Drive for Thinness Predicts Musculoskeletal Injuries in Division II NCAA Female Athletes

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Data Collection
2.2.1. General Health Assessment
2.2.2. Drive for Thinness
2.2.3. Injuries
2.2.4. Data Analysis
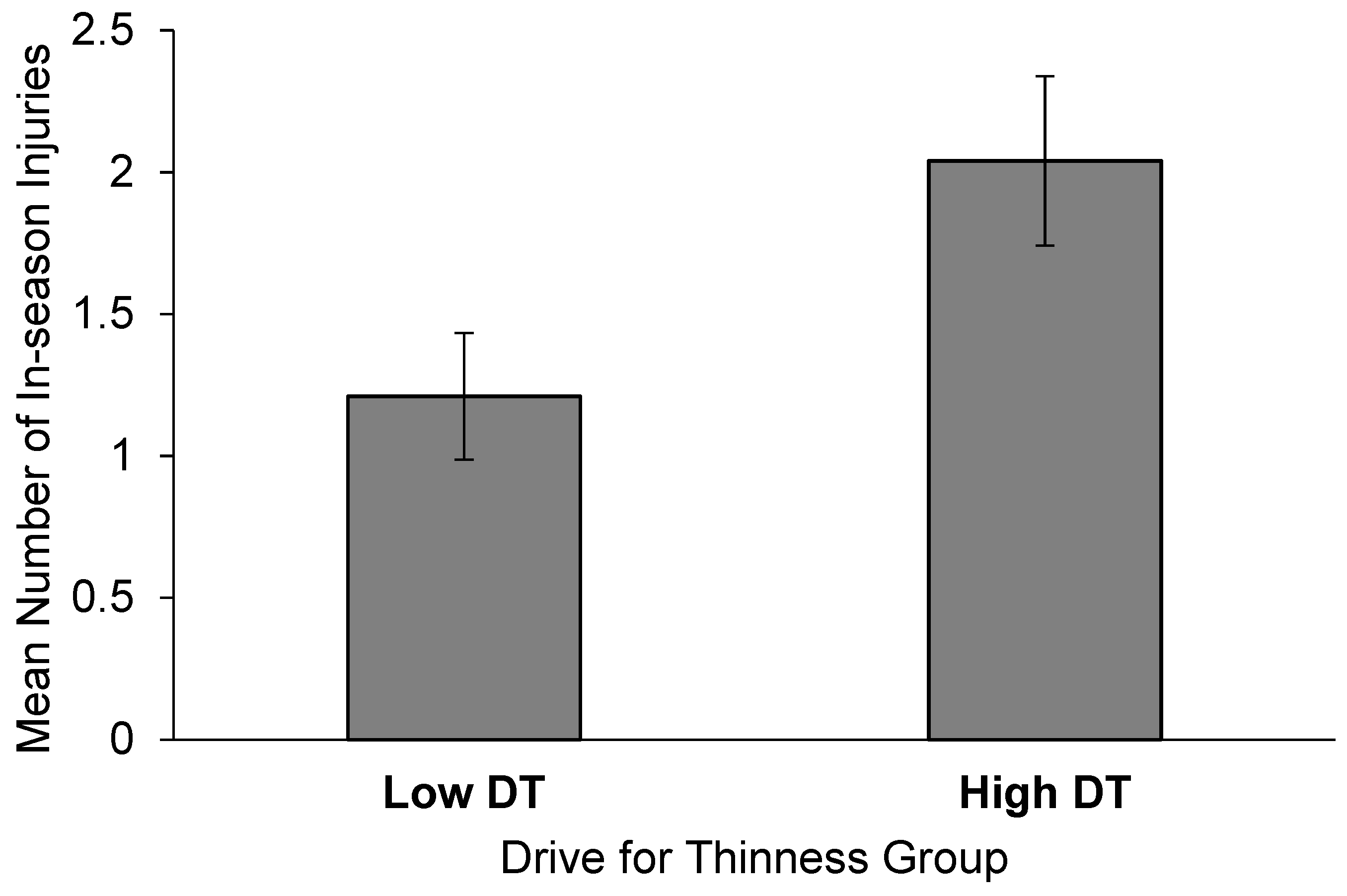
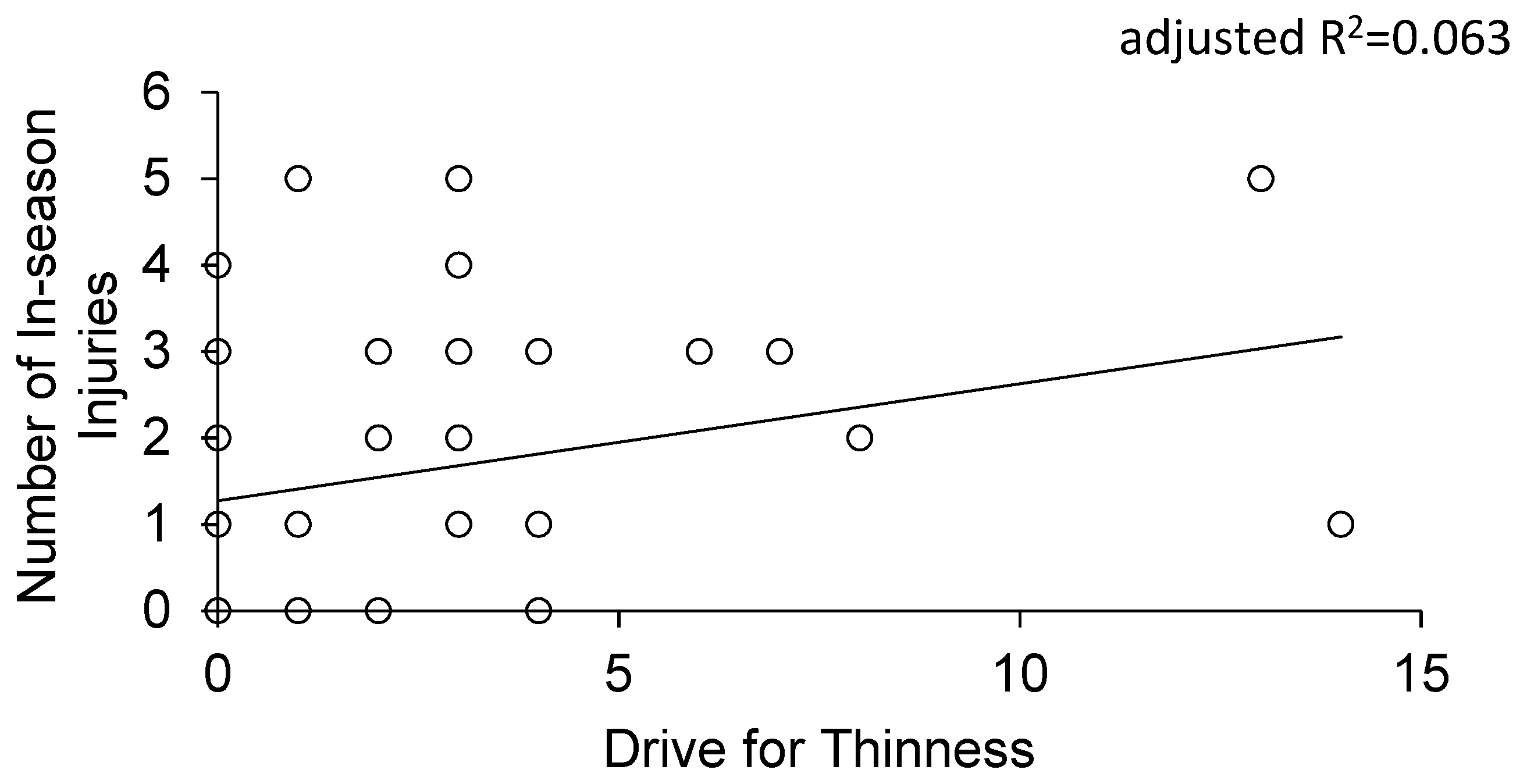
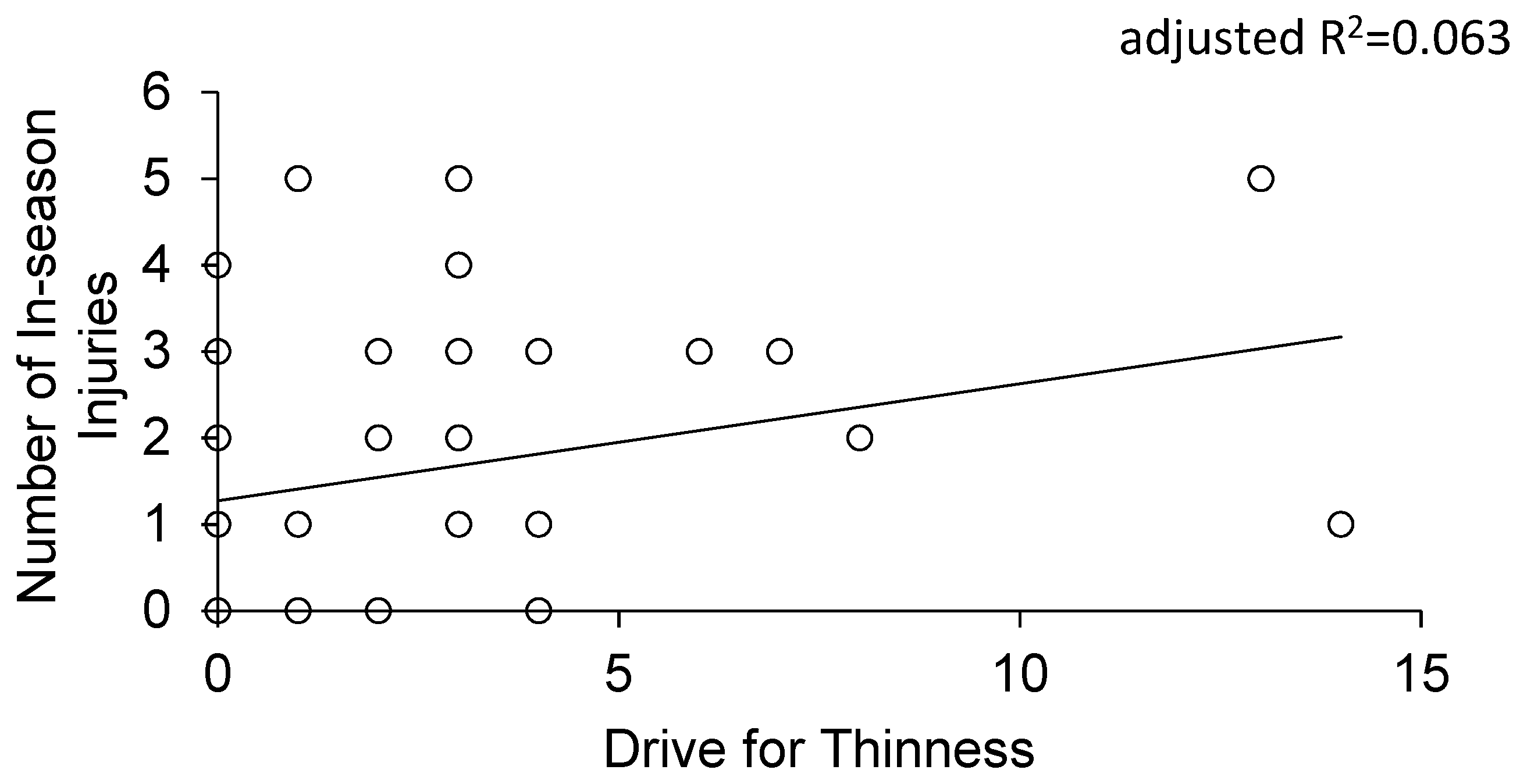
3. Results
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Baker, E.R.; Mathur, R.S.; Kirk, R.F.; Williamson, H.O. Female runners and secondary amenorrhea: Correlation with age, parity, mileage, and plasma hormonal and sex-hormone-binding globulin concentrations. Fertil. Steril. 1981, 36, 183–187. [Google Scholar] [CrossRef]
- Dale, E.; Gerlach, D.H.; Wilhite, A.L. Wilhite menstrual dysfunction in distance runners. Obstet. Gynecol. 1979, 54, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Otis, C.L.; Drinkwater, B.; Johnson, M.; Loucks, A.; Wilmore, J. ACSM position stand: The female athlete triad. Med. Sci. Sports Exerc. 1997, 29, i–ix. [Google Scholar] [CrossRef] [PubMed]
- Loveless, M.B. Female athlete triad. Curr. Opin. Obstet. Gynecol. 2017, 29, 301–305. [Google Scholar] [CrossRef] [PubMed]
- Nattiv, A.; Loucks, A.B.; Manore, M.M.; Sanborn, C.F.; Sundgot-Borgen, J.; Warren, M.P.; American College of Sports Medicine. American college of sports medicine position stand. The female athlete triad. Med. Sci. Sports Exerc. 2007, 39, 1867. [Google Scholar]
- Gibbs, J.C.; Williams, N.I.; De Souza, M.J. Prevalence of Individual and combined components of the female athlete triad. Med. Sci. Sports Exerc. 2013, 45, 985–996. [Google Scholar] [CrossRef]
