Balance Performance in Collegiate Athletes: A Comparison of Balance Error Scoring System Measures


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
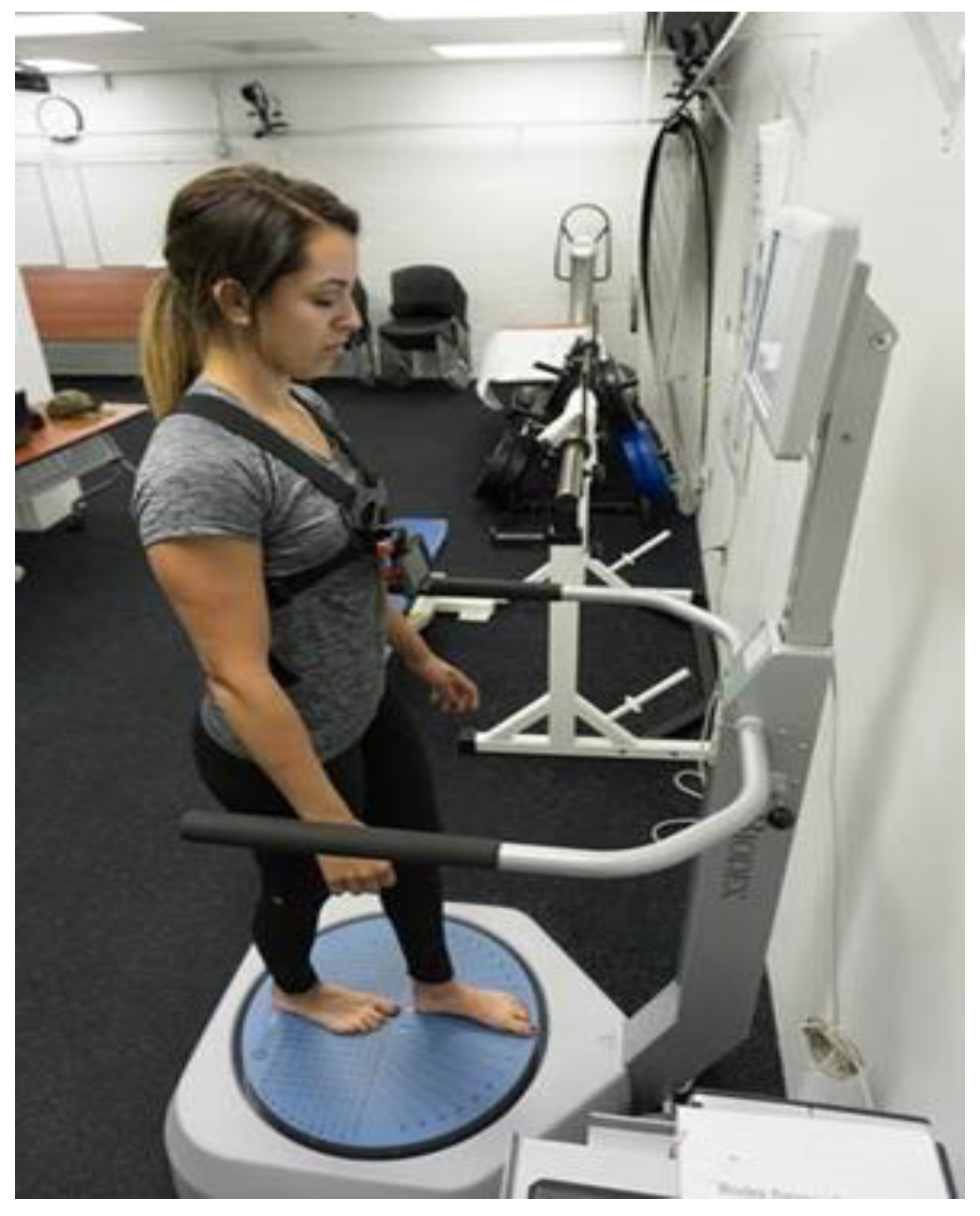
2.2. Instrumentation
2.3. Procedures
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Pai, Y.-C.; Patton, J. Center of mass velocity-position predictions for balance control. J. Biomech. 1997, 30, 347–354. [Google Scholar] [CrossRef]
- Manchester, D.; Woollacott, M.; Zederbauer-Hylton, N.; Marin, O.V. Vestibular and Somatosensory Contributions to Balance Control in the Older Adult. J. Gerontol. 1989, 44, M118–M127. [Google Scholar] [CrossRef] [PubMed]
- Winter, D.A. Human balance and posture control during standing and walking. Gait Post. 1995, 3, 193–214. [Google Scholar] [CrossRef]
- Horak, F.B.; Nashner, L.M.; Diener, H.C. Postural strategies associated with somatosensory and vestibular loss. Exp. Brain Res. 1990, 82, 167–177. [Google Scholar] [CrossRef] [PubMed]
- Aartolahti, E.; Häkkinen, A.; Lönnroos, E.; Kautiainen, H.; Sulkava, R.; Hartikainen, S. Relationship between functional vision and balance and mobility performance in community-dwelling older adults. Aging Clin. Exp. Res. 2013, 25, 545–552. [Google Scholar] [CrossRef] [PubMed]
- Susco, T.M.; Valovich McLeod, T.C.; Gansneder, B.M.; Shultz, S.J. Balance recovers within 20 minutes after exertion as measured by the balance error scoring system—proquest. J. Athl. Train. 2004, 39, 241–246. [Google Scholar] [PubMed]
- Freeman, M.A.R. Instability of the foot after injuries to the lateral ligament of the ankle. J. Bone Joint Surg. Br. 1965, 47, 669–677. [Google Scholar] [PubMed]
