
Effectiveness of an Unguided Online Intervention for Sexual Pleasure in Women: A Randomized Controlled Pilot Study

 ,
,
Abstract
1. Introduction
1.1. Sexual Pleasure in Sexual Health Interventions
1.2. Online Sexual Health Interventions
1.3. Sexual Pleasure and Sexocorporel
1.4. The Current Paper
2. Materials and Methods
2.1. Description of the Online Intervention PleaSure
- The first week focuses on mindful awareness of the body. The knowledge section includes information on mindfulness, the parasympathetic and sympathetic nervous systems, and Jacobsen’s progressive muscle relaxation (PMR); the link between body and mind is a key theme in Sexocorporel [48,52]. The exercises for this week are a mindful-based body scan and a PMR exercise [58] that treats the whole body including the genitals and can be listened to as audio or read as text.
- The second week focuses on exploring the vulva, as Sexocorporel assumes that the better the genital self-image is, the better the sexual experience will be [53]. Thus, general knowledge is provided about the vulva, and a summary of the OMGyes study describes various forms of genital stimulation [59]. The exercise is on genital self-image [58]. In the first part of the exercise, the vulva is explored with a hand mirror. In the second part of the exercise, the vulva is explored with the fingers.
- The third week focuses on the habitual arousal patterns and the variation of tension and relaxation of body regions that is integral to Sexocorporel practice [46,47]. Information was provided on arousal patterns and on the relationship between tension and relaxation. As an exercise, the participants were asked to masturbate while varying their habitual arousal patterns [51]. At the end of this step, the participants are encouraged to perform the exercise in couple sex as well. The participants receive input on the topic of consensus and communication in couple sex because it is known that experiences and skills acquired in solo sex can be transferred to couple sexuality [49].
- The fourth week focuses on the element movement and the body parts the pelvic floor and the inner vaginal space as these are central body regions for Sexocorporel [46,52]. The arousal modes were repeated, and reflection questions were asked about muscle tension during masturbation. The psychoeducative element relates to the pelvic floor, excessive muscle tension, and associated pain. An exercise on tensing and relaxing the pelvic floor provides a practical demonstration for the participant. In addition, the Sexocorporel double swing exercise [46] is introduced with a text and two videos. The double swing combines a movement of the pelvic swing with a movement of the chest, neck, and head [58] and is associated with greater physical and emotional intensity in sexual arousal [49]. Another exercise is the bullet fantasy journey exercise [58], which uses audio to help the participant imagine a ball making its way through her vagina.
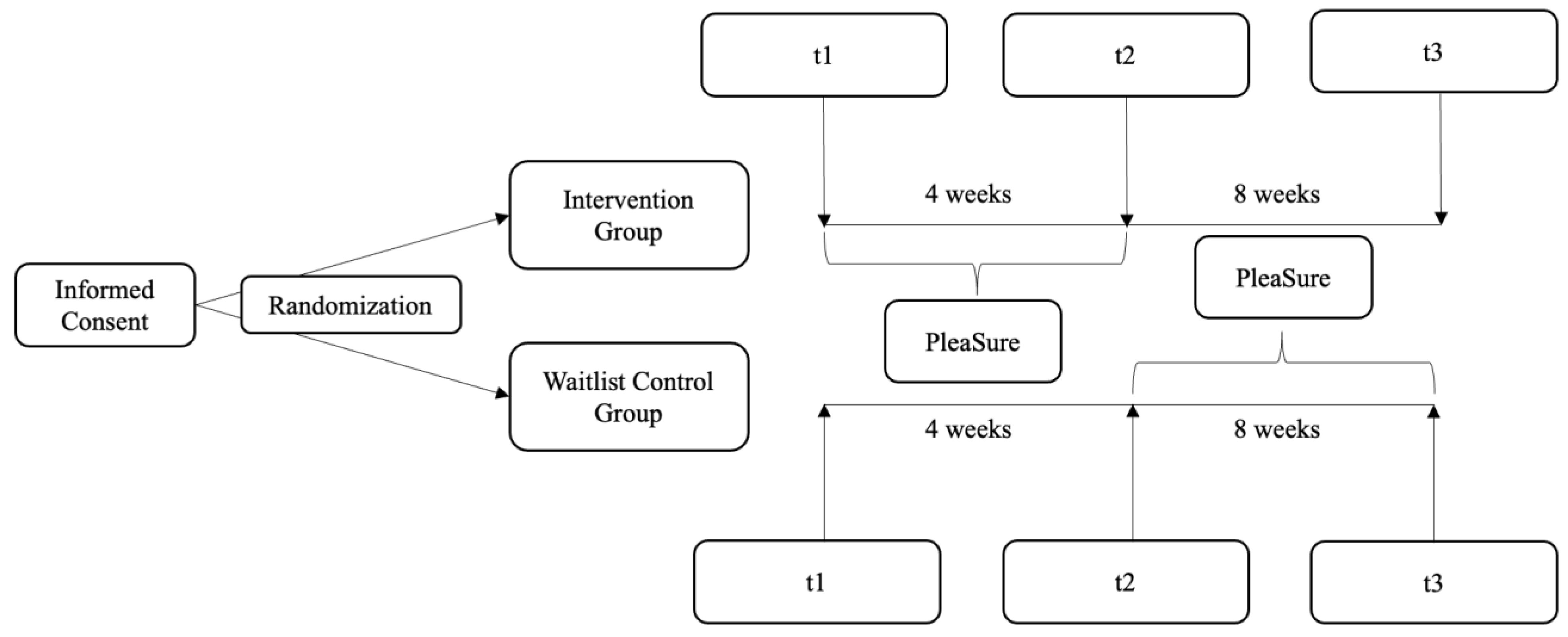
2.2. Procedure and Study Design
2.3. Measures
2.3.1. Demographic Data and Frequency of Sexual Behavior
2.3.2. Outcome Measure: Sexual Pleasure
- Sensual Pleasure: Level of pleasure experienced through sensual stimulation and its psychophysiological consequences (e.g., item 2: “Touching my erogenous zones was pleasurable.”). The reliability of the five-item scale was high (α = 0.80).
- Pleasure-Related Mastery: Level of experienced mastery in creating pleasurable sexual activities (e.g., item 6: “Shape my sex life in a way that I really enjoyed.”). The reliability of the six-item scale was high (α = 0.85).