- Beals, K.A.; Manore, M.M. Disorders of the female athlete triad among collegiate athletes. Int. J. Sport Nutr. Exerc. Metab. 2002, 12, 281. [Google Scholar] [CrossRef]
- Tenforde, A.S.; Sayres, L.C.; McCurdy, M.L.; Sainani, K.L.; Fredericson, M. Identifying sex-specific risk factors for stress fractures in adolescent runners. Med. Sci. Sports Exerc. 2013, 45, 1843–1851. [Google Scholar] [CrossRef]
- Rauh, M.J.; Nichols, J.F.; Barrack, M.T. Relationships among injury and disordered eating, menstrual dysfunction, and low bone mineral density in high school athletes: A prospective study. J. Athl. Train. 2010, 45, 243–252. [Google Scholar] [CrossRef]
- Rauh, M.J.; Barrack, M.T.; Nichols, J.F. Associations between the female athlete triad and injury among high school runners. Int. J. Sports Phys. Ther. 2014, 9, 948–958. [Google Scholar]
- Gibbs, J.C.; Williams, N.I.; Scheid, J.L.; Toombs, R.J.; De Souza, M.J. The association of a high drive for thinness with energy deficiency and severe menstrual disturbances: Confirmation in a large population of exercising women. Int. J. Sport Nutr. Exerc. Metab. 2011, 21, 280–290. [Google Scholar] [CrossRef]
- Garner, D.M.; Olmsted, M.P. Eating Disorder Inventory Manual; Psychological Assessment Resources: Odessa, FL, USA, 1991. [Google Scholar]
- Nyman-Carlsson, E.; Engström, I.; Norring, C.; Nevonen, L. Eating disorder inventory-3, validation in Swedish patients with eating disorders, psychiatric outpatients and a normal control sample. Nord. J. Psychiatry 2015, 69, 142–151. [Google Scholar] [CrossRef]
