Sexual Satisfaction in a Sample of Italian Women during the COVID-19 Lockdown Period

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Sample Characteristics and Data Collection
2.2. The Survey
2.3. Statistical Analyses
3. Results
3.1. Descriptive Statistics of the Sample
3.2. Correlational Analyses
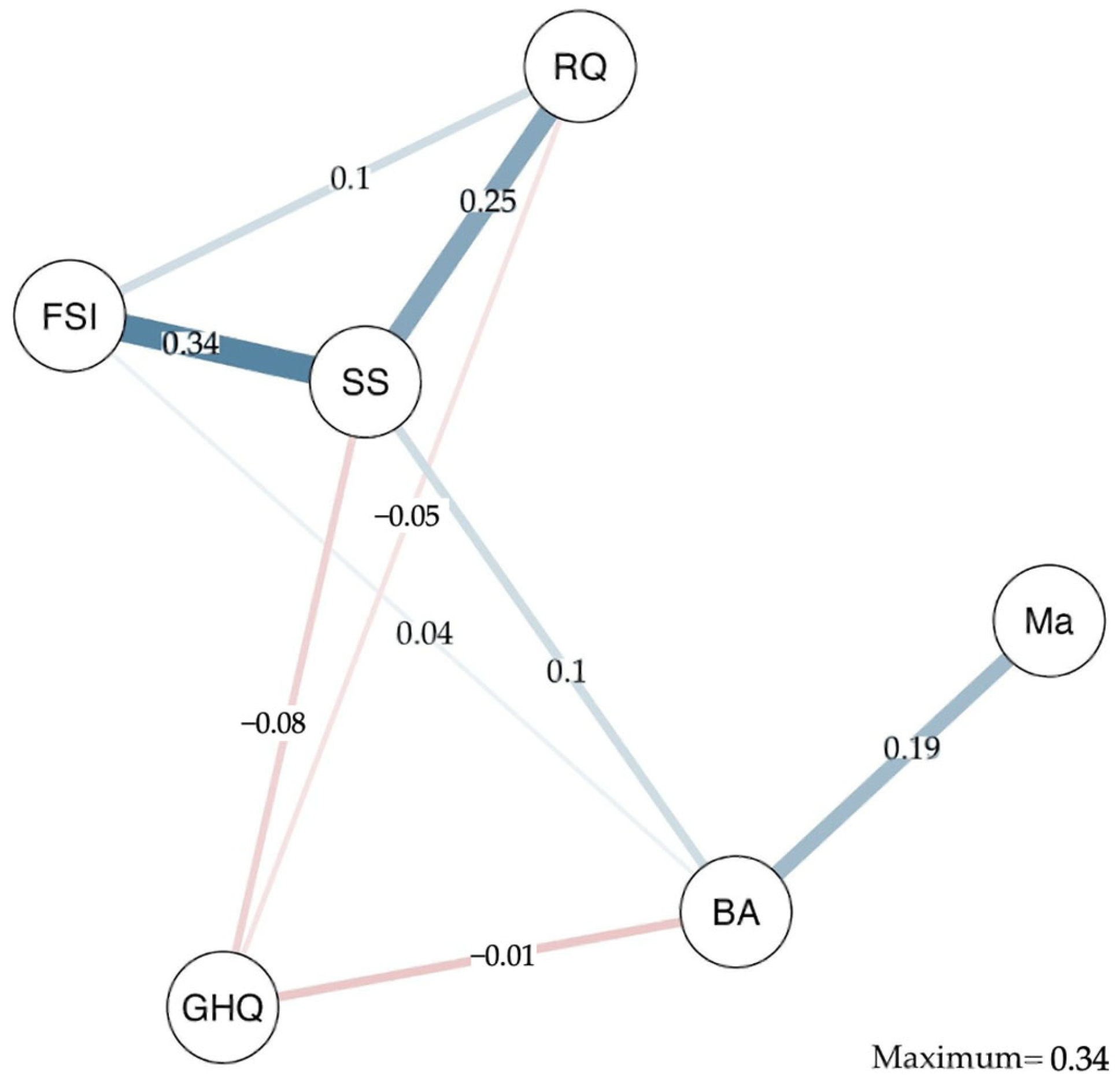
3.3. Network Analysis
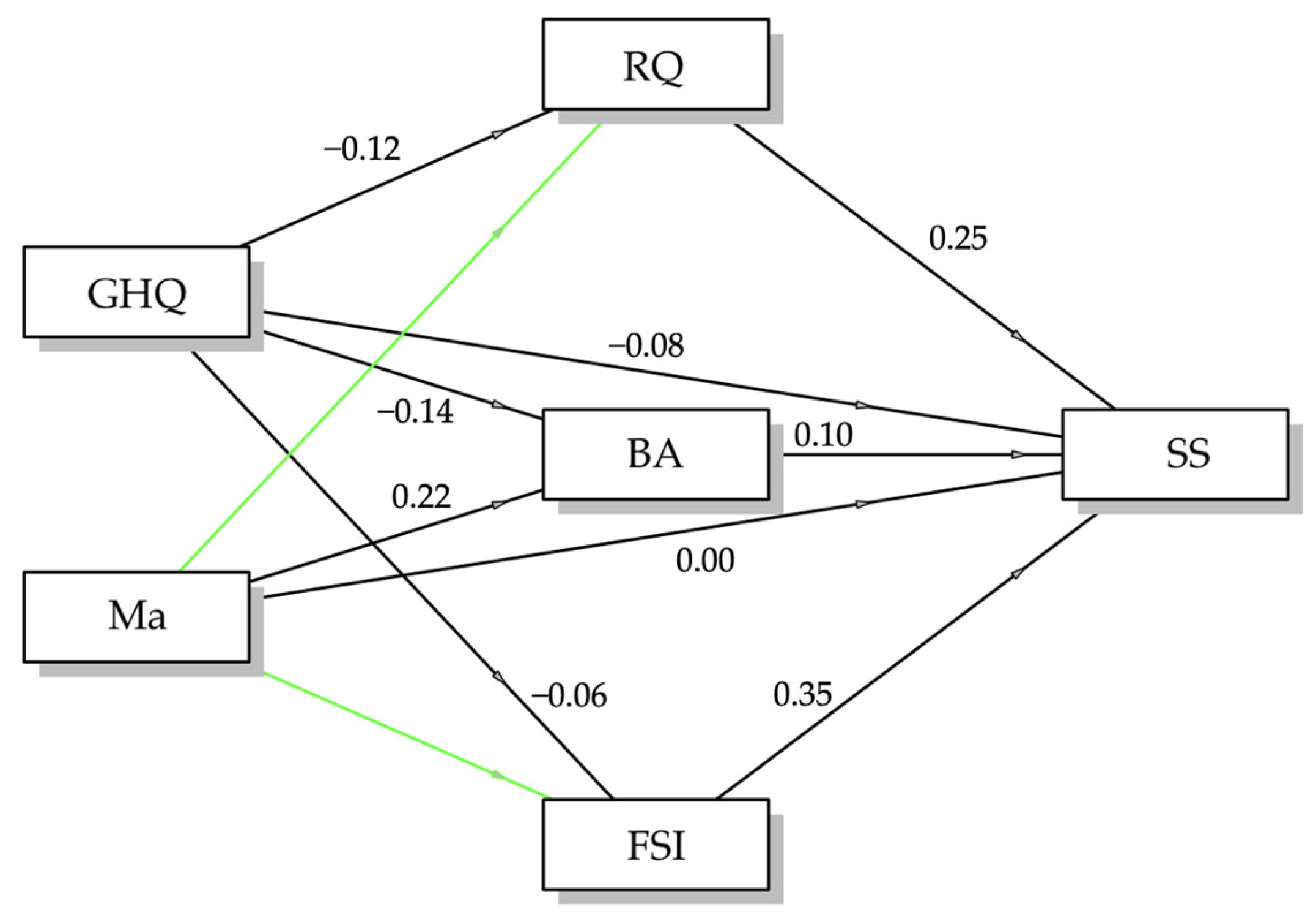
3.4. Mediation Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
- Demographic Questions
- Gender/Genere (multiple-choice question)
- ∘
- Italian: Genere (Femminile, Non-binary, FtM)
- ∘
- English: Gender (Female, Non-binary, FtM)
- Age/Età (open-ended numerical question)
- ∘
- Italian: Età
- ∘
- English: Age
- Region of Origin/Zona di Provenienza (multiple-choice question)
- ∘
- Italian: Zona di provenienza (Nord Italia, Centro Italia, Sud Italia)
- ∘
- English: Origin (North of Italia, Centre of Italy, South of Italy)
- Current Residential Context/Attuale Contesto di Residenza (multiple-choice question)
- ∘
- Italian: Attuale contesto di residenza (Città metropolitana, Paese, Provincia o quartiere residenziale, Contesto isolato)
- ∘
- English: Current residential context (Metropolitan City, Village, Province or Residential Neighborhood, Isolated Area)
- Education Level/Grado di Istruzione (multiple-choice question)
- ∘
- Italian: Grado di istruzione (Licenza elementare, Licenza media, Diploma di maturità, Laurea triennale, Laurea magistrale, Dottorato/Specializzazione)
- ∘
- English: Education level (Elementary School Diploma, Middle School Diploma, High School Diploma, Bachelor’s Degree, Master’s Degree, PhD/Specialization)
- Occupation/Attività Professionale (multiple-choice question)
- ∘
- Italian: Attività professionale (Libero Professionista, Studente, Imprenditore, Dipendente a tempo indeterminato, Dipendente a tempo determinato, Inoccupato, Disoccupato, Casalingo)
- ∘
- English: Occupation (Freelancer, Student, Entrepreneur, Permanent Employee, Fixed-Term Employee, Not Seeking Employment, Unemployed, Housewife)
- Who Do You Live With?/Con Chi Vive? (multiple-selection question)
- ∘
- Italian: Con chi vive? (Partner/coniuge, Da solo, Genitore/i, Fratello/i, Figlio/i, Coinquilino/i)
- ∘
- English: Who Do You Live With? (Partner/Spouse, Alone, Parent(s), Sibling(s), Child(ren), Roommate(s))
- Please Indicate Your Current Weight/Indichi il Suo Peso Attuale (open-ended numerical question)
- ∘
- Italian: Indichi il suo peso attuale (kg)
- ∘
- English: Please Indicate Your Current Weight (kg)
- Please Indicate Your Height (cm)/Indichi la Sua Altezza (cm) (open-ended numerical question)
- ∘
- Italian: Indichi la sua altezza (cm)
- ∘
- English: Please Indicate Your Height (cm)
- Do You Regularly Smoke Cigarettes?/Abitualmente Fuma Sigarette? (Likert scale 0–3)
- ∘