- Pleasure-Related Validation: Level of perceived worthiness to experience positive sexual experiences and experienced self-validation during sex (e.g., item 12: “I thought it was important to live out my sexual needs.”). The reliability of the three-item scale was questionable (α = 0.66).
- Interaction Pleasure: Level of pleasure experienced during sharing pleasure and from interaction with a sexual partner (e.g., item 18: “During partner sex, we were both completely absorbed in pleasure.”). The reliability of the five-item scale was excellent (α = 0.90).
- Bonding Pleasure: Level of experienced (pleasure through) feelings of closeness, affection, safety, and security during sexual interactions (e.g., item 24: “Sex brought me closer to my sex partner.”). The reliability of the five-item scale was excellent α = 0.93.
- General Sexual Pleasure: Level of recently experienced pleasure related to different sexual activities (i.e., items 26 and 28: “Partner sex was pleasurable.” and “Masturbation was pleasurable.”). The reliability of the six-item scale was high (α = 0.84).
2.3.3. Compliance with and Evaluation of the Online Intervention PleaSure
2.4. Power Analysis
2.5. Statistical Analysis
3. Results
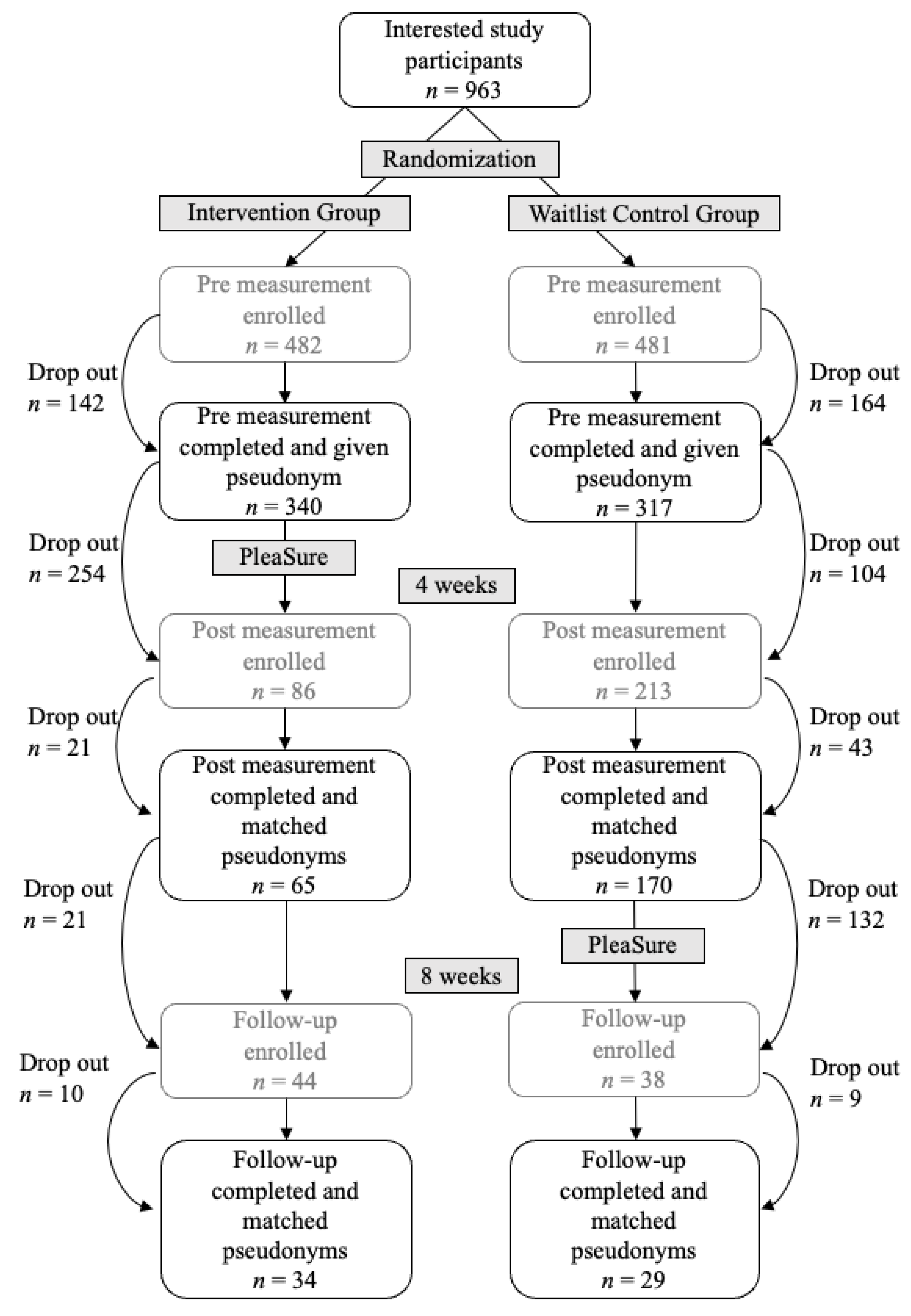
3.1. Participants
3.2. Randomization Check
3.3. Dropout Analysis
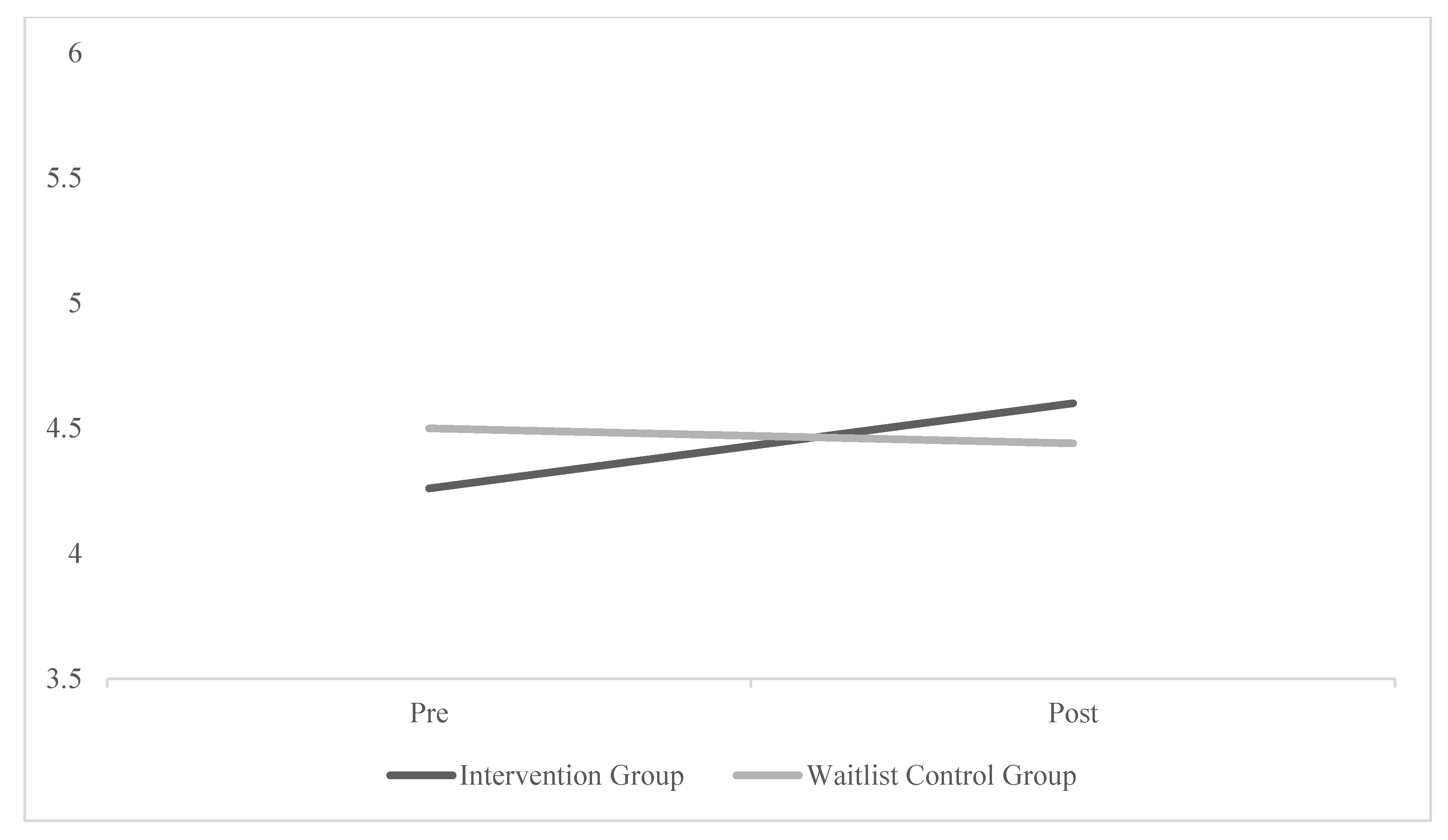
3.4. Effects at Postintervention: Mixed ANOVA with Repeated Measures
3.5. Stability of effects: One-Way ANOVAs with Repeated Measures
3.6. Compliance with and Evaluation of the Online Intervention
4. Discussion
Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Global Advisory Board for Sexual Health and Wellbeing. Working Definition of Sexual Pleasure. Available online: https://www.gab-shw.org/our-work/working-definition-of-sexual-pleasure/ (accessed on 12 September 2021).
- Hull, T.H. Sexual pleasure and wellbeing. Int. J. Sex. Health 2008, 20, 133–145. [Google Scholar] [CrossRef]
- Abramson, P.R.; Pinkerton, S.D. With Pleasure: Thoughts on the Nature of Human Sexuality; Oxford University Press: Oxford, UK, 2002. [Google Scholar]
- Meston, C.M.; Buss, D.M. Why humans have sex. Arch. Sex. Behav. 2007, 36, 477–507. [Google Scholar] [CrossRef] [PubMed]
- Van Lunsen, R.; Brauer, M.; Laan, E. Sex, pleasure and dyspareunia in liberal Northern Europe. In The Cultural Context of Sexual Pleasure and Problems; Routledge: Abington, UK, 2013. [Google Scholar]
- Werner, M.; Borgmann, M.; Laan, E. Sexual Pleasure Matters–and How to Define and Assess It too. A Conceptual Framework of Sexual Pleasure and the Sexual Response. Int. J. Sex. Health, 2023; Manuscript resubmitted for publication. [Google Scholar] [CrossRef]
- Goldey, K.L.; Posh, A.R.; Bell, S.N.; van Anders, S.M. Defining pleasure: A focus group study of solitary and partnered sexual pleasure in queer and heterosexual women. Arch. Sex. Behav. 2016, 45, 2137–2154. [Google Scholar] [CrossRef] [PubMed]
- Ford, J.V.; Vargas, E.C.; Finotelli, I., Jr.; Fortenberry, J.D.; Kismödi, E.; Philpott, A.; Rubio-Aurioles, E.; Coleman, E. Why pleasure matters: Its global relevance for sexual health, sexual rights and wellbeing. Int. J. Sex. Health 2019, 31, 217–230. [Google Scholar] [CrossRef]
- Gruskin, S.; Kismödi, E. A call for (renewed) commitment to sexual health, sexual rights, and sexual pleasure: A matter of health and well-being. Am. J. Public Health 2020, 110, 159–160. [Google Scholar] [CrossRef] [PubMed]
- Kismödi, E.; Corona, E.; Maticka-Tyndale, E.; Rubio-Aurioles, E.; Coleman, E. Sexual rights as human rights: A guide for the WAS declaration of sexual rights. Int. J. Sex. Health 2017, 29, 1–92. [Google Scholar] [CrossRef]
- Landers, S.; Kapadia, F. The public health of pleasure: Going beyond disease prevention. Am. J. Public Health 2020, 110, 140–141. [Google Scholar] [CrossRef]
- Mitchell, K.R.; Lewis, R.; O’Sullivan, L.F.; Fortenberry, J.D. What is sexual wellbeing and why does it matter for public health? Lancet Public Health 2021, 6, e608–e613. [Google Scholar] [CrossRef]
- Whipple, B.; Knowles, J.; Davis, J.; Koch, P.; Moglia, R.; Owens, A.; Golub, D. The Health Benefits of Sexual Expression [White Paper]; Updated 2007 by Gianotten, W.L. & Golub, D.; Planned Parenthood Federation of America, Inc.: New York, NY, USA; The Society for the Scientific Study of Sexuality: Whitehall, PA, USA, 2003. [Google Scholar]
