
Fiber-Type-Specific Hypertrophy with the Use of Low-Load Blood Flow Restriction Resistance Training: A Systematic Review


 , ,
, ,
Abstract
1. Introduction
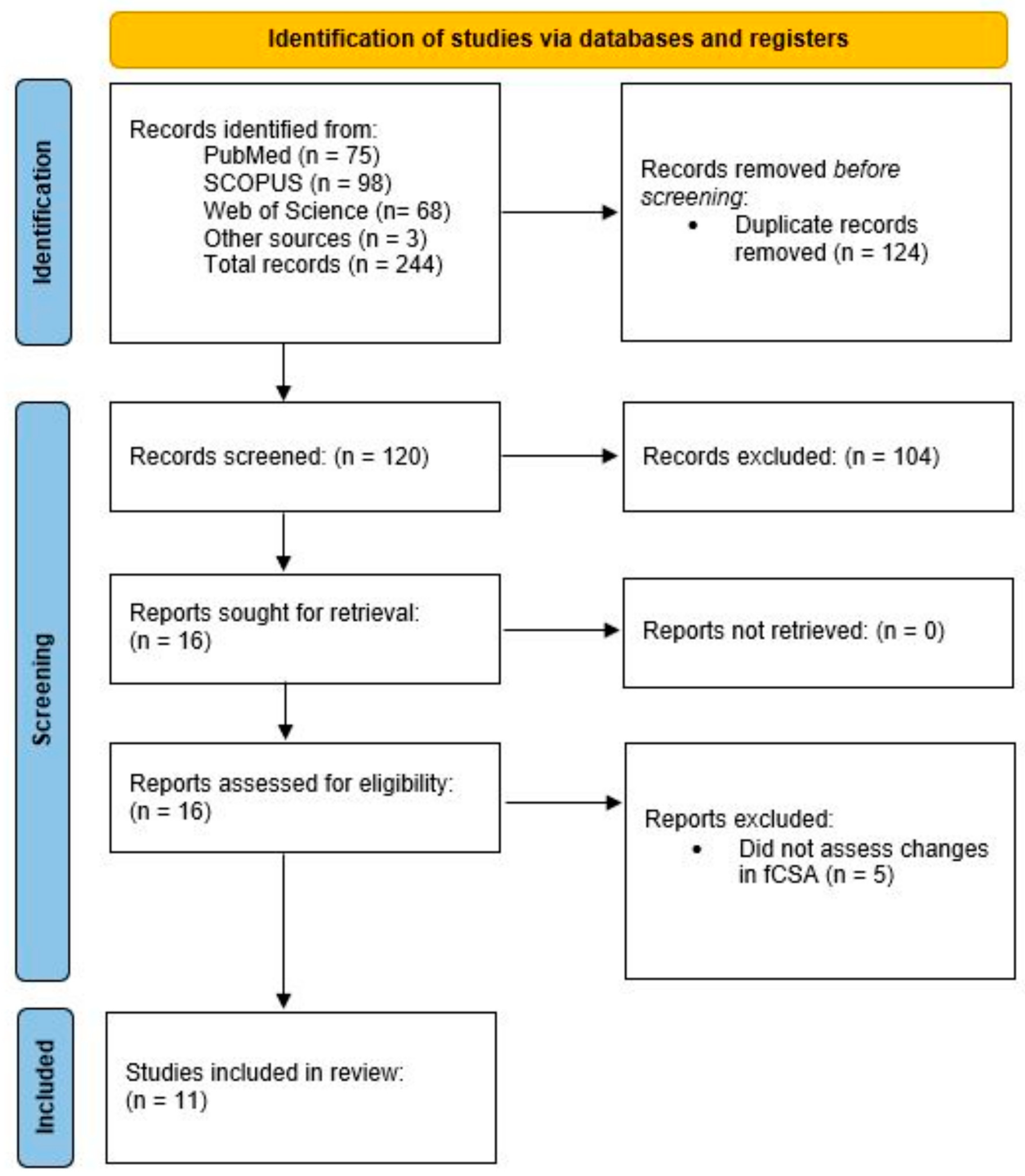
2. Methods
2.1. Literature Search
2.2. Inclusion/Exclusion Criteria
2.3. Data Coding and Analysis
2.4. Methodological Quality
3. Results and Discussion
3.1. Descriptive Data
3.2. Longitudinal Data
3.3. Methodological Quality
3.4. Reconciling Current Data
3.5. Limitations and Future Directions
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fry, A.C. The role of resistance exercise intensity on muscle fibre adaptations. Sport. Med. 2004, 34, 663–679. [Google Scholar] [CrossRef] [PubMed]
- Ogborn, D.; Schoenfeld, B.J. The role of fber types in muscle hypertrophy: Implications for loading strategies. Strength Cond. J. 2014, 36, 20–25. [Google Scholar] [CrossRef]
- Henneman, E.; Somjen, G.; Carpenter, D.O. Functional Significance of Cell Size in Spinal Motoneurons. J. Neurophysiol. 1965, 28, 560–580. [Google Scholar] [CrossRef]
- Chalmers, G.R. Can fast-twitch muscle fibres be selectively recruited during lengthening contractions? Review and applications to sport movements. Sport. Biomech. 2008, 7, 137–157. [Google Scholar] [CrossRef] [PubMed]
- Fleck, S.J.; Kraemer, W.J. Designing Resistance Training Programs, 3rd ed.; Human Kinetics Publishing: Champaign, IL, USA, 2004. [Google Scholar]
- Muddle, T.W.D.; Colquhoun, R.J.; Magrini, M.A.; Luera, M.J.; DeFreitas, J.M.; Jenkins, N.D.M. Effects of fatiguing, submaximal high- versus low-torque isometric exercise on motor unit recruitment and firing behavior. Physiol. Rep. 2018, 6, e13675. [Google Scholar] [CrossRef]
