
Full Recovery from O’Donoghue’s Triad with Autologous Bone Marrow Aspirate Matrix: A Case Report


 ,
,
Abstract
1. Introduction
2. Patient Information
3. Clinical Findings
4. Timeline
| Date | Event |
| 20 July 2020 | Injury |
| 28 July 2020 | First BMA Matrix Injection |
| 26 August 2020 | Second BMA Matrix Injection |
| 25 September 2020 | Third BMA Matrix Injection |
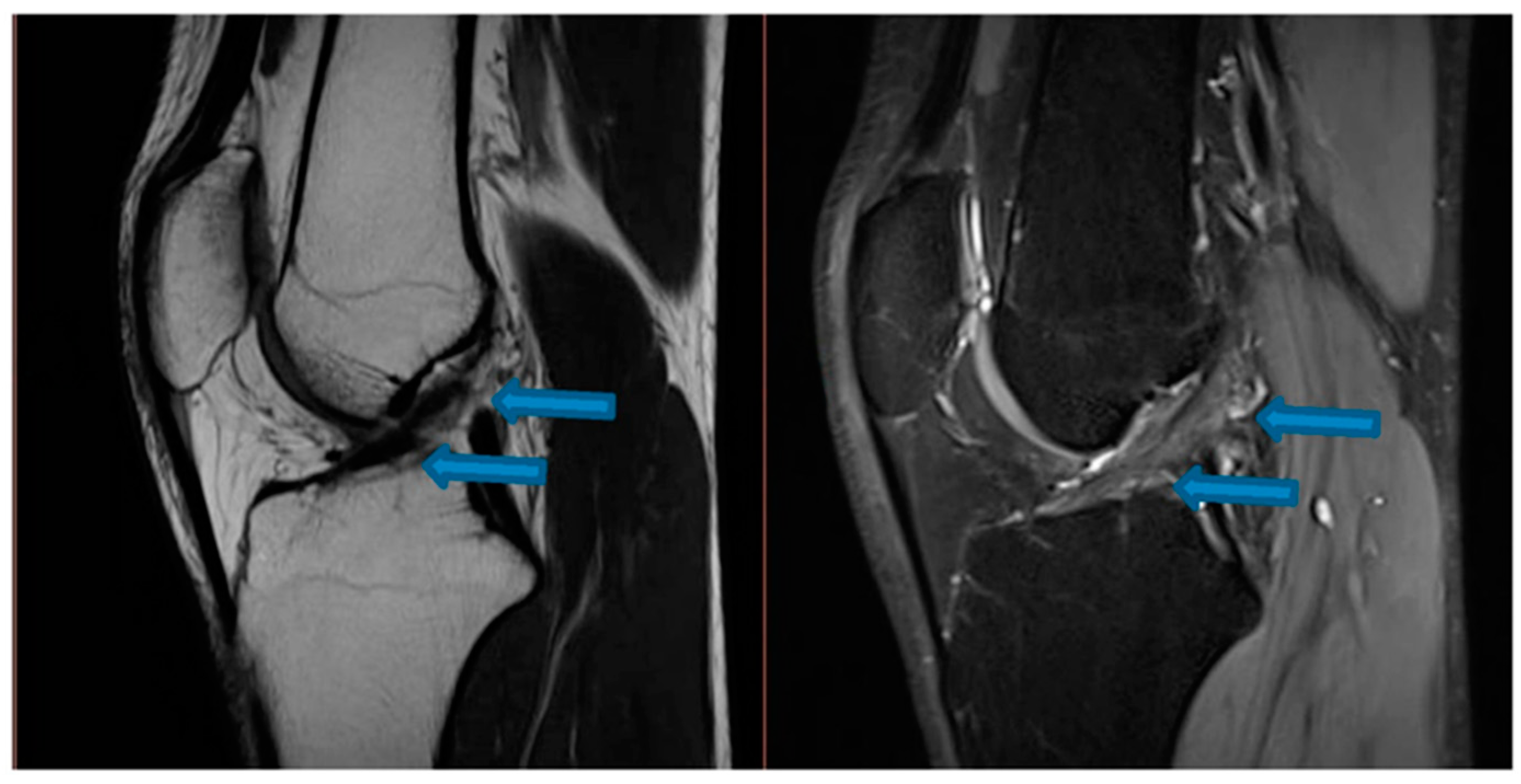
| 9 November 2020 | MRI scans demonstrating signs of partial ACL healing |
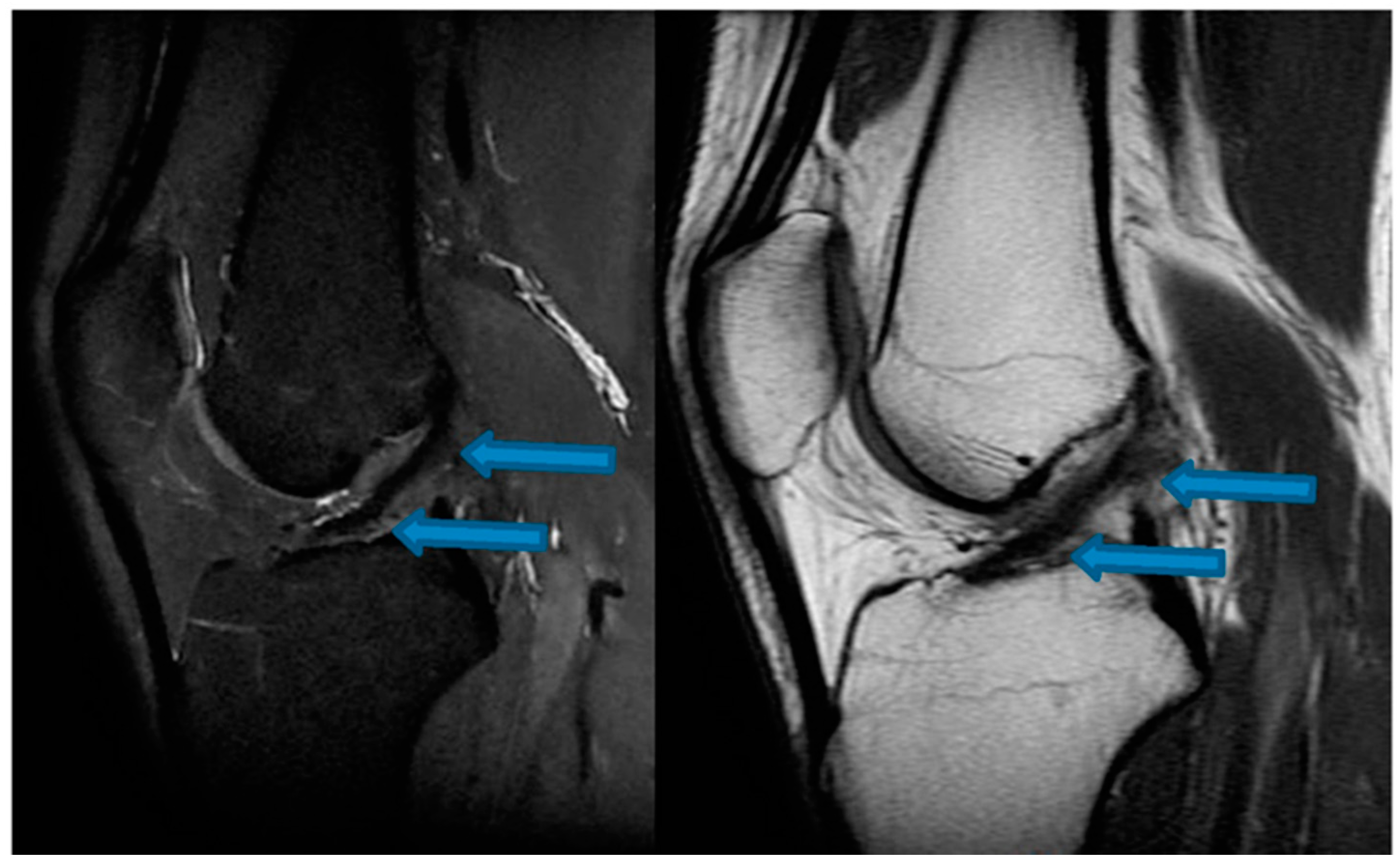
| 14 August 2021 | MRI scans demonstrating signs of complete ACL healing |
| 24 December 2021 | MRI scans confirming signs of complete ACL, MCL and medial meniscus healing |
5. Diagnostic Assessment
6. Therapeutic Intervention
7. Follow-Up and Outcomes
8. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hewett, T.E.; Myer, G.D.; Ford, K.R.; Paterno, M.V.; Quatman, C.E. Mechanisms, Prediction, and Prevention of ACL Injuries: Cut Risk with Three Sharpened and Validated Tools: ACL INJURY PREVENTION. J. Orthop. Res. 2016, 34, 1843–1855. [Google Scholar] [CrossRef] [PubMed]
- Hassebrock, J.D.; Gulbrandsen, M.T.; Asprey, W.L.; Makovicka, J.L.; Chhabra, A. Knee Ligament Anatomy and Biomechanics. Sport. Med. Arthrosc. Rev. 2020, 28, 80–86. [Google Scholar] [CrossRef] [PubMed]
- de Sire, A.; Demeco, A.; Marotta, N.; Moggio, L.; Palumbo, A.; Iona, T.; Ammendolia, A. Anterior Cruciate Ligament Injury Prevention Exercises: Could a Neuromuscular Warm-Up Improve Muscle Pre-Activation before a Soccer Game? A Proof-of-Principle Study on Professional Football Players. Appl. Sci. 2021, 11, 4958. [Google Scholar] [CrossRef]
- Smith, B.A.; Livesay, G.A.; Woo, S.L. Biology and Biomechanics of the Anterior Cruciate Ligament. Clin. Sport. Med. 1993, 12, 637–670. [Google Scholar] [CrossRef]
