

Presence of Pain Shows Greater Effect than Tendon Structural Alignment During Landing Dynamics

 , ,
, ,  , , , , ,
, , , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Inclusion/Exclusion Criteria
2.3. Outcome Measures
2.4. Procedure
2.5. Sample Size Calculation
2.6. Statistical Analysis
3. Results
3.1. Joint Kinematic Data
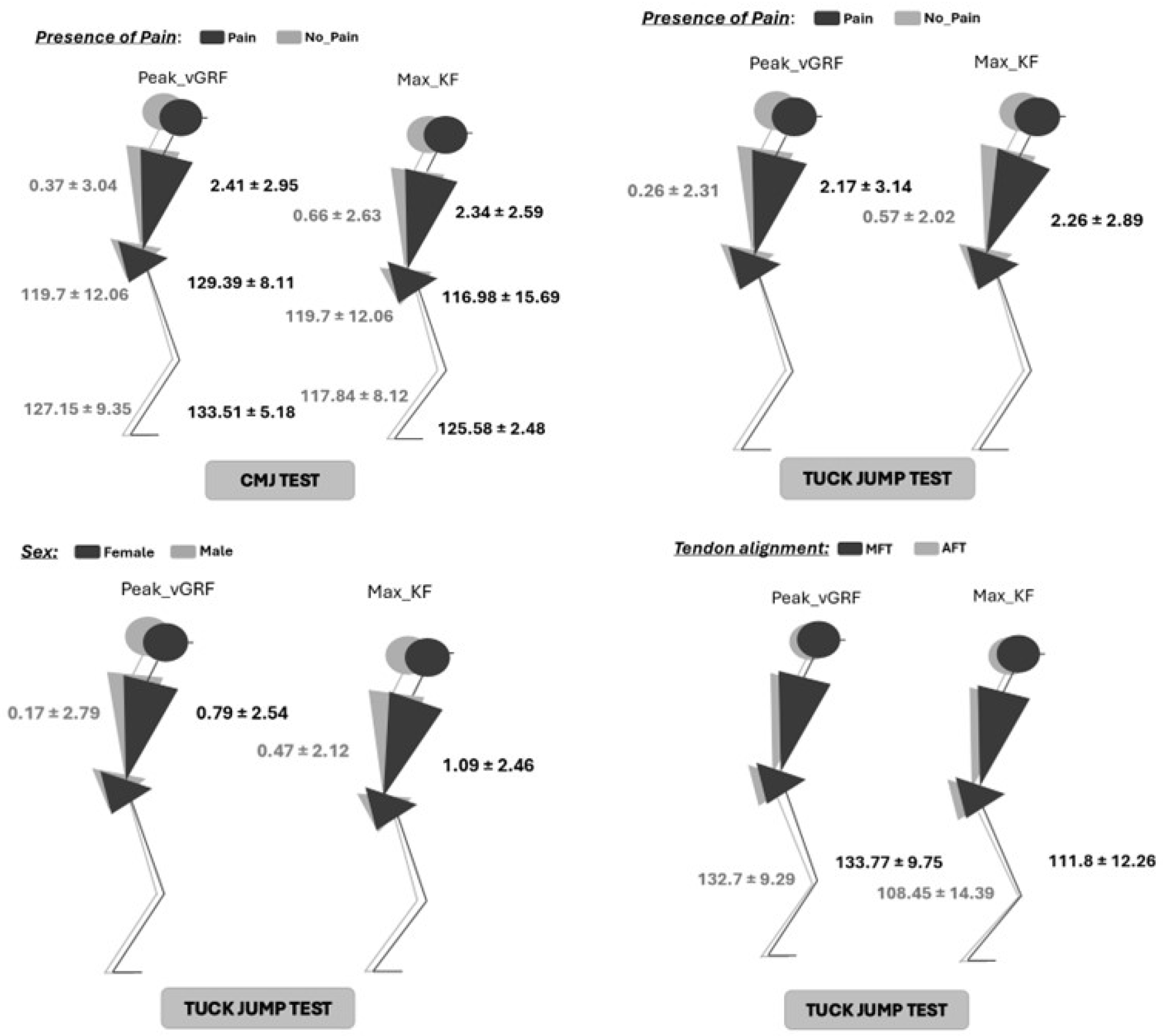
3.2. Join Kinetic Data
4. Discussion
4.1. Clinical Implications
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Theodorou, A.; Komnos, G.; Hantes, M. Patellar Tendinopathy: An Overview of Prevalence, Risk Factors, Screening, Diagnosis, Treatment and Prevention. Arch. Orthop. Trauma Surg. 2023, 143, 6695–6705. [Google Scholar] [CrossRef] [PubMed]
- Magnusson, S.; Langberg, H.; Kjaer, M. The Pathogenesis of Tendinopathy: Balancing the Response to Loading. Nat. Rev. Rheumatol. 2010, 6, 262–268. [Google Scholar] [CrossRef] [PubMed]
- Rio, E.; Moseley, L.; Purdam, C.; Samiric, T.; Kidgell, D.; Pearce, A.J.; Jaberzadeh, S.; Cook, J. The Pain of Tendinopathy: Physiological or Pathophysiological? Sport. Med. 2014, 44, 9–23. [Google Scholar] [CrossRef] [PubMed]
- Lundgreen, K.; Lian, O.B.; Engebretsen, L.; Scott, A. Tenocyte Apoptosis in the Torn Rotator Cuff: A Primary or Secondary Pathological Event? Br. J. Sports Med. 2011, 45, 1035–1039. [Google Scholar] [CrossRef]
- Docking, S.I.; Cook, J. Pathological Tendons Maintain Sufficient Aligned Fibrillar Structure on Ultrasound Tissue Characterization (UTC). Scand. J. Med. Sci. Sports 2016, 26, 675–683. [Google Scholar] [CrossRef]
- Leadbetter, W.B. Cell-Matrix Response in Tendon Injury. Clin. Sports Med. 1992, 11, 533–578. [Google Scholar] [CrossRef]
- Rees, J.D.; Maffulli, N.; Cook, J. Management of Tendinopathy. Am. J. Sports Med. 2009, 37, 1855–1867. [Google Scholar] [CrossRef]
- Andersson, G.; Forsgren, S.; Scott, A.; Gaida, J.E.; Stjernfeldt, J.E.; Lorentzon, R.; Alfredson, H.; Backman, C.; Danielson, P. Tenocyte Hypercellularity and Vascular Proliferation in a Rabbit Model of Tendinopathy: Contralateral Effects Suggest the Involvement of Central Neuronal Mechanisms. Br. J. Sports Med. 2011, 45, 399–406. [Google Scholar] [CrossRef]
- Malliaras, P.; Cook, J.; Purdam, C.; Rio, E. Patellar Tendinopathy: Clinical Diagnosis, Load Management, and Advice for Challenging Case Presentations. J. Orthop. Sport. Phys. Ther. 2015, 45, 887–898. [Google Scholar] [CrossRef]
- Longo, U.G.; Lamberti, A.; Maffulli, N.; Denaro, V. Tissue Engineered Biological Augmentation for Tendon Healing: A Systematic Review. Br. Med. Bull. 2011, 98, 31–59. [Google Scholar] [CrossRef]