- Italian: Abitualmente fuma sigarette? (Sì, A volte, No)
- ∘
- English: Do you Regularly Smoke Cigarettes? (Yes, Sometimes, No)
- Do You Engage in Physical Activity?/Svolge Attività Fisica? (Likert scale 0–5)
- ∘
- Italian: Svolge attività fisica? (Mai, Saltuariamente, 1–3 volte a settimana, Più di 3 volte a settimana, Tutti i giorni)
- ∘
- English: Do you Engage in Physical Activity? (Never, Occasionally, 1–3 Times a week, More Than 3 Times a Week, Daily)
- Do You Have an Important and Stable Emotional Relationship?/Ha una Relazione Affettiva Importante e Stabile? (multiple-choice question)
- ∘
- Italian: Ha una relazione affettiva importante e stabile? (Sì, No)
- ∘
- English: Do you Have an Important and Stable Emotional Relationship? (Yes, No)
- Please Rate the Quality of Your Relationship/Valuti la Qualità di Questa Relazione (Likert scale 5–1)
- ∘
- Italian: Valuti la qualità di questa relazione: (Molto buona, affettuosa, calda e serena; Buona, abbastanza serena e affettuosa, non ci sono liti importanti; Discreta, su alcune cose c’è incomprensione, potrebbe esserci più affetto; Non buona, c’è poco affetto e frequenti contrasti; Pessima, non c’è amore ma solo litigi e incomprensioni)
- ∘
- English: Please Rate the Quality of Your Relationship: (Very Good, Affectionate, Warm and Serene; Good, Quite Serene and Affectionate, No Major Quarrels; Fair, There Is Some Misunderstanding, There Could Be More Affection; Not Good, There Is Little Affection and Frequent Conflicts; Very Poor, There Is No Love, Only Arguments and Misunderstandings)
- How Often Do You Masturbate?/Con Quale Frequenza si Masturba? (Likert scale 4-1)
- ∘
- Italian: Con quale frequenza si masturba? (Tutti i giorni, Spesso, Raramente, Mai)
- ∘
- English: How Often Do You Masturbate? (Daily, Often, Rarely, Never)
- My Sexual Life Is Satisfying/La Mia Vita Sessuale è Soddisfacente (Likert scale 1–5)
- ∘
- Italian: La mia vita sessuale è (1 = per nulla soddisfacente, 5 = molto soddisfacente)
- ∘
- English: My Sexual Life Is (1 = Not At All Satisfying, 5 = Very Satisfying)
- How Well Do You Know Your Body?/Quanto Sente di Conoscere il Suo Corpo (Likert scale 1–5)
- ∘
- Italian: Quanto sente di conoscere il suo corpo (1 = per nulla, 5 = moltissimo)
- ∘
- English: How Well Do You Know Your Body? (1 = Not At All, 5 = Very Well)
- General Health Questionnaire/Questionario Generale di Salute (GHQ-12; Goldberg and Hillier; Giorgi Rossi et al.): 12 questions (Likert scales 0–3)
- Optional Email/Email Facoltativa
- Italian: Lasciaci la tua mail se sei curiosa di ricevere informazioni e una restituzione sullo studio! (non è un campo obbligatorio)
- English: Leave your email if you are interested in receiving information and feedback on the study! (optional field)
References
- Rausch, D.; Rettenberger, M. Predictors of Sexual Satisfaction in Women: A Systematic Review. Sex. Med. Rev. 2021, 9, 365–380. [Google Scholar] [CrossRef]