- Thomas, A.C.; Villwock, M.; Wojtys, E.M.; Palmieri-Smith, R.M. Lower Extremity Muscle Strength After Anterior Cruciate Ligament Injury and Reconstruction. J. Athl. Train. 2013, 48, 610–620. [Google Scholar] [CrossRef]
- Hasegawa, T.; Otani, T.; Takeda, K.; Matsumoto, H.; Harato, K.; Toyama, Y.; Nagura, T. Anterior Cruciate Ligament Reconstruction Does Not Fully Restore Normal 3D Knee Kinematics at 12 Months During Walking and Walk-Pivoting: A Longitudinal Gait Analysis Study. J. Appl. Biomech. 2015, 31, 330–339. [Google Scholar] [CrossRef]
- Lohmander, L.S.; Ionescu, M.; Jugessur, H.; Poole, A.R. Changes in Joint Cartilage Aggrecan after Knee Injury and in Osteoarthritis. Arthritis Rheum. 1999, 42, 534–544. [Google Scholar] [CrossRef]
- Nelson, F.; Billinghurst, R.C.; Pidoux, I.; Reiner, A.; Langworthy, M.; McDermott, M.; Malogne, T.; Sitler, D.F.; Kilambi, N.R.; Lenczner, E.; et al. Early Post-Traumatic Osteoarthritis-like Changes in Human Articular Cartilage Following Rupture of the Anterior Cruciate Ligament. Osteoarthr. Cartil. 2006, 14, 114–119. [Google Scholar] [CrossRef]
- Santos Duarte Lana, J.F.; Furtado da Fonseca, L.; Mosaner, T.; Tieppo, C.E.; Marques Azzini, G.O.; Ribeiro, L.L.; Setti, T.; Purita, J. Bone Marrow Aspirate Clot: A Feasible Orthobiologic. J. Clin. Orthop. Trauma 2020. [CrossRef]
- Lana, J.F.; da Fonseca, L.F.; Azzini, G.; Santos, G.; Braga, M.; Cardoso Junior, A.M.; Murrell, W.D.; Gobbi, A.; Purita, J.; de Andrade, M.A.P. Bone Marrow Aspirate Matrix: A Convenient Ally in Regenerative Medicine. Int. J. Mol. Sci. 2021, 22, 2762. [Google Scholar] [CrossRef]
