Abstract
Different types of orthoses are available to clinicians for non-surgical treatment of acute ankle sprains. The goal of this study was to scientifically compare the movement restrictions in the sagittal and frontal plane during simulated walking between one adaptable semi-rigid brace (OrthoTri-PhaseTM), four non-adaptable semi-rigid braces (OrthoStandardTM, MalleoLocTM, MalleoSprintTM, VACOankleTM), and one rigid cast. Predefined time sequences of rotational moments and axial loading during gait were applied via an ankle joint simulator, with the pneumatic pressure inside the orthoses kept constant to ensure the same condition for different trials and orthoses. The peak ranges of motion (RoMs) in the frontal and sagittal plane during gait were analyzed for statistically significant differences using single-factorial ANOVA with post-hoc Bonferroni analysis. Significant differences in peak plantar-/dorsiflexion and in-/eversion RoM during gait were found between different types of orthoses. In the sagittal plane, the rigid cast most significantly restricted overall RoM followed by the Ortho Tri-PhaseTM in Phase 1 and the Ortho StandardTM. The peak restriction in-/eversion RoM of the VACOankleTM came closest to the rigid cast, with a shift towards inversion. The VACOankleTM allowed for significantly larger dorsiflexion movement compared to all other orthoses. The present results may help clinicians in the decision-making process of finding the optimal orthosis for individual patients.
1. Introduction
Acute ankle sprains represent 40% of all sports injuries [1], especially associated with stop-and-go activities such as basketball, volleyball, and soccer [2]. According to Harrasser et al. (2016), approximately 8000 ankle sprains occur daily in Germany alone, with more than 6% of the general population reported to seek medical assistance for severe ankle sprains in Denmark [3]. Thereby, it is likely that the incidence rate of injuries to the ankle ligaments is significantly higher than reported in epidemiological studies because up to 50% of patients are estimated not to seek medical assistance, and thus, remain unregistered [4].
The most common mechanism for lateral ankle ligament injuries is a combination of inversion and adduction of the foot in plantarflexion (i.e., supination trauma) [5]. Using computational modelling of 3D ankle joint kinematics, Wei, Fong, Chan, and Haut (2015) [6] found the most significant stretch-induced stress in the ligaments as a result of inversion and plantar-flexion combined with internal rotation. Thereby, the anterior talofibular ligament of the lateral ligament complex represents the weakest part of the ankle joint, and thus, is affected in 85% of ankle sprains [7,8]. Isolated injuries to the medial ligament complex seem to occur less frequently compared to injuries to the lateral ligament complex, amounting to 3–4% of all ligament injuries to the ankle joint [9]. Nonetheless, there exists evidence suggesting that the incidence rate of medial ligament injuries to the ankle joint might be underestimated [10,11]. Frequently, patients will describe an eversion, external rotation, or abduction mechanism [8].
Chronic ankle joint instability is observed in up to 40% of patients [12], with the main cause being the inadequate treatment and recurrence of acute ankle supination traumas [1,13,14,15]. The primary clinical management of acute ankle sprains with injury to the lateral ligament complex is non-surgical treatment, including immobilization through casts, functional treatment with bandages, compression tapes, and different type of braces accompanied by medication for pain relief [5,16]. There is increasing evidence to suggest that functional treatment, possibly in combination with semi-rigid bracing, is more effective for regaining joint stability following an acute ankle distortion trauma compared to immobilization [5,17,18].
A range of materials is clinically used to stabilize the ankle during the recovery phase, which can be categorized into the following groups [19]: tape, compression bandages, lace-up ankle support, semi-rigid or rigid ankle support (i.e., brace). Thereby, the benefits of orthoses have been summarized as (i) increased resistance against passive joint motion, and thus, protection of ligaments from overextension; (ii) slowing-down of supination movement to allow adaptation of muscular structures for support; (iii) stabilization of foot in neutral position; and (iv) proprioceptive stimulation to encourage a change in movement patterns [18].