- De Souza, M.J.; Hontscharuk, R.; Olmsted, M.; Kerr, G.; Williams, N.I. Drive for thinness score is a proxy indicator of energy deficiency in exercising women. Appetite 2007, 48, 359–367. [Google Scholar] [CrossRef]
- De Souza, M.J.; Nattiv, A.; Joy, E.; Misra, M.; Williams, N.I.; Mallinson, R.J.; Gibbs, J.C.; Olmsted, M.; Goolsby, M.; Matheson, G.; et al. 2014 Female athlete triad coalition consensus statement on treatment and return to play of the female athlete triad: 1st international conference held in San Francisco, California, May 2012 and 2nd international conference held in Indianapolis, Indiana, May 2013. Br. J. Sports Med. 2014, 48, 289. [Google Scholar]
- Tenforde, A.S.; Carlson, J.L.; Chang, A.; Sainani, K.L.; Shultz, R.; Kim, J.H.; Cutti, P.; Golden, N.H.; Fredericson, M. Association of the female athlete triad risk assessment stratification to the development of bone stress injuries in collegiate athletes. Am. J. Sports Med. 2017, 45, 302–310. [Google Scholar] [CrossRef]
- Loucks, A.B. Low energy availability in the marathon and other endurance sports. Sports Med. 2007, 37, 348–352. [Google Scholar] [CrossRef]
- Bullen, B.A.; Skrinar, G.S.; Beitins, I.Z.; von Mering, G.; Turnbull, B.A.; McArthur, J.W. Induction of menstrual disorders by strenuous exercise in untrained women. N. Engl. J. Med. 1985, 312, 1349–1353. [Google Scholar] [CrossRef]
- Williams, N.I.; Helmreich, D.L.; Parfitt, D.B.; Caston-Balderrama, A.; Cameron, J.L. Evidence for a causal role of low energy availability in the induction of menstrual cycle disturbances during strenuous exercise training. J. Clin. Endocrinol. Metab. 2001, 86, 5184–5193. [Google Scholar] [CrossRef]