- Martineau, L.C.; Gardiner, P.F. Skeletal muscle is sensitive to the tension-time integral but not to the rate of change of tension, as assessed by mechanically induced signaling. J. Biomech. 2002, 35, 657–663. [Google Scholar] [CrossRef] [PubMed]
- Gundermann, D. Mechanisms of Blood Flow Restriction Exercise in Skeletal Muscle Adaptations. Ph.D. Thesis, University of Texas Medical Branch, Galveston, TX, USA, 2016. [Google Scholar]
- Grgic, J.; Schoenfeld, B.J. Are the Hypertrophic Adaptations to High and Low-Load Resistance Training Muscle Fiber Type Specific? Front. Physiol. 2018, 9, 402. [Google Scholar] [CrossRef]
- Grgic, J. The Effects of Low-Load vs. High-Load Resistance Training on Muscle Fiber Hypertrophy: A Meta-Analysis. J. Hum. Kinet. 2020, 74, 51–58. [Google Scholar] [CrossRef]
- Lixandrao, M.E.; Ugrinowitsch, C.; Berton, R.; Vechin, F.C.; Conceicao, M.S.; Damas, F.; Libardi, C.A.; Roschel, H. Magnitude of Muscle Strength and Mass Adaptations Between High-Load Resistance Training Versus Low-Load Resistance Training Associated with Blood-Flow Restriction: A Systematic Review and Meta-Analysis. Sport. Med. 2018, 48, 361–378. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Morris, B. Estimating effect sizes from pretest-posttest-control group designs. Organ. Res. Methods 2008, 11, 364–386. [Google Scholar] [CrossRef]
- Higgins, J.; Thomas, J. Obtaining Standard Deviations from Standard Errors and Confidence Intervals. Cochrane Handbook for Systematic Reviews of Interventions: Version 6.3. 2022. Available online: https://handbook-5-1.cochrane.org/chapter_7/7_7_3_2_obtaining_standard_deviations_from_standard_errors_and.htm (accessed on 10 January 2023).