- Lawless, N.J.; Karantzas, G.C.; Mullins, E.R.; McCabe, M.P. Does It Matter Who You Feel Sexually Aroused by? Associations between Sexual Arousal, Relationship Quality, and Sexual Satisfaction. Sex. Med. 2022, 10, 100523. [Google Scholar] [CrossRef] [PubMed]
- Buczak-Stec, E.W.; König, H.-H.; Hajek, A. Sexual Satisfaction Among Sexual Minority and Heterosexual Middle-Aged and Older Adults. Innov. Aging 2023, 7, igad010. [Google Scholar] [CrossRef]
- Mollaioli, D.; Sansone, A.; Ciocca, G.; Limoncin, E.; Colonnello, E.; Di Lorenzo, G.; Jannini, E.A. Benefits of sexual activity on psychological, relational, and sexual health during the COVID-19 breakout. J. Sex. Med. 2021, 18, 35–49. [Google Scholar] [CrossRef] [PubMed]
- Mallory, A.B.; Stanton, A.M.; Handy, A.B. Couples’ Sexual Communication and Dimensions of Sexual Function: A Meta-Analysis. J. Sex. Res. 2019, 56, 882–898. [Google Scholar] [CrossRef] [PubMed]
- Mark, K.P.; Vowels, L.M.; Murray, S.H. The Impact of Attachment Style on Sexual Satisfaction and Sexual Desire in a Sexually Diverse Sample. J. Sex. Marital. Ther. 2018, 44, 450–458. [Google Scholar] [CrossRef] [PubMed]
- Peixoto, M.M.; Amarelo-Pires, I.; Pimentel Biscaia, M.S.; Machado, P.P.P. Sexual Self-Esteem, Sexual Functioning and Sexual Satisfaction in Portuguese Heterosexual University Students. Psychol. Sex. 2018, 9, 305–316. [Google Scholar] [CrossRef]
- Vowels, L.M.; Vowels, M.J.; Mark, K.P. Identifying the Strongest Self-Report Predictors of Sexual Satisfaction Using Machine Learning. J. Soc. Pers. Relatsh. 2022, 39, 1191–1212. [Google Scholar] [CrossRef]
- Antičević, V.; Jokić-Begić, N.; Britvić, D. Sexual Self-concept, Sexual Satisfaction, and Attachment among Single and Coupled Individuals. Pers. Relatsh. 2017, 24, 858–868. [Google Scholar] [CrossRef]
- Murtagh, J. Female Sexual Function, Dysfunction, and Pregnancy: Implications for Practice. J. Midwife Womens Health 2010, 55, 438–446. [Google Scholar] [CrossRef]
- Carvalheira, A.; Leal, I. Masturbation Among Women: Associated Factors and Sexual Response in a Portuguese Community Sample. J. Sex. Marital. Ther. 2013, 39, 347–367. [Google Scholar] [CrossRef] [PubMed]
- Mollaioli, D.; Di Sante, S.; Limoncin, E.; Ciocca, G.; Gravina, G.L.; Maseroli, E.; Fanni, E.; Vignozzi, L.; Maggi, M.; Lenzi, A.; et al. Validation of a visual analogue scale to measure the subjective perception of orgasmic intensity in females: The Orgasmometer-F. PLoS ONE 2018, 13, e0202076. [Google Scholar] [CrossRef] [PubMed]
- Horvath, Z.; Smith, B.H.; Sal, D.; Hevesi, K.; Rowland, D.L. Body Image, Orgasmic Response, and Sexual Relationship Satisfaction: Understanding Relationships and Establishing Typologies Based on Body Image Satisfaction. Sex. Med. 2020, 8, 740–751. [Google Scholar] [CrossRef] [PubMed]
