Elastics Selector Gauge as Orthodontics Device Applied to Inter-Maxillary Traction during Malocclusion Correction

 ,
,  ,
,  and
and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
3. Results
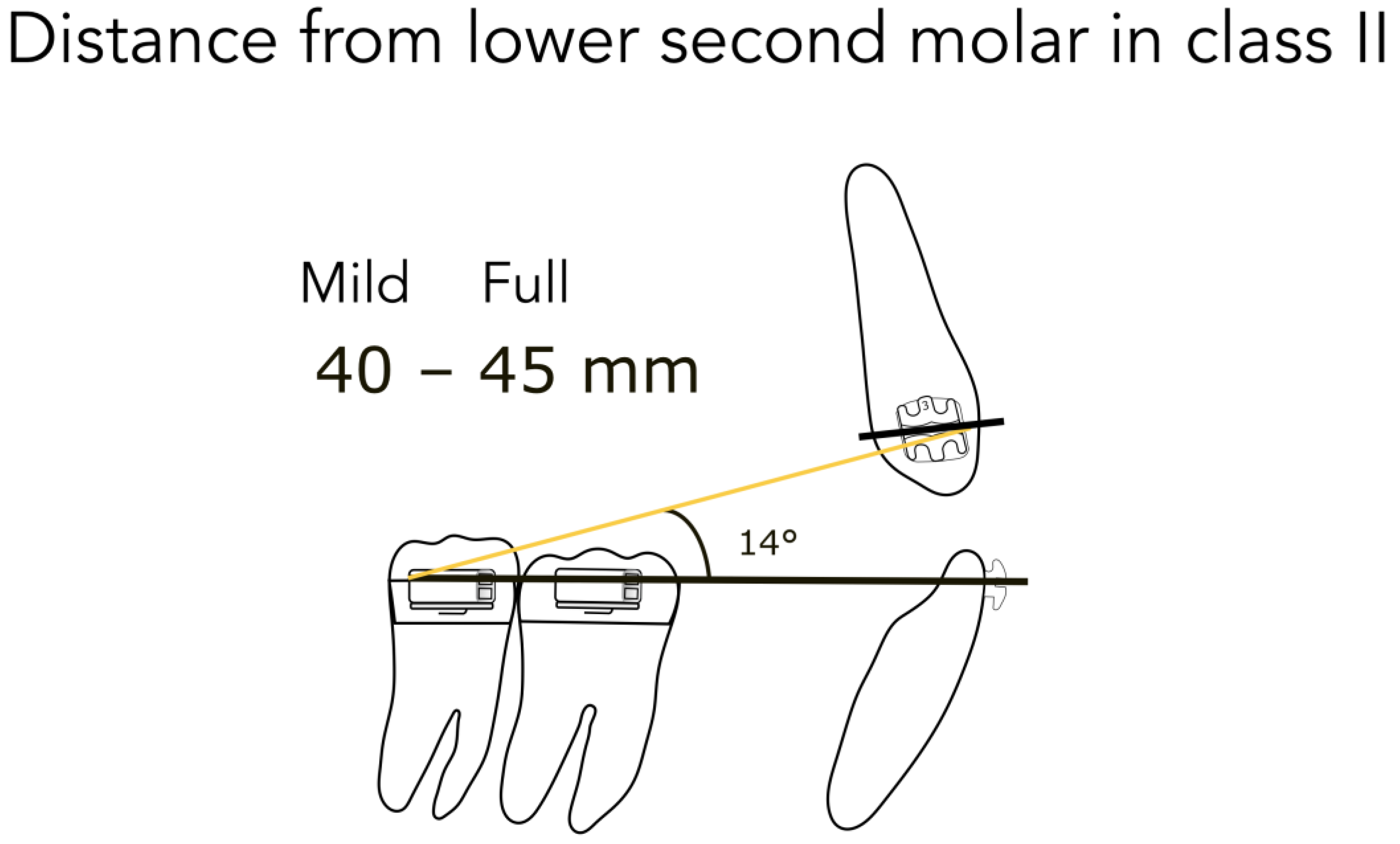
- 45 mm from the lower second molar in full Class II (Figure 4)
- 40 mm from the lower second molar in mild Class II (Figure 4)
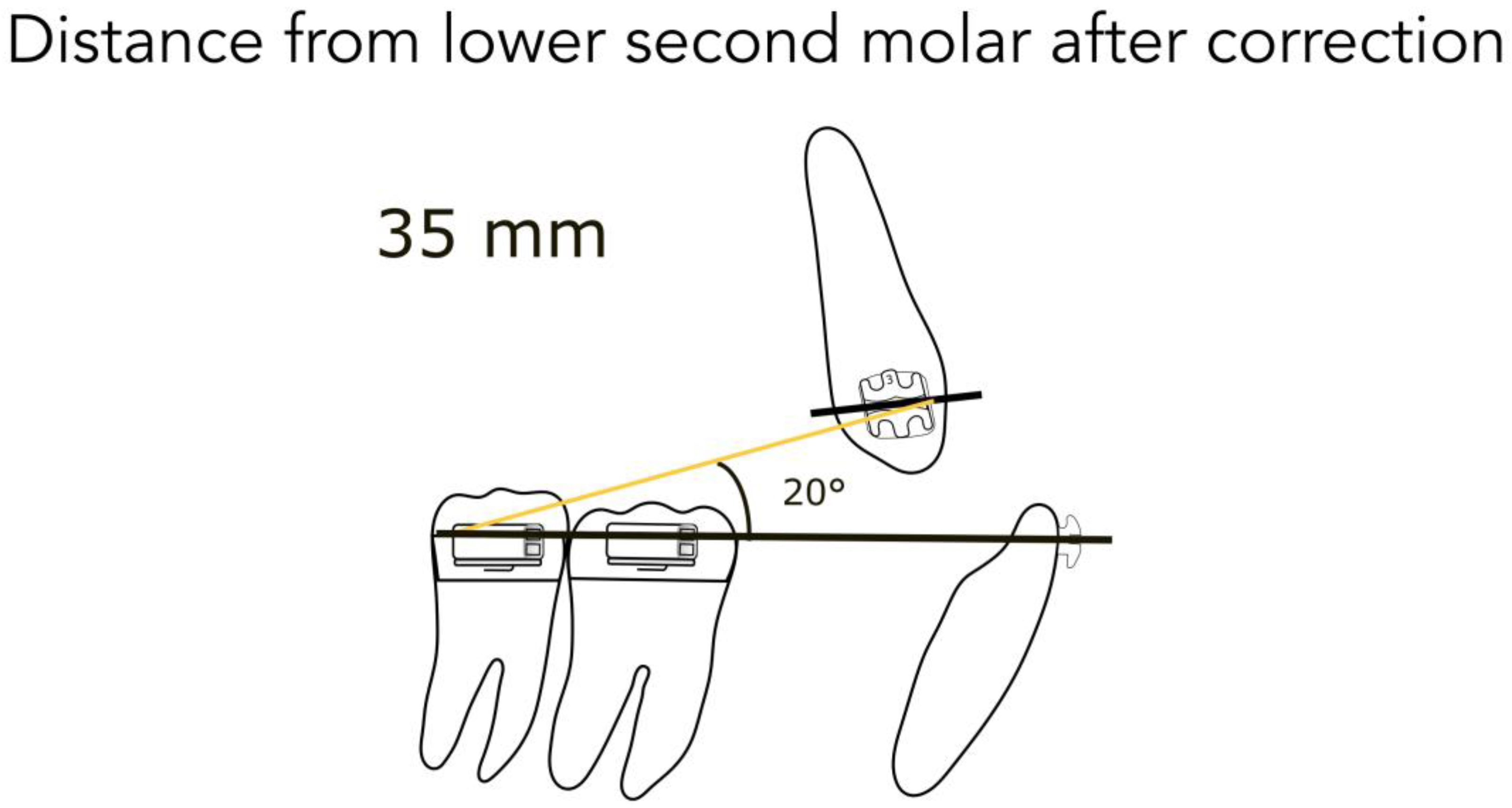
- 35 mm from the lower second molar after correction (Figure 5)
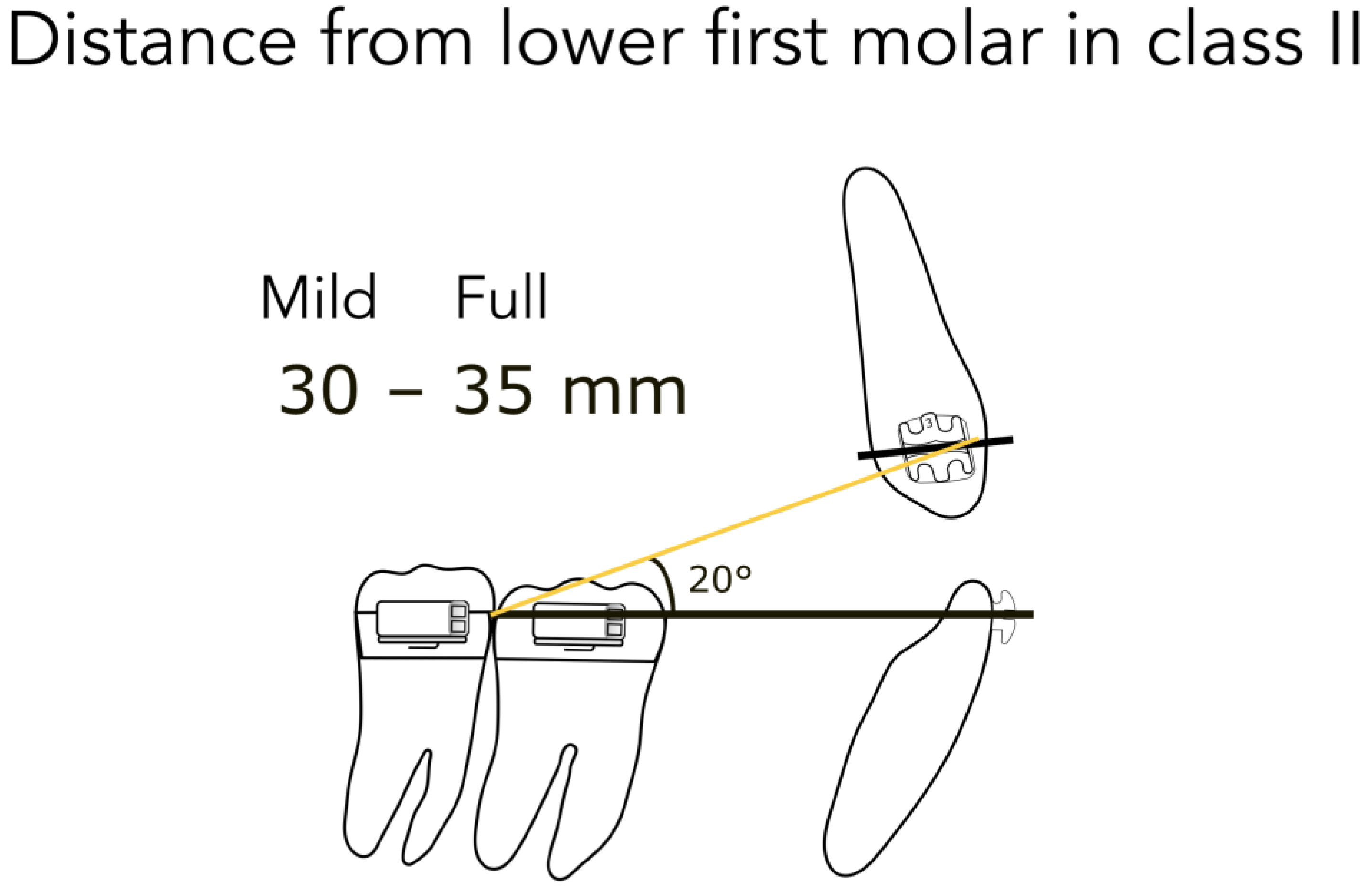
- 35 mm from the lower first molar in full Class II (Figure 6)
- 30 mm from the lower first molar in mild Class II (Figure 6)
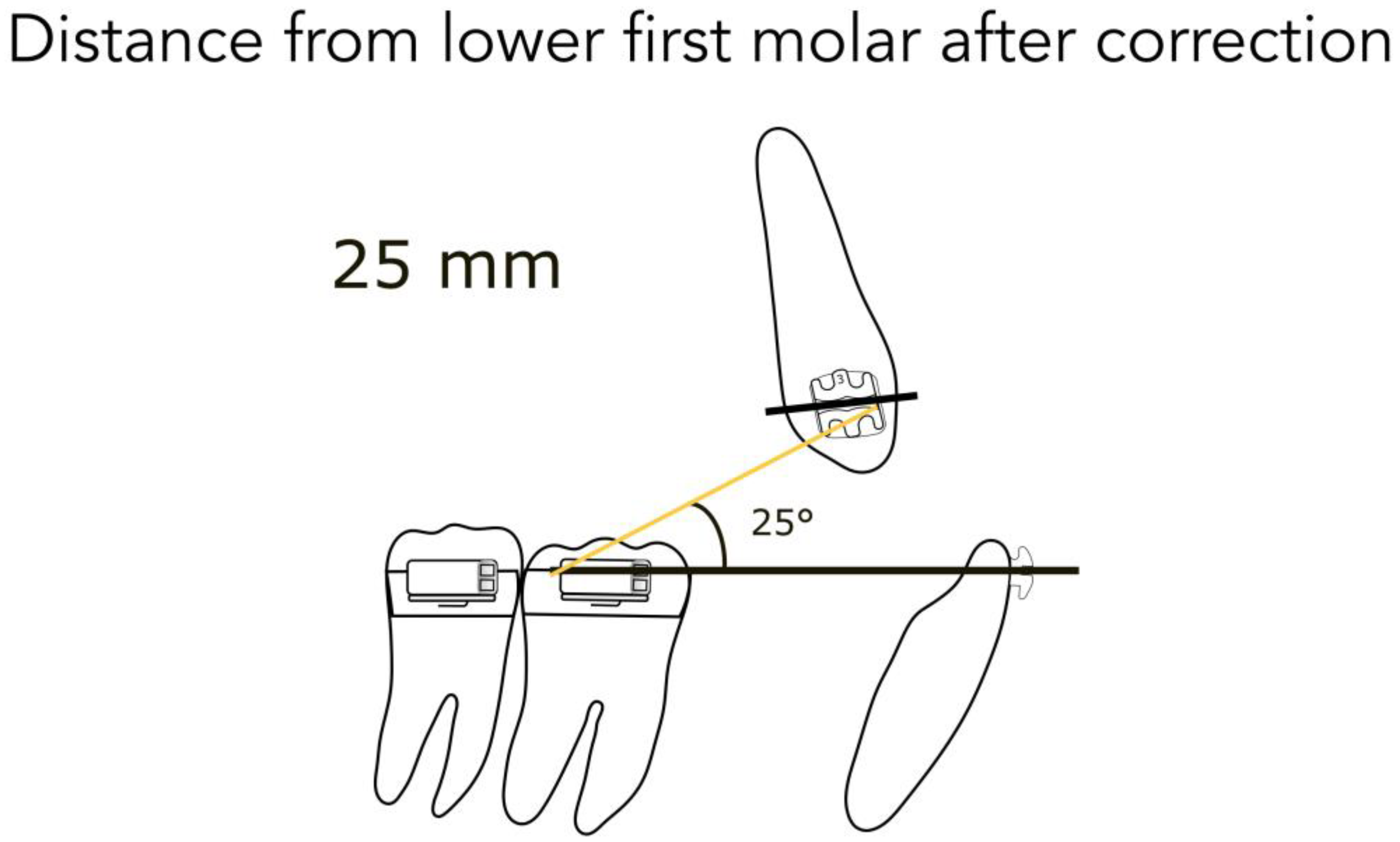
- 25 mm from the lower first molar after correction (Figure 7)
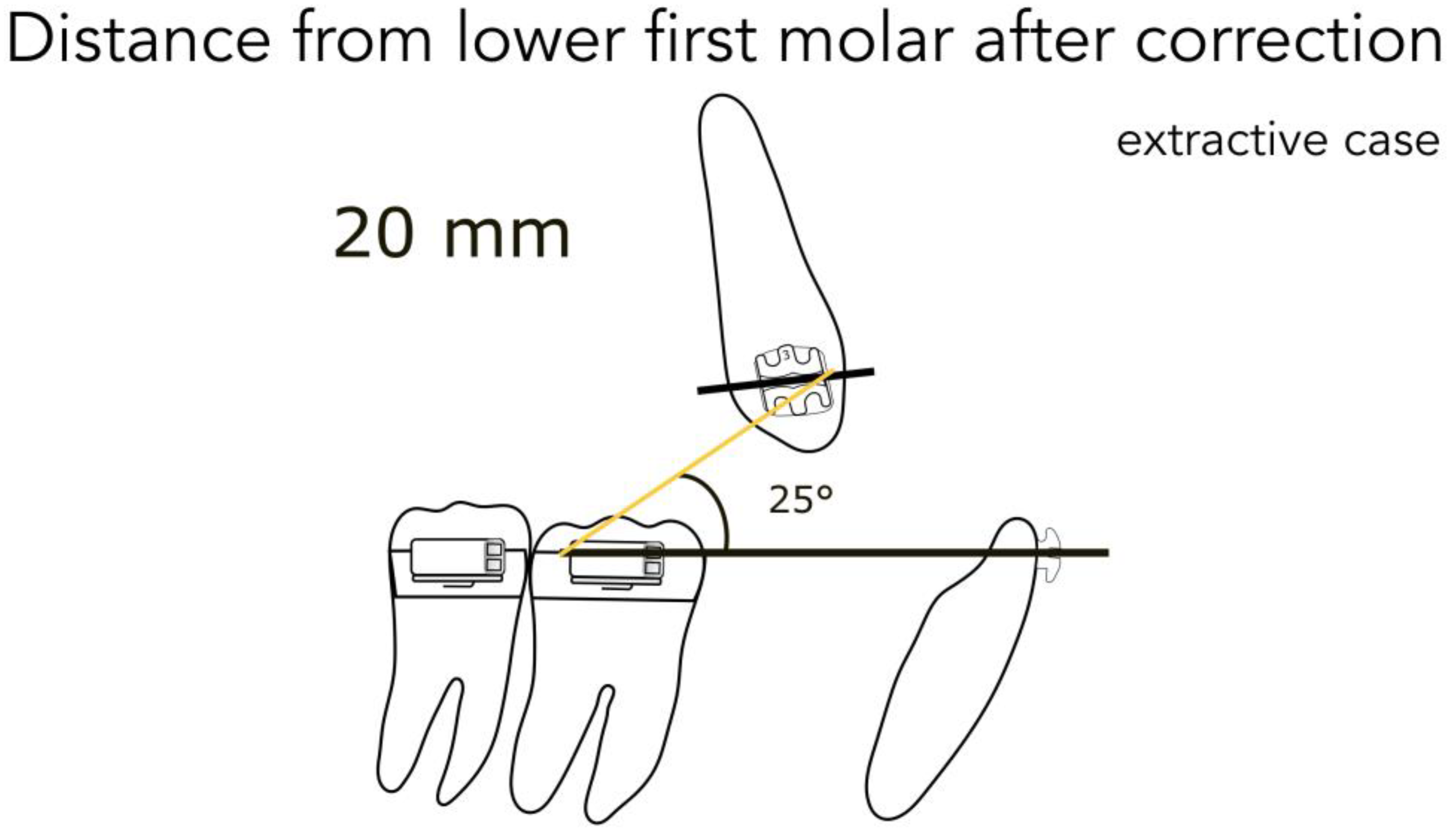
- 20 mm from the lower first molar in extractive cases (Figure 8)
4. Discussion
5. Conclusions
6. Patents
Author Contributions
Funding
Conflicts of Interest
References
- Asbell, M.B. A brief history of orthodontics. Am. J. Orthod. Dentofac. Orthop. 1990, 98, 176–183. [Google Scholar] [CrossRef]
- Eh, A. Malocclusion of the Teeth, 7th ed.; White Dental Manufacturing Company: Lakewood, NJ, USA, 1907. [Google Scholar]
- Bench, R.G.; Gugino, C.F.; Hilgers, J.J. Bioprogressive Therapy part 6—Forces used in Bioprogressive Therapy. J. Clin. Orthod. 1978, 12, 123–139. [Google Scholar] [PubMed]
