1. Introduction
Postural stability is essential for maintaining balance and proper body biomechanics. It is influenced by several factors, including the function of the deep core muscle system, sensory integration, and motor control. In recent years, there has been growing interest in innovative approaches to sports training, rehabilitation, and physiotherapy, with virtual reality emerging as one such method. This technology offers new opportunities for enhancing muscle activity and delivering therapeutic interventions through immersive therapy, which can effectively stimulate the deep core musculature. The deep core muscle system plays a crucial role in spinal stabilization and maintaining correct posture [
1]. Dysfunction in this system may result in impaired balance, musculoskeletal pain, and an increased risk of falls [
1,
2,
3]. Traditional methods of strengthening deep muscles include stabilization exercises, training on unstable surfaces, and proprioceptive training [
4,
5,
6]. Novel technological solutions, such as VR, allow for a more interactive and potentially more effective approach to core training.
The interactive and immersive nature of virtual reality can enhance patient motivation and improve adherence to training or rehabilitation protocols [
7]. VR technology enables users to experience presence within a computer-generated three-dimensional virtual environment so realistically that they may perceive themselves to be physically part of it [
8,
9]. Simulated environments created through VR can provide varying degrees of perceived realism and presence. The more realistic the virtual environment appears to the user, the more intense the immersive experience becomes. This experience depends on the number of physiological senses stimulated, the level of interaction with the virtual environment, and the degree of isolation from external stimuli, such as light or ambient noise [
10].
In physiotherapy, VR has also been proven to be an effective tool for managing acute pain [
11]. In the treatment of chronic patients, it can be utilized for cognitive rehabilitation, by applying principles of cognitive–behavioral therapy [
12]. Furthermore, the positive effects of VR-based kinesiotherapy have been demonstrated in the re-education of balance skills and gait patterns in individuals diagnosed with multiple sclerosis, Parkinson’s disease, stroke, and spinal cord injuries [
13,
14,
15,
16].
Several studies have confirmed that exposure to virtual reality (VR) may induce VR sickness, characterized by symptoms such as nausea, disorientation, a sense of instability, and impaired balance [
17]. According to current evidence, no studies have specifically investigated the effects of plank-position exercises in VR on the function of the deep core muscle system, using the Icaros
® device.
Since no prior study has been published on the effects of exercising using the Icaros® system, in combination with virtual reality (VR), and based on the existing findings related to VR-induced symptoms, such as motion sickness, we decided to conduct an initial investigation into the effects of this type of exercise in VR on individuals without any diagnosed medical conditions. This approach will allow us to assess how this combined therapy affects the human body and motor control immediately after exercise in healthy individuals. The results can then be used to adapt and tailor the exercise protocols for patients with specific diagnoses, as well as to identify which conditions are suitable for this form of exercise.
The aim of this study is to analyze the impact of deep core muscle activation during virtual reality exercise on selected posturographic parameters in healthy individuals immediately after training. The main motivation for conducting this study was the recurrent reports of instability and dizziness observed in previous clients following their first VR training session on the Icaros® system. This research explores the potential and applicability of VR in clinical practice, with findings that may contribute to a better understanding of the influence of VR on postural control.
3. Results
By evaluating the parameters, we can demonstrate the impact of deep core muscle training on the Icaros® therapeutic device in virtual reality on motor stability and coordination of the body after therapy. These parameters were analyzed across the entire sample of participants and, subsequently, evaluated separately for males and females.