- Rasool, J.; George, K. The impact of single-leg dynamic balance training on dynamic stability. Phys. Ther. Sport 2007, 8, 177–184. [Google Scholar] [CrossRef]
- Chander, H.; Dabbs, N.C. Balance performance and training among female athletes. J. Strength Cond. Res. 2016, 38, 8–13. [Google Scholar] [CrossRef]
- Chander, H.; MacDonald, C.J.; Dabbs, N.C.; Allen, C.R.; Lamont, H.S.; Garner, J.C. Balance Performance in female collegiate athletes. J. Sports Sci. 2014, 2, 13–20. [Google Scholar]
- Onate, J.A.; Beck, B.C.; Van Lunen, B.L. On-field testing environment and balance error scoring system performance during preseason screening of healthy collegiate baseball players. J. Athl. Train. 2007, 42, 446–451. [Google Scholar] [PubMed]
- Patterson, J.A.; Amick, R.Z.; Pandya, P.D.; Hakansson, N.; Jorgensen, M.J. Comparison of a mobile technology application with the balance error scoring system. Int. J. Athl. Ther. Train. 2014, 10, 4–7. [Google Scholar] [CrossRef]
- Patterson, J.A.; Amick, R.Z.; Thummar, T.; Rogers, M.E. Validation of measures from the smartphone sway balance application: A pilot study. Int. J. Sports Physcial Ther. 2014, 9, 135–139. [Google Scholar]
- Finnoff, J.T.; Peterson, V.J.; Hollman, J.H.; Smith, J. Intrarater and interrater reliability of the balance error scoring system (bess). PM&R 2009, 1, 50–54. [Google Scholar] [CrossRef]
- Chang, J.O.; Levy, S.S.; Seay, S.W.; Goble, D.J. An alternative to the balance error scoring system: Using a low-cost balance board to improve the validity/reliability of sports-related concussion balance testing. Clin. J. Sport Med. 2014, 24, 256–262. [Google Scholar] [CrossRef] [PubMed]
