
Extracellular to Intracellular Body Water and Cognitive Function among Healthy Older and Younger Adults

Abstract
:1. Introduction
2. Materials and Methods
2.1. Cognitive Testing
2.2. Regional Bioimpedance Analysis
2.3. Statistical Analysis
3. Results
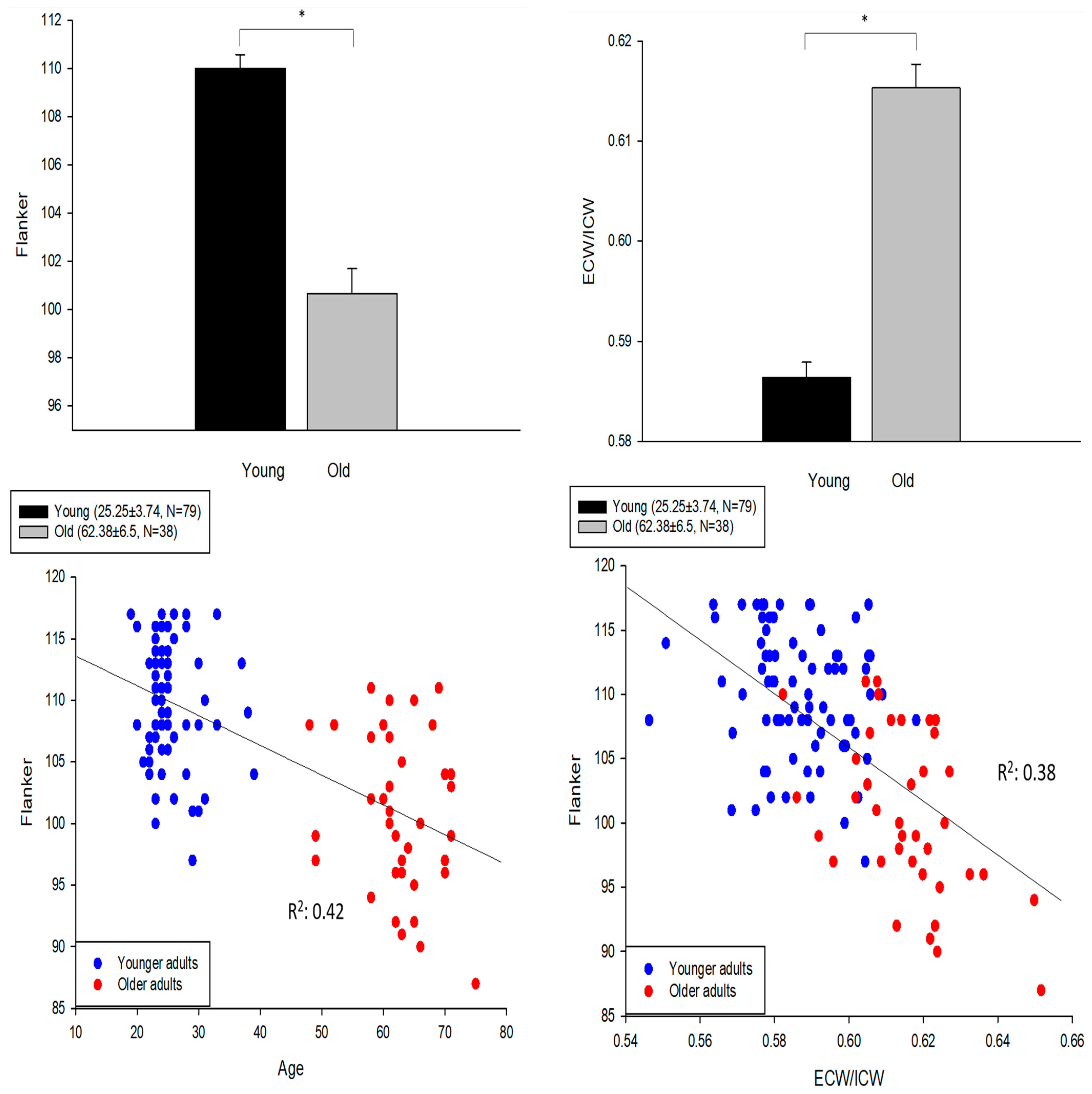
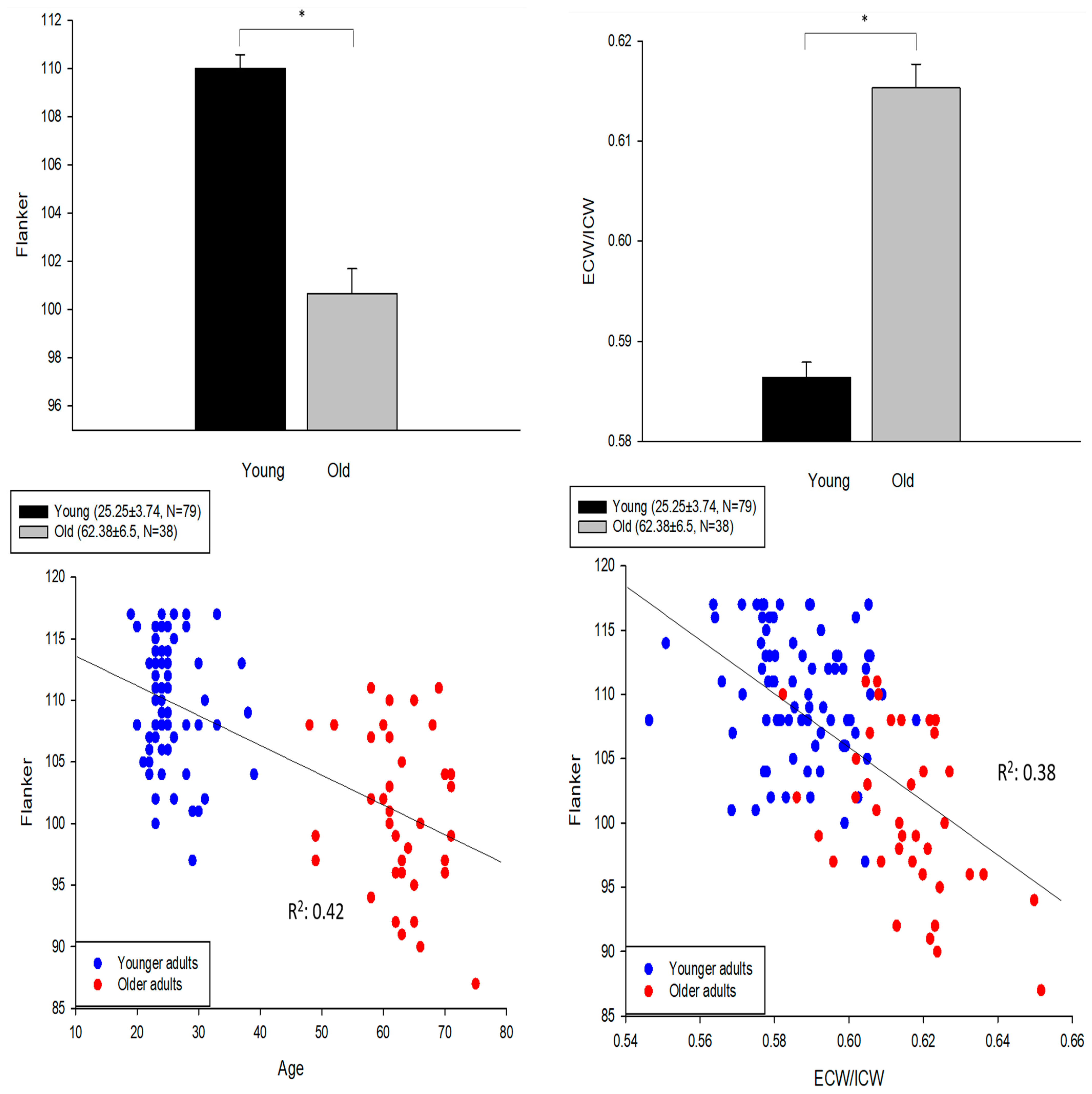
3.1. Fluid Cognition among Young and Older Groups
3.2. Associations with the Type of Cognitive Function Assessed
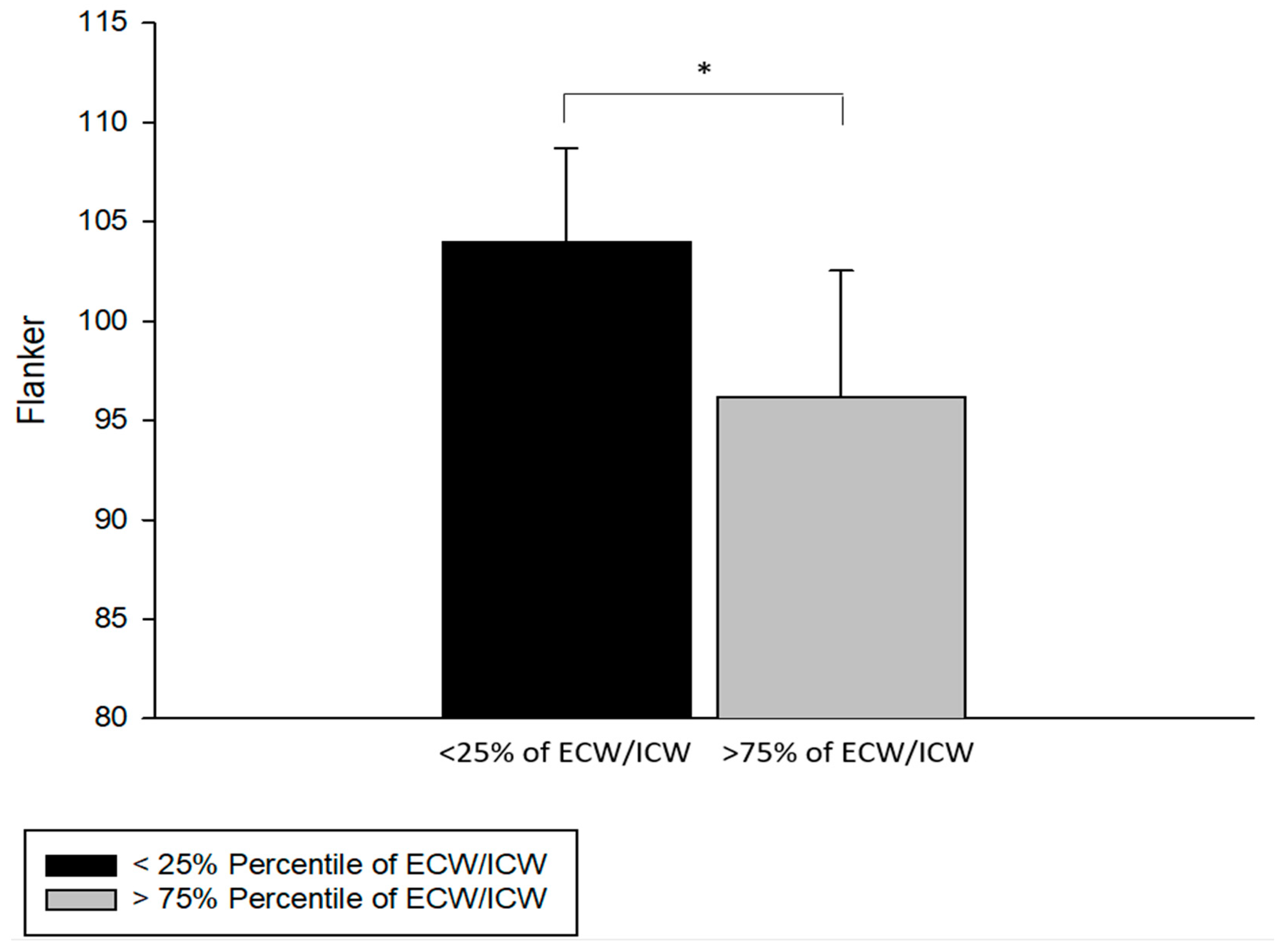
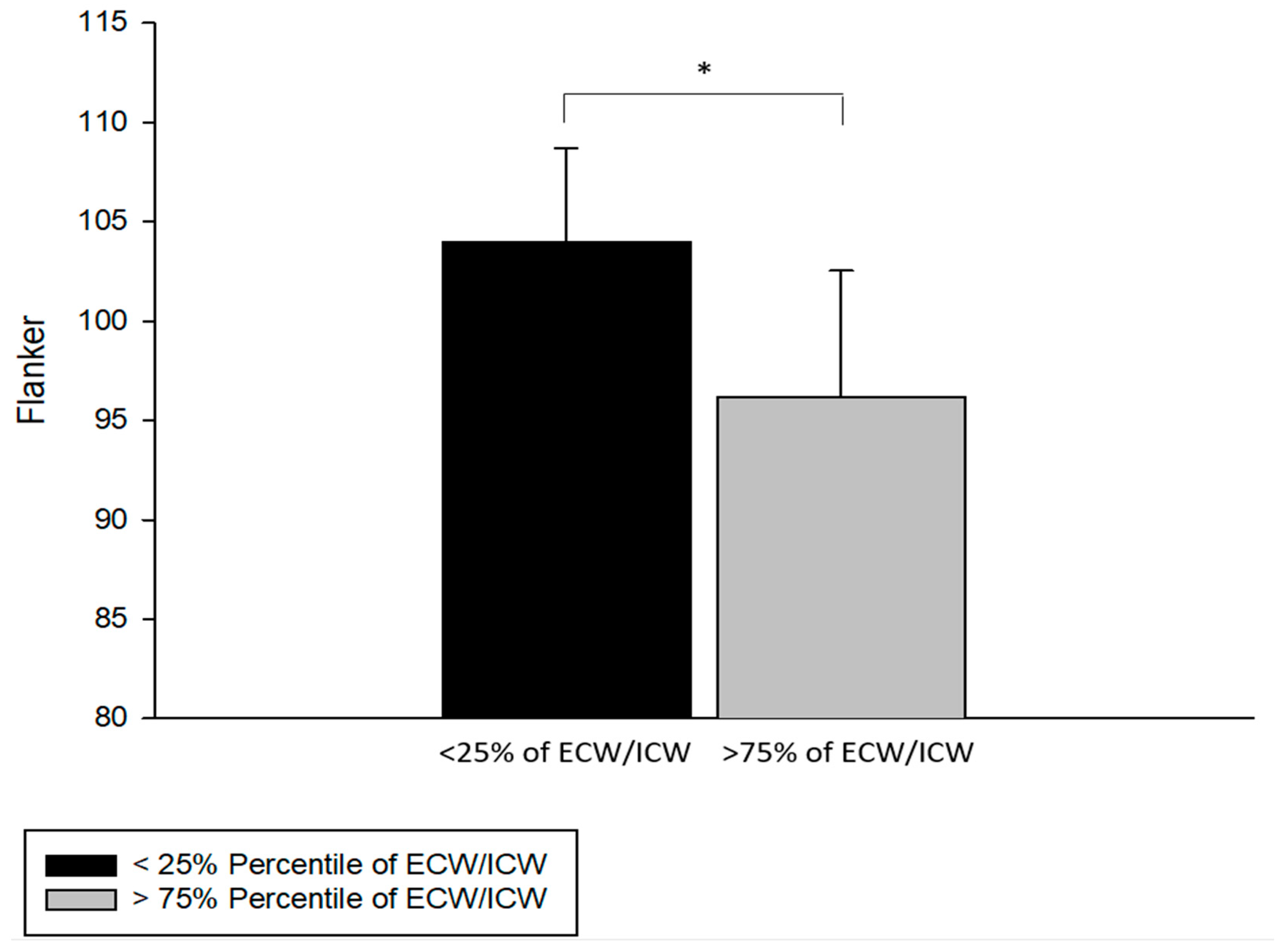
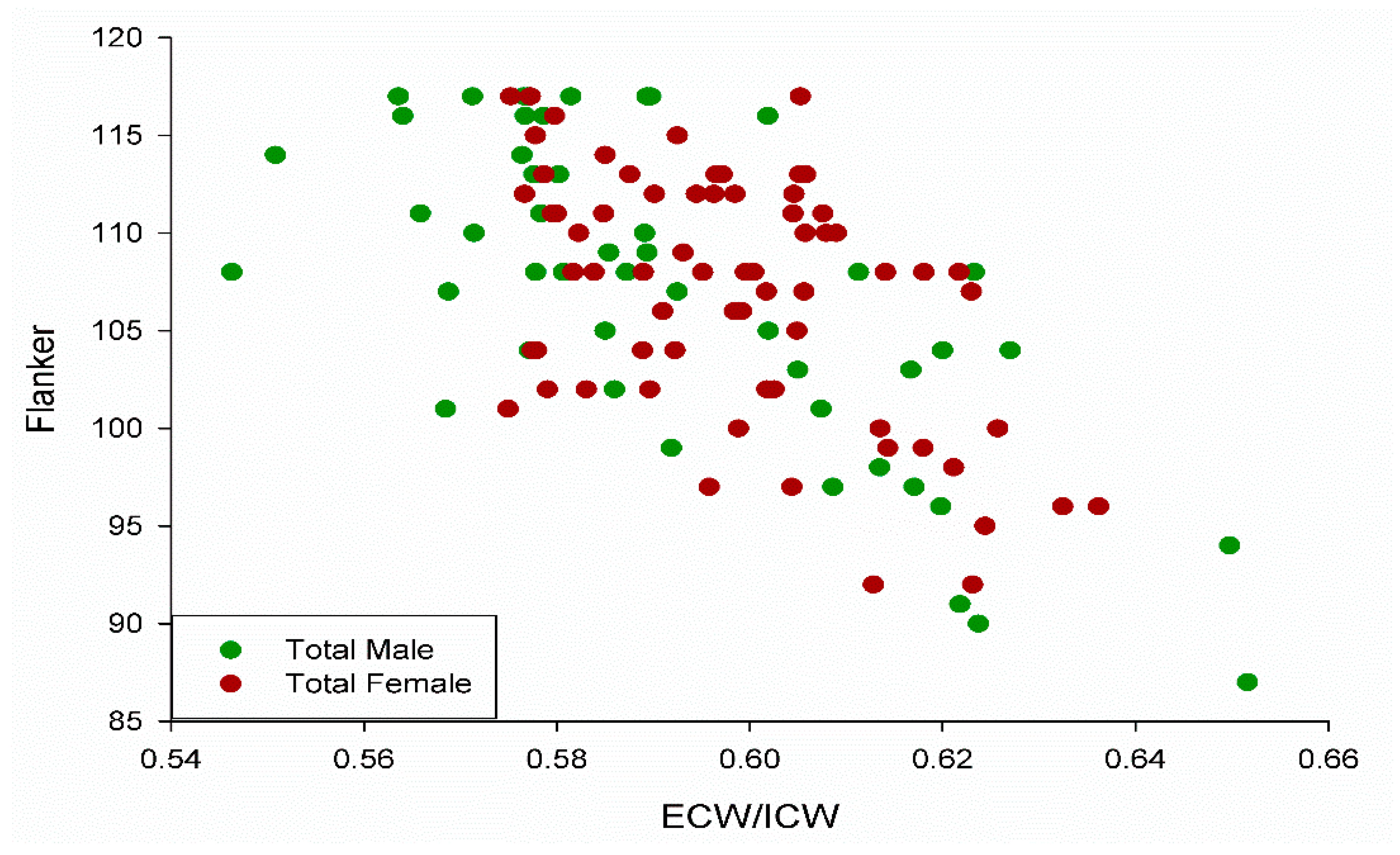
3.3. Extracellular/Intracellular Water and the Flanker Test
3.4. Stepwise Regression Analysis to Predict Cognitive Function
4. Discussion
4.1. Potential Mechanisms Relating Extracellular Water and Cognitive Function
4.2. Acute Regulation of Body Water Compartments
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Leibson, C.L.; Long, K.H.; Ransom, J.E.; Roberts, R.O.; Hass, S.L.; Duhig, A.M.; Smith, C.Y.; Emerson, J.A.; Pankratz, V.S.; Petersen, R.C. Direct medical costs and source of cost differences across the spectrum of cognitive decline: A population-based study. Alzheimers Dement. 2015, 11, 917–932. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santos-Parker, J.R.; Lubieniecki, K.L.; Rossman, M.J.; Van Ark, H.J.; Bassett, C.J.; Strahler, T.R.; Chonchol, M.B.; Justice, J.N.; Seals, D.R. Curcumin supplementation and motor-cognitive function in healthy middle-aged and older adults. Nutr. Healthy Aging 2018, 4, 323–333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muangpaisan, W.; Assantachai, P.; Intalapaporn, S.; Pisansalakij, D. Quality of life of the community-based patients with mild cognitive impairment. Geriatr. Gerontol. Int. 2008, 8, 80–85. [Google Scholar] [CrossRef] [PubMed]
- O’Shea, A.; Cohen, R.A.; Porges, E.C.; Nissim, N.R.; Woods, A.J. Cognitive aging and the hippocampus in older adults. Front. Aging Neurosci. 2016, 8, 298. [Google Scholar] [CrossRef]
- Akshoomoff, N.; Beaumont, J.L.; Bauer, P.J.; Dikmen, S.S.; Gershon, R.C.; Mungas, D.; Slotkin, J.; Tulsky, D.; Weintraub, S.; Zelazo, P.D.; et al. VIII. NIH toolbox cognition battery (CB): Composite scores of crystallized, fluid, and overall cognition. Monogr. Soc. Res. Child Dev. 2013, 78, 119–132. [Google Scholar] [CrossRef] [Green Version]
