1. Introduction
Non-specific chronic neck pain (NSCNP) is a significant and multifaceted health problem in today’s society, ranking as the fourth leading cause of disability, with an annual prevalence rate exceeding 30% [
1]. The economic burden of neck pain is considerable, encompassing treatment costs, decreased productivity, and job-related issues. Globally, in 2017, the age-standardized prevalence and incidence rates of neck pain were 3551.1 and 806.6 per 100,000, respectively, and the years lived with disability from neck pain per 100,000 population was 352.0 (245.6 to 493.3) [
2].
NSCNP is defined as neck pain that lasts for more than 12 weeks, even after the injury has healed, or that recurs intermittently over a prolonged period [
3]. In patients with NSCNP, studies have identified symptoms such as local hyperalgesia; impaired conditioned pain modulation; psychological disturbances, including depressive symptoms; pain catastrophizing [
4]; reduced neck muscle strength and endurance [
5]; alterations in the timing and activation of the cervical muscles; fatty degeneration [
6]; and increased forward head posture (FHP) [
7]. Additionally, moderate respiratory dysfunction [
8] including chest wall expansion [
9] and alterations in normal breathing patterns [
8] have been noted in this population. Their neck movements may also be limited in quantity and quality [
6].
The spine is a multi-segmental kinetic biomechanical chain, and usually, dysfunction in one of its parts may affect an adjacent part. Given the biomechanical link between the cervical and thoracic spine, it is plausible that impaired thoracic spine mobility may contribute to the development of neck disorders [
10,
11,
12]. Kinematic and electromyographic results indicate that motor changes are not isolated to the neck and also affect the thoracic spine, thus highlighting the need to assess the spine’s kinematic variables (position, velocities, and accelerations) of its adjacent segments, which reflect alterations in muscle recruitment [
13].
Conversely, neck pain may lead to thoracic spine and rib-cage biomechanical alterations, contributing to dysfunctional breathing [
14,
15,
16], which is multi-dimensional and characterized by biochemical, biomechanical, and psychophysiological dimensions [
17].
There is no single definitive treatment for neck pain, with a significant number of patients with NSCNP seeking physical therapy treatment [
18]. Physical therapists often conduct thorough physical examinations to assess impairments and effectively monitor the progress of rehabilitation interventions. The American Physical Therapy Association (APTA) guidelines emphasize the importance of using reliable measures to assess changes in a patient’s level of function during treatment for neck pain [
19]. One such measure specifically recommended by the APTA is the cervical spine range of motion (CS-ROM) [
19,
20]. A visual estimation of range of motion (ROM) has been shown to be inaccurate and is not recommended for evaluating passive or active ROM [
21].
The evaluation of CS-ROM serves as a typical clinical approach to appraise and categorize individuals experiencing neck pain, determine any functional restrictions, and supply helpful predictive data. Still, clinicians ought to be careful about forming clinical opinions mainly on CS-ROM [
22]. An analysis of chronic neck-pain recovery predictors revealed that higher anxiety and limited lateral flexion range of motion were associated with a greater probability of positive results from manual therapy delivered according to the Mulligan concept [
23].
A recent systematic review with a meta-analysis [
24] mentioned that smartphone apps (clinometer apps, compass apps, and other type of apps) have proven to be reliable tools for measuring CS-ROM in people both with and without neck pain. For physiotherapists assessing neck movement, smartphone applications (apps) offer a valuable resource. However, the overall quality of the research supporting these apps is still limited. More rigorous studies with larger sample sizes are necessary to strengthen the evidence base for using smartphone apps to assess CS-ROM.
The purpose of this study was to evaluate the measurement properties of an accelerometer sensor vs. a mobile phone device as measures of CS-ROM. Specifically, we sought to assess their within-day test–retest reliability and the parallel-forms reliability of the two measurement methods, as well as the within-day test–retest reliability of FHP. Furthermore, the association of CS-ROM with demographics, FHP, and other biomechanical respiratory measures, and the male–female differences in those measures, were examined.