- Bittel, A.J.; Elazzazi, A.; Bittel, D.C. Accuracy and precision of an accelerometer-based smartphone app designed to monitor and record angular movement over time. Telemed. E-Health 2015, 22, 302–309. [Google Scholar] [CrossRef] [PubMed]
- Amick, R.Z.; Chaparro, A.; Patterson, J.A.; Jorgensen, M.J. Test-retest reliability of the sway balance mobile application. J. Mob. Technol. Med. 2015, 4, 40–47. [Google Scholar] [CrossRef]
- Hopkins, W.; Burke, L. Design and analysis of research on sport performance enhancement. Med. Sci. Sports Exerc. 1999, 31, 472–485. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, W. Measures of Reliability in Sports Medicine and Science. Sports Med. 2000, 30, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Collins, M.W.; Lovell, M.R.; Iverson, G.L.; Cantu, R.C.; Maroon, J.C.; Field, M. Cumulative effects of concussion in high school athletes. J. Neurosurg. 2002, 51, 1175–1181. [Google Scholar] [CrossRef]
- Majerske, C.W.; Mihalik, J.P.; Ren, D.; Collins, M.W.; Reddy, C.C.; Lovell, M.R.; Wagner, A.K. Concussion in sports: Postconcussive activity levels, symptoms, and neurocognitive performance. J. Athl. Train. 2008, 43, 265–274. [Google Scholar] [CrossRef] [PubMed]
- Fazio, V.C.; Lovell, M.R.; Pardini, J.E.; Collins, M.W. The relation between post concussion symptoms and neurocognitive performance in concussed athletes. J. Neuorehab. 2007, 22, 207–216. [Google Scholar]
- Wasserman, E.B.; Kerr, Z.Y.; Zuckerman, S.L.; Covassin, T. Epidemiology of sports-related concussions in national collegiate athletic association athletes from 2009–2010 to 2013–2014 symptom prevalence, symptom resolution time, and return-to-play time. Am. J. Sports Med. 2015. [Google Scholar] [CrossRef]
