The Biomechanics of Pregnancy: A Systematic Review



Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
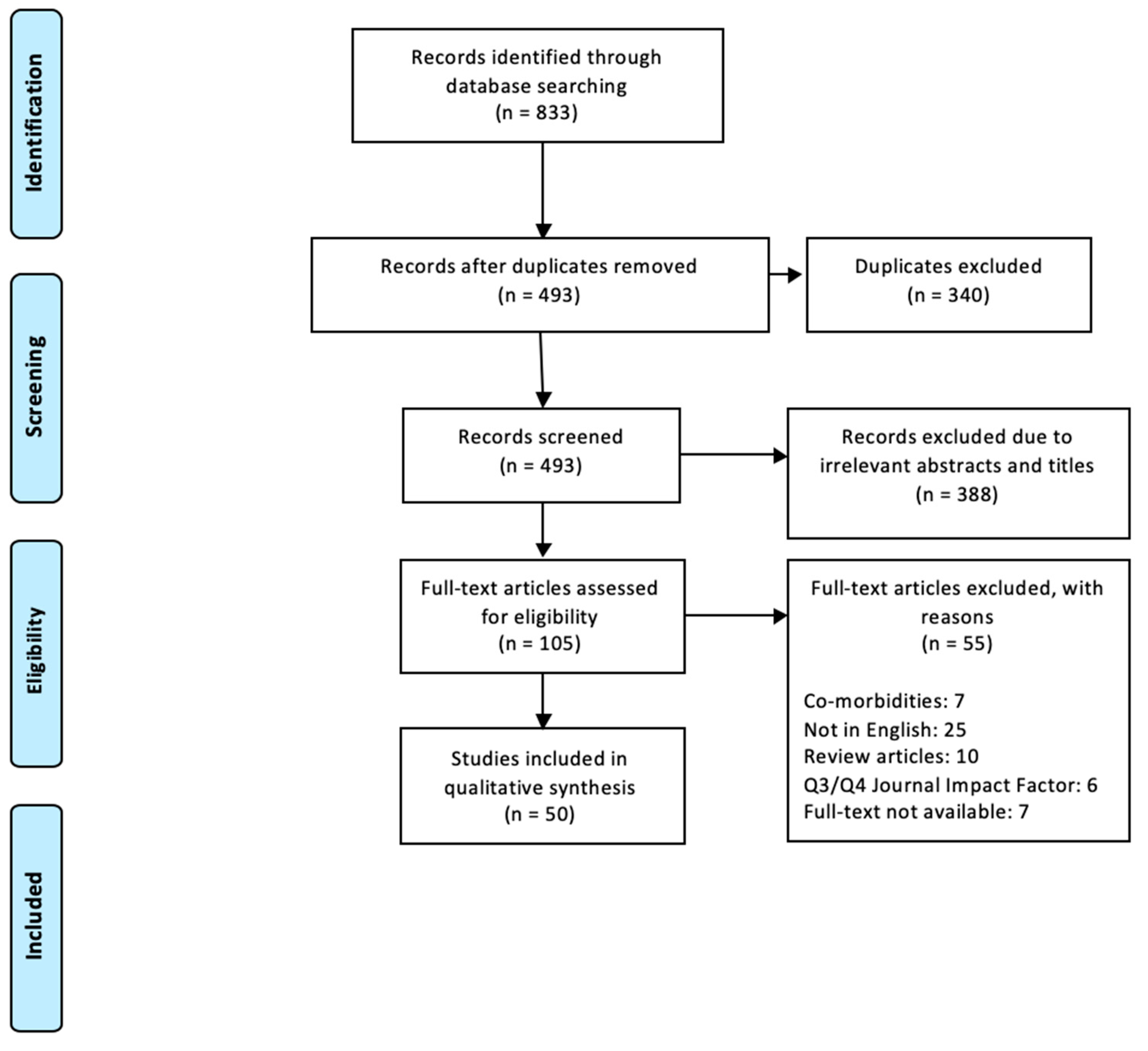
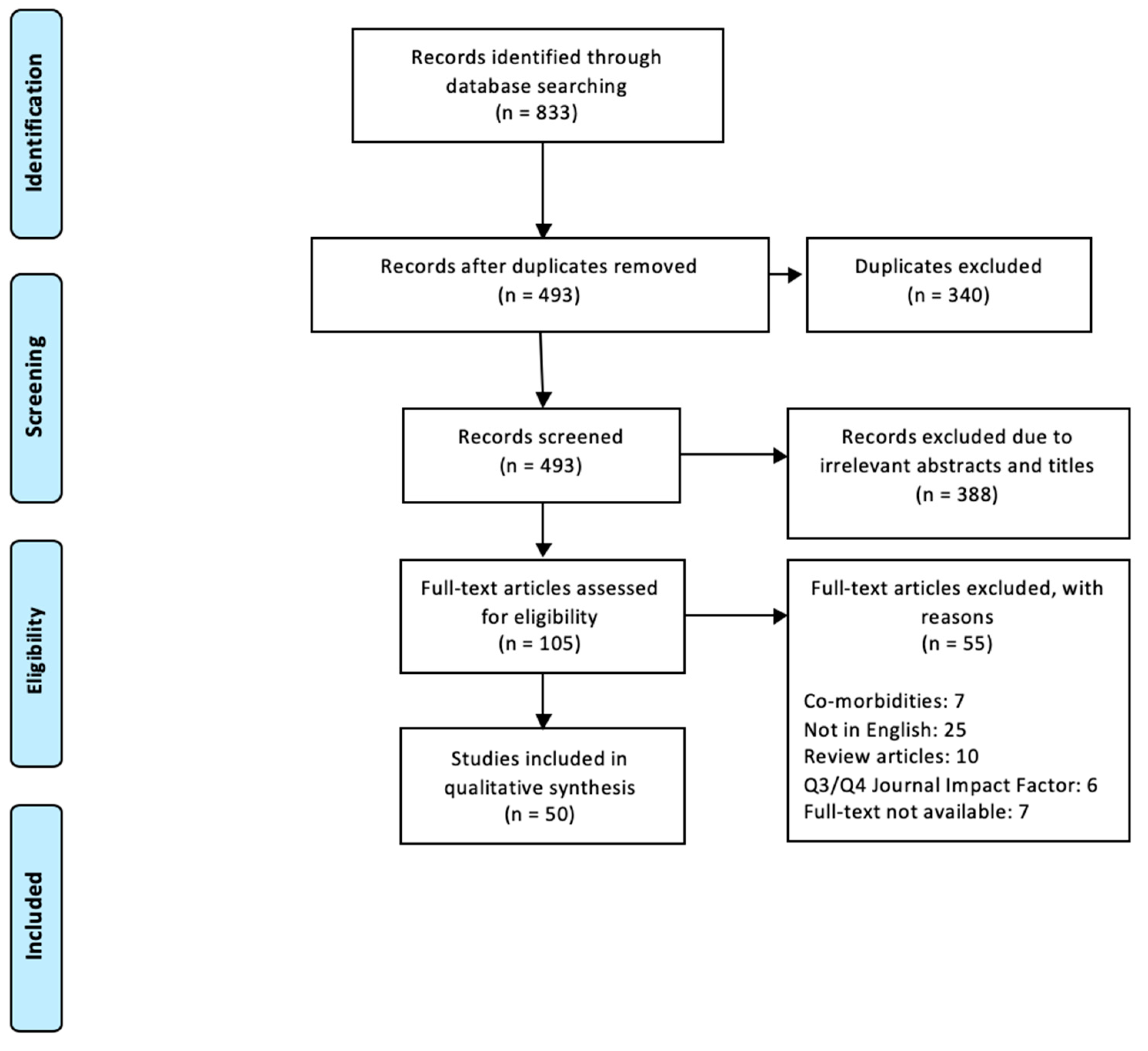
2.2. Selection Methods
- 1
- (Pregnancy OR Pregnant OR Pregnancies) AND (Biomechanics OR Biomechanical OR Biomechanically)
- 2
- (Pregnancy OR Pregnant OR Pregnancies) AND (Posture OR Postural)
- 3
- (Pregnancy OR Pregnant OR Pregnancies) AND (Gait)
- 4
- (Pregnancy OR Pregnant OR Pregnancies) AND (Stability)
3. Results and Discussion
3.1. Posture
3.1.1. Spinal Curvature
3.1.2. Trunk Range of Motion
3.2. Stability
3.2.1. Static Stability
3.2.2. Dynamic Stability
3.3. Gait
3.3.1. Spatial and Temporal Parameters
3.3.2. Joint Kinematics
3.3.3. Rising from a Chair
3.3.4. Trunk Control during Gait (Pelvic and Thoracic Rotations)
3.4. Anthropometric Changes
3.5. General Comments on the Quality of the Studies
4. Conclusions
Funding
Conflicts of Interest
Abbreviations
| COP | Centre of pressure |
| LBP | Lower back pain |
| WDI | Weight distribution index |
| COM | Centre of mass |
| AP | Anteroposterior |
| ML | Mediolateral |
| APSI | Anteroposterior stability index |
| OA | Overall stability index |
| MLSI | Mediolateral stability index |
| PGP | Pelvic girdle pain |
| PPP | Pregnancy-related pelvic girdle pain |
| QOL | Quality of life |
References
- Dunning, K.; LeMasters, G.; Levin, L.; Bhattacharya, A.; Alterman, T.; Lordo, K. Falls in workers during pregnancy: Risk factors, job hazards, and high risk occupations. Am. J. Ind. Med. 2003, 44, 664–672. [Google Scholar] [CrossRef] [PubMed]
- Fast, A.; Shapiro, D.; Ducommun, E.J.; Friedmann, L.W.; Bouklas, T.; Floman, Y. Low-back pain in pregnancy. Spine 1987, 12, 368–371. [Google Scholar] [CrossRef] [PubMed]
- Dehghan, F.; Haerian, B.S.; Muniandy, S.; Yusof, A.; Dragoo, J.L.; Salleh, N. The effect of relaxin on the musculoskeletal system. Scand. J. Med. Sci. Sports 2014, 24, e220–e229. [Google Scholar] [CrossRef] [PubMed]
- Yoo, H.; Shin, D.; Song, C. Changes in the spinal curvature, degree of pain, balance ability, and gait ability according to pregnancy period in pregnant and nonpregnant women. J. Phys. Ther. Sci. 2015, 27, 279–284. [Google Scholar] [CrossRef] [PubMed]
- Gilleard, W.L.; Crosbie, J.; Smith, R. Static trunk posture in sitting and standing during pregnancy and early postpartum. Arch. Phys. Med. Rehabil. 2002, 83, 1739–1744. [Google Scholar] [CrossRef] [PubMed]
- Butler, E.E.; Colón, I.; Druzin, M.L.; Rose, J. Postural equilibrium during pregnancy: Decreased stability with an increased reliance on visual cues. Am. J. Obstet. Gynecol. 2006, 195, 1104–1108. [Google Scholar] [CrossRef]
- Mei, Q.; Gu, Y.; Fernandez, J. Alterations of Pregnant Gait during Pregnancy and Post-Partum. Sci. Rep. 2018, 8, 2217. [Google Scholar] [CrossRef]
- Tapp, L.M. Pregnancy & ergonomics. Prof. Saf. 2000, 45, 4. [Google Scholar]
- Bertuit, J.; Leyh, C.; Rooze, M.; Feipel, F. Pregnancy-related changes in centre of pressure during gait. Acta Bioeng. Biomech. 2017, 19. [Google Scholar]
- Kristiansson, P.; Svärdsudd, K.; von Schoultz, B. Serum relaxin, symphyseal pain, and back pain during pregnancy. Am. J. Obstet. Gynecol. 1996, 175, 1342–1347. [Google Scholar] [CrossRef]
- Kristiansson, P.; Svärdsudd, K.; von Schoultz, B. Back pain during pregnancy: A prospective study. Spine 1996, 21, 702–708. [Google Scholar] [CrossRef] [PubMed]