4. Discussion
The first part of this study was a reliability investigation, examining the within-day test-retest and parallel forms reliability of the KForce Sens
® electrogoniometer and the smartphone-based i-Handy Level app and the pre-installed Compass app. The reliability of the CVA measurement was also examined with the method of lateral photography, using the FHP app. No statistically significant differences were found within and between the measurements of the two devices, with a low error level for CS-ROM. The error level was slightly lower for the KFORCE SENS
® electrogoniometer in the current study; therefore, measurements for the whole cohort were conducted with this device. Excellent within-day reliability was also reported for CS-ROM measurement with the KFORCE SENS
® (ICC = 0.99 and SEM = 1.20–2.28 %) in a group of healthy young participants [
28]. In agreement with this study, several studies indicate that smartphone apps, such as the "compass" [
49,
50,
51] and the "clinometer" [
49,
52], constitute an accessible, economical, and practical method and possess satisfactory reliability and validity for the quantification of CS-ROM in the frontal, transverse and sagittal planes within clinical settings, when compared with gravitational inclinometers.
In contrast to our results, a previous study concluded that clinical assessments of head posture and cervical mobility in adults with neck pain and associated conditions (grades I–III) do not have adequate evidence to support their reliability and validity [
53]. Another previous investigation conducted in patients with NP, although reporting a high degree of intra-rater reliability for the Android-based clinometer in the assessment of all cervical movements, found a notable exception of rotation, which exhibited poor to moderate level of reliability [
49]. In another study that quantified CS-ROM in a cohort of healthy individuals [
54], the Android clinometer application demonstrated excellent intra-rater reliability for cervical flexion, extension, and lateral flexion (ICC = 0.82–0.90), but it was poor for R and L rotation (ICC = 0.05–0.33)—a finding that partly aligns with the results of our present study.
In a study utilizing the KForce Sens
® electrogoniometer in 60 healthy adults aged 19–24 years, females had significantly higher CS-ROM in extension and lateral flexion than males (
p < 0.05) [
28]. Conversely, our research revealed that females with NSCNP demonstrated greater CS-ROM in flexion and left rotation compared to males (
p < 0.05). The difference in study populations between the two studies is most likely responsible for the differences noted. We chose to use only three repetitions for each test direction to reduce patient assessment time, thus lowering the chances of them becoming tired or being in pain, which is in line with the two earlier studies that used the KForce Sens
® electrogoniometer for CS-ROM assessment [
28,
55]. This contrasts with earlier research that advocated for two [
56], five [
49], or six [
57] repetitions per test direction as the benchmark for optimal data acquisition. The difference between the current study and the one by Batatolis et al. 2023 [
28] is that, in the latter, the highest of the three measurements was selected, whereas in this study, the average of the three was taken to determine the CS-ROM per movement direction. Differences also existed in the measurement procedure, such as the application of a belt to stabilize the thoracic spine, which was not used in this and our previous study [
55], as well as the fact that participants were not leaning against the backrest.