From a biomechanical point of view, the joint should be stabilized throughout the recovery phase with a gradual increase in the ankle joint loading and range of motion (RoM) to ensure enough mechanical stimulation for tissue healing while avoiding excessive loading [20]. According to an in vitro cadaveric study, the ankle joint can be plantar-flexed up to 16° and dorsi-flexed up to 18° to significantly induce stress in the ligaments under unloaded condition [21], with reports of a sometimes significant alteration of stretch-induced stress in the ligaments upon further axial loading [22]. Plantarflexion of 16° and dorsiflexion of 18° are referred to as the zero strain reference for the anterior talofibular ligament (ATFL) and the posterior tibiofibular ligament (PTFL) and calcaneofibular ligament (CL), respectively, by Ozeki et al. (2002) [21]. Thus, according to Ozeki et al. (2002) [21], the central fibers of these ligaments function only in plantarflexion and dorsiflexion greater than the abovementioned degrees. To our knowledge, zero strain references for the ankle ligaments with inversion and eversion RoM have not been determined yet in current literature.
In conclusion, a wide range of orthoses is available to stabilize the ankle joint following Grade I to III supination traumas, and selectively restrict RoM to avoid excessive loading during the recovery phase. To our knowledge, however, there is no scientifically-based evidence to confirm the level of support (i.e., restriction in RoM) for different types of semi-rigid braces. In recent times, adaptable semi-rigid ankle braces have been developed to change the level of support during the course of recovery, for example, the Ortho Tri-PhaseTM ankle brace (Künzli Swiss Schuh AG) (Figure 1). Yet, it remains unclear to what extent the mechanical performance of adaptable semi-rigid ankle braces compares with traditional semi-rigid braces or rigid casts. Thus, the goal of the present study was to quantify and compare the restrictions of RoM in the sagittal (plantar-/dorsiflexion) and frontal plane (in-/eversion) during simulated walking between the Ortho Tri-Phase ankle brace, four semi-rigid braces from different suppliers, as well as one rigid cast.

Figure 1.
The Ortho Tri-PhaseTM ©Künzli semi-rigid brace. The diagram depicts the phase adapted concept of the Ortho Tri-Phase according to the healing stage. Range of motion (RoM) is initially limited to 10° of flexion/extension and can be gradually increased, as shown above, without the need to change the device. (Graphic with Permission of Künzli/Switzerland).
2. Material and Method
2.1. Orthoses and Measurement Set-Up
The restrictions in RoM during gait of the following seven orthoses were analyzed: one adaptable semi-rigid ankle brace (OrthoTri-Phase TM by Künzli), four non-adaptable semi-rigid ankle braces (OrthoStandardTM by Künzli, MalleoLocTM by Bauerfeind, MalleoSprintTM by Ottobock, VACOankleTM by OPED) (Figure 2), as well as one rigid cast. Walking was simulated using the ankle joint simulator with the fast testing method (FTM) as outlined in [23] (Figure 3). Thereby, predefined time sequences of rotational moments and axial loading during gait were applied to the orthosis via a wooden shank-foot model. The shank-foot model was custom-made according to anthropometric measures with a foot size of 43. The foot was connected to a joint mechanically emulating the metatarsophalangeal joint, allowing physiologically similar movement in the forefoot region. The subtalar joint, between shank and foot, was represented by a ball-and-socket joint to allow for rotational degrees of freedom in all anatomical planes. Two pressure sensitive air pads were placed on the instep of the foot and the dorsal surface of the shank, kept in place via a sock, and filled with air to ensure constant pressure inside the shoe for different measurement set-ups (Figure 3). Prior to conducting measurements, each orthosis was mounted on the wooden shank-foot model and set-up inside the simulator. Laces were tied up manually such that pressures of 0.32 ± 0.02 bar and 0.25 ± 0.02 bar were reached for each air pad. Furthermore, a pre-trial was conducted with rotational moments that exceeded the applied moments during simulated walking in order to ensure optimal fitting of the shoe with even pressure distribution via the pneumatic sock, as well as to eliminate any bias due to changes in the initial material stiffness of new orthosis (i.e., hysteresis behavior).

Figure 2.
Orthoses considered in this study (left to right): Ortho Tri-PhaseTM ©Künzli; OrthoStandardTM ©Künzli; MalleoLocTM ©BauerfeindTM; VACOankleTM ©OPED; MalleoSprintTM ©Ottobock.