- Dwek, J.R. The Periosteum: What Is It, Where Is It, and What Mimics It in Its Absence? Skelet. Radiol 2010, 39, 319–323. [Google Scholar] [CrossRef] [PubMed]
- Frey, S.P.; Jansen, H.; Doht, S.; Filgueira, L.; Zellweger, R. Immunohistochemical and Molecular Characterization of the Human Periosteum. Sci. World J. 2013, 2013, 341078. [Google Scholar] [CrossRef] [PubMed]
- LaBella, C.R.; Hennrikus, W.; Hewett, T.E. COUNCIL ON SPORTS MEDICINE AND FITNESS, and SECTION ON ORTHOPAEDICS Anterior Cruciate Ligament Injuries: Diagnosis, Treatment, and Prevention. PEDIATRICS 2014, 133, e1437–e1450. [Google Scholar] [CrossRef] [PubMed]
- Monk, A.P.; Davies, L.J.; Hopewell, S.; Harris, K.; Beard, D.J.; Price, A.J. Surgical versus Conservative Interventions for Treating Anterior Cruciate Ligament Injuries. Cochrane Database Syst. Rev. 2016. [CrossRef]
- Themistocleous, G.S.; Chloros, G.D.; Kyrantzoulis, I.M.; Georgokostas, I.A.; Themistocleous, M.S.; Papagelopoulos, P.J.; Savvidou, O.D. Effectiveness of a Single Intra-Articular Bone Marrow Aspirate Concentrate (BMAC) Injection in Patients with Grade 3 and 4 Knee Osteoarthritis. Heliyon 2018, 4, e00871. [Google Scholar] [CrossRef]
- Imam, M.A.; Mahmoud, S.S.S.; Holton, J.; Abouelmaati, D.; Elsherbini, Y.; Snow, M. A Systematic Review of the Concept and Clinical Applications of Bone Marrow Aspirate Concentrate in Orthopaedics. Sicot-J 2017, 3, 17. [Google Scholar] [CrossRef]
- Lana, J.F.S.D.; da Fonseca, L.F.; Macedo, R.D.R.; Mosaner, T.; Murrell, W.; Kumar, A.; Purita, J.; de sAndrade, M.A.P. Platelet-Rich Plasma vs Bone Marrow Aspirate Concentrate: An Overview of Mechanisms of Action and Orthobiologic Synergistic Effects. World J. Stem Cells 2021. [CrossRef]