- Kılıç, D.; Armstrong, H.L.; Graham, C.A. The Role of Mutual Masturbation within Relationships: Associations with Sexual Satisfaction and Sexual Self-Esteem. Int. J. Sex. Health 2023, 35, 495–514. [Google Scholar] [CrossRef]
- Cervilla, O.; Sierra, J.C. Masturbation Parameters Related to Orgasm Satisfaction in Sexual Relationships: Differences between Men and Women. Front. Psychiatry 2022, 13, 903361. [Google Scholar] [CrossRef]
- Kvalem, I.L.; Træen, B.; Markovic, A.; Von Soest, T. Body Image Development and Sexual Satisfaction: A Prospective Study From Adolescence to Adulthood. J. Sex. Res. 2019, 56, 791–801. [Google Scholar] [CrossRef]
- Ashkinazi, M.; Wagner, S.A.; Cunningham, K.; Mattson, R.E. Body Image Satisfaction and Body-Related Partner Commentary Link to Marital Quality through Sexual Frequency and Satisfaction: A Path Model. Couple Fam. Psychol. Res. Pract. 2024, 13, 31–49. [Google Scholar] [CrossRef]
- Price, A.A.; McCann, K.G.Y.; Kunzler, L.; Leavitt, C.E.; Holmes, E.K. Body Image and Sex: A Dyadic Examination of Body Esteem and Sexual Inhibition, Obsession, and Harmony. J. Sex. Res. 2023, 60, 816–826. [Google Scholar] [CrossRef]
- Parma, C.; Doria, F.; Zulueta, A.; Lanzone, J.; Boscarino, M.; Giani, L.; Lunetta, C.; Vassallo, M.; Parati, E.A.; Picozzi, M.; et al. An Overview of the Bodily Awareness Representation and Interoception: Insights and Progress in the Field of Neurorehabilitation Research. Brain Sci. 2024, 14, 386. [Google Scholar] [CrossRef]
- Seal, B.N.; Meston, C.M. The Impact of Body Awareness on Women’s Sexual Health: A Comprehensive Review. Sex. Med. Rev. 2020, 8, 242–255. [Google Scholar] [CrossRef]
- Beaulieu, N.; Bergeron, S.; Brassard, A.; Byers, E.S.; Péloquin, K. Toward an Integrative Model of Intimacy, Sexual Satisfaction, and Relationship Satisfaction: A Prospective Study in Long-Term Couples. J. Sex. Res. 2023, 60, 1100–1112. [Google Scholar] [CrossRef] [PubMed]
- Mallory, A.B. Dimensions of Couples’ Sexual Communication, Relationship Satisfaction, and Sexual Satisfaction: A Meta-Analysis. J. Fam. Psychol. 2022, 36, 358–371. [Google Scholar] [CrossRef] [PubMed]
- Yagoob Idris, S.A.; ElSanousi, E.M. Pandemic of Coronavirus Disease 19 (COVID-19): A Comprehensive Review. Afr. J. Biol. Sci. 2020, 2, 1. [Google Scholar] [CrossRef]
- Stanton, R.; To, Q.G.; Khalesi, S.; Williams, S.L.; Alley, S.J.; Thwaite, T.L.; Fenning, A.S.; Vandelanotte, C. Depression, Anxiety and Stress during COVID-19: Associations with Changes in Physical Activity, Sleep, Tobacco and Alcohol Use in Australian Adults. Int. J. Environ. Res. Public Health 2020, 17, 4065. [Google Scholar] [CrossRef] [PubMed]
- Aolymat, I.; Abdul Kadir, L.; Al Nsour, M.; Taha, H. The Impact of the COVID-19 Pandemic on Female Sexual Function in Jordan: Cross-Sectional Study. JMIR Form. Res. 2023, 7, e40772. [Google Scholar] [CrossRef] [PubMed]