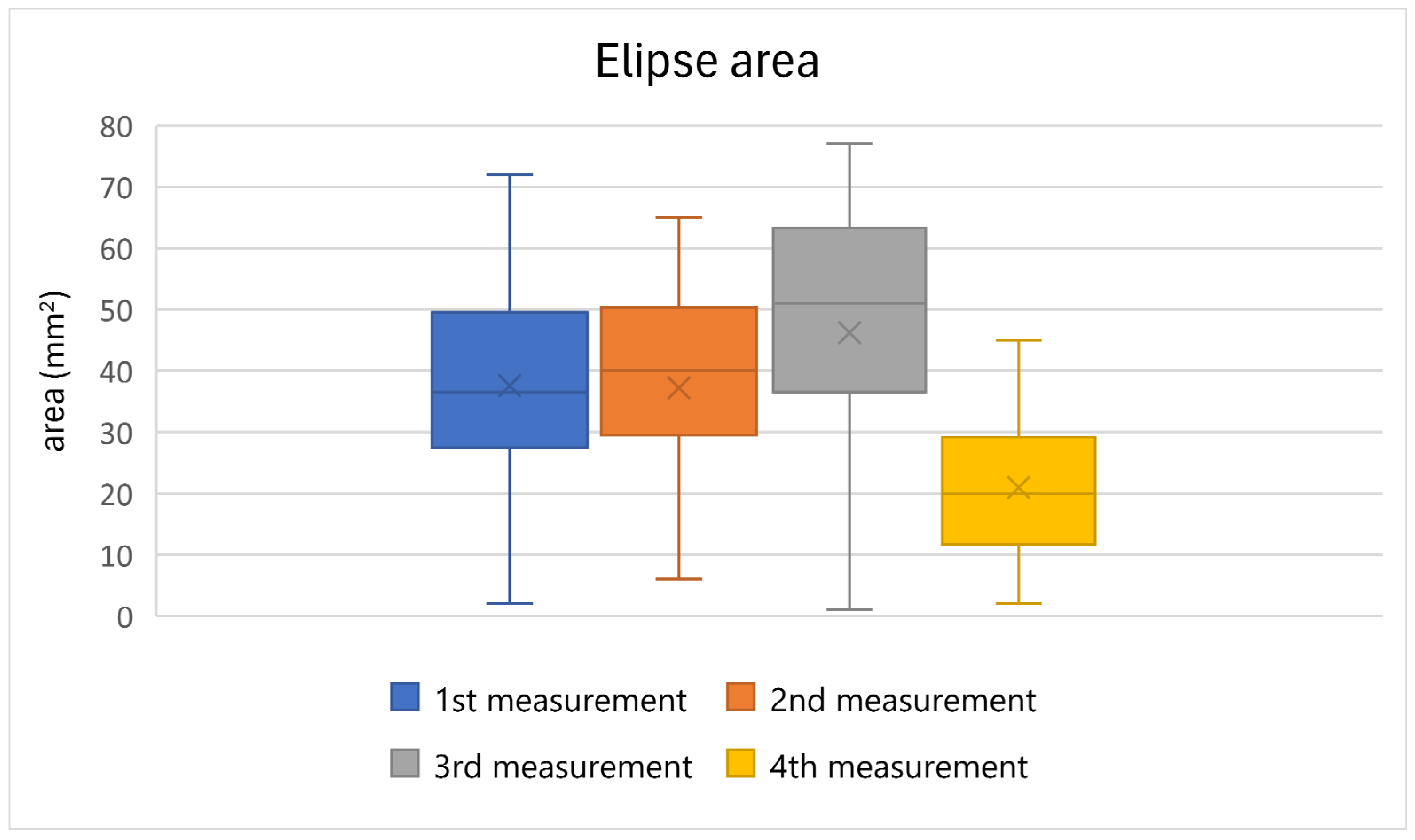
Table 2 presents the results of the statistical evaluation of the selected posturographic parameter, ellipse area, for all the participants. The results indicate a deterioration of this parameter during the first, second, and third measurements. In the final measurement, taken 15 min after the completion of the therapy on the Icaros
® VR system, a decrease in ellipse area values was observed. The results are supported by a statistically significant value (
p ≤ 0.05), indicating a significant difference between the measurements. A graphical representation of the results is shown in
Figure 4.
Table 3 presents the results of the post hoc analysis for the ellipse area parameter. This analysis compares the individual measurements and evaluates statistically significant differences. Significant differences were observed when comparing the 1st, 2nd, and 3rd measurements with the 4th measurement. No statistically significant differences were found between the remaining measurements.
Table 4 provides the results of a basic statistical evaluation of the ellipse area parameter, involving a comparison between the different genders. The results indicate that the average values of this parameter are higher in males, suggesting that the male population may require a longer period to stabilize the observed parameters and reduce the sensation of instability.
Table 5 presents the results of the statistical evaluation of the selected posturographic parameter, traveled distance, for all the participants. The values of this parameter showed a slight deterioration in the first three measurements, as demonstrated by the median values. Improvement and stabilization occurred in the fourth and final measurement, during which the participants also reported feeling subjectively more stable. The results are supported by a statistically significant value (
p ≤ 0.05), indicating a significant difference between the measurements. A graphical representation of the results is provided in
Figure 5.
Table 6 presents the results of the post hoc analysis of the traveled distance parameter. This analysis compares the individual measurements with each other and evaluates the statistically significant differences observed when comparing the 1st, 2nd, and 3rd measurements with the 4th. No statistically significant differences were observed when comparing the other measurements with each other.
Table 7 provides the results of a basic statistical evaluation of the traveled distance parameter when comparing men and women. The results suggest that the average values for this parameter are higher in men, which implies that the male population overall reacts to therapy using the Icaros
® system in VR with worsened coordination.