- Goulet, L.; Thériault, G. Association between spontaneous abortion and ergonomic factors: A literature review of the epidemiologic evidence. Scand. J. Work Environ. Health 1987, 399–403. [Google Scholar] [CrossRef] [PubMed]
- Inanir, A.; Cakmak, B.; Hisim, Y.; Demirturk, F. Evaluation of postural equilibrium and fall risk during pregnancy. Gait Posture 2014, 39, 1122–1125. [Google Scholar] [CrossRef] [PubMed]
- Karasek, R.; Brisson, C.; Kawakami, N.; Houtman, I.; Bongers, P.; Amick, B. The Job Content Questionnaire (JCQ): An instrument for internationally comparative assessments of psychosocial job characteristics. J. Occup. Health Psychol. 1998, 3, 322. [Google Scholar] [CrossRef] [PubMed]
- Rezaei, E.; Moghadam, Z.B.; Saraylu, K. Quality of life in pregnant women with sleep disorder. J. Fam. Reprod. Health 2013, 7, 87. [Google Scholar]
- Mens, J.M.; Damen, L.; Snijders, C.J.; Stam, H.J. The mechanical effect of a pelvic belt in patients with pregnancy-related pelvic pain. Clin. Biomech. 2006, 21, 122–127. [Google Scholar] [CrossRef]
- Dananberg, H.J.; Guiliano, M. Chronic low-back pain and its response to custom-made foot orthoses. J. Am. Podiatr. Med. Assoc. 1999, 89, 109–117. [Google Scholar] [CrossRef]
- Ostgaard, H.; Andersson, G.; Schultz, A.; Miller, J. Influence of some biomechanical factors on low-back pain in pregnancy. Spine 1993, 18, 61–65. [Google Scholar] [CrossRef]
- Morrissey, S.J. Work place design recommendations for the pregnant worker. Int. J. Ind. Ergon. 1998, 21, 383–395. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The, P.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Franklin, M.E.; Conner-Kerr, T. An analysis of posture and back pain in the first and third trimesters of pregnancy. J. Orthop. Sports Phys. Ther. 1998, 28, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Bullock, J.E.; Jull, G.A.; Bullock, M.I. The relationship of low back pain to postural changes during pregnancy. Aust. J. Physiother. 1987, 33, 10–17. [Google Scholar] [CrossRef]
- Dumas, G.; Reid, J.; Wolfe, L.; Griffin, M.; McGrath, M. Exercise, posture, and back pain during pregnancy: Part 1. Exercise and posture. Clin. Biomech. 1995, 10, 98–103. [Google Scholar] [CrossRef]
- Moore, K.; Dumas, G.; Reid, J. Postural changes associated with pregnancy and their relationship with low-back pain. Clin. Biomech. 1990, 5, 169–174. [Google Scholar] [CrossRef]
- Betsch, M.; Wehrle, R.; Dor, L.; Rapp, W.; Jungbluth, P.; Hakimi, M.; Wild, M. Spinal posture and pelvic position during pregnancy: A prospective rasterstereographic pilot study. Eur. Spine J. 2015, 24, 1282–1288. [Google Scholar] [CrossRef]
- Glinkowski, W.M.; Tomasik, P.; Walesiak, K.; Głuszak, M.; Krawczak, K.; Michoński, J.; Czyżewska, A.; Żukowska, A.; Sitnik, R.; Wielgoś, M. Posture and low back pain during pregnancy—3D study. Ginekol. Pol. 2016, 87, 575–580. [Google Scholar] [CrossRef]
- Schröder, G.; Kundt, G.; Otte, M.; Wendig, D.; Schober, H.-C. Impact of pregnancy on back pain and body posture in women. J. Phys. Ther. Sci. 2016, 28, 1199–1207. [Google Scholar] [CrossRef]
- McCrory, J.L.; Chambers, A.J.; Daftary, A.; Redfern, M.S. The pregnant “waddle”: An evaluation of torso kinematics in pregnancy. J. Biomech. 2014, 47, 2964–2968. [Google Scholar] [CrossRef]
- Krkeljas, Z. Changes in gait and posture as factors of dynamic stability during walking in pregnancy. Hum. Mov. Sci. 2018, 58, 315–320. [Google Scholar] [CrossRef]