- Coleman, M.; Harrison, K.; Arias, R.; Johnson, E.; Grgic, J.; Orazem, J.; Schoenfeld, B. Muscular Adaptations in Drop Set vs. Traditional Training: A meta-analysis. Int. J. Strength Cond. 2022, 28, 1. [Google Scholar] [CrossRef]
- Downs, S.H.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Grgic, J.; Schoenfeld, B.J.; Davies, T.B.; Lazinica, B.; Krieger, J.W.; Pedisic, Z. Effect of Resistance Training Frequency on Gains in Muscular Strength: A Systematic Review and Meta-Analysis. Sport. Med. 2018, 48, 1207–1220. [Google Scholar] [CrossRef]
- Grgic, J.; Schoenfeld, B.J.; Skrepnik, M.; Davies, T.B.; Mikulic, P. Effects of Rest Interval Duration in Resistance Training on Measures of Muscular Strength: A Systematic Review. Sport. Med. 2018, 48, 137–151. [Google Scholar] [CrossRef] [PubMed]
- Grgic, J.; Garofolini, A.; Orazem, J.; Sabol, F.; Schoenfeld, B.J.; Pedisic, Z. Effects of Resistance Training on Muscle Size and Strength in Very Elderly Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Sport. Med. 2020, 50, 1983–1999. [Google Scholar] [CrossRef]
- Yasuda, T.; Abe, T.; Sato, Y.; Midorikawa, T.; Kearns, C.F.; Inoue, K.; Ishii, R.N. Muscle fiber cross-sectional area is increased after two weeks of twice daily KAATSU-resistance training. Int. J. KAATSU Train. Res. 2005, 1, 65–70. [Google Scholar] [CrossRef]
- Sieljacks, P.; Wang, J.; Groennebaek, T.; Rindom, E.; Jakobsgaard, J.E.; Herskind, J.; Gravholt, A.; Moller, A.B.; Musci, R.V.; de Paoli, F. Six Weeks of Low-Load Blood Flow Restricted and High-Load Resistance Exercise Training Produce Similar Increases in Cumulative Myofibrillar Protein Synthesis and Ribosomal Biogenesis in Healthy Males. Front. Physiol. 2019, 10, 649. [Google Scholar] [CrossRef]
- Nielsen, J.L.; Aagaard, P.; Bech, R.D.; Nygaard, T.; Hvid, L.G.; Wernbom, M.; Suetta, C.; Frandsen, U. Proliferation of myogenic stem cells in human skeletal muscle in response to low-load resistance training with blood flow restriction. J. Physiol. 2012, 590, 4351–4361. [Google Scholar] [CrossRef]
- Hansen, S.K.; Ratzer, J.; Nielsen, J.L.; Suetta, C.; Karlsen, A.; Kvorning, T.; Frandsen, U.; Aagaard, P. Effects of alternating blood flow restricted training and heavy-load resistance training on myofiber morphology and mechanical muscle function. J. Appl. Physiol. 2020, 128, 1523–1532. [Google Scholar] [CrossRef]
- Davids, C.J.; Næss, T.C.; Moen, M.; Cumming, K.T.; Horwath, O.; Psilander, N.; Ekblom, B.; Coombes, J.S.; Peake, J.; Raastad, T.; et al. Acute cellular and molecular responses and chronic adaptations to low-load blood flow restriction and high-load resistance exercise in trained individuals. J. Appl. Physiol. 2021, 131, 1731–1749. [Google Scholar] [CrossRef] [PubMed]
- Bjornsen, T.; Wernbom, M.; Kirketeig, A.; Paulsen, G.; Samnoy, L.; Baekken, L.; Cameron-Smith, D.; Bernsten, S.; Raastad, T. Type 1 Muscle Fiber Hypertrophy after Blood Flow-restricted Training in Powerlifters. Med. Sci. Sport. Exerc. 2019, 51, 288–298. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Mogensen, A.G.; Thybo, F.; Brandbyge, M.; Jensen, J.B.; van Hall, G.; Agergaard, J.; de Paoli, F.V.; Miller, B.F.; Botker, H.E.; et al. Low-load blood flow-restricted resistance exercise produce fiber type-independent hypertrophy and improves muscle functional capacity in older individuals. J. Appl. Physiol. 2023, 134, 1047–1062. [Google Scholar] [CrossRef] [PubMed]
- Jakobsgaard, J.E.; Christiansen, M.; Sieljacks, P.; Wang, J.; Groennebaek, T.; de Paoli, F.; Vissing, K. Impact of blood flow-restricted bodyweight exercise on skeletal muscle adaptations. Clin. Physiol. Funct. Imaging 2018, 38, 965–975. [Google Scholar] [CrossRef]
