
Effects of Autologous Tenocyte Injection for Overuse and Degenerative Tendinopathies: A Systematic Review

 ,
,  ,
, 
 ,
,  ,
,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Protocol Design
2.2. Search Strategy
2.3. Study Selection
2.4. Data Extraction
2.5. Outcomes
2.6. Quality Assesment
3. Results
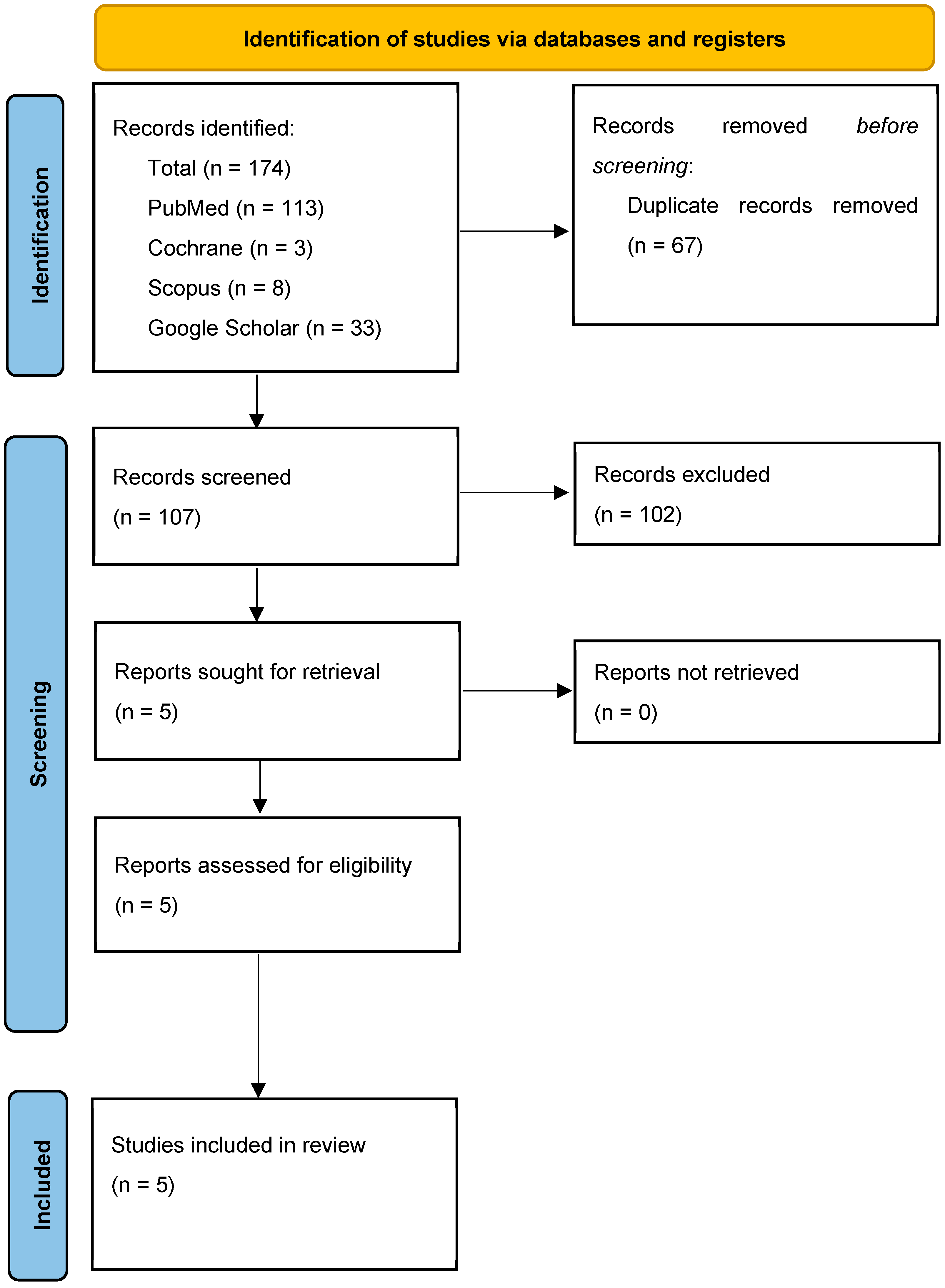
3.1. Study Selection
3.2. Characteristics of the Studies Included in the Review
3.3. Intervention Protocol
3.4. Side Effects
3.5. Outcome Measures Assessed
3.6. Pain
3.7. Function
3.8. MRI
3.9. Other Outcomes
3.10. Study Limitations
3.11. Study Quality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lin, T.W.T.W.; Cardenas, L.; Soslowsky, L.J.L.J. Biomechanics of tendon injury and repair. J. Biomech. 2004, 37, 865–877. [Google Scholar] [CrossRef] [PubMed]
- Millar, N.L.; Silbernagel, K.G.; Thorborg, K.; Kirwan, P.D.; Galatz, L.M.; Abrams, G.D.; Murrell, G.A.C.; McInnes, I.B.; Rodeo, S.A. Tendinopathy. Nat. Rev. Dis. Primer 2021, 7, 1. [Google Scholar] [CrossRef] [PubMed]
- Riley, G. Tendinopathy--from basic science to treatment. Nat. Clin. Pract. Rheumatol. 2008, 4, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Frizziero, A.; Maffulli, N.; Saglietti, C.; Sarti, E.; Bigliardi, D.; Costantino, C.; Demeco, A. A Practical Guide to Injection Therapy in Hand Tendinopathies: A Systematic Review of Randomized Controlled Trials. J. Funct. Morphol. Kinesiol. 2024, 9, 146. [Google Scholar] [CrossRef]
- Hopkins, C.; Fu, S.-C.; Chua, E.; Hu, X.; Rolf, C.; Mattila, V.M.; Qin, L.; Yung, P.S.-H.; Chan, K.-M. Critical review on the socio-economic impact of tendinopathy. Asia-Pac. J. Sports Med. Arthrosc. Rehabil. Technol. 2016, 4, 9–20. [Google Scholar] [CrossRef]
- Demeco, A.; de Sire, A.; Salerno, A.; Marotta, N.; Palermi, S.; Frizziero, A.; Costantino, C. Dry Needling in Overhead Athletes with Myofascial Shoulder Pain: A Systematic Review. Sports 2024, 12, 156. [Google Scholar] [CrossRef]
- Demeco, A.; Salerno, A.; Gusai, M.; Vignali, B.; Gramigna, V.; Palumbo, A.; Corradi, A.; Mickeviciute, G.C.; Costantino, C. The Role of Virtual Reality in the Management of Football Injuries. Medicina 2024, 60, 1000. [Google Scholar] [CrossRef]
- Demeco, A.; Bartocci, G.; Astore, N.; Vignali, B.; Salerno, A.; Palermi, S.; Foresti, R.; Martini, C.; Costantino, C. The Efficacy of Pelvic Floor Rehabilitation in the Treatment of Urinary Incontinence in Female Athletes: A Systematic Review. Sports 2024, 12, 338. [Google Scholar] [CrossRef]
- Niemiec, P.; Jarosz, A.; Nowak, T.; Balcerzyk-Matić, A.; Iwanicki, T.; Iwanicka, J.; Gawron, K.; Kalita, M.; Górczyńska-Kosiorz, S.; Kania, W.; et al. Impact of the COL1A1 Gene Polymorphisms on Pain Perception in Tennis Elbow Patients: A Two-Year Prospective Cohort Study. Int. J. Mol. Sci. 2024, 25, 13221. [Google Scholar] [CrossRef]