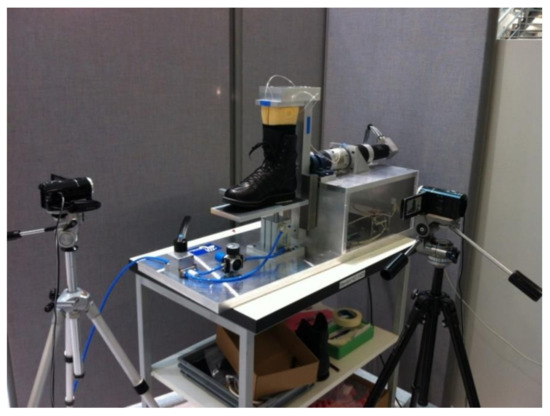
Figure 3.
Fast testing method (FTM) ankle joint simulator [23] used to assess restrictions in the RoM of plantar-/dorsiflexion for different orthoses. The movement of the wooden shank-foot couple is initiated via a motorized lever arm while the orthosis is resting on a pneumatic pressure plate to apply vertical ground reaction forces (body weight). Restrictions in the RoM of in-/eversion are measured by rotating the shoe by 90° degrees.
2.2. Simulation of Walking
Following measurement set-up and pre-trial, five trials of walking were simulated by applying the corresponding rotational moments and ground reaction forces (Figure 3) according to Bürgi et al. (2015) with the orthoses perpendicular to the frontal plane for deriving the RoM of plantar-/dorsiflexion as the average over the five trials. To simulate an adult gait, a vertical ground reaction force of 800 N and the following ankle joint moments were used: plantar flexion −3.1 Nm, dorsal extension 12.1 Nm, eversion −1.8 Nm, and inversion 4.6 Nm. Subsequently, another five trials of simulated walking were conducted with the same loading regime but with the shoe perpendicular to the sagittal plane for deriving the RoM of in-/eversion as the average over the five trials. The pneumatic pressure inside the shoe was measured throughout testing, as well as following the removal of the orthosis from the simulator, in order to ensure the same measurement set-up for different trials and different products.
2.3. Statistical Analysis
The peak values of plantar-/dorsiflexion and in-/eversion during simulated walking (recorded as averages over the five trials) were analyzed for statistically significant differences using single-factorial analysis of variance (ANOVA) with p < 0.05. The single independent variable was the type of orthoses. A post-hoc Bonferroni test was applied to the data in case of demonstrated significant differences from ANOVA.
3. Results
The validity of the FTM in reliably measuring ankle joint ROM in the sagittal and frontal plane at controlled torque levels with application of body weight forces was previously demonstrated, with the intra-class correlation coefficient (ICC) of 0.99 and the standard deviations between measurements with the same orthosis being consistently <9.8% [23]. Significant differences in peak plantar-/dorsiflexion as well as in-/eversion during gait were found between different types of orthoses (Table 1 and Table 2). In the sagittal plane, the greatest restriction in peak RoM was obtained by means of the rigid cast, followed by the Ortho Tri-PhaseTM in Phase 1 and the Ortho StandardTM (Figure 3). Three types of orthoses exceeded the zerostrain-refence of 18° dorsiflexion [21] during gait (Figure 4). Specifically, the peak dorsiflexion during gait for the MalleoSprintTM was 19.1°, for the Ortho Tri-PhaseTM in Phase 3 was 20.6°, and for the VACOankleTM was 24.7°, respectively. The rigid cast significantly restricted the RoM in the sagittal plane compared to all other orthoses, as can be seen in Table 1.

Table 1.
p-Values representing the significant differences (yellow), No difference (pink). not applycable (gray) in peak plantarflexion (lower left values) and dorsiflexion (upper right values) RoM during simulated walking between different types of orthoses.). Statistical result of the different orthoses for Dorsiflexion and Plantarflexion.
Table 2.
p-Values representing significant differences (yellow), No difference (pink). not applycable (gray) in peak eversion (lower left values) and inversion (upper right values) movement during simulated walking between different types of orthoses. Statistical result of the different orthoses for Inversion and Eversion.
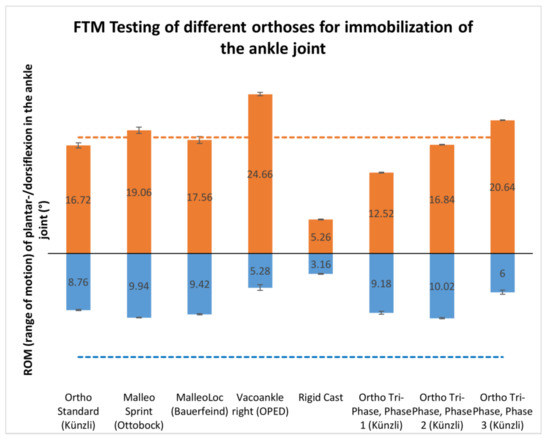
Figure 4.