- Register-Mihalik, J.K.; Mihalik, J.P. Guskiewcz balance deficits after sports-related concussions in individuals reporting posttraumatic headache. J. Neurosurg. 2008, 63, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Guskiewicz, K.M.; Marshall, S.W.; Bailes, J.; McCrea, M.; Cantu, R.C.; Randolph, C.; Jordan, B.D. Association between recurrent concussion and late-life cognitive impairment in retired professional football players. Neurosurgery 2005, 719–726. [Google Scholar] [CrossRef]
- Guskiewicz, K.; Marshall, S.; Bailes, J.; McCrea, M.; Harding, H.; Matthews, A.; Mihalik, J.; Cantu, R. Recurrent concussion and risk of depression in retired professional football players. Med. Sci. Sports Exerc. 2007, 39, 903–909. [Google Scholar] [CrossRef] [PubMed]
- Guskiewicz, K.M. Balance assessment in the management of sport-related concussion. Clin. Sports Med. 2011, 30, 89–102. [Google Scholar] [CrossRef] [PubMed]
- Broglio, S.P.; Cantu, R.C.; Gioia, G.A.; Guskiewcz, K.M.; Kutcher, J.; Palm, M.; Valovich McLeod, T.C. National athletic trainers’ association position statement: management of sport concussion. J. Athl. Train. 2014, 49, 245–265. [Google Scholar] [CrossRef] [PubMed]
- Mulligan, I.; Boland, M.; Payette, J. Prevalence of neurocognitive and balance deficits in collegiate football players without clinically diagnosed concussion. J. Orthop. Sports Phys. Ther. 2012, 42, 625–632. [Google Scholar] [CrossRef] [PubMed]
- McCrea, M.; Guskiewicz, K.M.; Marshall, S.W.; Barr, W.; Randolph, C.; Cantu, R.C.; Onate, J.A.; Yang, J.; Kelly, J.P. Acute effects and recovery time following concussion in collegiate football players: the NCAA concussion study. JAMA 2003, 290, 2556–2563. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Conditions | BioDex SD | SwayApp | r-Values | p-Value |