- Gleason, N.; Banik, S.; Braverman, J.; Coleman, E. The Impact of the COVID-19 Pandemic on Sexual Behaviors: Findings From a National Survey in the United States. J. Sex. Med. 2021, 18, 1851–1862. [Google Scholar] [CrossRef]
- Ko, N.-Y.; Lu, W.-H.; Chen, Y.-L.; Li, D.-J.; Chang, Y.-P.; Wu, C.-F.; Wang, P.-W.; Yen, C.-F. Changes in Sex Life among People in Taiwan during the COVID-19 Pandemic: The Roles of Risk Perception, General Anxiety, and Demographic Characteristics. Int. J. Environ. Res. Public Health 2020, 17, 5822. [Google Scholar] [CrossRef]
- Berdychevsky, L.; Cavanaugh, D.; Dariotis, J.K. Psychological, Socio-Demographic, and Logistical Factors Associated with Changes in Sex Life After Over a Year Into the COVID-19 Pandemic. Int. J. Sex. Health 2023, 35, 263–283. [Google Scholar] [CrossRef]
- Bonfanti, R.C.; Garro, M.; Lavanco, G.; Ruggieri, S. The Role of Sexting in Couple Wellbeing for Italian Women during the Second Wave of the COVID-19 Pandemic. Front. Psychol. 2023, 14, 1105556. [Google Scholar] [CrossRef]
- Bianchi, D.; Baiocco, R.; Lonigro, A.; Pompili, S.; Zammuto, M.; Di Tata, D.; Morelli, M.; Chirumbolo, A.; Di Norcia, A.; Cannoni, E.; et al. Love in Quarantine: Sexting, Stress, and Coping During the COVID-19 Lockdown. Sex. Res. Soc. Policy 2023, 20, 465–478. [Google Scholar] [CrossRef]
- Federici, S.; Lepri, A.; Mencarelli, A.C.; Zingone, E.; Leonibus, R.D.; Acocella, A.M.; Giammaria, A. The Sexual Experience of Italian Adults during the COVID-19 Lockdown. PLoS ONE 2022, 17, e0268079. [Google Scholar] [CrossRef] [PubMed]
- Borlimi, R.; Buattini, M.; Riboli, G.; Nese, M.; Brighetti, G.; Giunti, D.; Vescovelli, F. Menstrual Cycle Symptomatology during the COVID-19 Pandemic: The Role of Interoceptive Sensibility and Psychological Health. Compr. Psychoneuroendocrinology 2023, 14, 100182. [Google Scholar] [CrossRef]
- Schilt, K.; Westbrook, L. Doing Gender, Doing Heteronormativity: “Gender Normals,” Transgender People, and the Social Maintenance of Heterosexuality. Gend. Soc. 2009, 23, 440–464. [Google Scholar] [CrossRef]
- Giorgi, G.; Leon Perez, J.M.; Castiello D’Antonio, A.; Fiz Perez, F.J.; Arcangeli, G.; Cupelli, V.; Mucci, N. The General Health Questionaire (GHQ-12) in a Sample of Italian Workers: Mental Health at Individual and Organizational Level. World J. Med. Sci. 2014, 11, 47–56. [Google Scholar] [CrossRef]
- Goldberg, D.P.; Hillier, V.F. A Scaled Version of the General Health Questionnaire. Psychol. Med. 1979, 9, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Piccinelli, M.; Bisoffi, G.; Bon, M.G.; Cunico, L.; Tansella, M. Validity and Test-Retest Reliability of the Italian Version of the 12-Item General Health Questionnaire in General Practice: A Comparison between Three Scoring Methods. Compr. Psychiatry 1993, 34, 198–205. [Google Scholar] [CrossRef] [PubMed]