RoM in the sagittal plane with the maximum values of dorsiflexion (red) and plantarflexion (blue) recorded as averages over five trials of simulated walking. The zero strain reference of dorsiflexion (red, 18°) and plantarflexion (blue, 16°) by [20] are indicated with dashed lines.
The VACOankleTM allowed for the largest dorsiflexion movement during gait (Figure 3), being statistically relevant compared to all other devices (Table 1), while plantarflexion was significantly reduced except in comparison to the cast (Table 1).
In the frontal plane, the restriction of movement by means of the VACOankleTM semi-rigid brace most closely resembled that of the rigid cast (Figure 4), while in comparison with each of the other orthoses the cast showed a significant lesser peak inversion and a significantly higher eversion. Concerning inversion, the VACOankleTM showed significantly reduced values of all tested items with exception to the cast and the Ortho Tri-PhaseTM in Phase 1 (Table 2). The MalleoLocTM semi-rigid brace significantly limited dorsiflexion and eversion movement during gait compared to the MalleoSprintTM. Focusing on the Ortho Tri-PhaseTM, the largest difference in the restriction of movement was observed when changing to the Phase 3 configuration, leading to significantly larger dorsiflexion, inversion, and eversion, and significantly smaller plantarflexion compared to Phase 1 and Phase 2. In Phase 3, the Ortho Tri-PhaseTM allowed for the largest RoM in the frontal plane during gait out of all of the orthoses (Figure 4 and Figure 5). In Phase 1, the movement restrictions of the Ortho Tri-PhaseTM showed a significantly lower degree of dorsiflexion and eversion as compared to the Ortho StandardTM, while plantarflexion was higher and inversion lower without statistical significance, respectively.
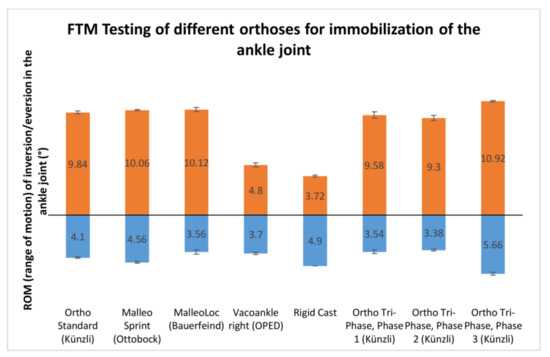
Figure 5.
RoM in the frontal plane with the maximum values of inversion (red) and eversion (blue) recorded as averages over five trials of simulated walking.
4. Discussion
The goal of the present study was to quantify and compare the restrictions in plantar-/dorsiflexion and in-/eversion RoM during simulated walking between six different orthoses, including one semi-rigid adaptable ankle brace, four non-adaptable semi-rigid ankle braces from different suppliers, as well as one rigid cast. Three types of orthoses (i.e., MalleoSprintTM, VACOankleTM, Ortho Tri-PhaseTM in Phase 3) exceeded the zero strain reference of 18° dorsiflexion during gait [21], with the highest peak dorsiflexion during gait measured for the VACOankleTM as 37% above the recommended limit. A higher risk of inducing critical stress in the ligaments is given for these orthoses, which may be disadvantageous during the recovery process from severe ankle sprains (Grade II and III), especially in the early stages of healing. It should be noted, however, that the Ortho Tri-PhaseTM in Phase 3 is only recommended for the final stages of recovery, with increased levels of stress needed for functional healing and remodeling of the connective tissue [5]. The significantly larger dorsiflexion RoM with the VACOankleTM may be associated with the lack of strapping across the dorsum of the foot compared to other semi-rigid braces (e.g., MalleoLocTM, the MalleoSprintTM, Ortho StandardTM, and Ortho Tri-PhaseTM). As such, the VACOankleTM appears to be designed to mainly restrict RoM in the frontal plane, which is confirmed in the present work, and may be best applied for functional treatment following isolated supination trauma to the lateral ligament complex. The observed inversion joint angles are larger compared to the eversion joint angle. This might be due to the fact that there is a higher demand during gait in the direction of inversion resulting in larger testing moment in this study. Although the joint angles are smaller for eversion, the same amount of significant differences were observed for eversion and inversion.