- Burstone, C.J.; Baldwin, J.J.; Lawless, D.T. The Application of Continuous Forces to Orthodontics. Angle Orthod. 1961, 31, 1–14. [Google Scholar]
- Lee, B. Relationship between tooth movement rate and estimated pressure applied. J. Dent. Res. 1965, 44, 1053. [Google Scholar] [CrossRef] [PubMed]
- Miura, F. Effect of orthodontic force on blood circula- tion in the periodontal membrane. In Transactions of the Third International Orthodontic Congress; Crosby Lockwood Staples: London, UK, 1973; pp. 35–41. [Google Scholar]
- Ricketts, R.M. Bioprogressive therapy as an answer to orthodontic needs Part II. Am. J. Orthod. 1976, 70, 359–397. [Google Scholar] [CrossRef]
- Ricketts, R.M. Bioprogressive therapy as an answer to orthodontic needs Part I. Am. J. Orthod. 1976, 70, 241–268. [Google Scholar] [CrossRef]
- Ricketts, R.M. Bioprogressive Therapy, Book One; Rocky Mountain Orthodontics: Denver, CO, USA, 1979; Volume 1, p. 367. [Google Scholar]
- Ricketts, R.M. Concepet of Mechanics and Biomechanics; American Institute for Bioprogressive Education: Scottsdale, AZ, USA, 1998. [Google Scholar]
- Storey, E.S. Force in orthodontics and its relation to tooth movement. Aust. J. Dent. 1952, 56, 11–18. [Google Scholar]
- Ricketts, R.M. Laminagraphy in the diagnosis of temporomandibular joint disorders. J. Am. Dent. Assoc. 1953, 46, 620–648. [Google Scholar] [CrossRef]