- Anderson, R. Positive sexuality and its impact on overall well-being. Bundesgesundheitsblatt-Gesundh.-Gesundh. 2013, 56, 208–214. [Google Scholar] [CrossRef]
- Palmore, E.B. Predictors of the longevity difference: A 25-year follow-up. Gerontologist 1982, 22, 513–518. [Google Scholar] [CrossRef]
- Laan, E.T.; Klein, V.; Werner, M.A.; van Lunsen, R.H.; Janssen, E. In pursuit of pleasure: A biopsychosocial perspective on sexual pleasure and gender. Int. J. Sex. Health 2021, 33, 516–536. [Google Scholar] [CrossRef]
- Galinsky, A.M.; Sonenstein, F.L. The association between developmental assets and sexual enjoyment among emerging adults. J. Adolesc. Health 2011, 48, 610–615. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, D.T.; Kiefer, A.K.; Ybarra, O. Sexual submissiveness in women: Costs for sexual autonomy and arousal. Personal. Soc. Psychol. Bull. 2006, 32, 512–524. [Google Scholar] [CrossRef]
- Klein, V.; Laan, E.; Brunner, F.; Briken, P. Sexual Pleasure Matters (Especially for Women)—Data from the German Sexuality and Health Survey (GeSiD). Sex. Res. Soc. Policy 2022, 19, 1879–1887. [Google Scholar] [CrossRef]
- World Association for Sexual Health. The Sexual Health for the Millennium Declaration; WAS Newsletter; World Association for Sexual Health: Minneapolis, MN, USA, 2007; pp. 1–10. [Google Scholar]
- Becasen, J.S.; Ford, J.; Hogben, M. Sexual health interventions: A meta-analysis. J. Sex Res. 2015, 52, 433–443. [Google Scholar] [CrossRef] [PubMed]
- Hogben, M.; Ford, J.; Becasen, J.S.; Brown, K.F. A systematic review of sexual health interventions for adults: Narrative evidence. J. Sex Res. 2015, 52, 444–469. [Google Scholar] [CrossRef]
- Philpott, A.; Knerr, W.; Boydell, V. Pleasure and prevention: When good sex is safer sex. Reprod. Health Matters 2006, 14, 23–31. [Google Scholar] [CrossRef]
- Scott-Sheldon, L.A.; Johnson, B.T. Eroticizing creates safer sex: A research synthesis. J. Prim. Prev. 2006, 27, 619–640. [Google Scholar] [CrossRef]
- Zaneva, M.; Philpott, A.; Singh, A.; Larsson, G.; Gonsalves, L. What is the added value of incorporating pleasure in sexual health interventions? A systematic review and meta-analysis. PLoS ONE 2022, 17, e0261034. [Google Scholar] [CrossRef]
- Philpott, A.; Larsson, G.; Singh, A.; Zaneva, M.; Gonsalves, L. How to navigate a Blindspot: Pleasure in Sexual and Reproductive Health and Rights programming and research. Int. J. Sex. Health 2021, 33, 587–601. [Google Scholar] [CrossRef]
- Weitkamp, K.; Hänisch, I.; Heesch, S.-C. A controlled pilot study to test the online intervention self: Cervix focusing on cervical pain, numbness, sexual pleasure and well-being. Psychol. Sex. 2021, 12, 279–288. [Google Scholar] [CrossRef]
- van Lankveld, J. Internet-based interventions for women’s sexual dysfunction. Curr. Sex. Health Rep. 2016, 8, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Chisari, C.; McCracken, L.M.; Cruciani, F.; Moss-Morris, R.; Scott, W. Acceptance and Commitment Therapy for women living with Vulvodynia: A single-case experimental design study of a treatment delivered online. J. Context. Behav. Sci. 2022, 23, 15–30. [Google Scholar] [CrossRef]
- Stephenson, K.R.; Zippan, N.; Brotto, L.A. Feasibility of a cognitive behavioral online intervention for women with Sexual Interest/Arousal Disorder. J. Clin. Psychol. 2021, 77, 1877–1893. [Google Scholar] [CrossRef] [PubMed]
- Zarski, A.-C.; Berking, M.; Fackiner, C.; Rosenau, C.; Ebert, D.D. Internet-based guided self-help for vaginal penetration difficulties: Results of a randomized controlled pilot trial. J. Sex. Med. 2017, 14, 238–254. [Google Scholar] [CrossRef] [PubMed]
- Zarski, A.-C.; Berking, M.; Ebert, D.D. Efficacy of Internet-Based Guided treatment for Genito-Pelvic Pain/Penetration Disorder: Rationale, treatment Protocol, and Design of a randomized controlled trial. Front. Psychiatry 2018, 8, 260. [Google Scholar] [CrossRef]
- Jones, L.M.; McCabe, M.P. The effectiveness of an internet-based psychological treatment program for female sexual dysfunction. J. Sex. Med. 2011, 8, 2781–2792. [Google Scholar] [CrossRef]
- Van Lankveld, J.J.; Leusink, P.; Van Diest, S.; Gijs, L.; Slob, A.K. Internet-based brief sex therapy for heterosexual men with sexual dysfunctions: A randomized controlled pilot trial. J. Sex. Med. 2009, 6, 2224–2236. [Google Scholar] [CrossRef]