In previous work, a prospective randomized controlled trial in 47 patients with acute ankle sprain Grade II demonstrated faster functional recovery (i.e., agility tests and activity levels) with a semi-rigid adaptable ankle brace (Malleo TriStepTM by Otto Bock) in comparison to a non-adaptable ankle brace (AircastTM Air-Stirrup by DJO Global) [24]. The differences between the two intervention groups in the study [24] were marginal but suggest that patients with a severe ankle sprain (Grade II or III) may benefit from a phase adaptable ankle brace, such as the Ortho Tri-PhaseTM. The different configurations of semi-rigid adaptable orthoses allow for successive increases of ligament loading during the recovery process, initially protecting from inversion to prevent chronic elongation of the ligaments, and subsequently, increasing the stretch-induced stress to promote proper collagen fiber orientation and avoid the harmful effects of immobilization [5,24,25]. Specifically, the exo-carbon joint support of the Ortho Tri-PhaseTM is removed in Phase 3 and should allow unrestricted movement in the sagittal plane and increased RoM in the frontal plane. We measured a reduced plantarflexion in Phase 3 in comparison to Phase 2; the reason for this remains unclear to the authors. The only stability in Phase 3 is provided through an exo-carbon base support in combination with Velcro straps. In the late recovery stages corresponding to Phase 3, it is crucial to avoid a new supination trauma, and therefore the exo-carbon base support acts as a guard against traumatic eversion and inversion.
Our results suggest that the Ortho Tri PhaseTM orthosis allows for non-surgical treatment of ankle sprains Grade I to III without the need for changing the type of orthosis during the recovery phase, providing successive and significant increase in peak RoM in the frontal and sagittal plane from Phase 1 to Phase 3, with the exception of the plantarflexion in Phase 3, which is decreased. Surprisingly, the theoretical peak restriction in plantar-/dorsiflexion with the Ortho-Tri-PhaseTM in Phase 1 is given to be 10° according to the supplier, yet we measured a peak dorsiflexion of more than 10° for all three configurations. While the reason for the difference between measured and theoretical values remains unclear, the movement restriction in the sagittal plane with the Ortho-Tri-PhaseTM in Phase 1 and Phase 2 did not exceed the zero-strain reference of 16° plantarflexion and 18° dorsiflexion suggested by [21]. Nevertheless, it should be noted that the suggested critical limits are derived from in vitro cadaveric experiments without vertical loading, with ligament loading known to alternate in the presence of gravitational forces [22].
The dynamics of the ankle joint are highly complex, with joint instability being caused by multiple factors, for example, anatomic deficits, muscular imbalance, or impaired neuromuscular control [22,26,27]. The ankle joint simulator in the present work was based on a wooden foot-shank couple with a metatarsophalangeal joint to represent the forefoot region and a ball-and-socket joint to represent the subtalar joint [23]. In reality, the subtalar joint resembles a hinge joint with dynamic rotational axes. Thereby, the congruent surfaces of the tibiotalar joint surfaces are anatomically restricting in-/eversion RoM [27]. Yet, it remains unclear to what extent these anatomical features are affecting peak RoM during gait for different orthoses because of the simplified representation of the ankle joint as a ball-and-socket joint in the present work. Furthermore, rotational movements of the shank that occur during plantar-/dorsiflexion in the natural joint were not considered in the present work and may further affect the present results.
A wide range of orthoses are available for non-surgical treatment of ankle sprains, yet science-based recommendations with regards to the specific range of movement restrictions in the frontal and sagittal plane to ensure enough mechanical stimulus for functional recovery of the ligaments without overloading remain largely lacking. Here, complementary research is needed to establish clear guidelines on the upper limits of RoM in the sagittal and frontal plane for Grade I to Grade III ankle sprains. The present results of peak RoM during simulated walking for different orthoses may help clinicians and physiotherapists in the decision-making process of finding the optimal orthosis for individual patients. An extension of the present research to elucidate the additional influence of rotational movements in the transverse plane, as well anatomical aspects of joint congruency, is recommended. Furthermore, in situ research using mechanical simulators should be accompanied by randomized controlled trials to confirm the clinical benefits, including patient satisfaction, for non -adaptable versus adaptable ankle braces in vivo.