- Zhi, Y.; Zhang, Y.; Zhang, Y.; Zhang, M.; Kong, Y. Age-Associated Changes in Multimodal Pain Perception. Age Ageing 2024, 53, afae107. [Google Scholar] [CrossRef] [PubMed]
- Miller, B.; Olesen, J.; Hansen, M.; Døssing, S.; Crameri, R.; Welling, R.; Langberg, H.; Flyvbjerg, A.; Kjaer, M.; Babraj, J.; et al. Coordinated Collagen and Muscle Protein Synthesis in Human Patella Tendon and Quadriceps Muscle after Exercise. J. Physiol. 2005, 567, 1021–1033. [Google Scholar] [CrossRef] [PubMed]
- Rio, E.; Kidgell, D.; Lorimer Moseley, G.; Gaida, J.; Docking, S.; Purdam, C.; Cook, J. Tendon Neuroplastic Training: Changing the Way We Think about Tendon Rehabilitation: A Narrative Review. Br. J. Sports Med. 2016, 50, 209–215. [Google Scholar] [CrossRef] [PubMed]
- Cook, J.L.; Purdam, C.R. The Challenge of Managing Tendinopathy in Competing Athletes. Br. J. Sports Med. 2014, 48, 506–509. [Google Scholar] [CrossRef]
- Florit, D.; Pedret, C.; Casals, M.; Malliaras, P.; Sugimoto, D.; Rodas, G. Incidence of Tendinopathy in Team Sports in a Multidisciplinary Sports Club Over 8 Seasons. J. Sports Sci. Med. 2019, 18, 780–788. [Google Scholar]
- Lian, Ø.; Engebretsen, L.; Bahr, R. Prevalence of Jumper’s Knee Among Elite Athletes From Different Sports A Cross-Sectional Study. Am. J. Sports Med. 2005, 33, 561–567. [Google Scholar] [CrossRef]
- Hägglund, M.; Zwerver, J.; Ekstrand, J. Epidemiology of Patellar Tendinopathy in Elite Male Soccer Players. Am. J. Sports Med. 2011, 39, 1906–1911. [Google Scholar] [CrossRef]
- Nutarelli, S.; Lodi, C.M.T.d.; Cook, J.L.; Deabate, L.; Filardo, G. Epidemiology of Patellar Tendinopathy in Athletes and the General Population: A Systematic Review and Meta-Analysis. Orthop. J. Sport. Med. 2023, 11, 1–11. [Google Scholar] [CrossRef]
- Rudavsky, A.; Cook, J.; Docking, S. Quantifying Proximal Patellar Tendon Changes during Adolescence in Elite Ballet Dancers, a 2-Year Study. Scand. J. Med. Sci. Sports 2018, 28, e13235. [Google Scholar] [CrossRef]
- Garcia, S.; Delattre, N.; Berton, E.; Rao, G. Patellar Tendon Force Differs Depending on Jump-Landing Tasks and Estimation Methods. Appl. Sci. 2022, 12, 488. [Google Scholar] [CrossRef]
- Ferretti, A.; Ippolito, E.; Mariani, P.; Puddu, G. Jumper’s Knee. Am. J. Sports Med. 1983, 11, 58–62. [Google Scholar] [CrossRef] [PubMed]
- Blazina, M.E.; Kerlan, R.K.; Jobe, F.W.; Carter, V.S.; Carlson, G.J. Jumper’s Knee. Orthop. Clin. North Am. 1973, 4, 665–678. [Google Scholar] [CrossRef] [PubMed]