- Bjornsen, T.; Wernbom, M.; Lovstad, A.; Paulsen, G.; D’Souza, R.F.; Cameron-Smith, D.; Flesche, A.; Hisdal, J.; Bernsten, S.; Raastad, T. Delayed myonuclear addition, myofiber hypertrophy, and increases in strength with high-frequency low-load blood flow restricted training to volitional failure. J. Appl. Physiol. 2019, 126, 578–592. [Google Scholar] [CrossRef]
- Pignanelli, C.; Petrick, H.L.; Keyvani, F.; Heigenhauser, G.J.F.; Quadrilatero, J.; Holloway, G.P.; Burr, J.F. Low-load resistance training to task failure with and without blood flow restriction: Muscular functional and structural adaptations. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2020, 318, R284–R295. [Google Scholar] [CrossRef]
- Bjørnsen, T.; Wernbom, M.; Paulsen, G.; Berntsen, S.; Brankovic, R.; Stålesen, H.; Sundens, J.; Raastad, T. Frequent blood flow restricted training not to failure and to failure induces similar gains in myonuclei and muscle mass. Scand. J. Med. Sci. Sport. 2021, 31, 1420–1439. [Google Scholar] [CrossRef]
- Bürkner, P. brms: An R package for Bayesian multilevel models using Stan. J. Stat. Softw. 2017, 80, 1–28. [Google Scholar] [CrossRef]
- Wernbom, M.; Aagaard, P. Muscle fibre activation and fatigue with low-load blood flow restricted resistance exercise-An integrative physiology review. Acta Physiol. 2020, 228, e13302. [Google Scholar] [CrossRef]
- Noble, E.G.; Milne, K.J.; Melling, C.W.J. Heat shock proteins and exercise: A primer. Appl. Physiol. Nutr. Metab. 2008, 33, 1050–1065. [Google Scholar] [CrossRef]
- Cumming, K.T.; Paulsen, G.; Wernbom, M.; Ugelstad, I.; Raastad, T. Acute response and subcellular movement of HSP27, αB-crystallin and HSP70 in human skeletal muscle after blood-flow-restricted low-load resistance exercise. Acta Physiol. 2014, 211, 634–646. [Google Scholar] [CrossRef] [PubMed]
- Bjørnsen, T.; Wernbom, M.; Paulsen, G.; Markworth, J.F.; Berntsen, S.; D’Souza, R.F.; Cameron-Smith, D.; Raastad, T. High-frequency blood flow-restricted resistance exercise results in acute and prolonged cellular stress more pronounced in type I than in type II fibers. J. Appl. Physiol. 2021, 131, 643–660. [Google Scholar] [CrossRef] [PubMed]
- Horwath, O.; Envall, H.; Röja, J.; Emanuelsson, E.B.; Sanz, G.; Ekblom, B.; Apro, W.; Moberg, M. Variability in vastus lateralis fiber type distribution, fiber size, and myonuclear content along and between the legs. J. Appl. Physiol. 2021, 131, 158–173. [Google Scholar] [CrossRef] [PubMed]
- Leeuwenburgh, C. Role of apoptosis in sarcopenia. J. Gerontol. A Biol. Sci. Med. Sci. 2003, 58, 999–1001. [Google Scholar] [CrossRef]
- Kraková, D.; Holwerda, A.M.; Betz, M.W.; Lavin, K.M.; Bamman, M.M.; van Loon, L.J.C.; Verdijk, L.B.; Snijders, T. Muscle fiber type grouping does not change in response to prolonged resistance exercise training in healthy older men. Exp. Gerontol. 2023, 173, 112083. [Google Scholar] [CrossRef]


{kind=link}
| Study | Sample | Design | Duration | Findings |
|---|---|---|---|---|
| Bjørnsen, Wernbom, Kirketeig et al. [25] | 17 nationally ranked powerlifters | Parallel design. Participants randomly assigned to either an HL group who performed front squats at 60–85% 1RM or an LL-BFR group who integrated 2 blocks (weeks 1 and 3) of 5 LL-BFR (~30% 1RM at a pressure of 120 mmHg) front squat sessions into the traditional training. Traditional training consisted of 6–7 sets per session whereas LL-BFR training consisted of 4 sets (first and last set to voluntary failure) with 30 s rest intervals; both groups trained 5 days/week. | 6.5 weeks | LL-BFR elicited a greater increase in type I fCSA compared to HL training (12% (ES: 0.80) vs. 0% (ES: 0.00), respectively); type II fCSA remained relatively unchanged over the study period. |