- Sambataro, S.; Fastuca, R.; Oppermann, N.J.; Lorusso, P.; Baccetti, T.; Franchi, L.; Caprioglio, A. Cephalometric changes in growing patients with increased vertical dimension treated with cervical headgear. J. Orofac. Orthop. 2017, 78, 312–320. [Google Scholar] [CrossRef]
- Huang, C.S.; Hsu, S.S.; Chen, Y.R. Systematic review of the surgery-first approach in orthognathic surgery. Biomed. J. 2014, 37, 184–190. [Google Scholar] [CrossRef]
- Proffit, W.R.; White, R.P., Jr. Who needs surgical-orthodontic treatment? Int. J. Adult Orthod. Orthognath Surg. 1990, 5, 81–89. [Google Scholar]
- Hammoudeh, J.A.; Howell, L.K.; Boutros, S.; Scott, M.A.; Urata, M.M. Current Status of Surgical Planning for Orthognathic Surgery: Traditional Methods versus 3D Surgical Planning. Plast. Reconstr. Surg. Glob. Open 2015, 3, e307. [Google Scholar] [CrossRef]
- Cicciu, M.; Cervino, G.; Herford, A.S.; Fama, F.; Bramanti, E.; Fiorillo, L.; Lauritano, F.; Sambataro, S.; Troiano, G.; Laino, L. Facial Bone Reconstruction Using both Marine or Non-Marine Bone Substitutes: Evaluation of Current Outcomes in a Systematic Literature Review. Mar. Drugs 2018, 16, 27. [Google Scholar] [CrossRef]