- Efficacy of Ultrasound-Guided Galvanic Electrolysis Technique and Physical Therapy in Patients with Achilles’ Tendinopathy: A Pilot Randomised Controlled Trial—IOS Press. Available online: https://content.iospress.com/articles/journal-of-back-and-musculoskeletal-rehabilitation/bmr230255 (accessed on 30 December 2024).
- Jarosz, A.; Nowak, T.; Szyluk, K.; Balcerzyk-Matić, A.; Iwanicki, T.; Iwanicka, J.; Kalita, M.; Gawron, K.; Kania, W.; Niemiec, P. The VEGFB Gene Variants and the Effectiveness of Platelet-Rich Plasma Treatment of Lateral Elbow Tendinopathy: A Prospective Cohort Study with a Two-Year Follow-Up. Int. J. Mol. Sci. 2024, 25, 13166. [Google Scholar] [CrossRef]
- Marotta, N.; de Sire, A.; Lippi, L.; Moggio, L.; Mondardini, P.; Sgro, M.; Bartalotta, I.; Zito, R.; Giroldini, T.; Invernizzi, M.; et al. Effectiveness of High-Power Laser Therapy via Shear Wave Speed Analysis on Pain and Functioning in Patients with Lateral Epicondylitis: A Proof-of-Concept Study. J. Clin. Med. 2024, 13, 2014. [Google Scholar] [CrossRef] [PubMed]
- Riel, H.; Lindstrøm, C.F.; Rathleff, M.S.; Jensen, M.B.; Olesen, J.L. Prevalence and incidence rate of lower-extremity tendinopathies in a Danish general practice: A registry-based study. BMC Musculoskelet. Disord. 2019, 20, 239. [Google Scholar] [CrossRef] [PubMed]
- Scott, A.; Zwerver, J.; Grewal, N.; de Sa, A.; Alktebi, T.; Granville, D.J.; Hart, D.A. Lipids, adiposity and tendinopathy: Is there a mechanistic link? Critical review. Br. J. Sports Med. 2015, 49, 984–988. [Google Scholar] [CrossRef]
- Abate, M.; Schiavone, C.; Salini, V.; Andia, I. Occurrence of tendon pathologies in metabolic disorders. Rheumatol. Oxf. Engl. 2013, 52, 599–608. [Google Scholar] [CrossRef]
- van der Vlist, A.C.; Breda, S.J.; Oei, E.H.G.; Verhaar, J.A.N.; de Vos, R.-J. Clinical risk factors for Achilles tendinopathy: A systematic review. Br. J. Sports Med. 2019, 53, 1352–1361. [Google Scholar] [CrossRef]
- September, A.; Rahim, M.; Collins, M. Towards an Understanding of the Genetics of Tendinopathy. Adv. Exp. Med. Biol. 2016, 920, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Vaughn, N.H.; Stepanyan, H.; Gallo, R.A.; Dhawan, A. Genetic Factors in Tendon Injury: A Systematic Review of the Literature. Orthop. J. Sports Med. 2017, 5, 2325967117724416. [Google Scholar] [CrossRef]
- Macedo, C.S.G.; Tadiello, F.F.; Medeiros, L.T.; Antonelo, M.C.; Alves, M.A.F.; Mendonça, L.D. Physical Therapy Service delivered in the Polyclinic During the Rio 2016 Paralympic Games. Phys. Ther. Sport Off. J. Assoc. Chart. Physiother. Sports Med. 2019, 36, 62–67. [Google Scholar] [CrossRef]
- Florit, D.; Pedret, C.; Casals, M.; Malliaras, P.; Sugimoto, D.; Rodas, G. Incidence of Tendinopathy in Team Sports in a Multidisciplinary Sports Club Over 8 Seasons. J. Sports Sci. Med. 2019, 18, 780–788. [Google Scholar]
- Francis, P.; Whatman, C.; Sheerin, K.; Hume, P.; Johnson, M.I. The Proportion of Lower Limb Running Injuries by Gender, Anatomical Location and Specific Pathology: A Systematic Review. J. Sports Sci. Med. 2019, 18, 21–31. [Google Scholar]