- Arvanitakis, Z.; Capuano, A.W.; Bennett, D.A.; Barnes, L.L. Body mass index and decline in cognitive function in older black and white persons. J. Gerontol. A Biol. Sci. Med. Sci. 2018, 73, 198–203. [Google Scholar] [CrossRef] [Green Version]
- Ohashi, Y.; Joki, N.; Yamazaki, K.; Kawamura, T.; Tai, R.; Oguchi, H.; Yuasa, R.; Sakai, K. Changes in the fluid volume balance between intra- and extracellular water in a sample of Japanese adults aged 15–88 yr old: A cross-sectional study. Am. J. Physiol. Ren. Physiol. 2018, 314, F614–F622. [Google Scholar] [CrossRef]
- Geng, J.; Wang, L.; Zhang, L.; Qin, C.; Song, Y.; Ma, Y.; Chen, Y.; Chen, S.; Wang, Y.; Zhang, Z.; et al. Blood-brain barrier disruption induced cognitive impairment is associated with increase of inflammatory cytokine. Front. Aging Neurosci. 2018, 10, 129. [Google Scholar] [CrossRef]
- Tsigos, C.; Stefanaki, C.; Lambrou, G.I.; Boschiero, D.; Chrousos, G.P. Stress and inflammatory biomarkers and symptoms are associated with bioimpedance measures. Eur. J. Clin. Investig. 2015, 45, 126–134. [Google Scholar] [CrossRef]
- Paulson, O.B. Blood–brain barrier, brain metabolism and cerebral blood flow. Eur. Neuropsychopharmacol. 2002, 12, 495–501. [Google Scholar] [CrossRef]
- Nishikawa, H.; Yoh, K.; Enomoto, H.; Ishii, N.; Iwata, Y.; Nakano, C.; Takata, R.; Nishimura, T.; Aizawa, N.; Sakai, Y.; et al. Extracellular water to total body water ratio in viral liver diseases: A study using bioimpedance analysis. Nutrients 2018, 10, 1072. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bektas, A.; Schurman, S.H.; Sen, R.; Ferrucci, L. Aging, inflammation and the environment. Exp. Gerontol. 2018, 105, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Hannoodee, S.; Nasuruddin, D.N. Acute inflammatory response. In StatPearls; StatPearls Publishing LLC: Treasure Island, FL, USA, 2021. [Google Scholar]