- Gilleard, W.L.; Brown, J.M.M. Structure and function of the abdominal muscles in primigravid subjects during pregnancy and the immediate postbirth period. Phys. Ther. 1996, 76, 750–762. [Google Scholar] [CrossRef]
- Preece, S.J.; Willan, P.; Nester, C.J.; Graham-Smith, P.; Herrington, L.; Bowker, P. Variation in pelvic morphology may prevent the identification of anterior pelvic tilt. J. Man. Manip. Ther. 2008, 16, 113–117. [Google Scholar] [CrossRef] [PubMed]
- Maratt, J.D.; Esposito, C.I.; McLawhorn, A.S.; Jerabek, S.A.; Padgett, D.E.; Mayman, D.J. Pelvic tilt in patients undergoing total hip arthroplasty: When does it matter? J. Arthroplast. 2015, 30, 387–391. [Google Scholar] [CrossRef] [PubMed]
- Ranawat, C.S.; Ranawat, A.S.; Lipman, J.D.; White, P.B.; Meftah, M. Effect of spinal deformity on pelvic orientation from standing to sitting position. J. Arthroplast. 2016, 31, 1222–1227. [Google Scholar] [CrossRef] [PubMed]
- Nicholls, J.; Grieve, D. Posture, performance and discomfort in pregnancy. Appl. Ergon. 1992, 23, 128–132. [Google Scholar] [CrossRef]
- Okanishi, N.; Kito, N.; Akiyama, M.; Yamamoto, M. Spinal curvature and characteristics of postural change in pregnant women. Acta Obstet. Et Gynecol. Scand. 2012, 91, 856–861. [Google Scholar] [CrossRef] [PubMed]
- Nichols, J.A.; Bednar, M.S.; Havey, R.M.; Murray, W.M. Decoupling the wrist: A cadaveric experiment examining wrist kinematics following midcarpal fusion and scaphoid excision. J. Appl. Biomech. 2017, 33, 12–23. [Google Scholar] [CrossRef] [Green Version]
- Paul, J.A.; Frings-Dresen, M.H. Standing working posture compared in pregnant and non-pregnant conditions. Ergonomics 1994, 37, 1563–1575. [Google Scholar] [CrossRef]
- Lee, Y.-H.; Her, L.-L.; Tsuang, Y.-H. A comparison of sitting posture adaptations of pregnant and non-pregnant females. Int. J. Ind. Ergon. 1999, 23, 391–396. [Google Scholar] [CrossRef]
- Biviá-Roig, G.; Lisón, J.F.; Sánchez-Zuriaga, D. Effects of pregnancy on lumbar motion patterns and muscle responses. Spine J. 2019, 19, 364–371. [Google Scholar] [CrossRef]
- Gilleard, W.; Crosbie, J.; Smith, R. Effect of pregnancy on trunk range of motion when sitting and standing. Acta Obstet. Gynecol. Scand. 2002, 81, 1011–1020. [Google Scholar] [CrossRef]
- Paul, J.; Salle, H.; Frings-Dresen, M. Effect of posture on hip joint moment during pregnancy, while performing a standing task. Clin. Biomech. 1996, 11, 111–115. [Google Scholar] [CrossRef]
- Sunaga, Y.; Kanemura, N.; Anan, M.; Takahashi, M.; Shinkoda, K. Estimation of inertial parameters of the lower trunk in pregnant Japanese women: A longitudinal comparative study and application to motion analysis. Appl. Ergon. 2016, 55, 173–182. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, L.F.; Vieira, T.M.M.; Macedo, A.R.; Simpson, D.M.; Nadal, J. Postural sway changes during pregnancy: A descriptive study using stabilometry. Eur. J. Obstet. Gynecol. Reprod. Biol. 2009, 147, 25–28. [Google Scholar] [CrossRef] [PubMed]
- McCrory, J.L.; Chambers, A.J.; Daftary, A.; Redfern, M.S. Dynamic postural stability during advancing pregnancy. J. Biomech. 2010, 43, 2434–2439. [Google Scholar] [CrossRef] [PubMed]
- Nagai, M.; Isida, M.; Saitoh, J.; Hirata, Y.; Natori, H.; Wada, M. Characteristics of the control of standing posture during pregnancy. Neurosci. Lett. 2009, 462, 130–134. [Google Scholar] [CrossRef]
