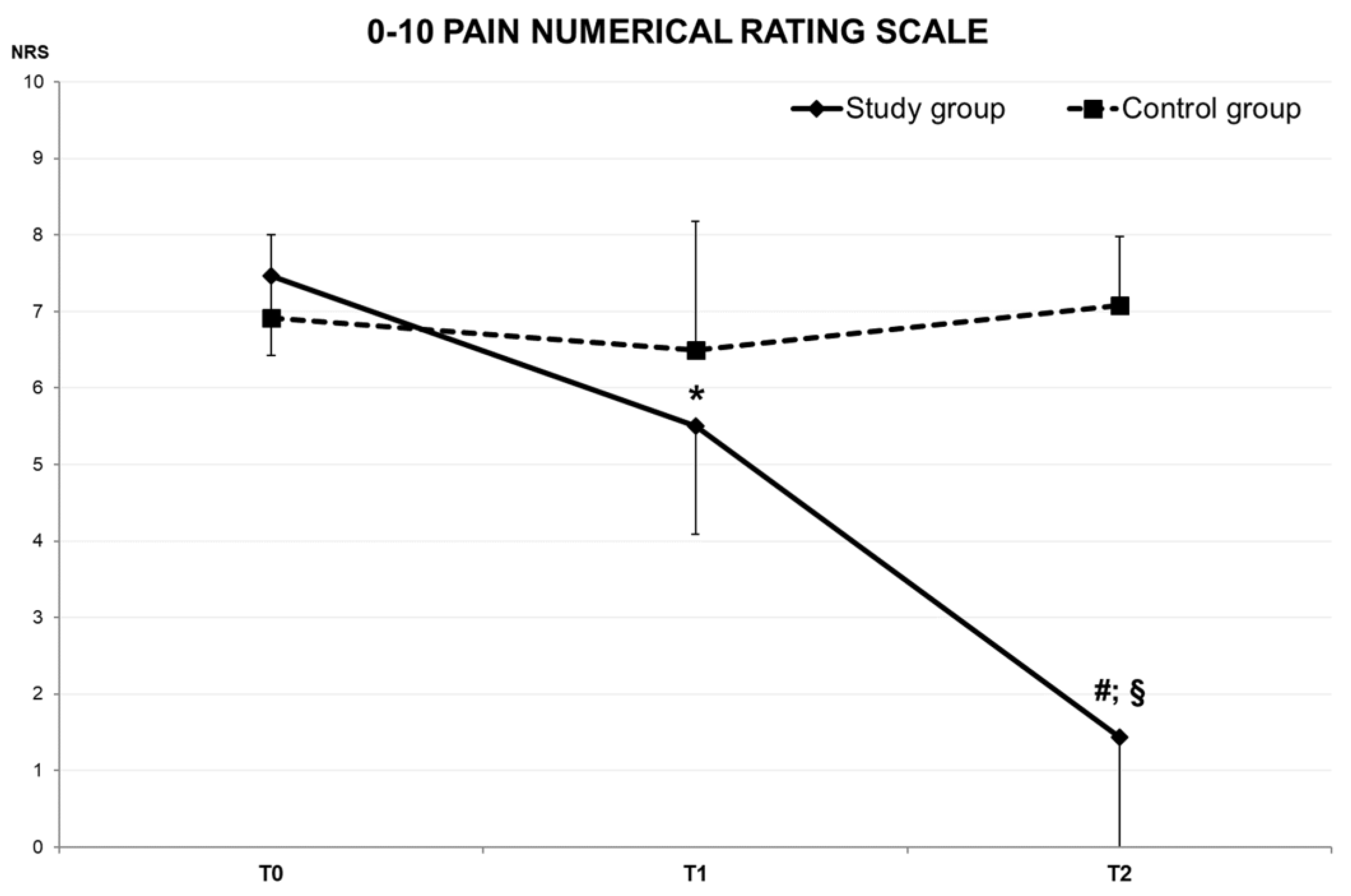
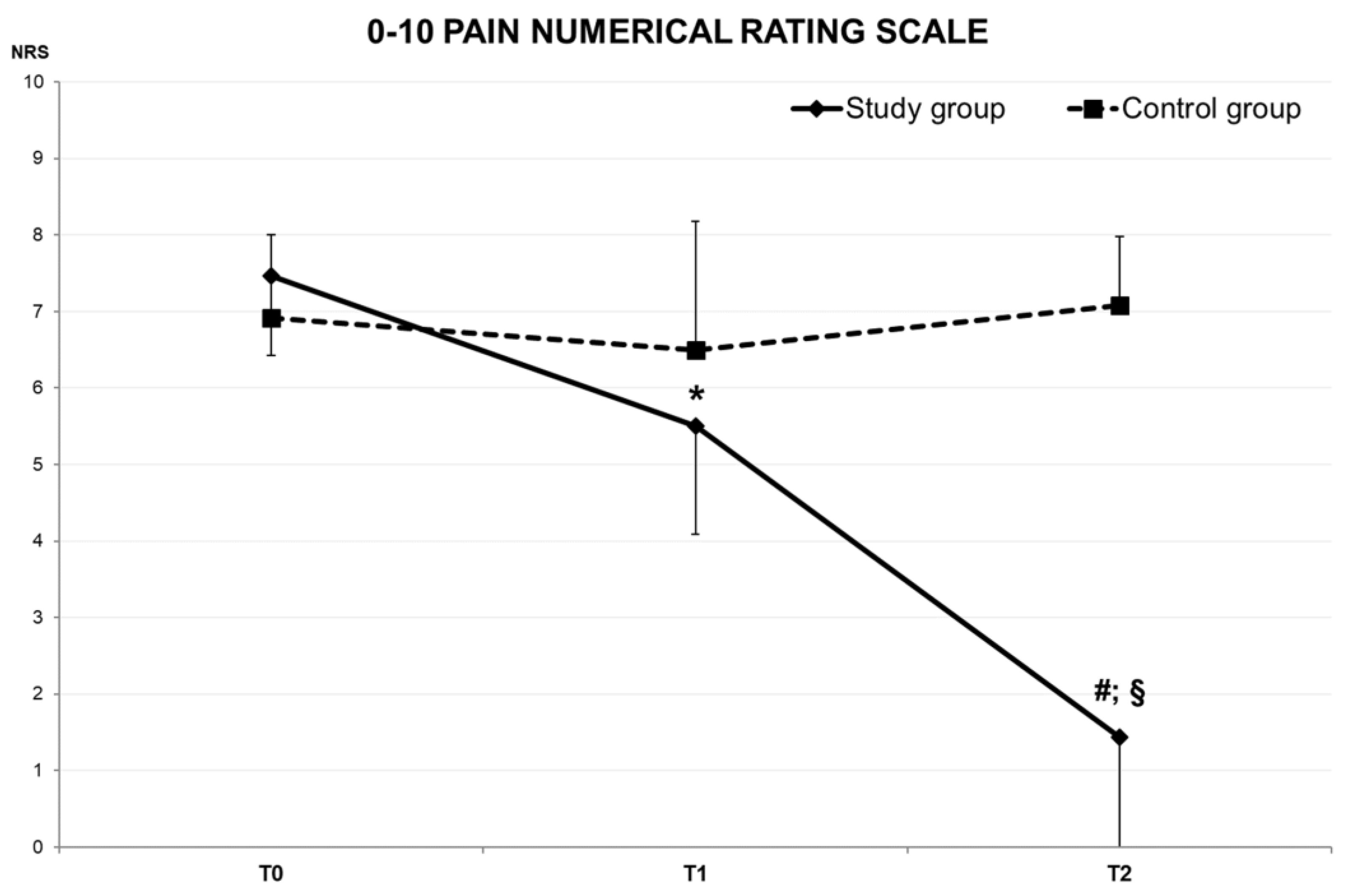
| Pain (A.U.) | 7.5 ± 1.0 | 5.5 ± 1.4 * | 1.4 ± 1.5 #§ | 0.945 | 0.000 | |
| Control Group (CG) | ACROM right rotation (°) | 62.5 ± 9.1 | 63.8 ± 9.3 | 63.0 ± 8.7 | 0.017 | 0.569 |
| ACROM left rotation (°) | 58.8 ± 7.0 | 60.9 ± 9.2 | 58.4 ± 7.5 | 0.012 | 0.630 | |
| ACROM right lateral inclination (°) | 36.0 ± 7.0 | 36.0 ± 6.7 | 34.1 ± 4.2 | 0.094 | 0.175 | |
| ACROM left lateral inclination (°) | 37.1 ± 7.1 | 36.4 ± 6.0 | 35.2 ± 6.6 | 0.009 | 0.675 | |
| ACROM extension (°) | 50.9 ± 11.6 | 52.9 ± 10.7 | 49.3 ± 10.8 | 0.049 | 0.337 | |
| ACROM flexion (°) | 56.5 ± 15.2 | 53.4 ± 14.1 | 54.3 ± 12.5 | 0.081 | 0.211 | |
| Pain (a.u.) | 6.9 ± 1.1 | 6.5 ± 1.7 | 7.1 ± 0.9 | 0.056 | 0.438 |
| Parameter | T0 | T1 | T2 | p Value | ||
|---|---|---|---|---|---|---|
| Study Group (SG) | ACROM right rotation (°) | 65.9 ± 11.0 | 68.2 ± 7.6 | 74.3 ± 7.4 #§ | 0.415 | 0.000 |
| ACROM left rotation (°) | 64.7 ± 8.1 | 70.6 ± 9.9 * | 75.9 ± 7.9 #§ | 0.680 | 0.001 | |
| ACROM right lateral inclination (°) | 35.9 ± 7.4 | 37.5 ± 7.4 | 40.7 ± 4.9 #§ | 0.536 | 0.000 | |
