
Analgesic Effect of Extracorporeal Shock-Wave Therapy in Individuals with Lateral Epicondylitis: A Randomized Controlled Trial

 , , and
, , and 
Abstract
1. Introduction
2. Methods
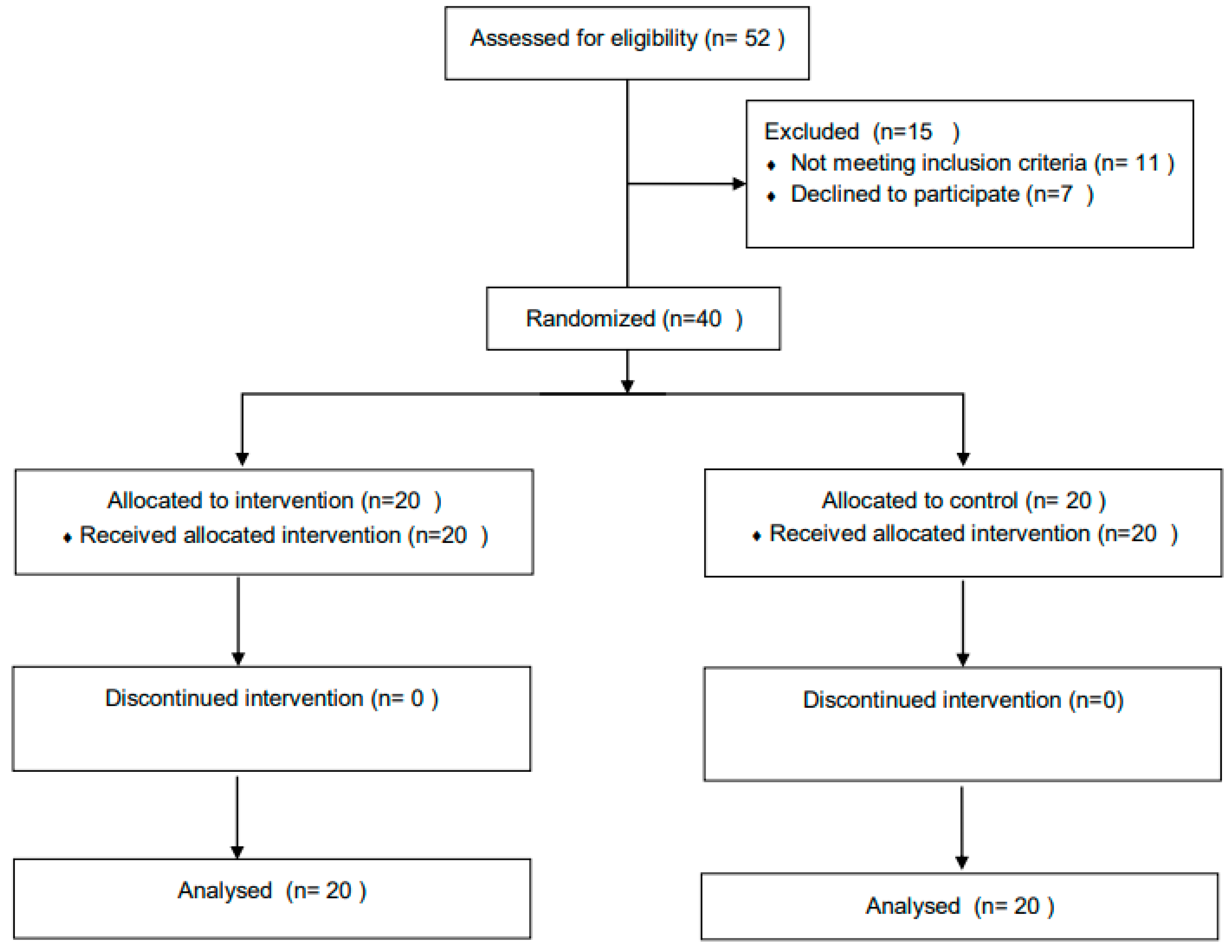
2.1. Participants
2.2. Intervention
2.3. Outcome Measures
2.3.1. Primary Outcome Measure
Pain Intensity
2.3.2. Secondary Outcome Measure
Upper-Extremity Function
Grip Strength
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Barrington, J.; Hage, W. Lateral Epicondylitis (Tennis Elbow). Curr. Opin. Orthop. 2003, 14, 291–295. [Google Scholar] [CrossRef]
- Ahmad, Z.; Siddiqui, N.; Malik, S.; Abdus-Samee, M.; Tytherleigh-Strong, G.; Rushton, N. Lateral Epicondylitis. Bone Jt. J. 2013, 95-B, 1158–1164. [Google Scholar] [CrossRef]
- Kraushaar, B.S.; Nirschl, R.P. Current Concepts Review—Tendinosis of the Elbow (Tennis Elbow). Clinical Features and Findings of Histological, Immunohistochemical, and Electron Microscopy Studies. J. Bone Jt. Surg. 1999, 81, 259–278. [Google Scholar] [CrossRef]
- Dorf, E.; Chhabra, A.; Golish, S.; McGinty, J.; Pannunzio, M. Effect of Elbow Position on Grip Strength in the Evaluation of Lateral Epicondylitis. J. Hand Surg. 2007, 32, 882–886. [Google Scholar] [CrossRef] [PubMed]
- Testa, G.; Vescio, A.; Perez, S.; Consoli, A.; Costarella, L.; Sessa, G.; Pavone, V. Extracorporeal Shockwave Therapy Treatment In Upper Limb Diseases: A Systematic Review. J. Clin. Med. 2020, 9, 453. [Google Scholar] [CrossRef] [PubMed]
- Ozkut, A.; Kilinçoğlu, V.; Ozkan, N.; Eren, A.; Ertaş, M. Extracorporeal Shock Wave Therapy in Patients with Lateral Epicondylitis. Acta Orthop. Traumatol. Turc. 2007, 41, 207–210. [Google Scholar] [PubMed]
- Rompe, J.; Hopf, C.; Küllmer, K.; Heine, J.; Bürger, R. Analgesic effect of extracorporeal shock-wave therapy on chronic tennis elbow. J. Bone Jt. Surg. Br. Vol. 1996, 78-B, 233–237. [Google Scholar] [CrossRef]
- Yang, T.; Huang, Y.; Lau, Y.; Wang, L. Efficacy Of Radial Extracorporeal Shock Wave Therapy on Lateral Epicondylosis, and Changes in the Common Extensor Tendon Stiffness with Pretherapy and Posttherapy in Real-Time Sonoelastography. Am. J. Phys. Med. Rehabil. 2017, 96, 93–100. [Google Scholar] [CrossRef]
- Devrimsel, G.; Kucukali Turkyilmaz, A.; Yildirim, M.; Ulasli, A. A Comparison of Laser and Extracorporeal Shock Wave Therapies in Treatment of Lateral Epicondylitis. Türkiye Fiz. Tip Rehabil. Derg. 2014, 60, 194–198. [Google Scholar] [CrossRef]
- Khoury, V.; Cardinal, É. “Tenomalacia”: A New Sonographic Sign of Tendinopathy? Eur. Radiol. 2008, 19, 144–146. [Google Scholar] [CrossRef]
- Fess, E. Grip Strength, Clinical Assessment Recommendations, 3rd ed.; American Society of Hand Therapists: Chicago, IL, USA, 1992; pp. 41–50. [Google Scholar]