- Carswell, K.; McCarthy, O.; Murray, E.; Bailey, J.V. Integrating psychological theory into the design of an online intervention for sexual health: The sexunzipped website. JMIR Res. Protoc. 2012, 1, e2114. [Google Scholar] [CrossRef]
- Williamson, A.; Barbarin, A.; Campbell, B.; Campbell, T.; Franzen, S.; Reischl, T.M.; Zimmerman, M.; Veinot, T.C. Uptake of and Engagement with an Online Sexual Health Intervention (HOPE eIntervention) Among African American Young Adults: Mixed Methods Study. J. Med. Internet Res. 2021, 23, e22203. [Google Scholar] [CrossRef]
- van Clief, L.; Anemaat, E. Good sex matters: Pleasure as a driver of online sex education for young people. Gates Open Res. 2020, 3, 1480. [Google Scholar] [CrossRef]
- Martin, P.; Cousin, L.; Gottot, S.; Bourmaud, A.; de La Rochebrochard, E.; Alberti, C. Participatory interventions for sexual health promotion for adolescents and young adults on the internet: Systematic review. J. Med. Internet Res. 2020, 22, e15378. [Google Scholar] [CrossRef]
- Wadham, E.; Green, C.; Debattista, J.; Somerset, S.; Sav, A. New digital media interventions for sexual health promotion among young people: A systematic review. Sex. Health 2019, 16, 101–123. [Google Scholar] [CrossRef] [PubMed]
- Mustanski, B.; Greene, G.J.; Ryan, D.; Whitton, S.W. Feasibility, acceptability, and initial efficacy of an online sexual health promotion program for LGBT youth: The Queer Sex Ed intervention. J. Sex Res. 2015, 52, 220–230. [Google Scholar] [CrossRef]
- Buntrock, C.; Ebert, D.D.; Lehr, D.; Cuijpers, P.; Riper, H.; Smit, F.; Berking, M. Evaluating the efficacy and cost-effectiveness of web-based indicated prevention of major depression: Design of a randomised controlled trial. BMC Psychiatry 2014, 14, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Ebert, D.D.; Van Daele, T.; Nordgreen, T.; Karekla, M.; Compare, A.; Zarbo, C.; Brugnera, A.; Øverland, S.; Trebbi, G.; Jensen, K.L. Internet-and mobile-based psychological interventions: Applications, efficacy, and potential for improving mental health. Eur. Psychol. 2018, 23, 167–187. [Google Scholar] [CrossRef]
- Berger, T.; Krieger, T. Internet-Interventionen: Ein Überblick. PiD-Psychother. Dialog 2018, 19, 18–24. [Google Scholar] [CrossRef]
- Kirana, P.-S.; Gudeloglu, A.; Sansone, A.; Fode, M.; Reisman, Y.; Corona, G.; Burri, A. E-sexual health: A position statement of the European Society for Sexual Medicine. J. Sex. Med. 2020, 17, 1246–1253. [Google Scholar] [CrossRef]
- Hensel, D.J.; Von Hippel, C.D.; Sandidge, R.; Lapage, C.C.; Zelin, N.S.; Perkins, R.H. “OMG, Yes!”: Feasibility, Acceptability, and Preliminary Efficacy of an Online Intervention for Female Sexual Pleasure. J. Sex Res. 2022, 59, 269–282. [Google Scholar] [CrossRef]
- Bischof, K. Sexocorporel in the promotion of sexual pleasure. In Proceedings of the Nordic Association for Clinical Sexology (NACS), Helsinki, Finland, 3 September 2012; Volume 60. [Google Scholar]
- Desjardins, J.-Y. Approche intégrative et sexocorporelle. Sexologies 1996, 5, 43–48. [Google Scholar]
- Desjardins, J.-Y.; Chatton, D.; Desjardins, L.; Tremblay, M. Le sexocorporel. La compétence érotique à la portée de tous. In La Sexothérapie: Quelle Thérapie Choisir En Sexologie Clinique; De Boeck: Leuven-New, Belgium, 2010; Volume 2, pp. 63–103. [Google Scholar]
- Bischof-Campbell, A.; Hilpert, P.; Burri, A.; Bischof, K. Body Movement Is Associated with Orgasm During Vaginal Intercourse in Women. J. Sex Res. 2018, 56, 356–366. [Google Scholar] [CrossRef]
- de Carufel, F.; Trudel, G. Effects of a new functional-sexological treatment for premature ejaculation. J. Sex Marital Ther. 2006, 32, 97–114. [Google Scholar] [CrossRef] [PubMed]
- Schiftan, D. Coming Soon: Orgasmus ist Übungssache—In 10 Schritten zum Vaginalen Höhepunkt; Piper Verlag GmbH: München, Germany, 2018. [Google Scholar]
- Sztenc, M. (Ed.) Klappts? Vom Leistungssex zum Liebesspiel—Ein Übungsbuch für Männer; Hirzel Verlag: Stuttgart, Germany, 2020; Volume 2. [Google Scholar]
- Sparmann, J. Körperorientierte Ansätze für die Sexuelle Bildung Junger Frauen; Psychosozial-Verlag: Giessen, Germany, 2015; Volume 3. [Google Scholar]
- Hall, K.S. Cultural differences in the treatment of sex problems. Curr. Sex. Health Rep. 2019, 11, 29–34. [Google Scholar] [CrossRef]
- Laumann, E.O.; Paik, A.; Glasser, D.B.; Kang, J.-H.; Wang, T.; Levinson, B.; Moreira, E.D.; Nicolosi, A.; Gingell, C. A cross-national study of subjective sexual well-being among older women and men: Findings from the Global Study of Sexual Attitudes and Behaviors. Arch. Sex. Behav. 2006, 35, 143–159. [Google Scholar] [CrossRef] [PubMed]