| ACROM left lateral inclination (°) | 36.0 ± 6.0 | 38.9 ± 7.6 | 42.5 ± 6.9 #§ | 0.626 | 0.000 | |
| ACROM extension (°) | 47.3 ± 13.1 | 51.7 ± 8.0 | 55.1 ± 9.4 # | 0.327 | 0.004 | |
| ACROM flexion (°) | 55.6 ± 10.8 | 62.5 ± 11.3 * | 63.2 ± 10.6 | 0.241 | 0.017 | |
| Pain (A.U.) | 7.5 ± 1.1 | 5.8 ± 1.3 * | 1.5 ± 1.6 #§ | 0.938 | 0.000 | |
| Control Group (CG) | ACROM right rotation (°) | 64.3 ± 9.0 | 64.4 ± 6.9 | 64.4 ± 6.7 | 0.002 | 0.892 |
| ACROM left rotation (°) | 58.9 ± 7.2 | 62.7 ± 8.5 | 59.0 ± 6.9 | 0.000 | 0.948 | |
| ACROM right lateral inclination (°) | 38.2 ± 7.1 | 38.1 ± 5.7 | 35.6 ± 3.1 | 0.279 | 0.077 | |
| ACROM left lateral inclination (°) | 38.4 ± 7.4 | 38.5 ± 5.5 | 36.8 ± 6.9 | 0.141 | 0.229 | |
| ACROM extension (°) | 47.6 ± 13.6 | 50.0 ± 12.3 | 45.1 ± 11.2 | 0.079 | 0.376 | |
| ACROM flexion (°) | 57.8 ± 13.9 | 53.5 ± 13.0 | 56.0 ± 10.4 | 0.034 | 0.568 | |
| Pain (a.u.) | 4.3 ± 3.5 | 3.8 ± 3.3 | 4.6 ± 3.7 | 0.364 | 0.058 |
| Parameter | T0 | T1 | T2 | p Value | ||
|---|---|---|---|---|---|---|
| Study Group (SG) | ACROM right rotation (°) | 66.5 ± 15.2 | 69.0 ± 13.6 | 73.7 ± 14.9 | 0.523 | 0.028 |
| ACROM left rotation (°) | 65.1 ± 6.7 | 69.9 ± 18.8 | 76.3 ± 18.0 | 0.451 | 0.047 | |