- Opala-Berdzik, A.; Błaszczyk, J.W.; Bacik, B.; Cieślińska-Świder, J.; Świder, D.; Sobota, G.; Markiewicz, A. Static Postural Stability in Women during and after Pregnancy: A Prospective Longitudinal Study. PLoS ONE 2015, 10, e0124207. [Google Scholar] [CrossRef]
- Jang, J.; Hsiao, K.T.; Hsiao-Wecksler, E.T. Balance (perceived and actual) and preferred stance width during pregnancy. Clin. Biomech. 2008, 23, 468–476. [Google Scholar] [CrossRef]
- Öztürk, G.; Geler Külcü, D.; Aydoğ, E.; Kaspar, Ç.; Uğurel, B. Effects of lower back pain on postural equilibrium and fall risk during the third trimester of pregnancy. J. Matern. -Fetal Neonatal Med. 2016, 29, 1358–1362. [Google Scholar]
- Takeda, K.; Yoshikata, H.; Imura, M. Changes in posture control of women that fall during pregnancy. Int. J. Womens Health Reprod. Sci. 2018, 6, 255–262. [Google Scholar] [CrossRef] [Green Version]
- Ersal, T.; McCrory, J.L.; Sienko, K.H. Theoretical and experimental indicators of falls during pregnancy as assessed by postural perturbations. Gait Posture 2014, 39, 218–223. [Google Scholar] [CrossRef]
- Kerbourc’h, F.; Bertuit, J.; Feipel, V.; Rooze, M. Pregnancy and Pelvic Girdle Pain. J. Am. Podiatr. Med Assoc. 2017, 107, 299–306. [Google Scholar] [CrossRef] [PubMed]
- Akrami, M.; Qian, Z.; Zou, Z.; Howard, D.; Nester, C.J.; Ren, L. Subject-specific finite element modelling of the human foot complex during walking: Sensitivity analysis of material properties, boundary and loading conditions. Biomech. Modeling Mechanobiol. 2018, 17, 559–576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sunaga, Y.; Anan, M.; Shinkoda, K. Biomechanics of rising from a chair and walking in pregnant women. Appl. Ergon. 2013, 44, 792–798. [Google Scholar] [CrossRef] [PubMed]
- Richards, J.G. The measurement of human motion: A comparison of commercially available systems. Hum. Mov. Sci. 1999, 18, 589–602. [Google Scholar] [CrossRef]
- Sagawa, Y.; Turcot, K.; Armand, S.; Thevenon, A.; Vuillerme, N.; Watelain, E. Biomechanics and physiological parameters during gait in lower-limb amputees: A systematic review. Gait Posture 2011, 33, 511–526. [Google Scholar] [CrossRef]
- Błaszczyk, J.W.; Opala-Berdzik, A.; Plewa, M. Adaptive changes in spatiotemporal gait characteristics in women during pregnancy. Gait Posture 2016, 43, 160–164. [Google Scholar] [CrossRef]
- Gilleard, W.L. Trunk motion and gait characteristics of pregnant women when walking: Report of a longitudinal study with a control group. BMC Pregnancy Childbirth 2013, 13, 71. [Google Scholar] [CrossRef] [Green Version]
- Bertuit, J.; Feipel, V.; Rooze, M. Temporal and spatial parameters of gait during pregnancy. Acta Bioeng. Biomech. 2015, 17, 93–101. [Google Scholar]
- Aguiar, L.; Santos-Rocha, R.; Vieira, F.; Branco, M.; Andrade, C.; Veloso, A. Comparison between overweight due to pregnancy and due to added weight to simulate body mass distribution in pregnancy. Gait Posture 2015, 42, 511–517. [Google Scholar] [CrossRef] [Green Version]
- Forczek, W.; Staszkiewicz, R. Changes of kinematic gait parameters due to pregnancy. Acta Bioeng. Biomech. 2012, 14, 113–119. [Google Scholar]
- Sawa, R.; Doi, T.; Asai, T.; Watanabe, K.; Taniguchi, T.; Ono, R. Differences in trunk control between early and late pregnancy during gait. Gait Posture 2015, 42, 455–459. [Google Scholar] [CrossRef] [Green Version]