- Rosenthal, R. The Handbook of Rsearch Syenthesis; Russell Sage Foundation: New York, NY, USA, 1994; pp. 231–244. [Google Scholar]
- Ialongo, C. Understanding the Effect Size and Its Measures. Biochem. Med. 2016, 26, 150–163. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioural Sciences; Lawrence 519 Earlbaum Associates: Hillside, NJ, USA, 1988; p. 26. [Google Scholar]
- Wang, C.; Wang, F.; Yang, K.; Weng, L.; Hsu, C.; Huang, C.; Yang, L. Shock Wave Therapy Induces Neovascularization at the Tendon–Bone Junction. A Study in Rabbits. J. Orthop. Res. 2003, 21, 984–989. [Google Scholar] [CrossRef]
- Wang, C. Extracorporeal Shockwave Therapy in Musculoskeletal Disorders. J. Orthop. Surg. Res. 2012, 7, 11. [Google Scholar] [CrossRef] [PubMed]
- Speed, C. Extracorporeal Shock-Wave Therapy in the Management of Chronic Soft-Tissue Conditions. J. Bone Jt. Surg. Br. Vol. 2004, 86-B, 165–171. [Google Scholar] [CrossRef]
- Chen, Y.; Wang, C.; Yang, K.; Kuo, Y.; Huang, H.; Huang, Y.; Sun, Y.; Wang, F. Extracorporeal Shock Waves Promote Healing of Collagenase-Induced Achilles Tendinitis and Increase TGF-Β1 and IGF-I Expression. J. Orthop. Res. 2004, 22, 854–861. [Google Scholar] [CrossRef]
- Ko, J.; Chen, H.; Chen, L. Treatment Of Lateral Epicondylitis of the Elbow with Shock Waves. Clin. Orthop. Relat. Res. 2001, 387, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Pettrone, F. Extracorporeal Shock Wave Therapy without Local Anesthesia for Chronic Lateral Epicondylitis. J. Bone Jt. Surg. 2005, 87, 1297. [Google Scholar]
- Korthals-de Bos, I.; Smidt, N.; Tulder, M.; Bouter, L. MS1: Cost-Effectiveness of Interventions for Lateral Epicondylitis: Results from a Randomized Controlled Trial in Primary Care. Value Health 2001, 2, 63. [Google Scholar] [CrossRef][Green Version]
- McClure, S. Extracorporeal Shock Wave Therapy: What? Why? Safety? Iowa State University, College of Veterinary Medicine: Iowa City, IA, USA, 2007; pp. 1–12. [Google Scholar]
- Haake, M.; Thon, A.; Bette, M. Absence of Spinal Response to Extracorporeal Shock Waves on the Endogenous Opioid Systems in the Rat. Ultrasound Med. Biol. 2001, 27, 279–284. [Google Scholar] [CrossRef]
- Bjordal, J.; Lopes-Martins, R.; Joensen, J.; Couppe, C.; Ljunggren, A.; Stergioulas, A.; Johnson, M. A Systematic Review with Procedural Assessments and Meta-Analysis of Low Level Laser Therapy in Lateral Elbow Tendinopathy (Tennis Elbow). BMC Musculoskelet. Disord. 2008, 9, 75. [Google Scholar] [CrossRef]
- D’Vaz, A.; Ostor, A.; Speed, C.; Jenner, J.; Bradley, M.; Prevost, A.; Hazleman, B. Pulsed Low-Intensity Ultrasound Therapy For Chronic Lateral Epicondylitis: A Randomized Controlled Trial. Rheumatology 2005, 45, 566–570. [Google Scholar] [CrossRef] [PubMed]