- Cervino, G.; Fiorillo, L.; Monte, I.P.; De Stefano, R.; Laino, L.; Crimi, S.; Bianchi, A.; Herford, A.S.; Biondi, A.; Cicciu, M. Advances in Antiplatelet Therapy for Dentofacial Surgery Patients: Focus on Past and Present Strategies. Materials 2019, 12, 1524. [Google Scholar] [CrossRef]
- Laino, L.; Cicciu, M.; Fiorillo, L.; Crimi, S.; Bianchi, A.; Amoroso, G.; Monte, I.P.; Herford, A.S.; Cervino, G. Surgical Risk on Patients with Coagulopathies: Guidelines on Hemophiliac Patients for Oro-Maxillofacial Surgery. Int. J. Environ. Res. Public Health 2019, 16, 1386. [Google Scholar] [CrossRef]
- Lombardi, T.; Bernardello, F.; Berton, F.; Porrelli, D.; Rapani, A.; Camurri Piloni, A.; Fiorillo, L.; Di Lenarda, R.; Stacchi, C. Efficacy of Alveolar Ridge Preservation after Maxillary Molar Extraction in Reducing Crestal Bone Resorption and Sinus Pneumatization: A Multicenter Prospective Case-Control Study. Biomed. Res. Int. 2018, 2018, 9352130. [Google Scholar] [CrossRef]
- Sato, S.A.; Matsumoto, A.; Shirasu, A.; Yoshida, J. Manual for the Clinical Application of the MEAW Tecnique: Orthodontic Theraphy Using Multiloop Edgewise Archwire; Meaw Publishing House: Yokosuka, Kanagawa, Japan, 2001. [Google Scholar]
- Sato, S. A Treatment Approach to Malocclusion under the Considerations of Craniofacial Dynamics; Meaw Publishing House: Yokosuka, Kanagawa, Japan, 1991. [Google Scholar]
- Fiorillo, L. Chlorhexidine Gel Use in the Oral District: A Systematic Review. Gels 2019, 5, 31. [Google Scholar] [CrossRef]