- Centeno, C.; Lucas, M.; Stemper, I.; Dodson, E. Image Guided Injection of Anterior Cruciate Ligament Tears with Autologous Bone Marrow Concentrate and Platelets: Midterm Analysis from A Randomized Controlled Trial. Biol. Orthop. J. 2022, 3, e7–e20. [Google Scholar] [CrossRef]
- Oe, K.; Kushida, T.; Okamoto, N.; Umeda, M.; Nakamura, T.; Ikehara, S.; Iida, H. New Strategies for Anterior Cruciate Ligament Partial Rupture Using Bone Marrow Transplantation in Rats. Stem Cells Dev. 2011, 20, 671–679. [Google Scholar] [CrossRef]
- Le Blanc, K.; Ringdén, O. Mesenchymal Stem Cells: Properties and Role in Clinical Bone Marrow Transplantation. Curr. Opin. Immunol. 2006, 18, 586–591. [Google Scholar] [CrossRef]
- Kuroda, R.; Kurosaka, M.; Yoshiya, S.; Mizuno, K. Localization of Growth Factors in the Reconstructed Anterior Cruciate Ligament: Immunohistological Study in Dogs. Knee Surg. Sport. Traumatol. Arthrosc. 2000, 8, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Mengsteab, P.Y.; Otsuka, T.; McClinton, A.; Shemshaki, N.S.; Shah, S.; Kan, H.-M.; Obopilwe, E.; Vella, A.T.; Nair, L.S.; Laurencin, C.T. Mechanically Superior Matrices Promote Osteointegration and Regeneration of Anterior Cruciate Ligament Tissue in Rabbits. Proc. Natl. Acad. Sci. USA 2020, 117, 28655–28666. [Google Scholar] [CrossRef] [PubMed]
- Holton, J.; Imam, M.; Ward, J.; Snow, M. The Basic Science of Bone Marrow Aspirate Concentrate in Chondral Injuries. Orthop. Rev. 2016. [CrossRef]
- Allouche, M.; Bikfalvi, A. The Role of Fibroblast Growth Factor-2 (FGF-2) in Hematopoiesis. Prog. Growth Factor Res. 1995, 6, 35–48. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Date | IKDC Questionnaire Scores |
|---|---|
| 28 July 2020 | 21.8% |
| 20 December 2020 | 74.7% |
| 18 August 2021 | 96.6% |
| 24 December 2021 | 100% |
| Date | VAS Scale Scores |
|---|---|