- Greg, W.; Johnson, M.; Kara, C. Treatment Of Lateral Epicondylitis. Am. Fam. Physician. 2007, 76, 843–848. [Google Scholar]
- Cherry, E.; Agostinucci, J.; McLinden, J. The Effect of Cryotherapy and Exercise on Lateral Epicondylitis: A Controlled Randomised Study. Int. J. Ther. Rehabil. 2012, 19, 641–650. [Google Scholar] [CrossRef]
- Robertson, C.; Saratsiotis, J. A Review of Compressive Ulnar Neuropathy at the Elbow. J. Manip. Physiol. Ther. 2005, 28, 345. [Google Scholar] [CrossRef] [PubMed]
- Shaheen, H.; Alarab, A.; Ahmad, M.S. Effectiveness of Therapeutic Ultrasound and Kinesio Tape in Treatment of Tennis Elbow. J. Nov. Physiother. Rehabil. 2019, 3, 25–33. [Google Scholar] [CrossRef]
- Draper, D.; Castel, J.; Castel, D. Rate of Temperature Increase in Human Muscle during 1 MHz and 3 MHz Continuous Ultrasound. J. Orthop. Sports Phys. Ther. 1995, 22, 142–150. [Google Scholar] [CrossRef]
- Noble, J.; Lee, V.; Griffith-Noble, F. Therapeutic Ultrasound: The Effects Upon Cutaneous Blood Flow in Humans. Ultrasound Med. Biol. 2007, 33, 279–285. [Google Scholar] [CrossRef]
- Lehmann, J.; Masock, A.; Warren, C.; Koblanski, J. Effect of Therapeutic Temperatures on Tendon Extensibility. Arch. Phys. Med. Rehabil. 1970, 51, 481–487. [Google Scholar] [PubMed]
- Knight, L.; Draper, D. Therapeutic Ultrasound: Therapeutic Modalities, 2nd ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2013; pp. 252–282. [Google Scholar]
- Dinno, M.; Crum, L.; Wu, J. The Effect of Therapeutic Ultrasound on Electrophysiological Parameters of Frog Skin. Ultrasound Med. Biol. 1989, 15, 461–470. [Google Scholar] [CrossRef]
- McConnell, J.; McIntosh, B. The Effect of Tape on Glenohumeral Rotation Range of Motion in Elite Junior Tennis Players. Clin. J. Sport Med. 2009, 19, 90–94. [Google Scholar] [CrossRef]
- Cyriax, J. Textbook of Orthopaedic Medicine; Baillière Tindall: London, UK, 1998. [Google Scholar]
- Lee, J.; Oh, J.; Kim, M. Effect of Deep Friction Massage with Taping Technique on Strength, Pain, Function and Wrist Extensor Muscle Activity in Patient with Tennis Elbow. J. Musculoskelet. Sci. Technol. 2020, 4, 76–83. [Google Scholar] [CrossRef]
- Whaley, A.; Baker, C. Lateral Epicondylitis. Clin. Sports Med. 2004, 23, 677–691. [Google Scholar] [CrossRef] [PubMed]
- Warren, R. Tennis Elbow (Epicondylitis): Epidemiology and Conservative Treatment. In AAOS Symposium and Upper Extremity Injuries in Athletes; Pettrone, F.A., Ed.; C.V. Mosby: St. Louis, MO, USA, 1986; pp. 233–243. [Google Scholar]