- Branco, M.A.; Santos-Rocha, R.; Vieira, F.; Aguiar, R.; Veloso, A.P. Three-dimensional kinematic adaptations of gait throughout pregnancy and post-partum. Acta Bioeng. Biomech. 2016, 18, 153–162. [Google Scholar]
- Branco, M.; Santos-Rocha, R.; Aguiar, L.; Vieira, F.; Veloso, A. Kinematic Analysis of Gait in the Second and Third Trimesters of Pregnancy. J. Pregnancy 2013, 2013, 718095. [Google Scholar] [CrossRef]
- Wu, W.H.; Meijer, O.G.; Bruijn, S.M.; Hu, H.; van Dieën, J.H.; Lamoth, C.J.C.; van Royen, B.J.; Beek, P.J. Gait in Pregnancy-related Pelvic girdle Pain: Amplitudes, timing, and coordination of horizontal trunk rotations. Eur. Spine J. 2008, 17, 1160–1169. [Google Scholar] [CrossRef] [Green Version]
- Wu, W.; Meijer, O.G.; Lamoth, C.J.C.; Uegaki, K.; van Dieën, J.H.; Wuisman, P.I.J.M.; de Vries, J.I.P.; Beek, P.J. Gait coordination in pregnancy: Transverse pelvic and thoracic rotations and their relative phase. Clin. Biomech. 2004, 19, 480–488. [Google Scholar] [CrossRef]
- Branco, M.; Santos-Rocha, R.; Vieira, F.; Silva, M.-R.; Aguiar, L.; Veloso, A.P. Influence of Body Composition on Gait Kinetics throughout Pregnancy and Postpartum Period. Scientifica 2016, 2016, 12. [Google Scholar] [CrossRef] [Green Version]
- Swärd Aminoff, A.; Agnvall, C.; Todd, C.; Jónasson, P.; Sansone, M.; Thoreson, O.; Swärd, L.; Karlsson, J.; Baranto, A. The effect of pelvic tilt and cam on hip range of motion in young elite skiers and nonathletes. Open Access J. Sports Med. 2018, 9, 147–156. [Google Scholar] [CrossRef] [Green Version]
- Levinger, P.; Menz, H.B.; Morrow, A.D.; Bartlett, J.R.; Feller, J.A.; Bergman, N.R. Relationship between foot function and medial knee joint loading in people with medial compartment knee osteoarthritis. J. Foot Ankle Res. 2013, 6, 33. [Google Scholar] [CrossRef] [Green Version]
- Chou, P.-H.; Yao, P.-L.; Chou, Y.-L.; Hone, J.-N.; Lin, T.-S. Biomechanical analysis of chair rising in the pregnant women. Biomed. Eng. Appl. Basis Commun. 2003, 15, 157–159. [Google Scholar] [CrossRef] [Green Version]
- Gilleard, W.; Crosbie, J.; Smith, R. A longitudinal study of the effect of pregnancy on rising to stand from a chair. J. Biomech. 2008, 41, 779–787. [Google Scholar] [CrossRef] [Green Version]
- Lou, S.-Z.; Chou, Y.-L.; Chou, P.-H.; Lin, C.-J.; Chen, U.-C.; Su, F.-C. Sit-to-stand at different periods of pregnancy. Clin. Biomech. 2001, 16, 194–198. [Google Scholar] [CrossRef]
- Akrami, M.; Craig, K.; Dibaj, M.; Javadi, A.A.; Benattayallah, A. A three-dimensional finite element analysis of the human hip. J. Med Eng. Technol. 2018, 42, 546–552. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, A.P.; João, S.M.A.; Sacco, I.C.N. Static and Dynamic Biomechanical Adaptations of the Lower Limbs and Gait Pattern Changes during Pregnancy. Women’s Health 2013, 9, 99–108. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.H.; Meijer, O.G.; Uegaki, K.; Mens, J.M.A.; van Dieën, J.H.; Wuisman, P.I.J.M.; Östgaard, H.C. Pregnancy-related pelvic girdle pain (PPP), I: Terminology, clinical presentation, and prevalence. Eur. Spine J. 2004, 13, 575–589. [Google Scholar] [CrossRef] [PubMed]
- Tanigawa, A.; Morino, S.; Aoyama, T.; Takahashi, M. Gait analysis of pregnant patients with lumbopelvic pain using inertial sensor. Gait Posture 2018, 65, 176–181. [Google Scholar] [CrossRef]