|---|---|---|---|---|
| Feet together | 0.72 ± 0.31 | 99.43 ± 1.03 | r = −0.32 | p < 0.001 * |
| Tandem left | 2.29 ± 1.19 | 88.39 ± 14.32 | r = − 0.32 | p < 0.001 * |
| Tandem right | 2.11 ± 0.99 | 88.04 ± 16.56 | r = −0.12 | p = 0.080 |
| Single-leg right | 3.35 ± 1.72 | 55.81 ± 34.72 | r = −0.64 | p < 0.010 * |
| Single-leg left | 3.61 ± 2.09 | 53.53 ± 36.16 | r = −0.69 | p < 0.010 * |
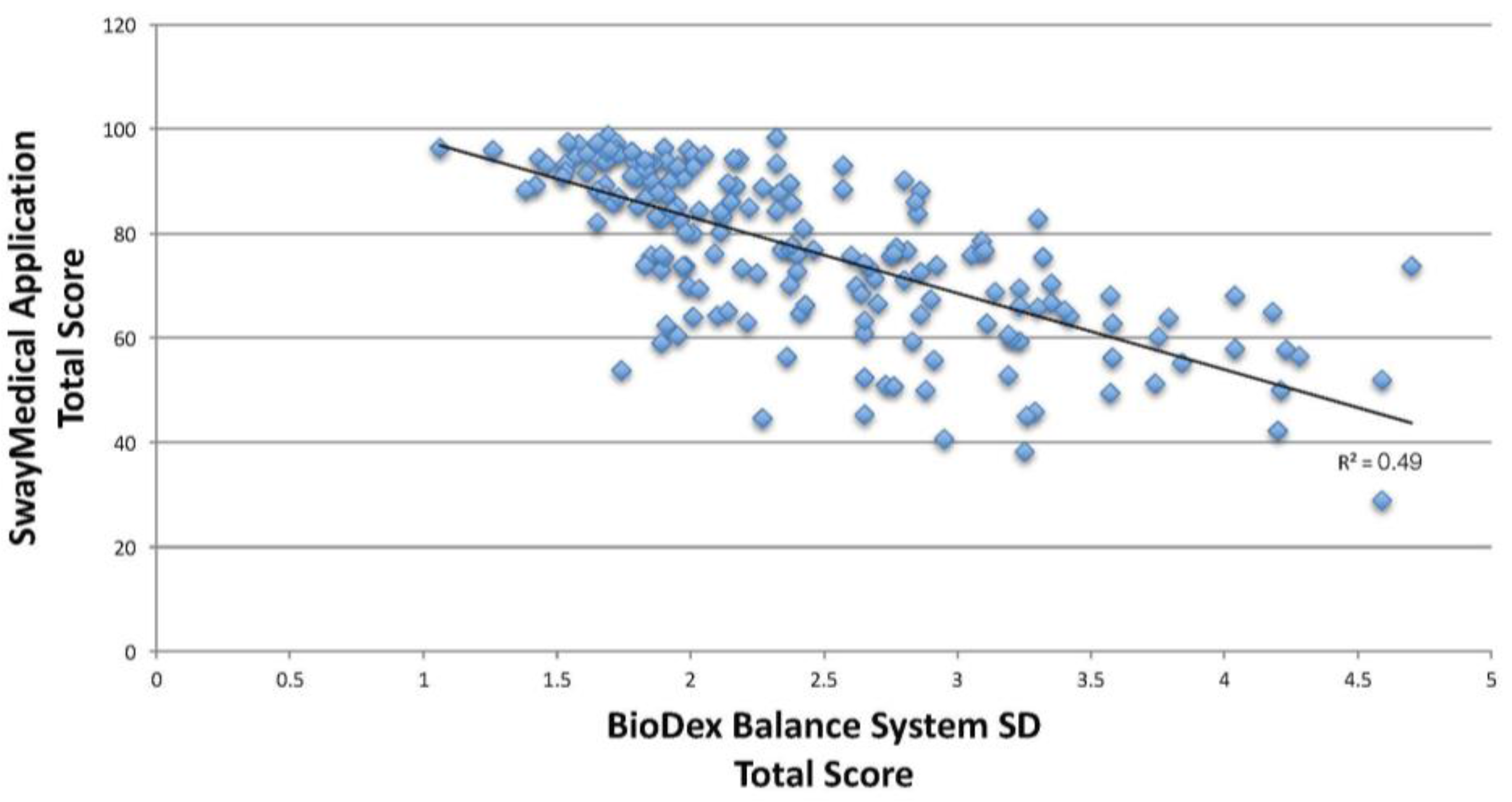
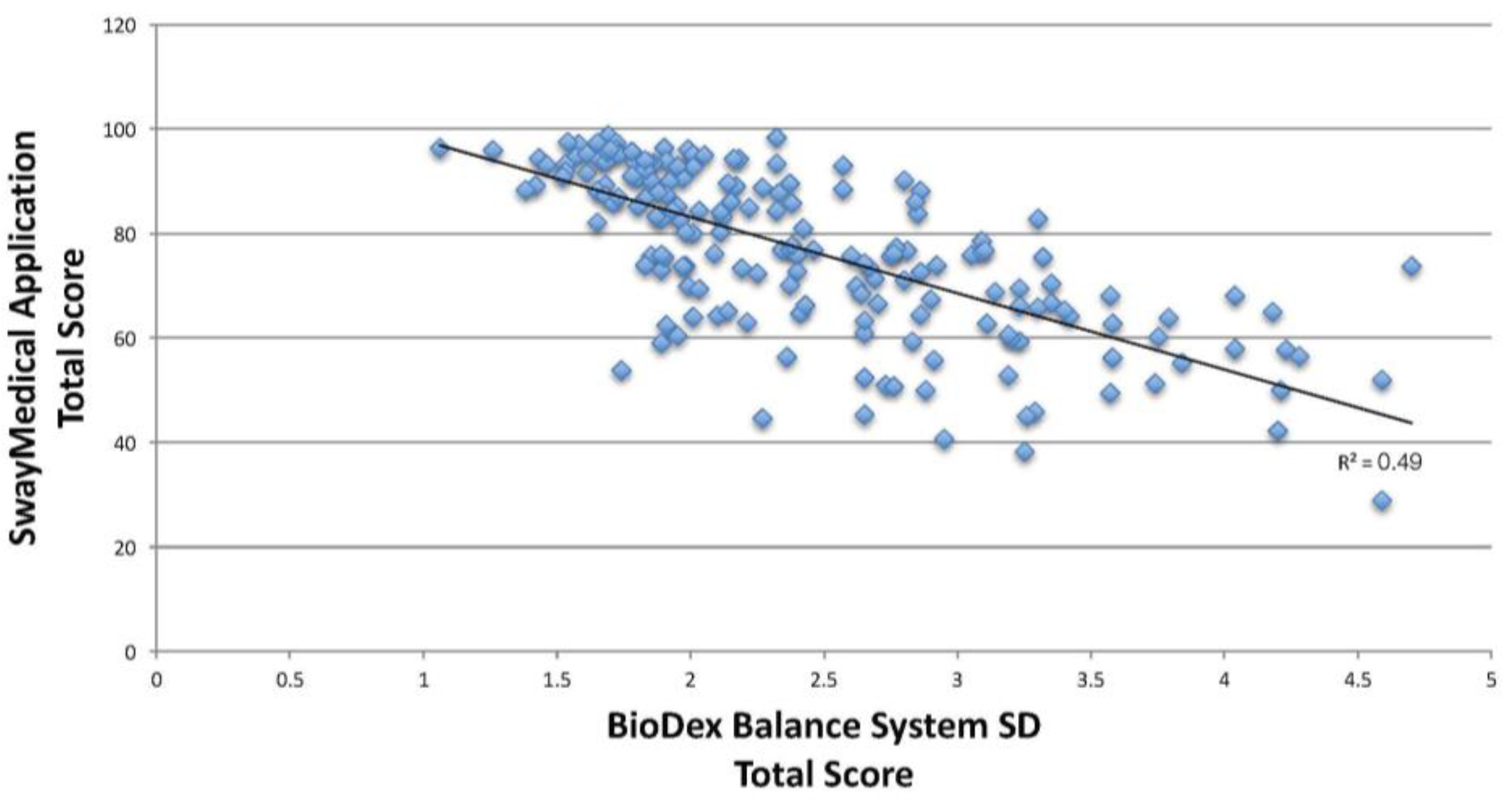
| Total score | 2.43 ± 0.75 | 76.85 ± 115.5 | r = −0.70 | p < 0.010 * |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dabbs, N.C.; Sauls, N.M.; Zayer, A.; Chander, H. Balance Performance in Collegiate Athletes: A Comparison of Balance Error Scoring System Measures. J. Funct. Morphol. Kinesiol. 2017, 2, 26. https://doi.org/10.3390/jfmk2030026
Dabbs NC, Sauls NM, Zayer A, Chander H. Balance Performance in Collegiate Athletes: A Comparison of Balance Error Scoring System Measures. Journal of Functional Morphology and Kinesiology. 2017; 2(3):26. https://doi.org/10.3390/jfmk2030026
Chicago/Turabian StyleDabbs, Nicole C., Nicole M. Sauls, Alice Zayer, and Harish Chander. 2017. "Balance Performance in Collegiate Athletes: A Comparison of Balance Error Scoring System Measures" Journal of Functional Morphology and Kinesiology 2, no. 3: 26. https://doi.org/10.3390/jfmk2030026
APA StyleDabbs, N. C., Sauls, N. M., Zayer, A., & Chander, H. (2017). Balance Performance in Collegiate Athletes: A Comparison of Balance Error Scoring System Measures. Journal of Functional Morphology and Kinesiology, 2(3), 26. https://doi.org/10.3390/jfmk2030026