4. Discussion
In this study, we tested the response of a healthy human organism to the use of the Icaros
® system, combined with VR, immediately after exercise; a study that has not yet taken place. The statistical analysis of the obtained data confirmed that a 15 min training session on this system significantly affects the coordination and stability of a healthy person, causing one of the symptoms of VR sickness. After completing the training on Icaros
®, the participants subjectively felt unstable, and this subjective assessment was confirmed by objective measurements taken by the pressure platform, which we performed four times, with 5 min breaks. Statistically significant differences were observed for both monitored parameters, ellipse area (
p = 0.000) and traveled distance (
p = 0.000) (
Table 2 and
Table 5). In the detailed post hoc analysis, which aimed to determine the differences between the individual measurements, statistically significant differences were confirmed only when comparing the first, second, and third measurements with the fourth (
Table 3 and
Table 6). Similar results were observed in studies that recorded changes in static balance after playing VR games with a fixed or non-fixed background, where significant deterioration in balance was observed [
24]. In our study, the exercise was performed during a VR game with a non-fixed background, which may have contributed to the deterioration of the participant’s stability after exercise.
A variety of VR systems are utilized globally, particularly in rehabilitation, sports, and fitness environments [
25]. In regard to rehabilitation, the primary focus is on neurorehabilitation for patients with neurological diagnoses (such as multiple sclerosis, Parkinson’s disease, or stroke), aimed at improving the overall quality of life and cognitive functions in elderly patients [
13,
14,
16,
18,
26]. Another major area where VR therapy is significantly utilized is in pain management [
8,
9,
10,
11,
27]. Athletes use VR systems due to the broad range of gaming scenarios and experiences available to enhance their performance and as injury prevention [
28,
29]. The advantage lies in the numerous active sports games that VR offers, which can engage individuals and, consequently, improve their physical health [
25,
30,
31,
32]. VR tools were also employed during the global COVID-19 pandemic, wherein athletes used them for training at home [
33]. However, there are studies that provide various training plans [
34,
35] or reference systems and methodological frameworks [
36] to prevent nausea, oculomotor deficits, disorientation, and VR sickness caused by using other VR systems [
37]. These studies, however, yield conflicting results.
Virtual reality (VR) sickness and its symptoms are mostly explained through two main theories: the sensory conflict theory and the postural instability theory. According to sensory conflict theory, motion sickness occurs due to a conflict between visual perception and signals from the vestibular system, leading to a perceptual mismatch [
38]. On the other hand, postural instability theory attributes the feeling of instability to difficulties in maintaining a stable body position [
39]. Beginners in virtual reality are, therefore, more likely to experience VR sickness symptoms, due to their lesser ability to maintain a stable posture. Based on these theories, several studies have been conducted to alleviate VR-induced sickness, often through the use of software solutions. One such approach involves visual effects. Groth et al. (2021) implemented techniques such as peripheral blur and narrowing of the field of view within the content, and the experimental results confirmed their effectiveness in reducing VR sickness [
40]. In a study by Nie et al. (2019), a dynamically changing blur effect was introduced in first-person perspective games, which, based on experimental data, proved to be an effective solution to reduce VR sickness [
41]. Another study presents design elements aimed at alleviating cybersickness, such as movement styles, panel placement, laser use, and the background of panels [
42].
The use of the Icaros
® system, combined with VR, has been shown to be an effective approach for training and therapy in terms of the deep muscular system. Furthermore, this training system significantly impacts the balance abilities and stability of healthy individuals immediately after the therapy. We hypothesize that the feeling of instability experienced by participants using the Icaros
® system is due to a combination of factors, as described by the theories on VR sickness, such as the initial VR experience, the use of VR goggles, prolonged engagement in the plank position, and the exercise involved in controlling the Icaros
® system. By engaging in the exercise using the Icaros
® system, in combination with VR, we influenced both components described in the theories of VR sickness symptoms. On one hand, the sensory component was affected by the use of VR goggles, wherein the participants were exposed to multiple sensory stimuli that could impact the function of their vestibular system. On the other hand, participants remained in the plank position throughout the exercise, which required significant activity from the deep muscular system, thus influencing the second theory related to postural instability. The prolonged stay in the plank position subjected the deep muscular system to demanding conditions, as the recommended duration for holding this position for healthy individuals aged 18–25 years typically ranges from 60 to 100 s [
43,
44].
An important question that remains is how real patients with specific diagnoses would respond to a similar exercise routine using this system, within a VR environment. Further research involving patients with neurological or musculoskeletal disorders, such as those with chronic low back pain, sciatica, or even those undergoing post-stroke rehabilitation, would be necessary to determine whether the therapeutic effect seen in healthy individuals translates to clinical populations. Additionally, examining the adaptation process to the plank position and VR could help in designing tailored therapies for different patient groups.


 ,
, 


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}