- Gijon-Nogueron, G.A.; Gavilan-Diaz, M.; Valle-Funes, V.; Jimenez-Cebrian, A.M.; Cervera-Marin, J.A.; Morales-Asencio, J.M. Anthropometric Foot Changes During Pregnancy. J. Am. Podiatr. Med Assoc. 2013, 103, 314–321. [Google Scholar] [CrossRef]
- Vico Pardo, F.J.; López del Amo, A.; Pardo Rios, M.; Gijon-Nogueron, G.; Yuste, C.C. Changes in foot posture during pregnancy and their relation with musculoskeletal pain: A longitudinal cohort study. Women Birth 2018, 31, e84–e88. [Google Scholar] [CrossRef]
- Pita-Fernandez, S.; Gonzalez-Martin, C.; Alonso-Tajes, F.; Seoane-Pillado, T.; Pertega-Diaz, S.; Perez-Garcia, S.; Seijo-Bestilleiro, R.; Balboa-Barreiro, V. Flat Foot in a Random Population and its Impact on Quality of Life and Functionality. J. Clin. Diagn Res. 2017, 11, LC22–LC27. [Google Scholar] [CrossRef]
- Dumas, G.; Reid, J.; Wolfe, L.; Griffin, M.; McGrath, M. Exercise, posture, and back pain during pregnancy: Part 2. Exercise and back pain. Clin. Biomech. 1995, 10, 104–109. [Google Scholar] [CrossRef]

{kind=link}
| Cardiovascular: 29 | Workplace: 4 | Kidneys/Renal Function: 24 | Cervical Changes: 29 | Road Safety: 9 |
|---|---|---|---|---|
| Blood pressure: 24 | Pre-eclampsia: 2 | Pregnancy behaviours: 11 | Treatments: 13 | Exercise effects: 14 |
| Animal models: 37 | Labor: 6 | Stability of proteins: 24 | Bipolar disorder: 1 | Genetic stability: 4 |
| Social stability: 18 | Skin biomechanics: 5 | Effects on fetus: 12 | No paper found: 7 | Diet: 8 |
| Ground reaction forces: 7 | Corneal related: 14 | Postural orthostatic tachycardia syndrome: 10 | Diabetes: 3 | Tumour stability: 1 |
| Reliability of pain classification system: 1 | Erythrocyte membrane stability: 1 | Bacterial stability: 1 | Respiratory system: 5 | Edema: 1 |
| Seizures: 1 | Mental stability: 6 | Brain injuries: 1 | Hormone stability: 9 | Circadian rhythm: 1 |
| Ankylosing spondylitis: 2 | Chronic hypoxia: 1 | Injury: 2 | Achilles reflex: 1 | Pelvic insufficiency: 3 |
| Musculoskeletal disorders: 1 | Measurement methods: 11 | Pelvic organ prolapse: 1 | Scoliosis: 1 | Geographic analysis: 2 |
| Osteoporosis: 1 | Betamimetic effects: 1 | Bone formation: 1 | HIV: 1 | Treating infertility: 1 |
| Uterus: 2 | Bladder function: 3 | Hyperemesis gravidarum: 1 | Magnetic field: 1 | Vestibular system: 1 |
| Neuralgia: 1 | Postpartum pain: 3 | Bone mineral density: 1 | Foot changes: 1 | Oculomotor: 1 |
| Reference | Title | Year | Participants | Objectives |
|---|---|---|---|---|
| [22] | The relationship of low back pain to postural changes during pregnancy | 1987 | 34 P | spinal curvature |
| [24] | Postural changes associated with pregnancy and their relationship with low-back pain | 1990 | 30 P | spinal curvature |
| [34] | Posture, performance and discomfort in pregnancy | 1992 | 12 P + 12 NP | sitting posture |
| [37] | Standing working posture compared in pregnant and non-pregnant conditions | 1994 | 27 P + 10 NP | standing posture |
| [23,79] | Exercise, posture, and back pain during pregnancy | 1995 | 65 P | spinal curvature |
| [41] | Effect of posture on hip joint moment during pregnancy, while performing a standing task | 1996 | 16 P | hip joint moment |
| [21] | An analysis of posture and back pain in the first and third trimesters of pregnancy | 1998 | 12 P | spinal curvature, torso kinematics |
| [38] | A comparison of sitting posture adaptations of pregnant and non-pregnant females | 1999 | 5 P + 5 NP | sitting posture |