- Sanders, T.L.; Maradit Kremers, H.; Bryan, A.J.; Ransom, J.E.; Smith, J.; Morrey, B.F. The epidemiology and health care burden of tennis elbow: A population-based study. Am. J. Sports Med. 2015, 43, 1066–1071. [Google Scholar] [CrossRef] [PubMed]
- Abat, F.; Alfredson, H.; Cucchiarini, M.; Madry, H.; Marmotti, A.; Mouton, C.; Oliveira, J.M.; Pereira, H.; Peretti, G.M.; Spang, C.; et al. Current trends in tendinopathy: Consensus of the ESSKA basic science committee. Part II: Treatment options. J. Exp. Orthop. 2018, 5, 38. [Google Scholar] [CrossRef] [PubMed]
- Agostini, F.; de Sire, A.; Di Giacomo, G.; Paoloni, M.; Murgia, M.; Di Cesare, A.; Ammendolia, A.; Bernetti, A.; Mangone, M. Postural Evaluation and Risk of Musculoskeletal Injuries in Professional Male Rugby Players: A Proof-of-Principle Study. J. Sports Med. Phys. Fit. 2022, 62, 1675–1684. Available online: https://www.minervamedica.it/it/riviste/sports-med-physical-fitness/articolo.php?cod=R40Y2022N12A1675 (accessed on 30 December 2024). [CrossRef]
- Demeco, A.; de Sire, A.; Marotta, N.; Spanò, R.; Lippi, L.; Palumbo, A.; Iona, T.; Gramigna, V.; Palermi, S.; Leigheb, M.; et al. Match Analysis, Physical Training, Risk of Injury and Rehabilitation in Padel: Overview of the Literature. Int. J. Environ. Res. Public. Health 2022, 19, 4153. [Google Scholar] [CrossRef]
- de Sire, A.; Demeco, A.; Frizziero, A.; Marotta, N.; Spanò, R.; Carozzo, S.; Costantino, C.; Ammendolia, A. Risk of Injury and Kinematic Assessment of the Shoulder Biomechanics During Strokes in Padel Players: A Cross-Sectional Study. J. Sports Med. Phys. Fit. 2024, 64, 383–391. Available online: https://www.minervamedica.it/it/riviste/sports-med-physical-fitness/articolo.php?cod=R40Y2024N04A0383 (accessed on 30 December 2024). [CrossRef]
- Tran, P.H.T.; Malmgaard-Clausen, N.M.; Puggaard, R.S.; Svensson, R.B.; Nybing, J.D.; Hansen, P.; Schjerling, P.; Zinglersen, A.H.; Couppé, C.; Boesen, M.; et al. Early development of tendinopathy in humans: Sequence of pathological changes in structure and tissue turnover signaling. FASEB J. Off. Publ. Fed. Am. Soc. Exp. Biol. 2020, 34, 776–788. [Google Scholar] [CrossRef]
- Kannus, P.; Józsa, L. Histopathological changes preceding spontaneous rupture of a tendon. A controlled study of 891 patients. J. Bone Jt. Surg. Am. 1991, 73, 1507–1525. [Google Scholar] [CrossRef]
- de Sire, A.; Marotta, N.; Lippi, L.; Scaturro, D.; Farì, G.; Liccardi, A.; Moggio, L.; Letizia Mauro, G.; Ammendolia, A.; Invernizzi, M. Pharmacological Treatment for Acute Traumatic Musculoskeletal Pain in Athletes. Medicina 2021, 57, 1208. [Google Scholar] [CrossRef]
- Dakin, S.G.; Dudhia, J.; Smith, R.K.W. Resolving an inflammatory concept: The importance of inflammation and resolution in tendinopathy. Vet. Immunol. Immunopathol. 2014, 158, 121–127. [Google Scholar] [CrossRef]