- Garrow, J.S.; Webster, J. Quetelet’s Index (W/H2) as a Measure of Fatness. Int. J. Obes. 1985, 9, 147–153. [Google Scholar]
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic. Report of a WHO Consultation. World Health Organ. Tech. Rep. Ser. 2000, 894, i–xii, 1–253. [Google Scholar]
- Foygel, R.; Drton, M. Extended Bayesian Information Criteria for Gaussian Graphical Models. Adv. Neural Inf. Process. Syst. 2010, 23, 1–14. [Google Scholar] [CrossRef]
- Gallucci, M. PATHj: Jamovi Path Analysis [Jamovi Module]. 2021. Available online: https://pathj.github.io/ (accessed on 24 June 2024).
- Rosseel, Y. lavaan: An R Package for Structural Equation Modeling. J. Stat. Softw. 2019, 48, 1–36. [Google Scholar] [CrossRef]
- Richetin, J.; Preti, E.; Costantini, G.; De Panfilis, C. The Centrality of Affective Instability and Identity in Borderline Personality Disorder: Evidence from Network Analysis. PLoS ONE 2017, 12, e0186695. [Google Scholar] [CrossRef] [PubMed]
- Thomas, H.N.; Hamm, M.; Borrero, S.; Hess, R.; Thurston, R.C. Body Image, Attractiveness, and Sexual Satisfaction Among Midlife Women: A Qualitative Study. J. Women’s Health 2019, 28, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Tosun Güleroğlu, F.; Uludağ, E. The Effects of Motherhood and Body Perception on Sexual Dysfunctions among Pregnant Women. Perspect. Psychiatr. Care 2022, 58, 2072–2078. [Google Scholar] [CrossRef] [PubMed]
- Carels, R.A.; Miller, J.C.; Hlavka, R.; Shonrock, A.M.T. The Interaction between BMI, Weight Criticism, Weight Bias, and Psychological and Relational Outcomes within Marriage. Eat. Weight Disord. 2022, 27, 1887–1893. [Google Scholar] [CrossRef] [PubMed]
- Dewitte, M.; Mayer, A. Exploring the Link Between Daily Relationship Quality, Sexual Desire, and Sexual Activity in Couples. Arch. Sex Behav. 2018, 47, 1675–1686. [Google Scholar] [CrossRef] [PubMed]
- Ihsan, A.; Khan, R.M.; Muhammad, K. Mediating Role of Psychological Distress between Body Image Concerns and Sexual Functioning in Primiparous Women. J. Prof. Appl. Psychol. 2023, 4, 342–351. [Google Scholar] [CrossRef]
- Mozafari, M.; Khajavikhan, J.; Jaafarpour, M.; Khani, A.; Direkvand-Moghadam, A.; Najafi, F. Association of Body Weight and Female Sexual Dysfunction: A Case Control Study. Iran. Red. Crescent Med. J. 2015, 17, e24685. [Google Scholar] [CrossRef]
- Rosen, C.; Brown, J.; Heiman, S.; Leib, R. The Female Sexual Function Index (FSFI): A Multidimensional Self-Report Instrument for the Assessment of Female Sexual Function. J. Sex Marital. Ther. 2000, 26, 191–208. [Google Scholar] [CrossRef]
- Italian National Institute of Statistics. Indicatori Demografici—Anno 2023. Available online: https://www.istat.it/wp-content/uploads/2024/03/Indicatori_demografici.pdf (accessed on 10 July 2024).