Further differences can be observed between the previous reliability and validity studies of smartphone apps, such as the ‘compass’ and ‘clinometer’ in the measurement method. In most studies, examiners appear to touch and hold the mobile phone in contact with participants’ heads, and the neutral head position was visually adjusted by the examiners before the initiation of each set of measurements [
49,
50,
58]. However, this methodological approach may have introduced measurement inaccuracies stemming from inconsistencies in the initial positioning across all experimental trials. The study by Saptute et al. 2019 [
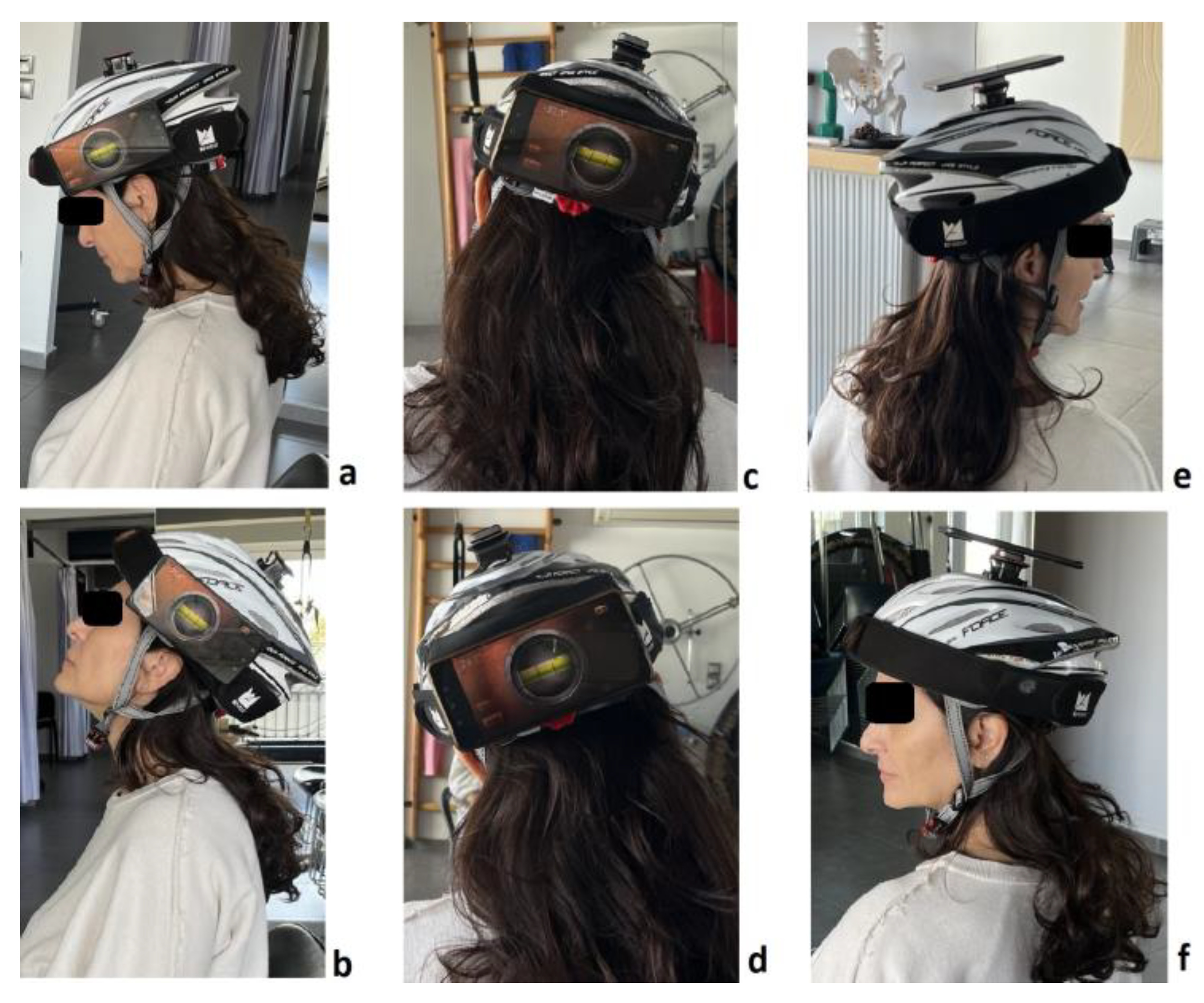
51] is an exception, as they used elasticated Velcro straps to secure the mobile phone to the participants’ heads. However, in that specific study, the researchers only evaluated rotation in the transverse plane. Conversely, in our study, the mobile phone was firmly attached to a magnet on the side (for sagittal-plane measurement), the back (for frontal-plane measurement), or the top (for transverse-plane measurement) of a helmet that was fitted tightly on participants’ heads.
The excellent reliability of the CVA measurement with low measurement error concurs with several previous studies conducted with the lateral photography method [
29,
59,
60]. The CVA measurement in previous studies was either conducted with the Auto CAD [
29], the Surgimap software [
61,
62], or with the FHP app [
60], the latter also being used in our study.