- Crowe, L.A.N.; McLean, M.; Kitson, S.M.; Melchor, E.G.; Patommel, K.; Cao, H.M.; Reilly, J.H.; Leach, W.J.; Rooney, B.P.; Spencer, S.J.; et al. S100A8 & S100A9: Alarmin mediated inflammation in tendinopathy. Sci. Rep. 2019, 9, 1463. [Google Scholar] [CrossRef]
- Dakin, S.G.; Newton, J.; Martinez, F.O.; Hedley, R.; Gwilym, S.; Jones, N.; Reid, H.A.B.; Wood, S.; Wells, G.; Appleton, L.; et al. Chronic inflammation is a feature of Achilles tendinopathy and rupture. Br. J. Sports Med. 2018, 52, 359–367. [Google Scholar] [CrossRef] [PubMed]
- Langberg, H.; Olesen, J.L.; Gemmer, C.; Kjaer, M. Substantial elevation of interleukin-6 concentration in peritendinous tissue, in contrast to muscle, following prolonged exercise in humans. J. Physiol. 2002, 542, 985–990. [Google Scholar] [CrossRef] [PubMed]
- Brown, K.L.; Seale, K.B.; El Khoury, L.Y.; Posthumus, M.; Ribbans, W.J.; Raleigh, S.M.; Collins, M.; September, A.V. Polymorphisms within the COL5A1 gene and regulators of the extracellular matrix modify the risk of Achilles tendon pathology in a British case-control study. J. Sports Sci. 2017, 35, 1475–1483. [Google Scholar] [CrossRef]
- The Utility of Clinical Measures for the Diagnosis of Achilles Tendon Injuries: A Systematic Review with Meta-Analysis—PMC. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4264655/ (accessed on 27 June 2024).
- Wan, X.-H.; Zeng, R. Handbook of Clinical Diagnostics; Springer Nature: Berlin/Heidelberg, Germany, 2019; ISBN 9789811376771. [Google Scholar]
- Malliaras, P.; Cook, J.; Purdam, C.; Rio, E. Patellar Tendinopathy: Clinical Diagnosis, Load Management, and Advice for Challenging Case Presentations. J. Orthop. Sports Phys. Ther. 2015, 45, 887–898. [Google Scholar] [CrossRef]
- Taylor, S.A.; Hannafin, J.A. Evaluation and management of elbow tendinopathy. Sports Health 2012, 4, 384–393. [Google Scholar] [CrossRef]
- Docking, S.I.; Ooi, C.C.; Connell, D. Tendinopathy: Is Imaging Telling Us the Entire Story? J. Orthop. Sports Phys. Ther. 2015, 45, 842–852. [Google Scholar] [CrossRef]
- de Oliveira, L.N.; Durigan, J.L.Q.; Sanchez, C.R.; Mansur, H.; Rosa, A.B.B.; Marqueti, R. de C. MRI-Based Morphometric Comparison of Lower Leg Muscles and Tendons in Individuals With Medial Tibial Stress Syndrome. BioMed Res. Int. 2024, 2024, 8827692. [Google Scholar] [CrossRef] [PubMed]
- Jarosz, A.; Balcerzyk-Matić, A.; Iwanicka, J.; Iwanicki, T.; Nowak, T.; Szyluk, K.; Kalita, M.; Górczyńska-Kosiorz, S.; Kania, W.; Niemiec, P. Association between Platelet-Derived Growth Factor Receptor Alpha Gene Polymorphisms and Platelet-Rich Plasma’s Efficiency in Treating Lateral Elbow Tendinopathy—A Prospective Cohort Study. Int. J. Mol. Sci. 2024, 25, 4266. [Google Scholar] [CrossRef]
- The Bioinductive Collagen Implant Yields Positive Histological, Clinical and MRI Outcomes in the Management of Rotator Cuff Tears: A Systematic Review—Longo—Knee Surgery, Sports Traumatology, Arthroscopy—Wiley Online Library. Available online: https://esskajournals.onlinelibrary.wiley.com/doi/10.1002/ksa.12429 (accessed on 30 December 2024).