Acknowledgements
This research was supported by Künzli SwissSchuh AG by providing the Ortho Tri-PhaseTM and Ortho StandardTM Orthoses. The other Orthoses were provided by Kantonsspital Olten SoH, thank you for that.
Author Contributions
Frank Thiele, Sebastian Schuhmacher contributed as follows: Study conception and design, acquisition of data, analysis and interpretation of data, drafting of manuscript, critical revision; Christoph Schwaller: Interpretation of data, drafting of manuscript; Stefan Plüss: Technical support during measurement, drafting of manuscript; Joël Rhiner: Data processing and calculating the statistics, drafting of manuscript; Renate List: Study conception and design, interpretation of data, drafting of manuscript; Silvio Lorenzetti: Study conception and design: Acquisition of data, Analysis and interpretation of data, Drafting of manuscript, Critical revision.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Valderrabano, V.; Hintermann, B.; Horisberger, M.; Fung, T.S. Ligamentous posttraumatic ankle osteoarthritis. Am. J. Sports Med. 2006, 34, 612–620. [Google Scholar] [CrossRef] [PubMed]
- Waterman, B.R.; Owens, B.D.; Davey, S.; Zacchilli, M.A.; Belmont, P.J., Jr. The epidemiology of ankle sprains in the United States. J. Bone Joint Surg. Am. 2010, 92, 2279–2284. [Google Scholar] [CrossRef] [PubMed]
- Hølmer, P.; Søndergaard, L.; Konradsen, L.; Nielsen, P.T.; Jørgensen, L.N. Epidemiology of sprains in the lateral ankle and foot. Foot Ankle Int. 1994, 15, 72–74. [Google Scholar] [CrossRef] [PubMed]
- Gribble, P.A.; Bleakley, C.M.; Caulfield, B.M.; Docherty, C.L.; Fourchet, F.; Fong, D.T.-P.; McKeon, P.O. 2016 consensus statement of the International Ankle Consortium: Prevalence, impact and long-term consequences of lateral ankle sprains. Br. J. Sports Med. 2016, 50, 1493–1495. [Google Scholar] [CrossRef] [PubMed]
- Petersen, W.; Rembitzki, I.V.; Koppenburg, A.G.; Ellermann, A.; Liebau, C.; Brüggemann, G.P.; Best, R. Treatment of acute ankle ligament injuries: A systematic review. Arch. Orthop. Trauma Surg. 2013, 133, 1129–1141. [Google Scholar] [CrossRef] [PubMed]
- Fong, D.T.-P.; Chan, Y.-Y.; Mok, K.-M.; Yung, P.S.; Chan, K.-M. Understanding acute ankle ligamentous sprain injury in sports. BMC Sports Sci. Med. Rehabil. 2009, 1, 14. [Google Scholar] [CrossRef] [PubMed]
- Giza, E.; Shin, E.C.; Wong, S.E.; Acevedo, J.I.; Mangone, P.G.; Olson, K.; Anderson, M.J. Arthroscopic suture anchor repair of the lateral ligament ankle complex: A cadaveric study. Am. J. Sports Med. 2013, 41, 2567–2572. [Google Scholar] [CrossRef] [PubMed]
- Wenny, R.; Duscher, D.; Meytap, E.; Weninger, P.; Hirtler, L. Dimensions and attachments of the ankle ligaments: Evaluation for ligament reconstruction. Anat. Sci. Int. 2015, 90, 161–171. [Google Scholar] [CrossRef] [PubMed]
- Ribbans, W.J.; Garde, A. Tibialis posterior tendon and deltoid and spring ligament injuries in the elite athlete. Foot Ankle Clin. 2013, 18, 255–291. [Google Scholar] [CrossRef] [PubMed]
- Crim, J.R.; Beals, T.C.; Nickisch, F.; Schannen, A.; Saltzman, C.L. Deltoid ligament abnormalities in chronic lateral ankle instability. Foot Ankle Int. 2011, 32, 873–878. [Google Scholar] [PubMed]
- Hintermann, B.; Boss, A.; Schäfer, D. Arthroscopic findings in patients with chronic ankle instability. Am. J. Sports Med. 2002, 30, 402–409. [Google Scholar] [CrossRef] [PubMed]