- Tarumi, T.; Zhang, R. Cerebral blood flow in normal aging adults: Cardiovascular determinants, clinical implications, and aerobic fitness. J. Neurochem. 2018, 144, 595–608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aging and metabolism: Two sides of the same coin. EBioMedicine 2017, 21, 1–2. [CrossRef]
- Marzuca-Nassr, G.N.; SanMartín-Calísto, Y.; Guerra-Vega, P.; Artigas-Arias, M.; Alegría, A.; Curi, R. Skeletal muscle aging atrophy: Assessment and exercise-based treatment. Adv. Exp. Med. Biol. 2020, 1260, 123–158. [Google Scholar] [CrossRef]
- Gekle, M. Kidney and aging—A narrative review. Exp. Gerontol. 2017, 87, 153–155. [Google Scholar] [CrossRef]
- Kehayias, J.J.; Ribeiro, S.M.; Skahan, A.; Itzkowitz, L.; Dallal, G.; Rogers, G.; Khodeir, M. Water homeostasis, frailty and cognitive function in the nursing home. J. Nutr. Health Aging 2012, 16, 35–39. [Google Scholar] [CrossRef]
- Low, S.; Ng, T.P.; Lim, C.L.; Ang, S.F.; Moh, A.; Wang, J.; Yap, P.; Cheong, C.Y.; Goh, K.S.; Ang, K.; et al. Higher ratio of extracellular water to total body water was associated with reduced cognitive function in type 2 diabetes. J. Diabetes 2021, 13, 222–231. [Google Scholar] [CrossRef]
- Zelazo, P.D.; Anderson, J.E.; Richler, J.; Wallner-Allen, K.; Beaumont, J.L.; Conway, K.P.; Gershon, R.; Weintraub, S. NIH Toolbox Cognition Battery (CB): Validation of executive function measures in adults. J. Int. Neuropsychol. Soc. 2014, 20, 620–629. [Google Scholar] [CrossRef] [Green Version]
- Tulsky, D.S.; Carlozzi, N.; Chiaravalloti, N.D.; Beaumont, J.L.; Kisala, P.A.; Mungas, D.; Conway, K.; Gershon, R. NIH Toolbox Cognition Battery (NIHTB-CB): List sorting test to measure working memory. J. Int. Neuropsychol. Soc. 2014, 20, 599–610. [Google Scholar] [CrossRef] [Green Version]
- Dikmen, S.S.; Bauer, P.J.; Weintraub, S.; Mungas, D.; Slotkin, J.; Beaumont, J.L.; Gershon, R.; Temkin, N.R.; Heaton, R.K. Measuring episodic memory across the lifespan: NIH toolbox picture sequence memory test. J. Int. Neuropsychol. Soc. 2014, 20, 611–619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heaton, R.K.; Akshoomoff, N.; Tulsky, D.; Mungas, D.; Weintraub, S.; Dikmen, S.; Beaumont, J.; Casaletto, K.B.; Conway, K.; Slotkin, J.; et al. Reliability and validity of composite scores from the NIH toolbox cognition battery in