| 28 July 2020 | 7 |
| 20 December 2020 | 2 |
| 18 August 2021 | 2 (with maximum knee flexion) |
| 24 December 2021 | 0 |
| Date | Injection |
|---|---|
| 28 July 2020 | 30 mL BMA (left posterior iliac crest) |
| 26 August 2020 | 30 mL BMA (right posterior iliac crest) |
| 25 September 2020 | 30 mL BMA (left posterior iliac crest) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lana, J.F.S.D.; Sugano, A.A.; De Barros, H.V.; Mosaner, T.; Santos, G.S.; Lana, J.V.B.; Vicente, R.; De Andrade, M.A.P. Full Recovery from O’Donoghue’s Triad with Autologous Bone Marrow Aspirate Matrix: A Case Report. J. Funct. Morphol. Kinesiol. 2022, 7, 100. https://doi.org/10.3390/jfmk7040100
Lana JFSD, Sugano AA, De Barros HV, Mosaner T, Santos GS, Lana JVB, Vicente R, De Andrade MAP. Full Recovery from O’Donoghue’s Triad with Autologous Bone Marrow Aspirate Matrix: A Case Report. Journal of Functional Morphology and Kinesiology. 2022; 7(4):100. https://doi.org/10.3390/jfmk7040100
Chicago/Turabian StyleLana, José Fábio Santos Duarte, André Atsushi Sugano, Henrique Valadão De Barros, Tomas Mosaner, Gabriel Silva Santos, João Vitor Bizinotto Lana, Rodrigo Vicente, and Marco Antônio Percope De Andrade. 2022. "Full Recovery from O’Donoghue’s Triad with Autologous Bone Marrow Aspirate Matrix: A Case Report" Journal of Functional Morphology and Kinesiology 7, no. 4: 100. https://doi.org/10.3390/jfmk7040100
APA StyleLana, J. F. S. D., Sugano, A. A., De Barros, H. V., Mosaner, T., Santos, G. S., Lana, J. V. B., Vicente, R., & De Andrade, M. A. P. (2022). Full Recovery from O’Donoghue’s Triad with Autologous Bone Marrow Aspirate Matrix: A Case Report. Journal of Functional Morphology and Kinesiology, 7(4), 100. https://doi.org/10.3390/jfmk7040100