- Mahar, E.A.; Mintz, L.B.; Akers, B.M. Orgasm equality: Scientific findings and societal implications. Curr. Sex. Health Rep. 2020, 12, 24–32. [Google Scholar] [CrossRef]
- Chatton, D.; Desjardins, J.-Y.; Desjardins, L.; Tremblay, M. La sexologie clinique basée sur un modèle de santé sexuelle. Psychothérapies 2005, 25, 3–19. [Google Scholar] [CrossRef]
- Sparmann, J. Lustvoll Körperwärts; Psychosozial-Verlag: Giessen, Germany, 2018. [Google Scholar]
- Herbenick, D.; Fu, T.-C.; Arter, J.; Sanders, S.A.; Dodge, B. Women’s experiences with genital touching, sexual pleasure, and orgasm: Results from a US probability sample of women ages 18 to 94. J. Sex Marital Ther. 2018, 44, 201–212. [Google Scholar] [CrossRef]
- Borgmann, M.; Werner, M.; Brandner, L.M.; D’Urso, D.; Gonin-Spahni, S.; Znoj, H.; Werner, M. A Psychometric Study of a Trait and State Assessment of Sexual Pleasure—The Amsterdam Sexual Pleasure Inventory (ASPI 1.0). J. Sex Res. 2023; manuscript submitted. [Google Scholar] [CrossRef]
- Jozkowski, K.N.; Sanders, S.A.; Rhoads, K.; Milhausen, R.R.; Graham, C.A. Examining the psychometric properties of the Sexual Excitation/Sexual Inhibition Inventory for Women (SESII-W) in a sample of lesbian and bisexual women. J. Sex Res. 2016, 53, 836–848. [Google Scholar] [CrossRef]
- Vigil, K.E.; de Jong, D.C.; Poovey, K.N. Roles of Genital Self-Image, Distraction, and Anxiety in Women’s Sexual Pleasure: A Preregistered Study. J. Sex Marital Ther. 2021, 47, 325–340. [Google Scholar] [CrossRef]
- Pascoal, P.M.; Sanchez, D.T.; Raposo, C.F.; Pechorro, P. Initial validation of the sexual pleasure scale in clinical and non-clinical samples of partnered heterosexual people. J. Sex. Med. 2016, 13, 1408–1413. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G* Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Spijkerman, M.; Pots, W.T.M.; Bohlmeijer, E. Effectiveness of online mindfulness-based interventions in improving mental health: A review and meta-analysis of randomised controlled trials. Clin. Psychol. Rev. 2016, 45, 102–114. [Google Scholar] [CrossRef] [PubMed]
- Swanton, R.; Allom, V.; Mullan, B. A meta-analysis of the effect of new-media interventions on sexual-health behaviours. Sex. Transm. Infect. 2015, 91, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Bailey, J.V.; Murray, E.; Rait, G.; Mercer, C.H.; Morris, R.W.; Peacock, R.; Cassell, J.; Nazareth, I. Interactive computer-based interventions for sexual health promotion. Cochrane Database Syst. Rev. 2010, 9, 1–68. [Google Scholar] [CrossRef]
- Tabachnick, B.G.; Fidell, L.S.; Ullman, J.B. Using Multivariate Statistics; Pearson: Boston, MA, USA, 2007; Volume 5. [Google Scholar]
- Blanca Mena, M.J.; Alarcón Postigo, R.; Arnau Gras, J.; Bono Cabré, R.; Bendayan, R. Non-normal data: Is ANOVA still a valid option? Psicothema 2017, 29, 552–557. [Google Scholar]
- Schmider, E.; Ziegler, M.; Danay, E.; Beyer, L.; Bühner, M. Is it really robust? Reinvestigating the robustness of ANOVA against violations of the normal distribution assumption. Methodol. Eur. J. Res. Methods Behav. Soc. Sci. 2010, 6, 147. [Google Scholar]
- Andrade, C. Multiple testing and protection against a type 1 (false positive) error using the Bonferroni and Hochberg corrections. Indian J. Psychol. Med. 2019, 41, 99–100. [Google Scholar] [CrossRef]
- Kislev, E. Does Marriage Really Improve Sexual Satisfaction? Evidence from the Pairfam Dataset. J. Sex Res. 2020, 57, 470–481. [Google Scholar] [CrossRef]
- Ritterband, L.M.; Thorndike, F.P.; Cox, D.J.; Kovatchev, B.P.; Gonder-Frederick, L.A. A behavior change model for internet interventions. Ann. Behav. Med. 2009, 38, 18–27. [Google Scholar] [CrossRef]
- Smith, A.; Lyons, A.; Ferris, J.; Richters, J.; Pitts, M.; Shelley, J.; Simpson, J.M. Sexual and relationship satisfaction among heterosexual men and women: The importance of desired frequency of sex. J. Sex Marital Ther. 2011, 37, 104–115. [Google Scholar] [CrossRef]
- Bodenmann, G.; Atkins, D.C.; Schär, M.; Poffet, V. The association between daily stress and sexual activity. J. Fam. Psychol. 2010, 24, 271. [Google Scholar] [CrossRef] [PubMed]
- Nowosielski, K.; Drosdzol, A.; Skrzypulec, V.; Plinta, R. Sexual satisfaction in females with premenstrual symptoms. J. Sex. Med. 2010, 7, 3589–3597. [Google Scholar] [CrossRef] [PubMed]