| [71] | Sit-to-stand at different periods of pregnancy | 2001 | 24 P | kinematics of chair rising |
| [5] | Static trunk posture in sitting and standing during pregnancy and early post partum | 2002 | 9 P + 12 NP | sitting and standing posture |
| [40] | Effect of pregnancy on trunk range of motion when sitting and standing | 2002 | 9 P + 12 NP | trunk kinematics |
| [64] | Gait in pregnancy-related pelvic pain: amplitudes, timing, and coordination of horizontal trunk rotations | 2008 | 24 P | trunk and lower limb kinematics and spatiotemporal gait kinematics |
| [69] | Biomechanical analysis of chair rising in the pregnant woman | 2003 | 30 P | kinematics of chair rising |
| [65] | Gait coordination in pregnancy: transverse pelvic and thoracic rotations and their relative phase | 2004 | 12 P + 13 NP | trunk kinematics during gait |
| [6] | Postural equilibrium during pregnancy: decreased stability with an increased reliance on visual cues | 2006 | 12 P + 12 NP | static posture and COP |
| [47] | Balance (perceived and actual) and preferred stance width during pregnancy. | 2008 | 15 P + 15 NP | COP and balance |
| [70] | A longitudinal study of the effect of pregnancy on rising to stand from a chair | 2008 | 9 P + 12 NP | kinematics of chair rising |
| [43] | Postural sway changes during pregnancy: A descriptive study using stabilometry | 2009 | 20 P | static sway changes and COP |
| [45] | Characteristics of the control of standing posture during pregnancy | 2009 | 35 P + 8 NP | static sway changes |
| [44] | Dynamic postural stability during advancing pregnancy | 2010 | 41 P + 40 NP | sway changes and COP |
| [44] | Spinal curvature and characteristics of postural change in pregnant women | 2012 | 15 P + 10 NP | posture - spinal curvature |
| [44] | Changes of kinematic gait parameters due to pregnancy | 2012 | 13 P | Spatiotemporal gait parameters |
| [53] | Biomechanics of rising from a chair and walking in pregnant women | 2013 | 12 P + 10 NP | kinematics of chair rising |
| [63] | Kinematic analysis of gait in the second and third trimesters of pregnancy | 2013 | 22 P + 12 NP | joint kinematics during gait |
| [57] | Trunk motion and gait characteristics of pregnant women when walking: report of longitudinal study with a control group | 2013 | 9 P | trunk kinematics during gait |
| [76] | Anthropometric foot changes during pregnancy: a pilot study | 2013 | 10 P | foot parameters |
| [13] | Evaluation of postural equilibrium and fall risk during pregnancy | 2014 | 80 P + 30 NP | dynamic posture |
| [28] | The pregnant “waddle”: An evaluation of torso kinematics in pregnancy | 2014 | 41 P + 40 NP | torso kinematics during gait |
| [50] | Theoretical and experimental indicators of falls during pregnancy as assessed by postural perturbations | 2014 | 14 P + 40 NP | static stability and COP |
| [25] | Spinal posture and pelvic position during pregnancy: a prospective rasterographic pilot study | 2015 | 13 P + 20 NP | spinal curvature and pelvic/ trunk tilt |
| [61] | Differences in trunk control between early and late pregnancy during gait | 2015 | 27 P | control of trunk during gait |
| [46] | Static postural stability in women during and after pregnancy: A prospective longitudinal study | 2015 | 45 P | static stability and COP |