Our study further confirms the correlation between age and CS-ROM in five (except for flexion) out of the six movement directions (
Table 6) but not with the other demographic characteristics (height, weight, BMI) or with leisure-time physical activity, as measured with a validated brief scale [
63]. In accordance with our study, Liu et al. 2015 mention that the regression coefficient for age was determined to be −6.46, indicating an inverse relationship whereby the total ROM decreased by 6.46° for each subsequent decade of life [
64]. Specifically, the mean (SD) total ROM in the third decade was 81.49 (14.27)°, which diminished to 53.37 (12.86)° by the eighth decade. Also, Park et al. 2021 mention that age was related only to cervical lateral flexion on both sides (R side: r = −0.423,
p < 0.05; L side: −0.448,
p < 0.05) [
65], and Quek et al. 2013 [
56] mentioned that increased age (60–78 years) was associated with reduced total (Spearman’s R = −0.42,
p < 0.01) and upper (Spearman R = −0.51,
p < 0.01) cervical rotation ROM. There was also a significant effect between self-reported leisure-time physical activity [
63] and the CVA, specifically between the CVA of subjects reporting a low level of physical activity and those reporting a high level of physical activity (between-group mean difference (MD) [95% CI] of −5.99° [−11.45 to −0.50]). A similar finding has been previously reported by a research study in healthy young adults with a between-group mean difference of 3.57° [
66]; however, it had not reached statistical significance, possibly because in that study subjects were younger and the CVA was measured in standing.
The second aim of our study was to examine the associations of aspects of the biomechanical dimension of DB (CWE, Hi-Lo Breathing Assessment, RR) with biomechanical measures of NSCNP, such as CVA, and CS-ROM.
Most participants (81 out of 90) were classified in the Hi group based on their breathing pattern (
Table 4), possibly because our study sample consisted of patients with chronic neck pain. The overwhelming majority of participants classified as having the Hi rather than the Lo breathing pattern has been previously reported [
16,
66,
67]. Consequently, it appears physiologically plausible that these patients had adopted an apical breathing pattern (Hi). This interpretation is further supported by many observational studies [
16,
41,
67,
68].
Additionally, a statistically significant difference was observed between participants with a different breathing pattern, specifically those exhibiting a Hi breathing pattern having a lower CWE-Up. This finding is perplexing, as one might have expected participants with a Hi respiratory pattern to have a higher CWE-Up. A potential explanation for this observation, other than being a ‘statistical anomaly’, could be that CWE is assessed during maximal inhalation and exhalation, whereas the Hi-Lo assessment evaluates the participants’ breathing pattern during quiet breathing. Furthermore, the age, sex, and BMI of participants did not differ between participants with Hi and Lo breathing patterns (
Table 4); therefore, these variables might not have contributed to this finding. In addition, participants with a Hi breathing pattern demonstrated a statistically significant lower extension CS-ROM compared to those with a Lo breathing pattern. This finding, combined with the positive association between CS-ROM extension and CVA (
Table 4), possibly indicates that the adoption of an FHP combined with an increased tension in certain cervicothoracic extensors, sternocleidomastoid, scalene, and anterior chest muscles [
41] may lead to the decreased extension of the middle and lower part of the cervical spine in subjects with a Hi breathing pattern. However, we did not identify any similar studies comparing CS-ROM in patients with a Hi vs. Lo breathing pattern.