- Haning, R.V.; O’Keefe, S.L.; Randall, E.J.; Kommor, M.J.; Baker, E.; Wilson, R. Intimacy, orgasm likelihood, and conflict predict sexual satisfaction in heterosexual male and female respondents. J. Sex Marital Ther. 2007, 33, 93–113. [Google Scholar] [CrossRef] [PubMed]
- Andersson, G.; Titov, N. Advantages and limitations of Internet-based interventions for common mental disorders. World Psychiatry Off. J. World Psychiatr. Assoc. WPA 2014, 13, 4–11. [Google Scholar] [CrossRef] [PubMed]
- Gonin-Spahni, S.; Borgmann, M.; Brandner, L.M.; Inauen, M. Promotion of genital self-image: Effectiveness of exposure to genital photos and knowledge transfer. Univ. Bern, 2023; manuscript in preparation. [Google Scholar]
- Musiat, P.; Tarrier, N. Collateral outcomes in e-mental health: A systematic review of the evidence for added benefits of computerized cognitive behavior therapy interventions for mental health. Psychol. Med. 2014, 44, 3137–3150. [Google Scholar] [CrossRef] [PubMed]
- Melville, K.M.; Casey, L.M.; Kavanagh, D.J. Dropout from Internet-based treatment for psychological disorders. Br. J. Clin. Psychol. 2010, 49, 455–471. [Google Scholar] [CrossRef]
- Cavanagh, K. Turn on, tune in and (don’t) drop out: Engagement, adherence, attrition, and alliance with internet-based interventions. Oxf. Guide Low Intensity CBT Interv. 2010, 227, 232. [Google Scholar]
- Beckmeyer, J.J.; Herbenick, D.; Eastman-Mueller, H. Sexual pleasure during college students’ most recent partnered sexual experiences. J. Am. Coll. Health 2021, 1–12. [Google Scholar] [CrossRef]
- Bailey, J.; Mann, S.; Wayal, S.; Abraham, C.; Murray, E. Digital media interventions for sexual health promotion—Opportunities and challenges. BMJ 2015, 350, h1099. [Google Scholar] [CrossRef]
- Guse, K.; Levine, D.; Martins, S.; Lira, A.; Gaarde, J.; Westmorland, W.; Gilliam, M. Interventions using new digital media to improve adolescent sexual health: A systematic review. J. Adolesc. Health 2012, 51, 535–543. [Google Scholar] [CrossRef]
- Hobbs, L.J. Psychotherapeutic Interventions for Sexual Problems Delivered via the Internet: Effectiveness, Acceptability and Reach. Ph.D. Thesis, UCL (University College London), London, UK, 2016. [Google Scholar]
- Twist, M.L.; McArthur, N. Introduction to special issue on digihealth and sexual health. Sex. Relatsh. Ther. 2020, 35, 131–136. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Topic | Psychoeducative Elements | Exercises | Learning Outcomes (in This Week You …) | |
|---|---|---|---|---|
| Start | Basics | Important theories (embodiment, mindfulness, and Sexocorporel) and terms (gender and sexuality) Refresh anatomy knowledge (vulva, vagina, clitoris, and pelvic floor) | Reflect actual state of own sexuality Set personal goals | Reflect your current state in sexuality and set personal goals for yourself, how intensively you want to deal with the course and what you want to achieve in the further development of your sexuality. Refresh your knowledge of the anatomy of sex and perhaps learn something new about it. |
| 1st week | Perception of one’s own genitals | Exploration on mindfulness and progressive muscle relaxation (PMR) | Opening exercise: exploration with the hand Mindful body scan including the genitals | Refresh your knowledge about mindfulness. Perceive your body in its present state. Explore and observe your body in a mindful, non-judgmental, and curious way. |
| 2nd week | Discovery of one’s own genitals | Description of the vulva and different forms of genital stimulation | Mindful exploration of the vulva with a hand mirror Mindful exploration of the vulva with fingers | Recognize the diversity of different vulvas. Establish acceptance and a sense of pride towards your genitals. Learn about different aspects of genital touch and stimulation. |
| 3rd week | Arousal tension and relaxation | Description of sexual response cycle, orgasm, and arousal modes | Masturbation exercise Getting to know their own arousal modes | Learn theoretical background knowledge about the sexual response cycle and ways of increasing arousal. Get to know and expand your own arousal patterns through pleasant touch of the genitals and the whole body. |