- Viswas, R.; Ramachandran, R.; Korde Anantkumar, P. Comparison of Effectiveness of Supervised Exercise Program and Cyriax Physiotherapy in Patients with Tennis Elbow (Lateral Epicondylitis): A Randomized Clinical Trial. Sci. World J. 2012, 2012, 939645. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | Shock-Wave Experimental Group (n = 20) | CPT Control Group (n = 20) | All Participants (n = 40) | p Value |
|---|---|---|---|---|
| Age: mean ± SD | 42.0 ± 7.30 | 42.37 ± 6.69 | 42.28 ± 6.91 | 0.923 |
| Gender: n (%) | 0.513 | |||
| Male | 11 | 10 | 24 | |
| Female | 9 | 10 | 19 | |
| Weight | 81.10 ± 13.30 | 81.89 ± 11.65 | 81.49 ± 12.37 | 0.967 |
| High | 1.77 ± 0.14 | 1.77 ± 0.15 | 1.77 ± 0.14 | 0.989 |
| Injury duration (Months) | 8.41 ± 1.33 | 9.23 ± 1.17 | 8.82 ± 1.25 | 0.671 |
| Right/Left elbow | 17/5 | 20/1 | 37/6 | 0.678 |
| Within Group Difference | Between Groups Difference | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Shock-Wave Experimental Group (n = 20) | CPT Control Group (n = 20) | |||||||||
| Baseline Mean ± SD | Post-treatment Mean ± SD | Effect size | p-Value | Baseline Mean ± SD | Post-treatment Mean ± SD | Effect size | p-Value | Cohen’s d | p-Value $ | |
| VAS | 8.25 ± 0.72 | 1.75 ± 0.85 | 0.18 | 0.000 * | 8.11 ± 0.81 | 3.37 ± 0.83 | 0.17 | 0.008 ** | 0.93 | 0.000 * |
| DASH | 59.70 ± 5.50 | 48.89 ± 2.77 | 0.17 | 0.000 * | 57.94 ± 6.15 | 54.47 ± 6.44 | 0.14 | 0.005 ** | 0.83 | 0.000 * |
| MGS | 23.20 ± 3.81 | 27.48 ± 2.69 | 0.21 | 0.000 * | 24.95 ± 3.96 | 25.68 ± 3.51 | 0.19 | 0.033 ** | 0.81 | 0.029 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aldajah, S.; Alashram, A.R.; Annino, G.; Romagnoli, C.; Padua, E. Analgesic Effect of Extracorporeal Shock-Wave Therapy in Individuals with Lateral Epicondylitis: A Randomized Controlled Trial. J. Funct. Morphol. Kinesiol. 2022, 7, 29. https://doi.org/10.3390/jfmk7010029
Aldajah S, Alashram AR, Annino G, Romagnoli C, Padua E. Analgesic Effect of Extracorporeal Shock-Wave Therapy in Individuals with Lateral Epicondylitis: A Randomized Controlled Trial. Journal of Functional Morphology and Kinesiology. 2022; 7(1):29. https://doi.org/10.3390/jfmk7010029
Chicago/Turabian StyleAldajah, Salameh, Anas R. Alashram, Giuseppe Annino, Cristian Romagnoli, and Elvira Padua. 2022. "Analgesic Effect of Extracorporeal Shock-Wave Therapy in Individuals with Lateral Epicondylitis: A Randomized Controlled Trial" Journal of Functional Morphology and Kinesiology 7, no. 1: 29. https://doi.org/10.3390/jfmk7010029
APA StyleAldajah, S., Alashram, A. R., Annino, G., Romagnoli, C., & Padua, E. (2022). Analgesic Effect of Extracorporeal Shock-Wave Therapy in Individuals with Lateral Epicondylitis: A Randomized Controlled Trial. Journal of Functional Morphology and Kinesiology, 7(1), 29. https://doi.org/10.3390/jfmk7010029