- Hintermann, B.; Valderrabano, V.; Boss, A.; Trouillier, H.H.; Dick, W. Medial ankle instability. Am. J. Sports Med. 2004, 32, 183–190. [Google Scholar] [CrossRef] [PubMed]
- Ferran, N.A.; Maffulli, N. Epidemiology of sprains of the lateral ankle ligament complex. Foot Ankle Clin. 2006, 11, 659–662. [Google Scholar] [CrossRef] [PubMed]
- Leumann, A.; Tsaknis, R.; Wiewiorski, M.; Valderrabano, V. Das akute Supinationstrauma des oberen Sprunggelenkes—Eine Bagatelle? Schweiz Med. Forum 2008, 8, 214–216. [Google Scholar]
- McCriskin, B.J.; Cameron, K.L.; Orr, J.D.; Waterman, B.R. Management and prevention of acute and chronic lateral ankle instability in athletic patient populations. World J. Orthop. 2015, 6, 161–171. [Google Scholar] [CrossRef] [PubMed]
- Van Rijn, R.M.; Van Os, A.G.; Bernsen, R.M.; Luijsterburg, P.A.; Koes, B.W.; Bierma-Zeinstra, S.M. What is the clinical course of acute ankle sprains? A systematic literature review. Am. J. Med. 2008, 121. [Google Scholar] [CrossRef] [PubMed]
- Kerkhoffs, G.; Rowe, B.H.; Assendelft, W.; Kelly, K.; Struijs, P.; Van Dijk, C. Immobilisation and functional treatment for acute lateral ankle ligament injuries in adults. Cochrane Database Syst. Rev. 2002, 3. [Google Scholar] [CrossRef]
- Struijs, P.A.; Kerkhoffs, G.M. Ankle sprain. BMJ Clin. Evid. 2010. [Google Scholar] [PubMed Central]
- Rosenbaum, D.; Becker, H. Ankle orthotic devices. Review, areas of application, and scientific results. Orthopade 1999, 28, 559–564. [Google Scholar] [CrossRef] [PubMed]
- Cottrell, J.A.; Turner, J.C.; Arinzeh, T.L.; O’Connor, J.P. The Biology of Bone and Ligament Healing. Foot Ankle Clin. 2016, 21, 739–761. [Google Scholar] [CrossRef] [PubMed]
- Ozeki, S.; Yasuda, K.; Kaneda, K.; Yamakoshi, K.; Yamanoi, T. Simultaneous strain measurement with determination of a zero strain reference for the medial and lateral ligaments of the ankle. Foot Ankle Int. 2002, 23, 825–832. [Google Scholar] [CrossRef] [PubMed]
- Cawley, P.W.; France, E.P. Biomechanics of the lateral ligaments of the ankle: An evaluation of the effects of axial load and single plane motions on ligament strain patterns. Foot Ankle 1991, 12, 92–99. [Google Scholar] [CrossRef] [PubMed]
- Bürgi, S.; Roost, J.; Hitz, M.R.; Schwilch, P.; Taylor, W.R.; Lorenzetti, S. A fast testing method to objectively quantify the stiffness of stability boots. Appl. Bion. Biomech. 2015, 595708. [Google Scholar] [CrossRef] [PubMed]
- Best, R.; Böhle, C.; Schiffer, T.; Petersen, W.; Ellermann, A.; Brueggemann, G.P.; Liebau, C. Early functional outcome of two different orthotic concepts in ankle sprains: A randomized controlled trial. Arch. Orthop. Trauma Surg. 2015, 135, 993–1001. [Google Scholar] [CrossRef] [PubMed]
- Mattacola, C.G.; Dwyer, M.K. Rehabilitation of the ankle after acute sprain or chronic instability. J. Athl. Train. 2002, 37, 413–429. [Google Scholar] [PubMed]
- Knupp, M.; Lang, T.H.; Zwicky, L.; Lötscher, P.; Hintermann, B. Chronic ankle instability (medial and lateral). Clin. Sports Med. 2015, 34, 679–688. [Google Scholar] [CrossRef] [PubMed]
- Knupp, M.; Valderrabano, V.; Hintermann, B. Anatomical and biomechanical aspects of total ankle replacement. Orthopade 2006, 35, 489–494. [Google Scholar] [CrossRef] [PubMed]





© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).