- Harris, M.; Schultz, A.; Drew, M.K.; Rio, E.; Charlton, P.; Edwards, S. Jump-Landing Mechanics in Patellar Tendinopathy in Elite Youth Basketballers. Scand. J. Med. Sci. Sport. 2020, 30, 540–548. [Google Scholar] [CrossRef] [PubMed]
- Tayfur, A.; Haque, A.; Salles, J.I.; Malliaras, P.; Screen, H.; Morrissey, D. Are Landing Patterns in Jumping Athletes Associated with Patellar Tendinopathy? A Systematic Review with Evidence Gap Map and Meta-Analysis. Sport. Med. 2022, 52, 123–137. [Google Scholar] [CrossRef]
- Richards, D.P.; Ajemian, S.V.; Wiley, J.P.; Zernicke, R.F. Knee Joint Dynamics Predict Patellar Tendinitis in Elite Volleyball Players. Am. J. Sports Med. 1996, 24, 676–683. [Google Scholar] [CrossRef]
- Van der Worp, H.; de Poel, H.J.; Diercks, R.L.; van den Akker-Scheek, I.; Zwerver, J. Jumper’s Knee or Lander’s Knee? A Systematic Review of the Relation between Jump Biomechanics and Patellar Tendinopathy. Int. J. Sports Med. 2014, 35, 714–722. [Google Scholar] [CrossRef]
- de Vries, A.J.; van der Worp, H.; Diercks, R.L.; van den Akker-Scheek, I.; Zwerver, J. Risk Factors for Patellar Tendinopathy in Volleyball and Basketball Players: A Survey-Based Prospective Cohort Study. Scand. J. Med. Sci. Sports 2015, 25, 678–684. [Google Scholar] [CrossRef]
- Tsehaie, J.; Poot, D.H.J.; Oei, E.H.G.; Verhaar, J.A.N.; de Vos, R.J. Value of Quantitative MRI Parameters in Predicting and Evaluating Clinical Outcome in Conservatively Treated Patients with Chronic Midportion Achilles Tendinopathy: A Prospective Study. J. Sci. Med. Sport 2017, 20, 633–637. [Google Scholar] [CrossRef]
- Docking, S.I.; Ooi, C.C.; Connell, D. Tendinopathy: Is Imaging Telling Us the Entire Story? J. Orthop. Sport. Phys. Ther. 2015, 45, 842–852. [Google Scholar] [CrossRef]
- Van Schie, H.; Docking, S.; Daffy, J.; Praet, S.; Rosengarten, S.; Cook, J.L. Ultrasound Tissue Characterization, an Innovative Technique for Injury-Prevention and Monitoring of Tendinopathy. Br. J. Sports Med. 2013, 47, e2. [Google Scholar] [CrossRef]
- Hernández, G.; Dominguez, D.; Moreno, J.; Til Perez, L.; Ortís, L.; Pedret, C.; Van Schie, H.; Rodas, G. Caracterización Por Ultrasound Tissue Characterization de Los Tendones Rotulianos de Jugadores de Baloncesto; Comparación Entre Profesionales versus Formativos y Asintomáticos versus Sintomáticos. Apunt. Med. l’Esport 2017, 52, 45–52. [Google Scholar] [CrossRef]
- Rabello, L.M.; Dams, O.; Akker-Scheek, I.; Zwerver, J.; O’Neill, S. Substantiating the Use of Ultrasound Tissue Characterization in the Analysis of Tendon Structure: A Systematic Review. Clin. J. Sport Med. 2019, 31, e161–e175. [Google Scholar] [CrossRef] [PubMed]