- Fiorillo, L.; Cervino, G.; Herford, A.S.; Lauritano, F.; D’Amico, C.; Lo Giudice, R.; Laino, L.; Troiano, G.; Crimi, S.; Cicciu, M. Interferon Crevicular Fluid Profile and Correlation with Periodontal Disease and Wound Healing: A Systemic Review of Recent Data. Int. J. Mol. Sci. 2018, 19, 1908. [Google Scholar] [CrossRef]
- Troiano, G.; Laino, L.; Cicciu, M.; Cervino, G.; Fiorillo, L.; D’Amico, C.; Zhurakivska, K.; Lo Muzio, L. Comparison of Two Routes of Administration of Dexamethasone to Reduce the Postoperative Sequelae After Third Molar Surgery: A Systematic Review and Meta-Analysis. Open Dent. J. 2018, 12, 181–188. [Google Scholar] [CrossRef]
- Cervino, G.; Terranova, A.; Briguglio, F.; De Stefano, R.; Fama, F.; D’Amico, C.; Amoroso, G.; Marino, S.; Gorassini, F.; Mastroieni, R.; et al. Diabetes: Oral Health Related Quality of Life and Oral Alterations. Biomed. Res. Int. 2019, 2019, 5907195. [Google Scholar] [CrossRef]
- Cervino, G.; Fiorillo, L.; Laino, L.; Herford, A.S.; Lauritano, F.; Giudice, G.L.; Fama, F.; Santoro, R.; Troiano, G.; Iannello, G.; et al. Oral Health Impact Profile in Celiac Patients: Analysis of Recent Findings in a Literature Review. Gastroenterol. Res. Pract. 2018, 2018, 7848735. [Google Scholar] [CrossRef]