| 4th week | Movement | Explanation of the pelvic floor, movement, and vagina | Tightening the pelvic floor Double swing Imagination to the inside of the vagina | Learn about the relevance and modulation of the pelvic floor. Learn that the increase in perception and arousal can be regulated by tension, relaxation, and movement of the pelvic floor. Feel the spread of sensory perception in the genitals with the help of movements of the pelvis and a fantasy journey. |
| Closing | Review | Encouraging further practice (also in couple sex) Further inspiration (links to info pages) | Review and reflection |
| Demographic Characteristic | IG | WCG | Significance Test | ||||||
|---|---|---|---|---|---|---|---|---|---|
| n | M/% | SD | n | M/% | SD | t | df | p | |
| Age | 340 | 31.20 | 8.79 | 317 | 31.75 | 8.77 | 0.80 | 655 | 0.425 |
| Education Level | 340 | 317 | 1.64 | 655 | 0.101 | ||||
| Higher Education or University | 229 | 67.4 | 224 | 70.7 | |||||
| College | 64 | 18.8 | 59 | 18.6 | |||||
| Apprenticeship | 43 | 12.6 | 28 | 8.8 | |||||
| Secondary school | 0 | 0.0 | 3 | 0.9 | |||||
| Other | 4 | 1.2 | 3 | 0.9 | |||||
| Sexual Orientation | 340 | 317 | −0.18 | 655 | 0.857 | ||||
| Heterosexual | 251 | 73.8 | 239 | 75.4 | |||||
| Bisexual | 64 | 18.8 | 56 | 17.7 | |||||
| Homosexual | 9 | 2.6 | 6 | 1.9 | |||||
| Other | 16 | 4.7 | 16 | 5.0 | |||||
| Relationship Status | 340 | 317 | 0.32 | 655 | 0.748 | ||||
| Yes | 225 | 66.2 | 206 | 65.0 | |||||
| No | 115 | 22.8 | 111 | 35.0 | |||||
| Frequency of Masturbation a | 340 | 3.05 | 0.74 | 317 | 2.98 | 0.75 | −1.14 | 655 | 0.257 |
| Frequency of Partnersex a | 340 | 3.24 | 0.72 | 317 | 3.21 | 0.71 | −0.48 | 655 | 0.632 |
| Pleasure-related Variables | |||||||||
| General Sexual Pleasure b | 336 | 4.68 | 0.90 | 314 | 4.59 | 1.01 | −1.19 | 648 | 0.235 |
| Sensual Pleasure b | 337 | 4.69 | 0.93 | 312 | 4.57 | 1.07 | −1.50 | 620 | 0.134 |
| Pleasure-related Mastery b | 331 | 4.45 | 1.01 | 300 | 4.45 | 1.09 | 0.05 | 629 | 0.960 |
| Pleasure-related Validation b | 332 | 4.39 | 1.20 | 311 | 4.32 | 1.28 | −0.72 | 641 | 0.471 |
| Interaction Pleasure b | 237 | 4.61 | 1.10 | 206 | 4.48 | 1.13 | −1.21 | 441 | 0.225 |
| Bonding Pleasure b | 237 | 4.97 | 1.03 | 206 | 4.91 | 1.18 | −0.54 | 441 | 0.589 |
| IG | WCG | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | Pre | Post | n | Pre | Post | |||||
| M | SD | M | SD | M | SD | M | SD | |||
| Sensual Pleasure | 57 | 4.55 | 1.03 | 4.75 | 0.88 | 148 | 4.59 | 1.03 | 4.60 | 1.04 |
| Pleasure-related Mastery | 54 | 4.26 | 1.23 | 4.60 | 1.08 | 140 | 4.50 | 1.05 | 4.44 | 1.05 |
| Pleasure-related Validation | 55 | 4.28 | 1.25 | 4.61 | 1.16 | 144 | 4.35 | 1.31 | 4.34 | 1.31 |
| Interaction Pleasure | 35 | 4.51 | 1.11 | 4.75 | 1.00 | 88 | 4.52 | 1.15 | 4.61 | 1.12 |
| Bonding Pleasure | 35 | 5.13 | 1.01 | 5.22 | 1.05 | 88 | 5.01 | 1.15 | 4.94 | 1.16 |
| General Sexual Pleasure | 56 | 4.70 | 1.01 | 4.85 | 0.82 | 148 | 4.66 | 0.93 | 4.65 | 0.97 |
| SS | F | df | η2 | p | ||
|---|---|---|---|---|---|---|
| Sensual Pleasure | time | 0.99 | 3.02 | 1, 203 | 0.015 | 0.084 |
| time × condition | 0.73 | 2.23 | 1, 203 | 0.011 | 0.137 | |
| Pleasure-related Mastery | time | 1.60 | 5.22 | 1, 192 | 0.026 | 0.023 |
| time × condition | 3.30 | 10.77 | 1, 192 | 0.053 | 0.001 | |
| Pleasure-related Validation | time | 2.06 | 3.32 | 1, 197 | 0.017 | 0.070 |
| time × condition | 2.37 | 3.81 | 1, 197 | 0.019 | 0.052 | |
| Interaction Pleasure | time | 1.32 | 4.80 | 1, 121 | 0.038 | 0.030 |
| time × condition | 0.26 | 0.93 | 1, 121 | 0.008 | 0.336 | |
| Bonding Pleasure | time | 0.01 | 0.02 | 1, 121 | 0.000 | 0.888 |
| time × condition | 0.30 | 0.10 | 1, 121 | 0.008 | 0.320 | |
| General Sexual Pleasure | time | 0.42 | 1.39 | 1, 202 | 0.007 | 0.241 |
| time × condition | 0.46 | 1.51 | 1, 202 | 0.007 | 0.220 |
| n | Pre | Post | Follow-Up | ||||
|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | ||
| Sensual Pleasure | 30 | 4.39 | 1.13 | 4.68 | 1.03 | 4.66 | 1.00 |
| Pleasure-related Mastery | 29 | 4.18 | 1.24 | 4.52 | 1.20 | 4.63 | 1.03 |
| Pleasure-related Validation | 29 | 4.37 | 1.23 | 4.63 | 1.09 | 4.67 | 1.21 |
| Interaction Pleasure | 19 | 4.45 | 1.08 | 4.63 | 1.00 | 4.59 | 1.07 |
| Bonding Pleasure | 19 | 5.06 | 0.96 | 5.07 | 1.16 | 5.00 | 0.95 |
| General Sexual Pleasure | 29 | 4.67 | 0.99 | 4.86 | 0.93 | 4.70 | 0.92 |
| SS | F | Df | η2 | p | |
|---|---|---|---|---|---|
| Sensual Pleasure | 1.54 | 2.66 | 2, 58 | 0.084 | 0.079 |
| Pleasure-Related Mastery | 3.14 | 4.04 | 2, 56 | 0.126 | 0.033 a |
| Pleasure-Related Validation | 1.55 | 1.41 | 2, 56 | 0.048 | 0.252 |