- Edwards, S.; Steele, J.R.; Cook, J.L.; Purdam, C.R.; McGhee, D.E.; Munro, B.J. Characterizing Patellar Tendon Loading during the Landing Phases of a Stop-Jump Task. Scand. J. Med. Sci. Sports 2012, 22, 2–11. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [PubMed]
- Puddle, D.L.; Maulder, P.S. Ground Reaction Forces and Loading Rates Associated with Parkour and Traditional Drop Landing Techniques. J. Sports Sci. Med. 2013, 12, 122–129. [Google Scholar]
- Haischer, M.H.; Krzyszkowski, J.; Roche, S.; Kipp, K. Impulse-Based Dynamic Strength Index: Considering Time-Dependent Force Expression. J. Strength Cond. Res. 2021, 35, 1177–1181. [Google Scholar] [CrossRef]
- Ark, M.; Rabello, L.; Hoevenaars, D.; Meijerink, J.; Gelderen, N.; Zwerver, J.; Akker-Scheek, I. Inter- and Intra-rater Reliability of Ultrasound Tissue Characterization (UTC) in Patellar Tendons. Scand. J. Med. Sci. Sports 2019, 29, e13439. [Google Scholar] [CrossRef]
- Davis, R.B.; Õunpuu, S.; Tyburski, D.; Gage, J.R. A Gait Analysis Data Collection and Reduction Technique. Hum. Mov. Sci. 1991, 10, 575–587. [Google Scholar] [CrossRef]
- Rosen, A.B.; Ko, J.; Simpson, K.J.; Kim, S.H.; Brown, C.N. Lower Extremity Kinematics during a Drop Jump in Individuals with Patellar Tendinopathy. Orthop. J. Sport. Med. 2015, 3, 1–8. [Google Scholar] [CrossRef]
- Ortega-Cebrián, S.; Navarro, R.; Seda, S.; Salas, S.; Guerra-Balic, M. Patellar Tendon Structural Adaptations Occur during Pre-Season and First Competitive Cycle in Male Professional Handball Players. Int. J. Environ. Res. Public Health 2021, 18, 2156. [Google Scholar] [CrossRef]
- Hopkins, W.G.; Marshall, S.W.; Batterham, A.M.; Hanin, J. Progressive Statistics for Studies in Sports Medicine and Exercise Science. Med. Sci. Sports Exerc. 2009, 41, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Richards, D.P.; Ajemian, S.V.; Wiley, J.P.; Brunet, J.A.; Zernicke, R.F. Relation Between Ankle Joint Dynamics and Patellar Tendinopathy in Elite Volleyball Players. Clin. J. Sport Med. 2002, 12, 266–272. [Google Scholar] [CrossRef] [PubMed]
- Scattone Silva, R.; Nakagawa, T.H.; Ferreira, A.L.G.; Garcia, L.C.; Santos, J.E.M.; Serrão, F.V. Lower Limb Strength and Flexibility in Athletes with and without Patellar Tendinopathy. Phys. Ther. Sport 2016, 20, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Moseley, G.L.; Arntz, A. The Context of a Noxious Stimulus Affects the Pain It Evokes. Pain 2007, 133, 64–71. [Google Scholar] [CrossRef] [PubMed]