Furthermore, a trend towards an elevated RR was noted in the Hi compared to the Lo group. While this difference was statistically significant, it is pertinent to consider that the study population comprised individuals with musculoskeletal rather than primary respiratory conditions. Consequently, substantially greater RR values (over 18 breaths/min) would not necessarily be anticipated. Our study findings on RR number align with the findings of Stephen et al. (2022), who investigated the relationship between neck pain and dysfunctional breathing in a cohort study of 49 participants with neck pain and a control group of 49 individuals matched for age and sex [
69]. Their results indicated a comparable RR number between participants with (Mean (SD) 15.0 (3.6), Min–Max 9–24 breaths/min) and without neck pain (Mean (SD) 14.7 (3.1), Min–Max 7–20 breaths/min). However, in that study [
69], the majority of participants reported low levels of pain intensity. On the contrary, a case series by McLaughlin in 2011 [
67], involving twenty-nine outpatients with neck pain (
n = 12), back pain (
n = 8), or both (
n = 9), who had experienced symptoms for a considerable duration (median 24 months, mean 38 months), identified poor breathing profiles characterized by an RR of 20 breaths/min. Also, another study with 29 females with chronic shoulder/neck pain (mean age 48.3 years, mean (SD) pain duration 8 (8) years, and mean (SD) RR of 17 ± 3 breaths/min) and 35 healthy female controls (mean age 41.1 years and mean (SD) RR of 15 ± 3 breaths/min) reported that the between-group difference in RR was statistically significant [
70]. In our population, the mean pain duration was much lower (6.39 months on average) than that those two aforementioned studies. Therefore, there may be variability inherent in the breathing responses to pain, influenced by a multitude of factors, encompassing the specific context, the duration of symptoms and the individual emotional reaction to the nociceptive experience [
71].
Finally, a statistically significant positive correlation was observed between CVA and CWE-Up (
R = 0.29,
p = 0.01), as well as between CVA and extension CS-ROM (
R = 0.29,
p = 0.01). In agreement with our own study, the study by Lau et al. (2011) demonstrated a correlation between CWE and FHP [
72], possibly denoting a functional inter-connection between the cervical and thoracic spine. However, in contrast to our study, the study by Ozge Solakoglou et al. [
73] did not demonstrate any correlation between CWE and FHP in patients with chronic neck pain. Furthermore, CWE correlated significantly with all neck ROM (r = 0.39–0.59) in the study of Wirth et al. 2014 [
15] in patients with chronic neck pain, but no such correlations were observed in our study. Differences in population and methodological approaches between studies may have accounted for these disparities.
In summary, the findings of this study suggest that in the context of NSCNP of not particularly prolonged pain duration, an apical breathing pattern (Hi classification) appears to be prevalent. Other possible explanations for participants’ adopting a Hi breathing pattern may have been a sedentary way of life, reduced physical activity [
16], smoking habits (frequency and duration), or central-type obesity [
74] (that might be restricting diaphragmatic excursion); however, our findings show that there was no effect of self-reported physical activity, smoking frequency, age, and BMI on breathing pattern. Also, the presence of FHP appears to be associated with a limitation in cervical extension, potentially due to an extended upper cervical spine posture coupled with the straightening and flexion of the middle and lower cervical segments. Additionally, FHP appears to be associated both with CWE-Up and CWE-Lw, with the link between those measures perhaps being that the smaller the CVA (the more FHP), the more reduced the CS-ROM (extension and left lateral flexion), allowing for less expansion of the thoracic cage [
54].
Among the limitations of our study are that we only measured the within-day test–retest reliability of CS-ROM and CVA using a sample of convenience from a single physical therapy practice. We also did not measure other variables related to the biomechanical/neuromotor control aspects of neck pain, such as neck muscle strength, endurance, proprioception, and thoracic spine ROM, which would have perhaps enhanced the clinical profile of patients with NSCNP, possibly providing some further explanations on the interconnections between variables.
Regarding future avenues of investigation, we are focused on the administration of the Hi-Lo assessment from multiple testing positions, alongside the Lateral Rib Expansion (LRE) test, in the evaluation of breathing pattern dysfunction, to furnish the clinician with a more comprehensive evaluation of respiratory mechanics, as recommended [
37]. Furthermore, the reliability of the measures examined could be expanded by examining their between-days inter-examiner reliability, as well as their responsiveness, in future studies. The findings of this study could potentially contribute to the evaluation of additional clinical measures, like neuromuscular control tests. This may assist in identifying knowledge gaps and guide future research endeavors.


 ,
, 




{kind=link}
{kind=link}
{kind=link}