- McNabney, S.M.; Gletsu-Miller, N.; Rowland, D.L. Sexual Function and Satisfaction in the Context of Obesity. Curr. Diab. Rep. 2023, 23, 315–327. [Google Scholar] [CrossRef] [PubMed]
- Mernone, L.; Fiacco, S.; Ehlert, U. Positive Body Perception and Its Link to Sexual Satisfaction in Aging Women—Findings from the Women 40+ Healthy Aging Study. J. Women Aging 2023, 35, 152–167. [Google Scholar] [CrossRef]
- Henning, G.; Segel-Karpas, D.; Praetorius Björk, M.; Bjälkebring, P.; Berg, A.I. Retirement and Sexual Satisfaction. Gerontologist 2023, 63, 274–284. [Google Scholar] [CrossRef] [PubMed]
- Leonhardt, N.D.; Busby, D.M.; Hanna-Walker, V.R.; Leavitt, C.E. Sanctification or Inhibition? Religious Dualities and Sexual Satisfaction. J. Fam. Psychol. 2021, 35, 433–444. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Variable | Mean ± SD | Min-Max | Skewness ± SE | Kurtosis ± SE | Frequency Distribution (%) |
|---|---|---|---|---|---|
| Age | 23.4 ± 5.59 | 18–64 | 2.80 ± 0.040 | 11.3 ± 0.080 | 20s (90.6), 30s (7.1), 40s (1.3), 50s (0.8), 60s (0.2) |
| BMI | 18.6 ± 3.64 | 11.7–52.5 | 2.27 ± 0.040 | 11.2 ± 0.080 | very underweight (38.1), underweight (20.8) normal weight (35.3), overweight (4.5), obese (1.2) |
| Sport | 1.42 ± 1.01 | 0–4 | 0.653 ± 0.040 | 0.0626 ± 0.080 | Never (16.1), Occasionally (44.5), 1–3 times/week (25.1), >3 times/week (10.2), Daily (4.0) |
| GHQ-12 | 6.81 ± 2.73 | 0–12 | −0.330 ± 0.040 | −0.276 ± 0.080 | under cut-off: 13.2 over cut-off: 86.8 |
| Body awareness | 3.89 ± 0.750 | 1–5 | −0.412 ± 0.040 | 0.234 ± 0.080 | 1 (0.3), 2 (3.2), 3 (23.3), 4 (54.1), 5 (19.1) |
| Relationship quality | 3.36 ± 0.839 | 0–4 | −1.56 ± 0.040 | 2.96 ± 0.080 | Very good (54.6), Good (33.9), Fair (10.3), Poor (1.2), Very poor (0.2) |
| F. of masturbation | 1.37 ± 0.734 | 0–3 | −0.170 ± 0.040 | −0.465 ± 0.080 | Never (11.8), Rarely (43.1), Often (41.6), Daily (3.5) |
| Sexual satisfaction | 3.93 ± 0.880 | 1–5 | −0.788 ± 0.040 | 0.712 ± 0.080 | / |
| F. of sexual intercourse | 2.72 ± 0.678 | 0–3 | −2.71 ± 0.040 | 7.02 ± 0.080 | No sexual activity (2.8), No complete sexual experience (3.3), Occasional sexual activity (12.4), Regular sexual activity (81.4) |
| Sexual Satisfaction | Body Awareness | Masturbation Frequency | Relationship Quality | F. of Sexual Intercourse | |
|---|---|---|---|---|---|
| Body Awareness | 0.169 *** | — | |||
| Masturbation Frequency | 0.025 | 0.223 *** | — | ||
| Relationship Quality | 0.341 *** | 0.052 ** | −0.016 | — | |
| F. of Sexual Intercourse | 0.421 *** | 0.120 *** | 0.004 | 0.239 *** | — |
| GHQ-12 Tot | −0.146 *** | −0.143 *** | 0.006 | −0.114 *** | −0.059 *** |