| ACROM right lateral inclination (°) | 38.1 ± 9.5 | 39.4 ± 9.3 | 41.4 ± 6.3 | 0.256 | 0.165 | |
| ACROM left lateral inclination (°) | 41.6 ± 8.0 | 45.1 ± 16.7 | 45.3 ± 10.8 | 0.355 | 0.091 | |
| ACROM extension (°) | 46.2 ± 13.0 | 43.8 ± 16.8 | 55.1 ± 16.3 § | 0.466 | 0.043 | |
| ACROM flexion (°) | 53.2± 12.2 | 59.5 ± 16.9 | 62.2 ± 16.2 | 0.484 | 0.037 | |
| Pain (A.U.) | 7.3 ± 0.7 | 4.8 ± 1.4 * | 1.1 ± 1.5 #§ | 0.965 | 0.000 | |
| Control Group (CG) | ACROM right rotation (°) | 60.4 ± 10.4 | 63.1 ± 12.0 | 61.1 ± 10.9 | 0.072 | 0.453 |
| ACROM left rotation (°) | 58.7 ± 7.2 | 58.7 ± 10.0 | 57.7 ± 8.4 | 0.078 | 0.434 | |
| ACROM right lateral inclination (°) | 33.4 ± 6.2 | 33.3 ± 7.1 | 32.3 ± 4.9 | 0.129 | 0.308 | |
| ACROM left lateral inclination (°) | 35.5 ± 6.9 | 33.9 ± 5.9 | 33.2 ± 6.0 | 0.318 | 0.090 | |
| ACROM extension (°) | 54.8 ± 7.5 | 56.3 ± 7.7 | 54.4 ± 8.3 | 0.011 | 0.770 | |
| ACROM flexion (°) | 55.0 ± 17.3 | 53.3 ± 16.3 | 51.9 ± 15.0 | 0.185 | 0.215 | |
| Pain (a.u.) | 4.0 ± 3.9 | 4.1 ± 3.9 | 3.9 ± 3.5 | 0.053 | 0.594 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Russo, L.; Panessa, T.; Bartolucci, P.; Raggi, A.; Migliaccio, G.M.; Larion, A.; Padulo, J. Elastic Taping Application on the Neck: Immediate and Short-Term Impacts on Pain and Mobility of Cervical Spine. J. Funct. Morphol. Kinesiol. 2023, 8, 156. https://doi.org/10.3390/jfmk8040156
Russo L, Panessa T, Bartolucci P, Raggi A, Migliaccio GM, Larion A, Padulo J. Elastic Taping Application on the Neck: Immediate and Short-Term Impacts on Pain and Mobility of Cervical Spine. Journal of Functional Morphology and Kinesiology. 2023; 8(4):156. https://doi.org/10.3390/jfmk8040156
Chicago/Turabian StyleRusso, Luca, Tommaso Panessa, Paolo Bartolucci, Andrea Raggi, Gian Mario Migliaccio, Alin Larion, and Johnny Padulo. 2023. "Elastic Taping Application on the Neck: Immediate and Short-Term Impacts on Pain and Mobility of Cervical Spine" Journal of Functional Morphology and Kinesiology 8, no. 4: 156. https://doi.org/10.3390/jfmk8040156
APA StyleRusso, L., Panessa, T., Bartolucci, P., Raggi, A., Migliaccio, G. M., Larion, A., & Padulo, J. (2023). Elastic Taping Application on the Neck: Immediate and Short-Term Impacts on Pain and Mobility of Cervical Spine. Journal of Functional Morphology and Kinesiology, 8(4), 156. https://doi.org/10.3390/jfmk8040156