- Mann, K.J.; Edwards, S.; Drinkwater, E.J.; Bird, S.P. A Lower Limb Assessment Tool for Athletes at Risk of Developing Patellar Tendinopathy. Med. Sci. Sports Exerc. 2013, 45, 527–533. [Google Scholar] [CrossRef] [PubMed]
- Sorenson, S.C.; Arya, S.; Souza, R.B.; Pollard, C.D.; Salem, G.J.; Kulig, K. Knee Extensor Dynamics in the Volleyball Approach Jump: The Influence of Patellar Tendinopathy. J. Orthop. Sports Phys. Ther. 2010, 40, 568–576. [Google Scholar] [CrossRef]
- Obara, K.; Chiba, R.; Takahashi, M.; Matsuno, T.; Takakusaki, K. Knee Dynamics during Take-off and Landing in Spike Jumps Performed by Volleyball Players with Patellar Tendinopathy. J. Phys. Ther. Sci. 2022, 34, 103–109. [Google Scholar] [CrossRef]
- Mousavi, S.H.; Hijmans, J.M.; Rajabi, R.; Diercks, R.; Zwerver, J.; van der Worp, H. Kinematic Risk Factors for Lower Limb Tendinopathy in Distance Runners: A Systematic Review and Meta-Analysis. Gait Posture 2019, 69, 13–24. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Mean | SD | |
|---|---|---|
| AFT (female n = 21; male n = 28) | ||
| Age * | 24.95 | 3.16 |
| Height | 175.66 | 13.92 |
| Weight | 89.74 | 8.52 |
| Years of practice | 13.52 | 3.67 |
| Pain n = 5 | ||
| VISA-P * | 54 | 7.85 |
| MFT (female n = 7; male n = 12) | ||
| Age | 26.32 | 2.98 |
| Height | 179.86 | 11.71 |
| Weight | 86.49 | 9.14 |
| Years of practice | 14.78 | 4.12 |
| Pain n = 12 | ||
| VISA-P | 76 | 12.37 |
| Factor | Moment | Join | Variable | n | Mean ± SD | 95% CI (Inf to Sup Limit) | p-Value | Effect Size | Mean ± SD | 95% CI (Inf to Sup Limit) | p-Value | Effect Size |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Tendon | Peak_vGRF | Trunk | AFT | 38 | 0.48 ± 3.42 | −0.42 to 1.38 | 0.52 | −0.19 | 0.34 ± 2.88 | −0.4 to 1.08 | 0.334 | 0.04 |
| MFT | 24 | 1.19 ± 1.94 | 0.07 to 2.31 | 1.23 ± 1.21 | 0.53 to 1.92 | |||||||
| Hip | AFT | 38 | 121.89 ± 12.67 | 118.56 to 125.23 | 0.80 | 0.05 | 124.55 ± 12.03 | 121.44 to 127.66 | 0.207 | −0.73 | ||
| MFT | 24 | 119.77 ± 8.31 | 114.97 to 124.57 | 117.96 ± 8.69 | 112.94 to 122.97 | |||||||
| Knee | AFT | 38 | 133.77 ± 9.75 | 131.21 to 136.34 | 0.60 | 0.02 | 129.73 ± 6.69 | 128 to 131.46 | 0.012 * | −0.66 | ||
| MFT | 24 | 132.7 ± 9.29 | 127.34 to 138.06 | 126.48 ± 5.94 | 123.05 to 129.91 | |||||||
| Ankle | AFT | 38 | 128.65 ± 8.86 | 126.32 to 130.98 | 0.32 | 0.06 | 125.67 ± 10.36 | 122.99 to 128.34 | 0.956 | −0.26 | ||
| MFT | 24 | 126.14 ± 9.75 | 120.51 to 131.77 | 123.71 ± 8.32 | 118.91 to 128.52 | |||||||
| Max_KF | Trunk | AFT | 38 | 0.71 ± 2.8 | −0.02 to 1.45 | 0.35 | −0.02 | 0.74 ± 2.49 | 0.1 to 1.38 | 0.573 | 0.02 | |