- Sambataro, S.; Cervino, G.; Fiorillo, L.; Cicciu, M. Upper First Premolar Positioning Evaluation for the Stability of the Dental Occlusion: Anatomical Considerations. J. Craniofac. Surg. 2018, 29, 1366–1369. [Google Scholar] [CrossRef]
- Sambataro, S.; Bocchieri, S.; Cervino, G.; La Bruna, R.; Cicciù, A.; Innorta, M.; Torrisi, B.; Cicciù, M. Correlations between Malocclusion and Postural Anomalies in Children with Mixed Dentition. J. Funct. Morphol. Kinesiol. 2019, 4, 45. [Google Scholar] [CrossRef]
- Ricketts, R.M. The Widsom of Sectional Mechanics; American Institute for Bioprogressive Education: Scottsdale, AZ, USA, 1998. [Google Scholar]
- Proffit, W.; Fields, H. Contemporary Orthodontics, 5th ed.; Elsevier: Amsterdam, The Netherlands, 2013. [Google Scholar]
- Janson, G.; Sathler, R.; Fernandes, T.M.; Branco, N.C.; Freitas, M.R. Correction of Class II malocclusion with Class II elastics: A systematic review. Am. J. Orthod. Dentofac. Orthop. 2013, 143, 383–392. [Google Scholar] [CrossRef]
- Mizrahi, E. The Use of Miniscrews in Orthodontics: A Review of Selected Clinical Applications. Prim. Dent. J. 2016, 5, 20–27. [Google Scholar]
- Beattie, S.; Monaghan, P. An in vitro study simulating effects of daily diet and patient elastic band change compliance on orthodontic latex elastics. Angle Orthod. 2004, 74, 234–239. [Google Scholar]