adults. J. Int. Neuropsychol. Soc. 2014, 20, 588–598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carlozzi, N.E.; Tulsky, D.S.; Chiaravalloti, N.D.; Beaumont, J.L.; Weintraub, S.; Conway, K.; Gershon, R.C. NIH toolbox cognitive battery (NIHTB-CB): The NIHTB pattern comparison processing speed test. J. Int. Neuropsychol. Soc. 2014, 20, 630–641. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slotkin, J.; Kallen, M.; Griffith, J.; Magasi, S.; Salsman, J.; Nowinski, C.J.; Gershon, R. NIH Toolbox Technical Manual—Dimensional Change Card Sort Test; National Institutes of Health and Northwestern University: Chicago, IL, USA, 2012. [Google Scholar]
- Slotkin, J.; Kallen, M.; Griffith, J.; Magasi, S.; Salsman, J.; Nowinski, C.J.; Gershon, R. NIH Toolbox Technical Manual—Flanker Inhibitory Control and Attention Test; National Institutes of Health and Northwestern University: Chicago, IL, USA, 2012. [Google Scholar]
- Slotkin, J.; Kallen, M.; Griffith, J.; Magasi, S.; Salsman, J.; Nowinski, C.J.; Gershon, R. NIH Toolbox Technical Manual—List Sorting Working Memory Test; National Institutes of Health and Northwestern University: Chicago, IL, USA, 2012. [Google Scholar]
- Cole, K.R.; Yen, C.L.; Dudley-Javoroski, S.; Shields, R.K. NIH toolbox cognition battery in young and older adults: Reliability and relationship to adiposity and physical activity. J. Geriatr. Phys. Ther. 2019, 44, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Dudley-Javoroski, S.; Shields, R.K. Motor demands of cognitive testing may artificially reduce executive function scores in individuals with spinal cord injury. J. Spinal Cord Med. 2019, 44, 253–261. [Google Scholar] [CrossRef] [PubMed]
- Bauer, P.J.; Dikmen, S.S.; Heaton, R.K.; Mungas, D.; Slotkin, J.; Beaumont, J.L. III. NIH toolbox cognition battery (CB): Measuring episodic memory. Monogr Soc. Res. Child Dev. 2013, 78, 34–48. [Google Scholar] [CrossRef] [Green Version]
- Slotkin, J.; Kallen, M.; Griffith, J.; Magasi, S.; Salsman, J.; Nowinski, C.J.; Gershon, R. NIH Toolbox Technical Manual—Picture Sequence Memory Test; National Institutes of Health and Northwestern University: Chicago, IL, USA, 2012. [Google Scholar]