| Interaction Pleasure | 0.33 | 0.65 | 2, 36 | 0.035 | 0.527 |
| Bonding Pleasure | 0.06 | 0.10 | 2, 36 | 0.006 | 0.905 |
| General Sexual Pleasure | 0.60 | 1.12 | 2, 56 | 0.038 | 0.334 |
| Quote 1 | “I have a totally new view of my sexuality. Before, it all scared me and today, I know exercises and steps to approach it. I have sex very differently than before this month”. |
| Quote 2 | “At the beginning of the month, I perceived the lack of a (sexual) partner as something negative [...], now I still wish for someone with whom I could try out what I have learned here, but at the same time, I am much more in tune with myself and I am satisfied in and with my sexuality”. |
| Quote 3 | “That I found my way back to more pleasurable masturbation and was ready to explore myself in a new way”. |
| Quote 4 | “The relationship with my sexuality has strengthened in a positive way just by dealing with myself and the gained knowledge through the program”. |
| Quote 5 | “Recognizing one’s own sexual needs and seeing them as normal. Learning to control arousal and feeling that you can actively influence it during couple sex and have it in your own hands”. |
| Quote 6 | “I found it easier to talk about it [sexuality]. I am more open. I use my toy differently. I try to stimulate myself in a more varied way. I try to be more aware of my body, to breathe more and to use my body differently. I would say that I have more confidence to express my needs and fears to my partner”. |
| Quote 7 | “I feel much more comfortable with my genitals than before the program”. |
| Quote 8 | “I experienced an orgasm for the first time”. |
| Quote 9 | “I was never dissatisfied with my vulva, but I didn’t pay any more attention to it than I did during masturbation. Now I’m proud of it, I know exactly how it looks when I’m not aroused, when I’m aroused, and even when I have an orgasm”. |
| Quote 10 | “Knowing what my vulva really looks like and finding her beautiful has had a positive effect on masturbation and couple sexuality. I have become more confident in this regard and can generally enjoy my sexuality more”. |
| Quote 11 | “Realization that I am fully functional after all”. |
| Quote 12 | “A new area is opening up in my sexuality!” |
| Quote 13 | “The change has been significant for me because now instead of a feeling of lack dominating my thoughts, I feel complete and good about the way my life is right now.” |
| Quote 14 | “It has brought us once again after 16 years of relationship even closer to each other and we enjoy our sexuality more than ever.” |
| Quote 15 | “Now I can finally live and feel myself. (put harshly—but true)”. |
| Quote 16 | “I found it frightening how little I had dealt with it before and what a big positive difference the confrontation with the vulva makes in my sexual life, but also in my normal life”. |
| Quote 17 | “Because I feel more and more that I can perceive and acknowledge my needs and feelings better and better, and it is becoming easier and easier for me to show and communicate what is good for me, what I want, and where my limits are”. |
| Quote 18 | “Sexuality was previously very shameful. I felt somewhat exposed and passive with regard to the speed and sequence of the build-up of arousal. I can now actively control this better”. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borgmann, M.; Brandner, L.M.; Affolter, L.; Vonesch, J.; Gonin-Spahni, S. Effectiveness of an Unguided Online Intervention for Sexual Pleasure in Women: A Randomized Controlled Pilot Study. Sexes 2023, 4, 133-154. https://doi.org/10.3390/sexes4010012
Borgmann M, Brandner LM, Affolter L, Vonesch J, Gonin-Spahni S. Effectiveness of an Unguided Online Intervention for Sexual Pleasure in Women: A Randomized Controlled Pilot Study. Sexes. 2023; 4(1):133-154. https://doi.org/10.3390/sexes4010012
Chicago/Turabian StyleBorgmann, Michèle, Lucca Michelle Brandner, Linda Affolter, Julia Vonesch, and Stefanie Gonin-Spahni. 2023. "Effectiveness of an Unguided Online Intervention for Sexual Pleasure in Women: A Randomized Controlled Pilot Study" Sexes 4, no. 1: 133-154. https://doi.org/10.3390/sexes4010012
APA StyleBorgmann, M., Brandner, L. M., Affolter, L., Vonesch, J., & Gonin-Spahni, S. (2023). Effectiveness of an Unguided Online Intervention for Sexual Pleasure in Women: A Randomized Controlled Pilot Study. Sexes, 4(1), 133-154. https://doi.org/10.3390/sexes4010012