- Wu, K.-T.; Chen, P.-C.; Chou, W.-Y.; Chang, C.-D.; Lien, J.-J.J. Diagnostic Accuracy and Interobserver Reliability of Rotator Cuff Tear Detection with Ultrasonography are Improved with Attentional Deep Learning. Arthroscopy 2024, 24, S0749-8063(24)01088-0. [Google Scholar] [CrossRef]
- Lim, H.Y.; Wong, S.H. Effects of isometric, eccentric, or heavy slow resistance exercises on pain and function in individuals with patellar tendinopathy: A systematic review. Physiother. Res. Int. J. Res. Clin. Phys. Ther. 2018, 23, e1721. [Google Scholar] [CrossRef]
- Visnes, H.; Bahr, R. The evolution of eccentric training as treatment for patellar tendinopathy (jumper’s knee): A critical review of exercise programmes. Br. J. Sports Med. 2007, 41, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Maffulli, N.; Longo, U.G.; Loppini, M.; Denaro, V. Current treatment options for tendinopathy. Expert Opin. Pharmacother. 2010, 11, 2177–2186. [Google Scholar] [CrossRef]
- Rio, E.; Kidgell, D.; Purdam, C.; Gaida, J.; Moseley, G.L.; Pearce, A.J.; Cook, J. Isometric exercise induces analgesia and reduces inhibition in patellar tendinopathy. Br. J. Sports Med. 2015, 49, 1277–1283. [Google Scholar] [CrossRef]
- Andres, B.M.; Murrell, G.A.C. Treatment of Tendinopathy: What Works, What Does Not, and What is on the Horizon. Clin. Orthop. 2008, 466, 1539–1554. [Google Scholar] [CrossRef]
- Santilli, G.; Vetrano, M.; Mangone, M.; Agostini, F.; Bernetti, A.; Coraci, D.; Paoloni, M.; de Sire, A.; Paolucci, T.; Latini, E.; et al. Predictive Prognostic Factors in Non-Calcific Supraspinatus Tendinopathy Treated with Focused Extracorporeal Shock Wave Therapy: An Artificial Neural Network Approach. Life 2024, 14, 681. [Google Scholar] [CrossRef] [PubMed]
- Di Gesù, M.; Alito, A.; Borzelli, D.; Romeo, D.; Bonomolo, F.; Calafiore, D.; de Sire, A. Efficacy of ultrasound-guided galvanic electrolysis technique and physical therapy in patients with Achilles’ tendinopathy: A pilot randomised controlled trial. J Back Musculoskelet Rehabil. 2024, 37, 1177–1188. [Google Scholar] [CrossRef] [PubMed]
- Cotler, H.B.; Chow, R.T.; Hamblin, M.R.; Carroll, J. The Use of Low Level Laser Therapy (LLLT) For Musculoskeletal Pain. MOJ Orthop. Rheumatol. 2015, 2, 00068. [Google Scholar] [CrossRef]
- Rompe, J.D.; Nafe, B.; Furia, J.P.; Maffulli, N. Eccentric loading, shock-wave treatment, or a wait-and-see policy for tendinopathy of the main body of tendo Achillis: A randomized controlled trial. Am. J. Sports Med. 2007, 35, 374–383. [Google Scholar] [CrossRef]
- Rompe, J.D.; Maffulli, N. Repetitive shock wave therapy for lateral elbow tendinopathy (tennis elbow): A systematic and qualitative analysis. Br. Med. Bull. 2007, 83, 355–378. [Google Scholar] [CrossRef]
- Pitsilos, C.; Karachrysafi, S.; Fragou, A.; Gigis, I.; Papadopoulos, P.; Chalidis, B. The Biological Effect of Platelet-Rich Plasma on Rotator Cuff Tears: A Prospective Randomized In Vivo Study. Int. J. Mol. Sci. 2024, 25, 7957. [Google Scholar] [CrossRef]
- Agostini, F.; de Sire, A.; Paoloni, M.; Finamore, N.; Ammendolia, A.; Mangone, M.; Bernetti, A. Effects of hyaluronic acid injections on pain and functioning in patients affected by tendinopathies: A narrative review. J. Back Musculoskelet. Rehabil. 2022, 35, 949–961. [Google Scholar] [CrossRef]
- Zhou, Y.; Wang, J.H. PRP treatment efficacy for tendinopathy: A review of basic science studies. BioMed Res. Int. 2016, 2016, 9103792. [Google Scholar] [CrossRef] [PubMed]
- Rees, J.D.; Maffulli, N.; Cook, J. Management of Tendinopathy. Am. J. Sports Med. 2009, 37, 1855–1867. [Google Scholar] [CrossRef] [PubMed]
- Dean, B.J.F.; Lostis, E.; Oakley, T.; Rombach, I.; Morrey, M.E.; Carr, A.J. The risks and benefits of glucocorticoid treatment for tendinopathy: A systematic review of the effects of local glucocorticoid on tendon. Semin. Arthritis Rheum. 2014, 43, 570–576. [Google Scholar] [CrossRef]
- Gaujoux-Viala, C.; Dougados, M.; Gossec, L. Efficacy and safety of steroid injections for shoulder and elbow tendonitis: A meta-analysis of randomised controlled trials. Ann. Rheum. Dis. 2009, 68, 1843–1849. [Google Scholar] [CrossRef]
- Dadgostar, H.; Fahimipour, F.; Pahlevan Sabagh, A.; Arasteh, P.; Razi, M. Corticosteroids or platelet-rich plasma injections for rotator cuff tendinopathy: A randomized clinical trial study. J. Orthop. Surg. 2021, 16, 333. [Google Scholar] [CrossRef] [PubMed]
- Barker-Davies, R.M.; Nicol, A.; McCurdie, I.; Watson, J.; Baker, P.; Wheeler, P.; Fong, D.; Lewis, M.; Bennett, A.N. Study protocol: A double blind randomised control trial of high volume image guided injections in Achilles and patellar tendinopathy in a young active population. BMC Musculoskelet. Disord. 2017, 18, 204. [Google Scholar] [CrossRef]
- Schwab, L.M.; Blanch, P.; Young, M. Autologous tenocyte implantation into shoulder tendon pathology in an elite swimmer. Phys. Ther. Sport Off. J. Assoc. Chart. Physiother. Sports Med. 2018, 29, 19–25. [Google Scholar] [CrossRef]
- Wang, K.; Wang, A.; Cheng, T.S.; Landao-Bassonga, E.; Lee, C.; Tai, A.; Damiani, M.; Zheng, M.H. Impact of age and donor sites on bioactivities of tendon cells in autologous tenocyte implantation (OrthoATITM) for treatment of chronic tendinopathy. J. ISAKOS Jt. Disord. Orthop. Sports Med. 2024, 9, 603–608. [Google Scholar] [CrossRef]
- Bucher, T.A.; Ebert, J.R.; Smith, A.; Breidahl, W.; Fallon, M.; Wang, T.; Zheng, M.-H.; Janes, G.C. Autologous tenocyte injection for the treatment of chronic recalcitrant gluteal tendinopathy: A prospective pilot study. Orthop. J. Sports Med. 2017, 5, 2325967116688866. [Google Scholar] [CrossRef]
- PRISMA Statement. Available online: https://www.prisma-statement.org (accessed on 25 February 2025).