| Variable | Betweenness | Closeness | Strength | Expected Influence | Barrat | Zhang |
|---|---|---|---|---|---|---|
| RQ | −0.612 | −0.246 | −0.081 | 0.113 | 0.785 | 1.371 |
| Ma | −0.612 | −1.105 | −1.077 | −0.254 | −1.603 | −1.141 |
| FSI | −0.612 | 0.157 | 0.324 | 0.754 | 0.918 | 0.994 |
| SS | 1.725 | 1.571 | 1.700 | 1.204 | 0.359 | −0.485 |
| BA | 0.724 | 0.570 | 0.049 | −0.117 | −0.837 | −0.771 |
| GHQ | −0.612 | −0.948 | −0.915 | −1.700 | 0.377 | −0.031 |
| Type | Effect | Estimate ± SE | 95% CI | β | z | p |
|---|---|---|---|---|---|---|
| Indirect | GHQ ⇒ RQ ⇒ SS | −0.009 ± 0.001 | −0.012; −0.007 | −0.030 | −6.301 | <0.001 |
| GHQ ⇒ BA ⇒ SS | −0.005 ± 0.001 | −0.007; −0.003 | −0.015 | −5.391 | <0.001 | |
| GHQ ⇒ FSI ⇒ SS | −0.007 ± 0.002 | −0.011; −0.004 | −0.023 | −3.846 | <0.001 | |
| Ma ⇒ BA ⇒ SS | 0.027 ± 0.005 | 0.019; 0.037 | 0.023 | 5.908 | <0.001 | |
| Component | GHQ ⇒ RQ | −0.036 ± 0.005 | −0.045; −0.026 | −0.118 | −7.156 | <0.001 |
| RQ ⇒ SS | 0.263 ± 0.019 | 0.227; 0.300 | 0.253 | 14.119 | <0.001 | |
| GHQ ⇒ BA | −0.040 ± 0.004 | −0.048; −0.031 | −0.144 | −9.062 | <0.001 | |
| BA ⇒ SS | 0.119 ± 0.017 | 0.085; 0.154 | 0.104 | 6.769 | <0.001 | |
| GHQ ⇒ FSI | −0.015 ± 0.004 | −0.022; −0.008 | −0.064 | −3.945 | <0.001 | |
| FSI ⇒ SS | 0.480 ± 0.027 | 0.428; 0.533 | 0.357 | 17.817 | <0.001 | |
| Ma ⇒ BA | 0.228 ± 0.017 | 0.195; 0.261 | 0.222 | 13.305 | <0.001 | |
| Direct | GHQ ⇒ SS | −0.026 ± 0.005 | −0.035; −0.017 | −0.082 | −5.493 | <0.001 |
| Ma ⇒ SS | 0.002 ± 0.017 | −0.031; 0.037 | 0.002 | 0.142 | 0.887 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buattini, M.; Daminato, L.; Riboli, G.; Nese, M.; Brighetti, G.; Giunti, D.; Borlimi, R. Sexual Satisfaction in a Sample of Italian Women during the COVID-19 Lockdown Period. Sexes 2024, 5, 428-443. https://doi.org/10.3390/sexes5040031
Buattini M, Daminato L, Riboli G, Nese M, Brighetti G, Giunti D, Borlimi R. Sexual Satisfaction in a Sample of Italian Women during the COVID-19 Lockdown Period. Sexes. 2024; 5(4):428-443. https://doi.org/10.3390/sexes5040031
Chicago/Turabian StyleBuattini, Matilde, Luca Daminato, Greta Riboli, Mattia Nese, Gianni Brighetti, Daniel Giunti, and Rosita Borlimi. 2024. "Sexual Satisfaction in a Sample of Italian Women during the COVID-19 Lockdown Period" Sexes 5, no. 4: 428-443. https://doi.org/10.3390/sexes5040031
APA StyleBuattini, M., Daminato, L., Riboli, G., Nese, M., Brighetti, G., Giunti, D., & Borlimi, R. (2024). Sexual Satisfaction in a Sample of Italian Women during the COVID-19 Lockdown Period. Sexes, 5(4), 428-443. https://doi.org/10.3390/sexes5040031