| MFT | 24 | 1.55 ± 2.3 | 0.22 to 2.88 | 1.09 ± 1.31 | 0.33 to 1.84 | |||||||
| Hip | AFT | 38 | 103.98 ± 23.94 | 97.68 to 110.27 | 0.33 | 0.23 | 117.6 ± 15.14 | 113.69 to 121.51 | 0.166 | −0.63 | ||
| MFT | 24 | 95.12 ± 27.48 | 79.25 to 110.98 | 110.38 ± 9.2 | 105.07 to 115.69 | |||||||
| Knee | AFT | 38 | 111.8 ± 12.26 | 108.57 to 115.02 | 0.367 | 0.08 | 117.03 ± 9.85 | 114.49 to 119.58 | 0.028 * | −0.23 | ||
| MFT | 24 | 108.45 ± 14.39 | 100.14 to 116.75 | 115.22 ± 10.71 | 109.04 to 121.4 | |||||||
| Ankle | AFT | 38 | 119.79 ± 7.76 | 117.75 to 121.83 | 0.14 | 0.09 | 119.62 ± 11 | 116.77 to 122.46 | 0.985 | −0.16 | ||
| MFT | 24 | 116.28 ± 8.44 | 121.16 to 121.16 | 118.24 ± 9.69 | 112.65 to 123.84 | |||||||
| Pain | Peak_vGRF | Trunk | P | 17 | 2.41 ± 2.95 | 0.54 to 4.29 | 0.037 * | 0.12 | 2.17 ± 3.14 | 0.28 to 4.07 | 0.041 * | 0.14 |
| N_P | 45 | 0.37 ± 3.04 | −0.42 to 1.16 | 0.26 ± 2.31 | -0.34 to 0.85 | |||||||
| Hip | P | 17 | 129.39 ± 8.11 | 124.24 to 134.55 | 0.031 * | 0.56 | 128.53 ± 6.62 | 124.53 to 132.53 | 0.191 | 1.02 | ||
| N_P | 45 | 119.79 ± 12.06 | 116.65 to 122.93 | 122.22 ± 12.39 | 119.02 to 125.42 | |||||||
| Knee | P | 17 | 133.92 ± 10.18 | 127.45 to 140.38 | 0.38 | 0.01 | 129.04 ± 7.44 | 124.54 to 133.53 | 0.186 | −0.04 | ||
| N_P | 45 | 133.64 ± 9.6 | 131.13 to 136.14 | 129.19 ± 6.57 | 127.5 to 130.89 | |||||||
| Ankle | P | 17 | 133.51 ± 5.18 | 130.22 to 136.8 | 0.00 * | 0.37 | 133.92 ± 7.66 | 129.29 to 138.55 | 0.061 | 2.20 | ||
| N_P | 45 | 127.15 ± 9.35 | 124.71 to 129.59 | 123.28 ± 9.46 | 120.84 to 125.73 | |||||||
| Max_KF | Trunk | P | 17 | 2.34 ± 2.59 | 0.7 to 3.99 | 0.039* | 0.09 | 2.26 ± 2.86 | 0.54 to 3.99 | 0.029 * | 0.15 | |
| N_P | 45 | 0.66 ± 2.63 | −0.03 to 1.34 | 0.57 ± 2.02 | 0.05 to 1.09 | |||||||
| Hip | P | 17 | 116.98 ± 15.69 | 107.01 to 126.95 | 0.023 * | 0.14 | 123.49 ± 10.55 | 117.11 to 129.86 | 0.254 | 1.14 | ||
| N_P | 45 | 98.89 ± 25.23 | 92.32 to 105.47 | 114.62 ± 14.86 | 110.78 to 118.46 | |||||||
| Knee | P | 17 | 113.9 ± 14.43 | 104.73 to 123.07 | 0.83 | 0.19 | 117.92 ± 13.22 | 109.93 to 125.9 | 0.157 | 0.27 | ||
| N_P | 45 | 110.53 ± 12.44 | 107.29 to 113.77 | 116.42 ± 9.33 | 114.01 to 118.83 | |||||||
| Ankle | P | 17 | 125.58 ± 2.48 | 124.01 to 127.16 | 0.027 * | 0.45 | 128.39 ± 8.14 | 123.48 to 133.31 | 0.075 | 2.10 | ||
| N_P | 45 | 117.84 ± 8.12 | 115.73 to 119.96 | 117.2 ± 10.18 | 114.57 to 119.83 | |||||||
| Sex | Peak_vGRF | Trunk | F | 28 | 0.76 ± 3.13 | −0.25 to 1.78 | 0.60 | 0.01 | 0.79 ± 2.54 | −0.02 to 1.6 | 0.024 * | 0.02 |
| M | 34 | 0.45 ± 3.29 | −0.72 to 1.62 | 0.17 ± 2.79 | −0.8 to 1.15 | |||||||