- Slotkin, J.; Nowinski, C.; Hays, R.; Beaumont, J.; Griffith, J.; Magasi, S.; Gershon, R. NIH Toolbox Scoring and Interpretation Guide; National Institutes of Health and Northwestern University: Washington, DC, USA, 2012. [Google Scholar]
- Cha, K. InBody S10 User’s Manual; InBody: Seoul, Korea, 1996. [Google Scholar]
- Bosy-Westphal, A.; Schautz, B.; Later, W.; Kehayias, J.J.; Gallagher, D.; Müller, M.J. What makes a BIA equation unique? Validity of eight-electrode multifrequency BIA to estimate body composition in a healthy adult population. Eur. J. Clin. Nutr. 2013, 67, S14–S21. [Google Scholar] [CrossRef] [Green Version]
- Mooijaart, S.P.; Sattar, N.; Trompet, S.; Lucke, J.; Stott, D.J.; Ford, I.; Jukema, J.W.; Westendorp, R.G.; de Craen, A.J.; Group, P.S. Circulating interleukin-6 concentration and cognitive decline in old age: The PROSPER study. J. Intern. Med. 2013, 274, 77–85. [Google Scholar] [CrossRef]
- Li, M.; Li, Y.; Zuo, L.; Hu, W.; Jiang, T. Increase of blood-brain barrier leakage is related to cognitive decline in vascular mild cognitive impairment. BMC Neurol. 2021, 21, 159. [Google Scholar] [CrossRef]
- Sui, S.X.; Williams, L.J.; Holloway-Kew, K.L.; Hyde, N.K.; Pasco, J.A. Skeletal muscle health and cognitive function: A narrative review. Int. J. Mol. Sci. 2020, 22, 255. [Google Scholar] [CrossRef] [PubMed]
- Noh, H.M.; Oh, S.; Song, H.J.; Lee, E.Y.; Jeong, J.Y.; Ryu, O.H.; Hong, K.S.; Kim, D.H. Relationships between cognitive function and body composition among community-dwelling older adults: A cross-sectional study. BMC Geriatr. 2017, 17, 259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeki Al Hazzouri, A.; Haan, M.N.; Whitmer, R.A.; Yaffe, K.; Neuhaus, J. Central obesity, leptin and cognitive decline: The Sacramento area Latino study on aging. Dement. Geriatr. Cogn. Disord. 2012, 33, 400–409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gumus, M.; Multani, N.; Mack, M.L.; Tartaglia, M.C. Progression of neuropsychiatric symptoms in young-onset versus late-onset Alzheimer’s disease. GeroScience 2021, 43, 213–223. [Google Scholar] [CrossRef] [PubMed]