| [58] | Temporal and spatial parameters of gait during pregnancy | 2015 | 58 P + 23 NP + 9 PP | Spatiotemporal gait parameters |
| [4] | Changes in the spinal curvature, degree of pain, balance ability, and gait ability according to pregnancy period in pregnant and nonpregnant women | 2015 | 34 P + 15 NP | spinal curvature, balance, spatiotemporal gait parameters, torso kinematics |
| [59] | Comparison between overweight due to pregnancy and due to added weight to stimulate body mass distribution in pregnancy | 2015 | 18 P + 18 NP | Spatiotemporal gait parameters and joint kinematics |
| [56] | Adaptive changes in spatiotemporal gait characteristics in women during pregnancy | 2016 | 28 P | Spatiotemporal gait parameters |
| [27] | Impact of pregnancy on back pain and body posture in pregnant women | 2016 | 26 P | spinal curvature |
| [26] | Posture and low back pain during pregnancy - 3D study | 2016 | 65 P | spinal curvature |
| [62] | Three-dimensional kinematic adaptations of gait throughout pregnancy and post-partum | 2016 | 11 P | lower limb kinematics |
| [42] | Estimation of inertial parameters of the lower trunk in pregnant Japanese women: A longitudinal comparative study and application to motion analysis | 2016 | 8 P + 7 NP | trunk kinematics |
| [48] | Effects of lower back pain on postural equilibrium and fall risk during the third trimester of pregnancy | 2016 | 68 P | static stability |
| [66] | Influence of body composition on gait kinetics throughout pregnancy and postpartum period | 2016 | 11 P | Anthropometric changes and joint kinematics |
| [9] | Pregnancy-related changes in center of pressure during gait | 2017 | 58 P + 23 NP + 9 PP | dynamic sway changes and COP |
| [51] | Pregnancy and pelvic girdle pain: analysis of centre of pressure during gait | 2017 | 127 P + 22 NP | dynamic stability and COP |
| [39] | Effects of pregnancy on lumbar motion patterns and muscle responses | 2018 | 34 P + 34 NP | lumbar motion |
| [7] | Alterations of pregnant gait during pregnancy and post-partum | 2018 | 16 P | gait kinematics and COP |
| [29] | Changes in gait and posture as factors of dynamic stability during walking in pregnancy | 2018 | 35 P | trunk kinematics and COP |
| [49] | Changes in posture control of women that fall during pregnancy | 2018 | 100 P | Static stability |
| [75] | Gait analysis of pregnant patients with lumbopelvic pain using inertial sensor | 2018 | 52 P | trunk kinematics during gait |
| [77] | Changes in foot posture during pregnancy and their relation with musculoskeletal pain: A longitudinal cohort study | 2018 | 62 P | foot parameters |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Conder, R.; Zamani, R.; Akrami, M. The Biomechanics of Pregnancy: A Systematic Review. J. Funct. Morphol. Kinesiol. 2019, 4, 72. https://doi.org/10.3390/jfmk4040072
Conder R, Zamani R, Akrami M. The Biomechanics of Pregnancy: A Systematic Review. Journal of Functional Morphology and Kinesiology. 2019; 4(4):72. https://doi.org/10.3390/jfmk4040072
Chicago/Turabian StyleConder, Rebecca, Reza Zamani, and Mohammad Akrami. 2019. "The Biomechanics of Pregnancy: A Systematic Review" Journal of Functional Morphology and Kinesiology 4, no. 4: 72. https://doi.org/10.3390/jfmk4040072
APA StyleConder, R., Zamani, R., & Akrami, M. (2019). The Biomechanics of Pregnancy: A Systematic Review. Journal of Functional Morphology and Kinesiology, 4(4), 72. https://doi.org/10.3390/jfmk4040072