- Syed-Abdul, M.; Soni, D.; Wagganer, J. Impact of a professional nutrition program on a female cross country collegiate athlete: A case report. Sports 2018, 6, 82. [Google Scholar] [CrossRef]
- De Souza, M.J.; West, S.L.; Jamal, S.A.; Hawker, G.A.; Gundberg, C.M.; Williams, N.I. The presence of both an energy deficiency and estrogen deficiency exacerbate alterations of bone metabolism in exercising women. Bone 2008, 43, 140–148. [Google Scholar] [CrossRef]
- Haberland, C.A.; Seddick, D.; Marcus, R.; Bachrach, L.K. A physician survey of therapy for exercise-associated amenorrhea: A brief report. Clin. J. Sport Med. 1995, 5, 246–250. [Google Scholar] [CrossRef]
- Hulme, A.; Nielsen, R.O.; Timpka, T.; Verhagen, E.; Finch, C. Risk and protective factors for middle- and long-distance running-related injury. Sports Med. 2017, 47, 869–886. [Google Scholar] [CrossRef]
- Torstveit, M.K. Participation in leanness sports but not training volume is associated with menstrual dysfunction: A national survey of 1276 elite athletes and controls. Br. J. Sports Med. 2005, 39, 141–147. [Google Scholar] [CrossRef]
- Schaumberg, M.A.; Emmerton, L.M.; Jenkins, D.G.; Burton, N.W.; Janse de Jonge, X.A.K.; Skinner, T.L. Use of oral contraceptives to manipulate menstruation in young, physically active women. Int. J. Sports Physiol. Perform. 2018, 13, 82–87. [Google Scholar] [CrossRef]
- Daniels, K.; Daugherty, J.; Jones, J. Current Contraceptive Status Among Women Aged 15–44: United States, 2011–2013; National Center for Health Statistics: Hyattsville, MD, USA, 2014.

{kind=link}
{kind=link}
| Low DT (n = 33) | High DT (n = 24) | |
|---|---|---|
| Body dissatisfaction | 1.7 ± 0.4 | 5.8 ± 0.8 * |