- Becky Alford, M. LibGuides: Evidence Based Medicine: PICO. Available online: https://mcw.libguides.com/EBM/PICO (accessed on 25 February 2025).
- Barker, T.H.; Stone, J.C.; Sears, K.; Klugar, M.; Leonardi-Bee, J.; Tufanaru, C.; Aromataris, E.; Munn, Z. Revising the JBI quantitative critical appraisal tools to improve their applicability: An overview of methods and the development process. JBI Evid. Synth. 2023, 21, 478–493. [Google Scholar] [CrossRef] [PubMed]
- Munn, Z.; Barker, T.H.; Moola, S.; Tufanaru, C.; Stern, C.; McArthur, A.; Stephenson, M.; Aromataris, E. Methodological quality of case series studies: An introduction to the JBI critical appraisal tool. JBI Database Syst. Rev. Implement. Rep. 2019, publish ahead of print. Available online: https://journals.lww.com/10.11124/JBISRIR-D-19-00099 (accessed on 4 July 2024). [CrossRef] [PubMed]
- Wang, A.W.; Bauer, S.; Goonatillake, M.; Breidahl, W.; Zheng, M.-H. Autologous tenocyte implantation, a novel treatment for partial-thickness rotator cuff tear and tendinopathy in an elite athlete. BMJ Case Rep. 2013, 2013, bcr2012007899. [Google Scholar] [CrossRef] [PubMed]
- Wang, A.; Breidahl, W.; MacKie, K.; Zhen, L.; Qin, A.; Chen, J.; Zheng, M. Autologous tenocyte injection (ati) for treatment of severe chronic resistant lateral epicondylitis: A pilot study. Intern. Med. J. 2013, 43, 32. [Google Scholar]
- Wang, A.; Mackie, K.; Breidahl, W.; Wang, T.; Zheng, M.H. Evidence for the Durability of Autologous Tenocyte Injection for Treatment of Chronic Resistant Lateral Epicondylitis: Mean 4.5-Year Clinical Follow-up. Am. J. Sports Med. 2015, 43, 1775–1783. [Google Scholar] [CrossRef]
- Gilmor, R.; Remily, E.A.; Ingari, J.V. Management of Lateral Epicondylosis. J. Hand Surg. 2024, 49, 1124–1128. [Google Scholar] [CrossRef]
- Bahadir, B.; Sarikaya, B. Platelet-rich plasma in the management of rotator cuff tendinopathy. Jt. Dis. Relat. Surg. 2024, 35, 462–467. [Google Scholar] [CrossRef]
- Maffulli, N.; Longo, U.G.; Loppini, M.; Spiezia, F.; Denaro, V. New options in the management of tendinopathy. Open Access J. Sports Med. 2010, 1, 29–37. [Google Scholar] [CrossRef]
- Carr, J.B. Editorial Commentary: Platelet-Rich Plasma Shows Promise for Improving Shoulder Tendinopathy. Arthroscopy 2021, 37, 2754–2755. [Google Scholar] [CrossRef]
- Balasubramaniam, U.; Dissanayake, R.; Annabell, L. Efficacy of platelet-rich plasma injections in pain associated with chronic tendinopathy: A systematic review. Phys. Sportsmed. 2015, 43, 253–261. [Google Scholar] [CrossRef]
- Johannsen, F.; Olesen, J.L.; Øhlenschläger, T.F.; Lundgaard-Nielsen, M.; Cullum, C.K.; Jakobsen, A.S.; Rathleff, M.S.; Magnusson, P.S.; Kjær, M. Effect of Ultrasonography-Guided Corticosteroid Injection vs Placebo Added to Exercise Therapy for Achilles Tendinopathy. JAMA Netw. Open 2022, 5, e2219661. [Google Scholar] [CrossRef] [PubMed]
- Mellor, R.; Bennell, K.; Grimaldi, A.; Nicolson, P.; Kasza, J.; Hodges, P.; Wajswelner, H.; Vicenzino, B. Education plus exercise versus corticosteroid injection use versus a wait and see approach on global outcome and pain from gluteal tendinopathy: Prospective, single blinded, randomised clinical trial. BMJ 2018, 361, k1662. [Google Scholar] [CrossRef]
- Moosmayer, S.; Ekeberg, O.M.; Hallgren, H.B.; Heier, I.; Kvalheim, S.; Juel, N.G.; Blomquist, J.; Pripp, A.H.; Brox, J.I. Ultrasound guided lavage with corticosteroid injection versus sham lavage with and without corticosteroid injection for calcific tendinopathy of shoulder: Randomised double blinded multi-arm study. BMJ 2023, 383, e076447. [Google Scholar] [CrossRef]
- ACTRN12617000684325. Defining a Randomised, Controlled Study of Ortho-ATI (Trademark) vs. Corticosteroid Injection for Treatment of Rotator Cuff Tendinopathy and Tear. 2019. Available online: https://trialsearch.who.int/Trial2.aspx?TrialID=ACTRN12617000684325; (accessed on 29 April 2024).