| Hip | F | 28 | 118.76 ± 10.78 | 115.27 to 122.25 | 0.47 | −0.12 | 121.61 ± 10.41 | 118.28 to 124.94 | 0.458 | −0.26 | ||
| M | 34 | 124.7 ± 12.57 | 120.24 to 129.15 | 125.3 ± 12.95 | 120.78 to 129.82 | |||||||
| Knee | F | 28 | 134.28 ± 9.27 | 131.27 to 137.28 | 0.59 | 0.05 | 129.93 ± 5.96 | 128.03 to 131.84 | 0.358 | 0.14 | ||
| M | 34 | 132.72 ± 10.08 | 129.15 to 136.29 | 128.16 ± 7.34 | 125.6 to 130.72 | |||||||
| Ankle | F | 28 | 128.28 ± 9.08 | 125.33 to 131.22 | 0.99 | 0.00 | 124.27 ± 10.49 | 120.91 to 127.62 | 0.449 | −0.17 | ||
| M | 34 | 128.02 ± 9.1 | 124.79 to 131.25 | 126.51 ± 9.37 | 123.24 to 129.78 | |||||||
| Max_KF | Trunk | F | 28 | 1.02 ± 2.74 | 0.13 to 1.91 | 0.64 | 0.011 | 1.09 ± 2.46 | 0.31 to 1.88 | 0.000 * | 0.03 | |
| M | 34 | 0.7 ± 2.72 | −0.26 to 1.67 | 0.47 ± 2.12 | −0.27 to 1.21 | |||||||
| Hip | F | 28 | 98.51 ± 23.25 | 90.97 to 106.05 | 0.11 | −0.29 | 112.91 ± 13.11 | 108.71 to 117.1 | 0.744 | −0.46 | ||
| M | 34 | 106.68 ± 26 | 97.46 to 115.9 | 120.15 ± 15.12 | 114.87 to 125.43 | |||||||
| Knee | F | 28 | 111.4 ± 12.63 | 107.31 to 115.5 | 0.50 | 0.02 | 116.87 ± 9.43 | 113.85 to 119.89 | 0.614 | 0.03 | ||
| M | 34 | 110.84 ± 12.89 | 106.27 to 115.41 | 116.48 ± 10.71 | 112.74 to 120.21 | |||||||
| Ankle | F | 28 | 118.44 ± 7.53 | 116 to 120.88 | 0.51 | −0.05 | 117.62 ± 11.07 | 114.08 to 121.16 | 0.456 | −0.28 | ||
| M | 34 | 119.9 ± 8.48 | 116.89 to 122.9 | 121.4 ± 10.06 | 117.89 to 124.91 |
| Factor | Variable | Tendon Alingment | n | Mean ± SD | 95% CI (Sup to Inf) | p-Value | Effect Size |
|---|---|---|---|---|---|---|---|
| Peak_vGRF (N) | Tendon Structure | AFT | 208 | 2.44 ± 10.49 | 26.93 to 21.99 | 0.871 | −0.56 |
| MFT | 72 | 2.47 ± 10.52 | 26.15 to 23.26 | ||||
| Pain | No_Pain | 112 | 24.75 ± 10.61 | 26. 32 to 23. 18 | 0.836 | 0.84 | |
| Pain | 110 | 2.44 ± 10.82 | 26. 51 to 22. 42 | ||||
| Sex | Female | 152 | 23.07± 8.38 | 24.41 to 21.72 | 0.011 * | −0.48 | |
| Male | 128 | 26.51 ± 12.40 | 2868.27 to 2434.45 | ||||
| Jump | CMJ | 140 | 18.11 ± 8.01 | 19.45 to 16.7 | 0.000 * | −0.02 | |
| TJT | 140 | 31.17 ± 8.53 | 32.59 to 29.74 | ||||
| Load_Time/Knee (sec) | Tendon Structure | AFT | 208 | 0.18 ± 0.03 | 0.18 to 0.17 | 0.028 | −0.8 |
| MFT | 72 | 0.2 ± 0.17 | 0.23 to 0.18 | ||||
| pain | No_Pain | 112 | 0.19 ± 0.15 | 0.22 to 0.17 | 0.735 | −0.32 | |
| Pain | 110 | 0.2 ± 0.16 | 0.23 to 0.17 | ||||
| Sex | Female | 152 | 0.19 ± 0.14 | 0.21 to 0.17 | 0.389 * | −0.8 | |
| Male | 128 | 0.21 ± 0.16 | 0.23 to 0.18 | ||||
| Jump | CMJ | 140 | 0.19 ± 0.03 | 0.2 to 0.19 | 0.684 | −0.37 | |