| Interoceptive awareness | 1.4 ± 0.4 | 2.0 ± 0.4 |
| Drive for thinness | 0.3 ± 0.1 | 4.5 ± 0.6 * |
| Bulimia | 1.9 ± 1.2 | 1.6 ± 0.4 |
| Ineffectiveness | 0.9 ± 0.4 | 1.6 ± 0.5 |
| Interpersonal distrust | 1.6 ± 0.3 | 1.9 ± 0.6 |
| Perfectionism | 5.9 ± 0.5 | 9.6 ± 0.7 * |
| Maturity fears | 2.9 ± 0.4 | 5.4 ± 0.9 |
| Sum | 14.4 ± 2.1 | 30.8 ± 3.8 * |
| Low DT (n = 33) | High DT (n = 24) | |
|---|---|---|
| Age (yr) | 19.0 ± 0.2 | 19.1 ± 0.9 |
| Height (m) | 1.65 ± 0.02 | 1.68 ± 0.02 |
| Weight (kg) | 60.7 ± 1.5 | 64.0 ± 1.8 |
| Body Mass Index (kg/m2) | 22.2 ± 0.3 | 22.6 ± 0.5 |
| Team Training Per Week (hours) | 14.0 ± 0.9 | 13.2 ± 1.4 |
| Non-Team Training Per Week (hours) | 2.4 ± 0.3 | 3.2 ± 0.2 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scheid, J.L.; Stefanik, M.E. Drive for Thinness Predicts Musculoskeletal Injuries in Division II NCAA Female Athletes. J. Funct. Morphol. Kinesiol. 2019, 4, 52. https://doi.org/10.3390/jfmk4030052
Scheid JL, Stefanik ME. Drive for Thinness Predicts Musculoskeletal Injuries in Division II NCAA Female Athletes. Journal of Functional Morphology and Kinesiology. 2019; 4(3):52. https://doi.org/10.3390/jfmk4030052
Chicago/Turabian StyleScheid, Jennifer L., and Morgan E. Stefanik. 2019. "Drive for Thinness Predicts Musculoskeletal Injuries in Division II NCAA Female Athletes" Journal of Functional Morphology and Kinesiology 4, no. 3: 52. https://doi.org/10.3390/jfmk4030052
APA StyleScheid, J. L., & Stefanik, M. E. (2019). Drive for Thinness Predicts Musculoskeletal Injuries in Division II NCAA Female Athletes. Journal of Functional Morphology and Kinesiology, 4(3), 52. https://doi.org/10.3390/jfmk4030052