- Gioka, C.; Zinelis, S.; Eliades, T.; Eliades, G. Orthodontic latex elastics: A force relaxation study. Angle Orthod. 2006, 76, 475–479. [Google Scholar]
- Kamisetty, S.K.; Nimagadda, C.; Begam, M.P.; Nalamotu, R.; Srivastav, T.; Gs, S. Elasticity in Elastics-An in-vitro study. J. Int. Oral. Health 2014, 6, 96–105. [Google Scholar]
- Russell, K.A.; Milne, A.D.; Khanna, R.A.; Lee, J.M. In vitro assessment of the mechanical properties of latex and non-latex orthodontic elastics. Am. J. Orthod. Dentofac. Orthop. 2001, 120, 36–44. [Google Scholar] [CrossRef]
- Seibt, S.; Salmoria, I.; Cericato, G.O.; Paranhos, L.R.; Rosario, H.D.; El Haje, O. Comparative analysis of force degradation of latex orthodontic elastics of 5/16’’ diameter: An in vitro study. Minerva Stomatol. 2016, 65, 284–290. [Google Scholar]
- Kanchana, P.; Godfrey, K. Calibration of force extension and force degradation characteristics of orthodontic latex elastics. Am. J. Orthod. Dentofac. Orthop. 2000, 118, 280–287. [Google Scholar] [CrossRef]
- Liu, C.C.; Wataha, J.C.; Craig, R.G. The effect of repeated stretching on the force decay and compliance of vulcanized cis-polyisoprene orthodontic elastics. Dent. Mater. 1993, 9, 37–40. [Google Scholar] [CrossRef]
- Wang, T.; Zhou, G.; Tan, X.; Dong, Y. Evaluation of force degradation characteristics of orthodontic latex elastics in vitro and in vivo. Angle Orthod. 2007, 77, 688–693. [Google Scholar] [CrossRef]











© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sambataro, S.; Bocchieri, S.; Bafumi, L.; Fiorillo, L.; Cervino, G.; Cicciù, M. Elastics Selector Gauge as Orthodontics Device Applied to Inter-Maxillary Traction during Malocclusion Correction. J. Funct. Morphol. Kinesiol. 2019, 4, 63. https://doi.org/10.3390/jfmk4030063
Sambataro S, Bocchieri S, Bafumi L, Fiorillo L, Cervino G, Cicciù M. Elastics Selector Gauge as Orthodontics Device Applied to Inter-Maxillary Traction during Malocclusion Correction. Journal of Functional Morphology and Kinesiology. 2019; 4(3):63. https://doi.org/10.3390/jfmk4030063
Chicago/Turabian StyleSambataro, Sergio, Salvatore Bocchieri, Luigi Bafumi, Luca Fiorillo, Gabriele Cervino, and Marco Cicciù. 2019. "Elastics Selector Gauge as Orthodontics Device Applied to Inter-Maxillary Traction during Malocclusion Correction" Journal of Functional Morphology and Kinesiology 4, no. 3: 63. https://doi.org/10.3390/jfmk4030063
APA StyleSambataro, S., Bocchieri, S., Bafumi, L., Fiorillo, L., Cervino, G., & Cicciù, M. (2019). Elastics Selector Gauge as Orthodontics Device Applied to Inter-Maxillary Traction during Malocclusion Correction. Journal of Functional Morphology and Kinesiology, 4(3), 63. https://doi.org/10.3390/jfmk4030063