| Bjørnsen, Wernbom, Løvstad et al. [28] | 13 young, untrained men and women | One group, pre-/post-test design. Participants performed two 5-day blocks of 7 LL-BFR (20% 1RM at a pressure of 90–100 mmHg) sessions, separated by a 10-day rest period. Exercise consisted of 4 sets of unilateral knee extensions to volitional failure with 30 s rest intervals. | 3 weeks | Type I and type II fCSA decreased after the first training block (−6% and −15%, respectively). Alternatively, type I fCSA increased to a greater extent than type II fCSA after the second training block (19% (ES: 0.64) vs. 11% (ES: 0.51), respectively). |
| Bjørnsen, Wernbom, Paulsen, Berntsen et al. [30] | 17 young, untrained men | Within-subject design. Participants had their legs randomized to perform two 5-day blocks of 7 LL-BFR (20% 1RM sessions at a pressure of 90–100 mmHg), separated by a 10-day rest period, either to volitional failure or not to failure (30-15-15-15 repetitions). Exercise consisted of 4 sets of unilateral knee extensions with 30 s rest intervals. | 3 weeks | Type I fCSA decreased by 10.3% (ES: 0.70) after 10-days post-training in the failure leg while no appreciable change was observed in the nonfailure leg. Type II fCSA did not appreciably change from baseline in either condition. |
| Davids et al. [24] | 21 young, trained men and women | Parallel group design. Random assignment to either HL training (8 repetitions at 10 RM) or LL-BFR (~30% to 50% 1RM at 60% arterial occlusion pressure). Exercise consisted of combinations of the barbell back squat, leg press, Bulgarian split squat, and leg extension. Both groups performed 4 sets of 2–3 exercises 3 days/week. Intensity of effort was standardized so that both conditions trained within 1-4 repetitions from failure. | 9 weeks | Type I fCSA increased to a greater extent in LL-BFR compared to HL (10.6% (ES: 0.32) vs. 1.7% (ES: 0.07), respectively); type II hypertrophy favored HL vs. LL-BFR (17.7% (ES: 0.53) vs. 12.6% (ES: 0.36), respectively). |
| Hansen et al. [23] | 18 young men and women | Parallel group design. Random assignment to perform either HL training (70–90% 1RM) or an LL-BFR group who alternated weekly between LL-BFR (20% 1RM at a pressure of 110 mmHg) and HL Exercise consisted of the leg press and leg extension carried out 4 days/week; HL performed 2–4 sets per exercise of 3–10 repetitions with 2 min rest intervals whereas LL-BFR performed 4 sets to volitional failure with 30 s rest intervals | 6 weeks | Type I fCSA increased to a greater extent in the HL group compared to LL-BFR (12% (ES: 0.81) vs. 2.5% (ES: 0.17), respectively); type II fCSA increased similarly between groups (~16%). |
| Jakobsgaard et al. [27] | 6 healthy young untrained men and women | One group, pre-/post-test design. Subjects performed 5 sets of sit-to-stand LL-BFR (pressure of 100–180 mmHg) to volitional failure with 30 s rest intervals carried out 3 days/week. | 6 weeks | Type I fCSA increased to a greater extent than type II fCSA (8.7% (ES: 0.76) vs. 0% (ES: 0.06), respectively). |
| Nielsen et al. [22] | 18 young untrained men | Parallel group design. Participants assigned to LL training (20% 1RM) either using BFR (at a pressure of 100 mmHg) or performing exercise without occlusion. Training consisted of 4 sets of knee extension exercise carried out once or twice daily for a total of 23 sessions performed within 19 days). LL-BFR carried out sets to volitional failure, whereas LL carried out sets in a work-matched fashion. | 3 weeks | For LL-BFR, type I and type II fCSA increased similarly from baseline to 3 days post-study (35% (ES: 1.87) and 37% (ES: 1.99), respectively). Alternatively, type I and type II fCSA did not appreciably change from pre–post study in LL. |