- Kholinne, E.; Singjie, L.C.; Anastasia, M.; Liu, F.; Anestessia, I.J.; Kwak, J.-M.; Jeon, I.-H. Comparison of Clinical Outcomes After Different Surgical Approaches for Lateral Epicondylitis: A Systematic Review and Meta-analysis. Orthop. J. Sports Med. 2024, 12, 23259671241230292. [Google Scholar] [CrossRef] [PubMed]
- Burn, M.B.; Mitchell, R.J.; Liberman, S.R.; Lintner, D.M.; Harris, J.D.; McCulloch, P.C. Open, Arthroscopic, and Percutaneous Surgical Treatment of Lateral Epicondylitis: A Systematic Review. Hand 2018, 13, 264–274. [Google Scholar] [CrossRef] [PubMed]
- Loppini, M.; Maffulli, N. Conservative management of tendinopathy: An evidence-based approach. Muscles Ligaments Tendons J. 2012, 1, 134–137. [Google Scholar] [PubMed]
- Čobec, J.; Kozinc, Ž. Conservative Treatments for Patellar Tendinopathy: A Review of Recent High-Quality Evidence. BioMed 2022, 2, 359–375. [Google Scholar] [CrossRef]
- Bruno, F.; Palumbo, P.; Arrigoni, F.; Mariani, S.; Aringhieri, G.; Carotti, M.; Natella, R.; Zappia, M.; Cipriani, P.; Giacomelli, R.; et al. Advanced diagnostic imaging and intervention in tendon diseases. Acta Bio Medica Atenei Parm. 2020, 91, 98–106. [Google Scholar] [CrossRef]
- Weinreb, J.H.; Sheth, C.; Apostolakos, J.; McCarthy, M.-B.; Barden, B.; Cote, M.P.; Mazzocca, A.D. Tendon structure, disease, and imaging. Muscles Ligaments Tendons J. 2014, 4, 66–73. [Google Scholar] [CrossRef]

{kind=link}
| PUBMED: |
| (autologous tenocyte injection OR autologous tenocyte implant) AND (tendon OR tendinopathy) AND treatment |
| SCOPUS: |
| (TITLE-ABS ((autologous tenocyte injection OR autologous tenocyte implant) AND (tendon OR tendinopathy) AND treatment) |
| WEB OF SCIENCE: |
| (autologous tenocyte injection OR autologous tenocyte implant) AND (tendon OR tendinopathy) AND treatment |
| Article | Nation | Population | Intervention | Outcomes | Results |
|---|---|---|---|---|---|
| Wang et al., 2013 [69] | Australia | n = 1; Age: 20; Diagnosis: Increased tendon size associated with a partial-thickness supraspinatus rim-rent tear with fluid signal; Symptom duration: 3 y | Tenocytes were obtained from the patient’s patellar tendon. Three weeks later, 2 mL of tenocyte suspension was administered under ultrasound guidance. | At 10 months: VAS pain, Oxford Shoulder Score, and QuickDASH with sports module). At four and ten months post-ATI, control with 3 Tesla MRIs. | At 4 and 10 months, the athlete reported no pain, and the partial-thickness rim-rent tear had healed, becoming undetectable. |
| Wang et al., 2013 [70] | Australia | n = 20 (11M/9F); Age: 49.4 ± 7.69, range, 37–63; Diagnosis: refractory lateral epicondylitis; Symptom duration: ≥6 months | Patients received a single injection of autologous tenocytes at the extensor carpi radialis brevis tendon under ultrasound guidance and local anesthetic. | VAS for pain, quick Disabilities of the Arm, Shoulder, and Hand (QuickDASH), and grip strength measurements before and after ATI at one, two, three, six, and twelve months. At 12 months, these were also evaluated via MRI. | ATI treatment resulted in significant improvements across pain, function, strength, and MRI findings within 12 months: |
| Wang et al., 2015 [71] | Australia | n = 16 (9M/7F); Age: 47.76 ± 1.79 years, range, 37–63 years; Diagnosis: chronic lateral epicondylitis; Symptom duration: 29.24 ± 14.26 (6–240) mo; Follow-up duration: 4.06 ± 0.33 (0.5–5) y. | 2 mL of autologous tenocytes was injected into the extensor carpi radialis brevis under ultrasound guidance. | QuickDASH, UEFS, VAS, and dynamometer. Patient satisfaction was evaluated on a scale of 0 to 10 at final follow-up. The MRI assessment was performed at T0 and after twelve months. | ATI treatment demonstrated significant improvements in pain, function, strength, and MRI findings, with high patient satisfaction. |