- Shields, R.K. Precision rehabilitation: How lifelong healthy behaviors modulate biology, determine health, and affect populations. Phys. Ther. 2021, 102, pzab248. [Google Scholar] [CrossRef] [PubMed]
- Petrie, M.A.; Taylor, E.B.; Suneja, M.; Shields, R.K. Genomic and Epigenomic evaluation of electrically induced exercise in people with spinal cord injury: Application to precision rehabilitation. Phys. Ther. 2021, 102, pzab248. [Google Scholar] [CrossRef] [PubMed]
- Shields, R.K.; Dudley-Javoroski, S. Epigenetics and the international classification of functioning, disability and health model: Bridging nature, nurture, and patient-centered population health. Phys. Ther. 2021, 102, pzab247. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Lee, S.; Wong, W.T.; Waleed, K.B.; Leung, K.S.K.; Lee, T.T.L.; Wai, A.K.C.; Liu, T.; Chang, C.; Cheung, B.M.Y.; et al. Gender-specific clinical risk scores incorporating blood pressure variability for predicting incident dementia. J. Am. Med Inform. Assoc. 2021, 29, 335–347. [Google Scholar] [CrossRef]
- Abramowitz, M.K.; Hall, C.B.; Amodu, A.; Sharma, D.; Androga, L.; Hawkins, M. Muscle mass, BMI, and mortality among adults in the United States: A population-based cohort study. PLoS ONE 2018, 13, e0194697. [Google Scholar] [CrossRef]
- De Silva, N.A.; Gregory, M.A.; Venkateshan, S.S.; Verschoor, C.P.; Kuspinar, A. Examining the association between life-space mobility and cognitive function in older adults: A systematic review. J. Aging Res. 2019, 2019, 3923574. [Google Scholar] [CrossRef] [Green Version]
- Stephenson, L.A.; Kolka, M.A. Plasma volume during heat stress and exercise in women. Eur. J. Appl. Physiol. Occup. Physiol. 1988, 57, 373–381. [Google Scholar] [CrossRef]
- Draper, C.F.; Duisters, K.; Weger, B.; Chakrabarti, A.; Harms, A.C.; Brennan, L.; Hankemeier, T.; Goulet, L.; Konz, T.; Martin, F.P.; et al. Menstrual cycle rhythmicity: Metabolic patterns in healthy women. Sci. Rep. 2018, 8, 14568. [Google Scholar] [CrossRef] [PubMed]
- Stachenfeld, N.S.; Silva, C.; Keefe, D.L.; Kokoszka, C.A.; Nadel, E.R. Effects of oral contraceptives on body fluid regulation. J. Appl. Physiol. 1999, 87, 1016–1025. [Google Scholar] [CrossRef] [PubMed]