| Pignanelli et al. [29] | 10 young, untrained men | Within-subject design. Participants had their legs randomly assigned to LL training (30% 1RM) either using BFR (at 60–70% of the lowest effective occlusive pressure) or performing exercise without occlusion. Training consisted of 4 sets of single leg squats to volitional failure with 100 s rest intervals carried out 3 days/week. | 6 weeks | Type I fCSA increased to a greater extent in LL compared to LL-BFR (15.8% (ES: 0.56) vs. 10.1% (ES: 0.38), respectively); type II fCSA increased similarly between conditions (~9% (~ES: 0.30)). |
| Sieljacks et al. [21] | 34 young, untrained men and women | Parallel group design. Random assignment to either HL training (70% 1RM) or LL-BFR (~30%/1RM at a pressure of 97 mmHg) training carried out to volitional failure. Training consisted of 4 sets of knee extension exercise carried out 3 days/week. HL performed 12 repetitions with 3 min rest intervals whereas LL-BFR performed sets to volitional failure with 30 s rest intervals | 6 weeks | Minimal pre–post study changes were observed in LL-BFR and HL conditions for both type I fCSA (−2.4% (ES: −0.20) and −2.3% (ES: −0.11), respectively) and type II fCSA (2.6% (ES: 0.15) and −2.3% (ES: −0.11), respectively). |
| Wang et al. [26] | 23 older, untrained men and women | Parallel group design. Random assignment to either LL-BFR (~30%/1RM at a pressure of 97 mmHg) training carried out to volitional failure or a nontraining control. LL-BFR training consisted of 4 sets of knee extension exercise with 30 s rest intervals carried out 3 days/week. | 6 weeks | Type I and type II fCSA increased to a similar extent (18.1% (ES: 0.62) vs. 22.2% (ES: 0.53), respectively). |
| Yasuda et al. [20] | 5 young men | Parallel group design. Participants performed either LL-BFR (20% 1RM at a pressure of 160–240 mmHg) training or LL training without occlusion. Exercise consisted of 3 sets of 15 repetitions of the squat and leg curl with 30 s rest intervals carried out twice daily for the duration of the study period. | 2 weeks | For LL-BFR, type II fCSA increased to a greater extent than type I fCSA (27.6% (ES: 0.77) vs. 5.9% (ES: 0.16), respectively). Type I and type II fCSA showed minimal pre–post study changes in LL (−2.1% (ES: −0.11) and 0.5% (ES: 0.7), respectively). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schoenfeld, B.J.; Ogborn, D.; Piñero, A.; Burke, R.; Coleman, M.; Rolnick, N. Fiber-Type-Specific Hypertrophy with the Use of Low-Load Blood Flow Restriction Resistance Training: A Systematic Review. J. Funct. Morphol. Kinesiol. 2023, 8, 51. https://doi.org/10.3390/jfmk8020051
Schoenfeld BJ, Ogborn D, Piñero A, Burke R, Coleman M, Rolnick N. Fiber-Type-Specific Hypertrophy with the Use of Low-Load Blood Flow Restriction Resistance Training: A Systematic Review. Journal of Functional Morphology and Kinesiology. 2023; 8(2):51. https://doi.org/10.3390/jfmk8020051
Chicago/Turabian StyleSchoenfeld, Brad J., Dan Ogborn, Alec Piñero, Ryan Burke, Max Coleman, and Nicholas Rolnick. 2023. "Fiber-Type-Specific Hypertrophy with the Use of Low-Load Blood Flow Restriction Resistance Training: A Systematic Review" Journal of Functional Morphology and Kinesiology 8, no. 2: 51. https://doi.org/10.3390/jfmk8020051
APA StyleSchoenfeld, B. J., Ogborn, D., Piñero, A., Burke, R., Coleman, M., & Rolnick, N. (2023). Fiber-Type-Specific Hypertrophy with the Use of Low-Load Blood Flow Restriction Resistance Training: A Systematic Review. Journal of Functional Morphology and Kinesiology, 8(2), 51. https://doi.org/10.3390/jfmk8020051