| TJT | 140 | 0.2 ± 0.21 | 0.24 to 0.17 | ||||
| Load_Rate/Knee | Tendon Structure | AFT | 208 | 13.72 ± 9.28 | 15.90 to 11. 54 | 0.993 | 0.22 |
| MFT | 72 | 13.72 ± 10.10 | 15.10 to 12.34 | ||||
| pain | No_Pain | 112 | 13.70 ± 9.79 | 15.18 to 12.23 | 0.976 | −0.65 | |
| Pain | 110 | 13.74 ± 10.06 | 15.65 to 11.84 | ||||
| Sex | Female | 152 | 13.26 ± 9.21 | 14.74 to 11.79 | 0.412 * | −0.06 | |
| Male | 128 | 14.26 ± 10.63 | 16.12 to 12.40 | ||||
| Jump | CMJ | 140 | 7.42 ± 2.23 | 7.79 to 7.05 | 0.000 * | −0.62 | |
| TJT | 140 | 20.02 ± 10.53 | 21.78 to 18.26 | ||||
| Area/Knee | Tendon Structure | AFT | 208 | 332.72 ± 62.2 | 347.34 to 318.11 | 0.733 | −0.62 |
| MFT | 72 | 336.59 ± 125.9 | 353.8 to 319.38 | ||||
| pain | No_Pain | 112 | 336.57 ± 117.4 | 354.34 to 318.79 | 0.856 | 0.32 | |
| Pain | 110 | 334.09 ± 106.08 | to 314.04 | ||||
| Sex | Female | 152 | 290.42 ± 85.21 | 304.07 to 276.76 | 0.000 * | −0.73 | |
| Male | 128 | 389.24 ± 118.43 | 409.95 to 368.53 | ||||
| Jump | CMJ | 140 | 313.3 ± 56.16 | 322.69 to 303.92 | 0.000 * | −0.86 | |
| TJT | 140 | 357.88 ± 146.39 | 382.34 to 333.42 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ortega-Cebrián, S.; Silva, D.C.F.; Carneiro, D.F.; Zárate, V.; Alves, L.A.T.; Guedes, D.C.; Zárate-Tejero, C.A.; Cadellans-Arróniz, A.; Montes, A.M. Presence of Pain Shows Greater Effect than Tendon Structural Alignment During Landing Dynamics. J. Funct. Morphol. Kinesiol. 2025, 10, 74. https://doi.org/10.3390/jfmk10010074
Ortega-Cebrián S, Silva DCF, Carneiro DF, Zárate V, Alves LAT, Guedes DC, Zárate-Tejero CA, Cadellans-Arróniz A, Montes AM. Presence of Pain Shows Greater Effect than Tendon Structural Alignment During Landing Dynamics. Journal of Functional Morphology and Kinesiology. 2025; 10(1):74. https://doi.org/10.3390/jfmk10010074
Chicago/Turabian StyleOrtega-Cebrián, Silvia, Diogo C. F. Silva, Daniela F. Carneiro, Victor Zárate, Leonel A. T. Alves, Diana C. Guedes, Carlos A. Zárate-Tejero, Aïda Cadellans-Arróniz, and António Mesquita Montes. 2025. "Presence of Pain Shows Greater Effect than Tendon Structural Alignment During Landing Dynamics" Journal of Functional Morphology and Kinesiology 10, no. 1: 74. https://doi.org/10.3390/jfmk10010074
APA StyleOrtega-Cebrián, S., Silva, D. C. F., Carneiro, D. F., Zárate, V., Alves, L. A. T., Guedes, D. C., Zárate-Tejero, C. A., Cadellans-Arróniz, A., & Montes, A. M. (2025). Presence of Pain Shows Greater Effect than Tendon Structural Alignment During Landing Dynamics. Journal of Functional Morphology and Kinesiology, 10(1), 74. https://doi.org/10.3390/jfmk10010074