- Le, J.; Thomas, N.; Gurvich, C. Cognition, the menstrual cycle, and premenstrual disorders: A review. Brain Sci. 2020, 10, 198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sherwin, B.B. Estrogen and cognitive functioning in women. Endocr. Rev. 2003, 24, 133–151. [Google Scholar] [CrossRef] [Green Version]
- Wilson, A.C.; Clemente, L.; Liu, T.; Bowen, R.L.; Meethal, S.V.; Atwood, C.S. Reproductive hormones regulate the selective permeability of the blood-brain barrier. Biochim. Biophys. Acta 2008, 1782, 401–407. [Google Scholar] [CrossRef] [Green Version]
- Wittbrodt, M.T.; Millard-Stafford, M. Dehydration impairs cognitive performance: A meta-analysis. Med. Sci. Sports Exerc. 2018, 50, 2360–2368. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Older (n = 39, 48–75 y, 20F) | Younger (n = 79, 19–39 y, 48F) | p-Value | |
|---|---|---|---|
| Age | 62.38 ± 6.5 | 25.25 ± 3.74 | <0.05 |
| Weight | 78.41 ± 18.44 (kg) | 72.1 ± 14.1 (kg) | =0.09 |
| Height | 167.77 ± 8.71 (cm) | 172.91 ± 9.73 (cm) | <0.05 |
| Body Mass Index (BMI) | 27.8 ± 5.9 | 24.08 ± 4.3 | <0.05 |
| ECW/ICW | 0.61 ± 0.02 | 0.59 ± 0.01 | <0.05 |
| Lean (kg) | 14.35 ± 3.03 | 15.41 ± 3.41 | =0.16 |
| Fat (kg) | 24.26 ± 12.74 | 15.15 ± 9.89 | <0.05 |
| Lean/Fat | 0.93 ± 1.25 | 1.51 ± 1.14 | <0.05 |
| % Body Fat | 29.84 ± 11.21 | 20.65 ± 10.5 | <0.05 |
| Pattern Comparison | 101.56 ± 17.79 | 133.46 ± 13.22 | <0.05 |
| Picture Sequence | 111 ± 14.19 | 124.3 ± 11.8 | <0.05 |
| Dim Change Card Sort | 107.62 ± 7.21 | 115.84 ± 4.97 | <0.05 |
| Flanker | 100.54 ± 6.3 | 110 ± 4.97 | <0.05 |
| List Sorting | 107.44 ± 8.14 | 113.11 ± 9.59 | <0.05 |
| Pattern Comparison | Weight | Height | BMI | Percentage Body Fat | Lean/Fat | Age | ECW/ICW |
|---|---|---|---|---|---|---|---|
| Combined Group | 0.02 | 0.01 | 0.04 | 0.05 | 0.03 | 0.51 | 0.32 |
| Older Group | <0.01 | 0.1 | 0.02 | 0.06 | 0.03 | 0.05 | 0.15 |
| Younger Group | <0.01 | <0.01 | <0.01 | <0.01 | 0.02 | <0.01 | <0.01 |
| Picture Sequence Memory | |||||||
| Combined Group | 0.01 | 0.01 | <0.01 | <0.01 | <0.01 | 0.24 | 0.11 |
| Older Group | 0.01 | 0.16 | 0.01 | 0.07 | 0.03 | 0.13 | 0.05 |
| Younger Group | <0.01 | 0.02 | 0.02 | 0.01 | 0.02 | <0.01 | 0.01 |