| Bucher et al., 2017 [64] | Australia | n = 12 (0M/12F); Age: mean 52.6 y (range, 41–67 y); Diagnosis: symptomatic gluteal tendinopathy; Symptom duration: 33 m (range, 6–144 m). | Single tenocyte injection was injected into the tendinopathic area, under ultrasound guidance. | OHS, VAS, SF-36, and patient satisfaction (evaluated on a scale of 0 to 7). All outcomes were evaluated at T0 and after three, six, twelve, and twenty-four months. | Autologous tenocyte injection resulted in significant clinical improvements in pain, function, and physical health over 12–24 months but did not show significant changes in tendon features on MRI. |
| Schwab et al., 2018 [62] | Australia | n = 1 (M); Age: 28 y; Diagnosis: anterior/lateral shoulder pain surrounding the deltoid tubercle; Symptom duration: 2 months | Three 1 mL vials containin g a total of 5 × 106 tenocytes were injected into the subscapularis tendon under ultrasound guidance. | MRI images after seven and eighteen months | An MRI showed a marked decrease in tear size and an improvement in tendon morphology. Futhermore, athletes returned to complete training. |
| Wang, 2013 [69] | Schwab, 2018 [62] | |
|---|---|---|
| Were patient’s demographic characteristics clearly described? | Y | Y |
| Was the patient’s history clearly described and presented as a timeline? | U | Y |
| Was the current clinical condition of the patient on presentation clearly described? | Y | Y |
| Were diagnostic tests or assessment methods and the results clearly described? | Y | Y |
| Was the intervention(s) or treatment procedure(s) clearly described? | Y | Y |
| Was the post-intervention clinical condition clearly described? | Y | Y |
| Were adverse events (harms) or unanticipated events identified and described? | N | N |
| Does the case report provide takeaway lessons? | Y | Y |
| Inclusion? | Y | Y |
| Wang, 2013 [69] | Wang, 2015 [71] | Bucher, 2017 [64] | |
|---|---|---|---|
| Were there clear criteria for inclusion in the case series? | Y | Y | Y |
| Was the condition measured in a standard, reliable way for all participants included in the case series? | Y | Y | Y |
| Were valid methods used for identification of the condition for all participants included in the case series? | Y | Y | Y |
| Did the case series have consecutive inclusion of participants? | N | N | Y |
| Did the case series have complete inclusion of participants? | U | U | Y |
| Was there clear reporting of the demographics of the participants in the study? | Y | Y | N |
| Was there clear reporting of clinical information of the participants? | U | U | U |
| Were the outcomes or follow-up results of cases clearly reported? | Y | Y | Y |
| Was there clear reporting of the presenting site(s)/clinic(s) demographic information? | Y | Y | Y |
| Was statistical analysis appropriate? | Y | Y | Y |
| Inclusion? | Y | Y | Y |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Demeco, A.; de Sire, A.; Salerno, A.; Marotta, N.; Comuni, B.; Gabbi, M.; Lippi, L.; Invernizzi, M.; Ammendolia, A.; Costantino, C. Effects of Autologous Tenocyte Injection for Overuse and Degenerative Tendinopathies: A Systematic Review. J. Funct. Morphol. Kinesiol. 2025, 10, 95. https://doi.org/10.3390/jfmk10010095
Demeco A, de Sire A, Salerno A, Marotta N, Comuni B, Gabbi M, Lippi L, Invernizzi M, Ammendolia A, Costantino C. Effects of Autologous Tenocyte Injection for Overuse and Degenerative Tendinopathies: A Systematic Review. Journal of Functional Morphology and Kinesiology. 2025; 10(1):95. https://doi.org/10.3390/jfmk10010095
Chicago/Turabian StyleDemeco, Andrea, Alessandro de Sire, Antonello Salerno, Nicola Marotta, Beatrice Comuni, Matteo Gabbi, Lorenzo Lippi, Marco Invernizzi, Antonio Ammendolia, and Cosimo Costantino. 2025. "Effects of Autologous Tenocyte Injection for Overuse and Degenerative Tendinopathies: A Systematic Review" Journal of Functional Morphology and Kinesiology 10, no. 1: 95. https://doi.org/10.3390/jfmk10010095
APA StyleDemeco, A., de Sire, A., Salerno, A., Marotta, N., Comuni, B., Gabbi, M., Lippi, L., Invernizzi, M., Ammendolia, A., & Costantino, C. (2025). Effects of Autologous Tenocyte Injection for Overuse and Degenerative Tendinopathies: A Systematic Review. Journal of Functional Morphology and Kinesiology, 10(1), 95. https://doi.org/10.3390/jfmk10010095