| Dimensional Change Card Sort | |||||||
| Combined Group | 0.01 | <0.01 | 0.02 | 0.05 | 0.05 | 0.3 | 0.24 |
| Older Group | <0.01 | 0.06 | 0.01 | 0.02 | <0.01 | 0.02 | 0.09 |
| Younger Group | <0.01 | <0.01 | <0.01 | 0.01 | <0.01 | <0.01 | 0.01 |
| Flanker Inhibitory Control and Attention | |||||||
| Combined Group | 0.01 | 0.03 | 0.04 | 0.12 | 0.11 | 0.42 | 0.38 |
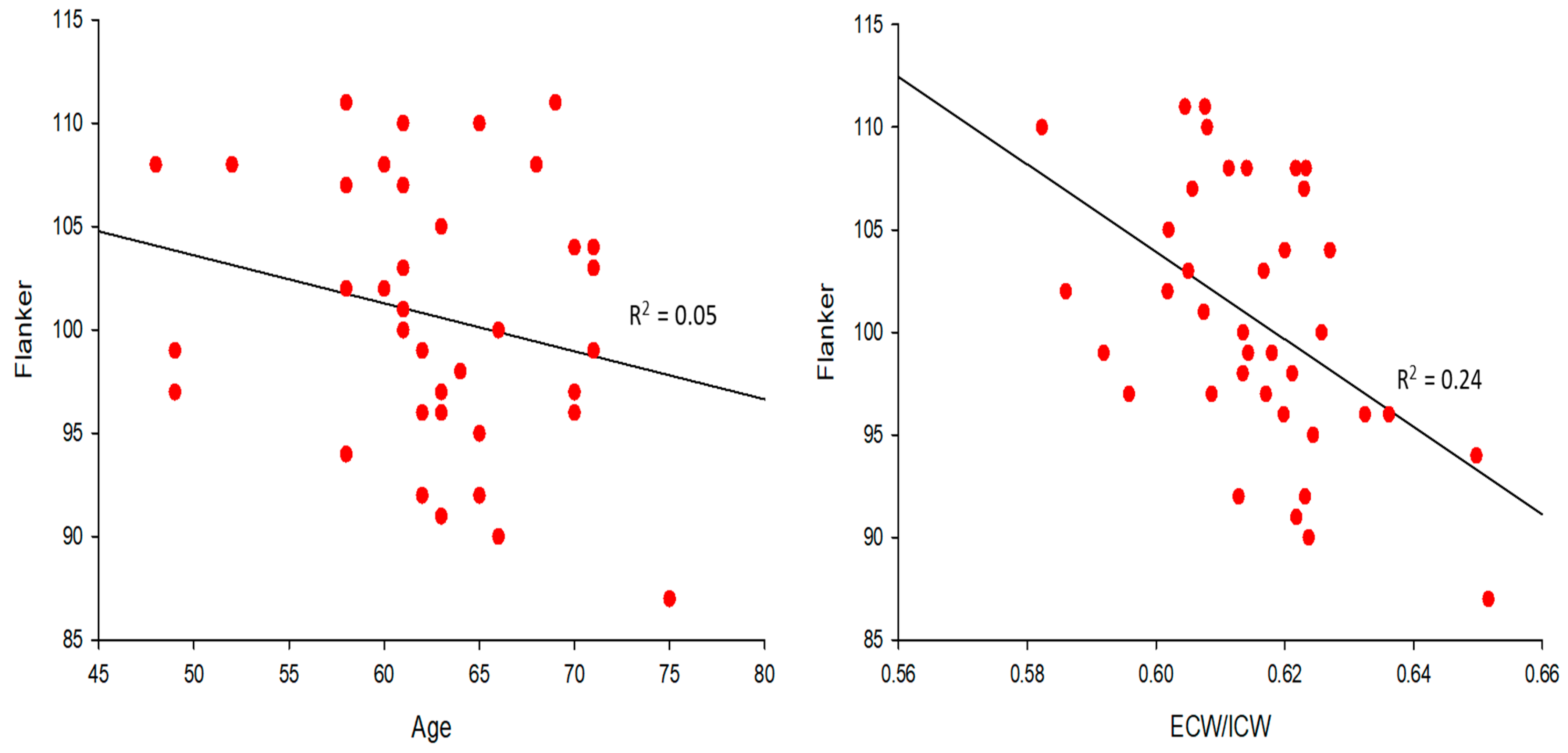
| Older Group | 0.01 | 0.08 | <0.01 | 0.01 | <0.01 | 0.05 | 0.24 |
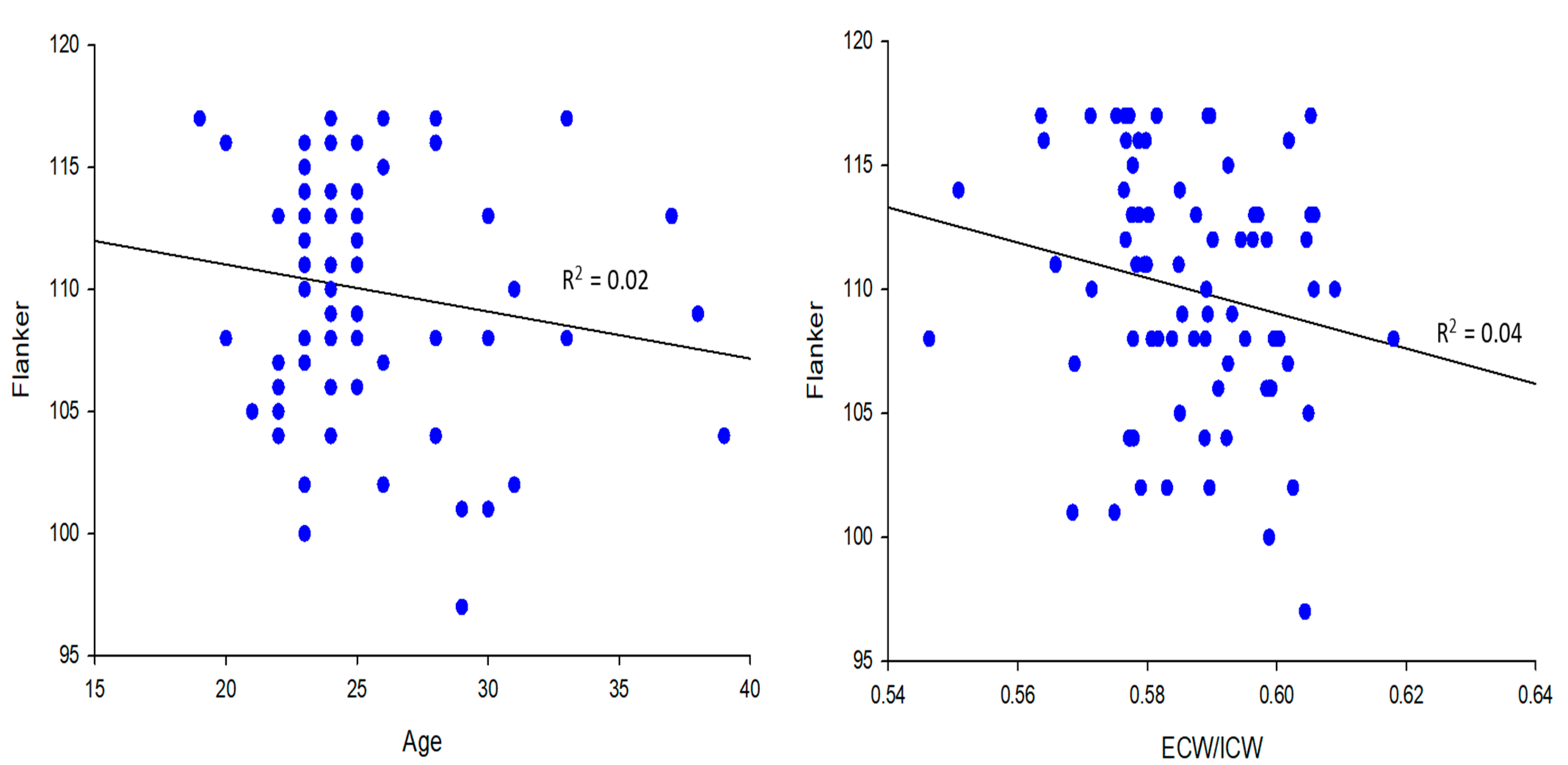
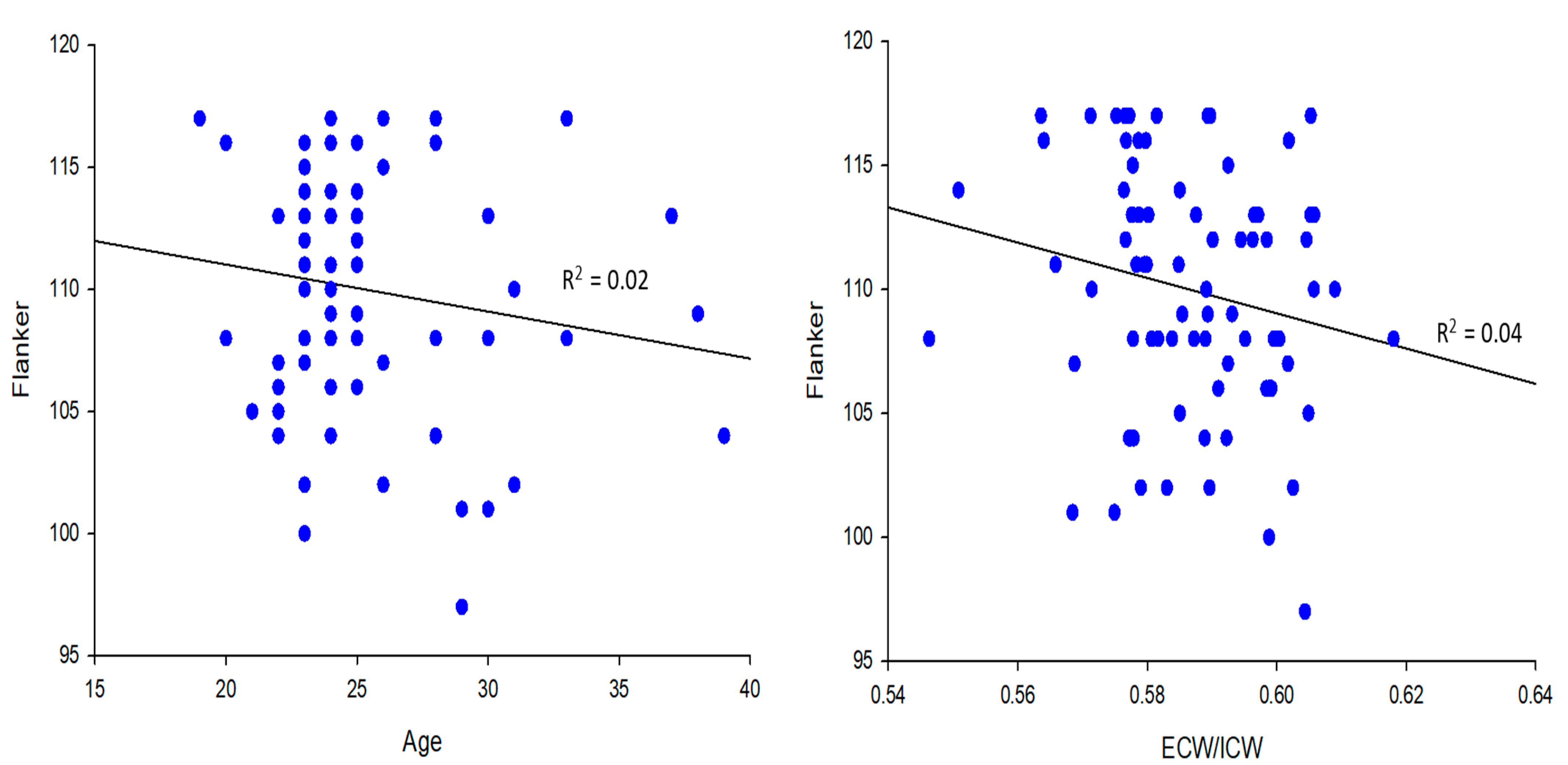
| Younger Group | <0.01 | 0.02 | <0.01 | 0.08 | 0.04 | 0.02 | 0.04 |
| List Sorting Working Memory | |||||||
| Combined Group | <0.01 | <0.01 | <0.01 | 0.01 | <0.01 | 0.08 | 0.06 |
| Older Group | 0.04 | 0.02 | 0.03 | <0.01 | <0.01 | 0.02 | 0.04 |
| Younger Group | <0.01 | 0.01 | <0.01 | <0.01 | 0.02 | 0.01 | <0.01 |
| Combined Group | Variable | R-Squared |
|---|---|---|
| Step 1 | Age | 0.42 |
| Step 2 | ECW/ICW | 0.48 |
| Young Group | ||
| Step 1 | Young Percentage Body Fat | 0.08 |
| Step 2 | Young BMI | 0.11 |
| Step 3 | Age | 0.13 |
| Step 4 | Lean/Fat | 0.16 |
| Old Group | ||
| Step 1 | ECW/ICW | 0.24 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.; Shields, R.K. Extracellular to Intracellular Body Water and Cognitive Function among Healthy Older and Younger Adults. J. Funct. Morphol. Kinesiol. 2022, 7, 18. https://doi.org/10.3390/jfmk7010018
Lee J, Shields RK. Extracellular to Intracellular Body Water and Cognitive Function among Healthy Older and Younger Adults. Journal of Functional Morphology and Kinesiology. 2022; 7(1):18. https://doi.org/10.3390/jfmk7010018
Chicago/Turabian StyleLee, Jinhyun, and Richard K. Shields. 2022. "Extracellular to Intracellular Body Water and Cognitive Function among Healthy Older and Younger Adults" Journal of Functional Morphology and Kinesiology 7, no. 1: 18. https://doi.org/10.3390/jfmk7010018
APA StyleLee, J., & Shields, R. K. (2022). Extracellular to Intracellular Body Water and Cognitive Function among Healthy Older and Younger Adults. Journal of Functional Morphology and Kinesiology, 7(1), 18. https://doi.org/10.3390/jfmk7010018