
Exploring the Linkages between Substance Use, Natural Disasters, Pandemics, and Intimate Partner Violence against Women: A Rapid Review in the Context of COVID-19

 , , and
, , and 
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
- RQ1: What is the relationship between natural disasters or pandemics on women’s experiences of IPV?
- RQ2: What is the relationship between substance use and women’s experiences of IPV?
2.2. Eligibility Criteria
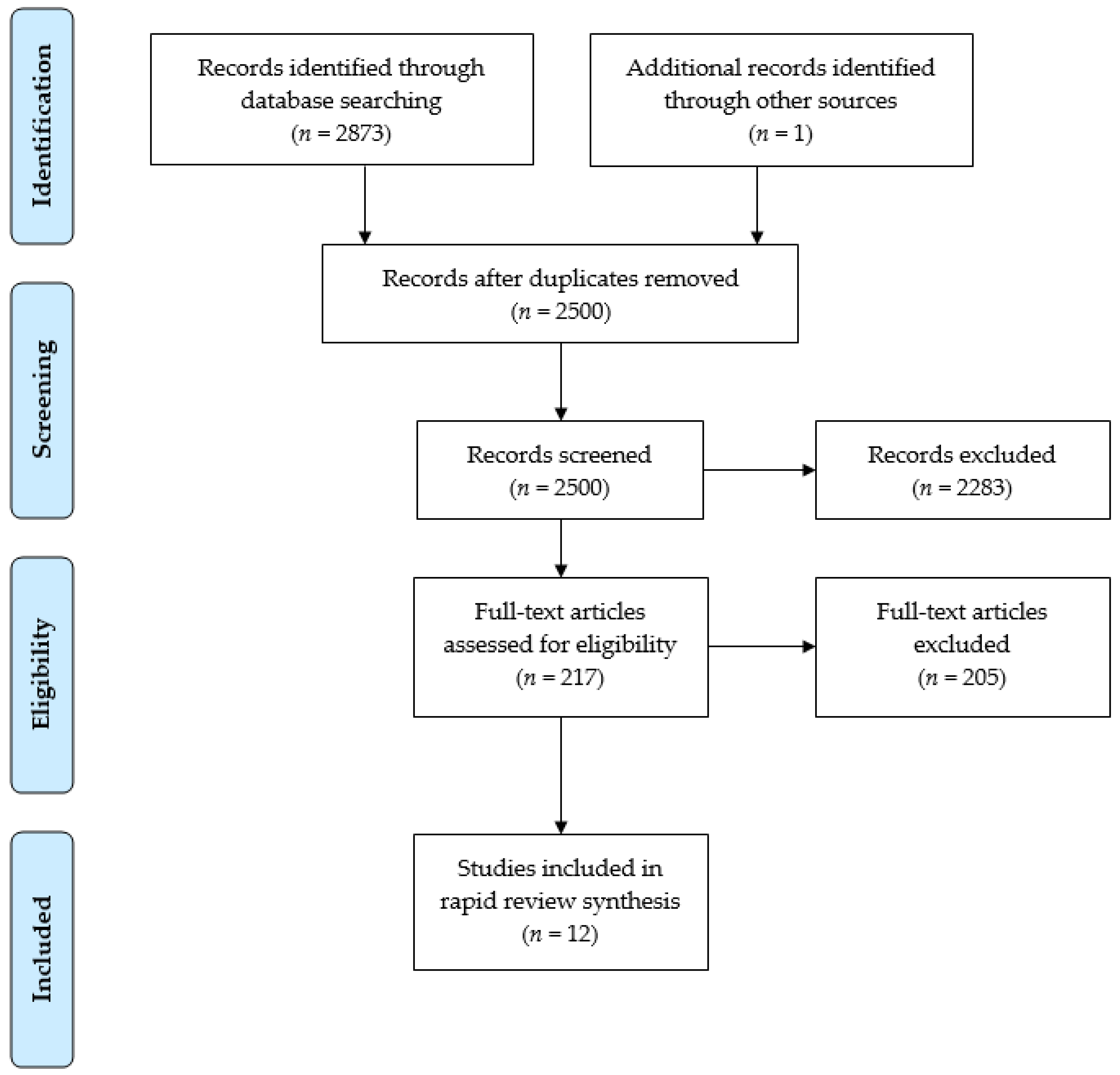
2.3. Study Selection
2.4. Quality Appraisal
3. Results
3.1. The Relationships between Natural Disasters and/or Pandemics and IPV
3.1.1. Mechanisms of IPV in the Natural Disaster and/or Pandemic Context
3.1.2. IPV and Women’s Health in a Disaster/Pandemic Context
3.2. The Relationships between Substance Use and IPV
3.2.1. Alcohol and IPV
3.2.2. Tobacco and IPV
3.2.3. Multiple Substance Use and IPV
3.2.4. The Mechanisms of IPV and Substance Use
3.3. The Mechanisms of IPV and Alcohol
4. Discussion
4.1. Developing IPV Services That Are Responsive to Women’s Needs
4.2. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- World Health Organization. Violence Against Women; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- World Health Organization. Understanding and Addressing Violence against Women: Intimate Partner Violence; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- UN Women. COVID-19 and Ending Violence Against Women and Girls; UN Women: New York, NY, USA, 2020; p. 10. [Google Scholar]
- Statistics Canada. Canadian Perspectives Survey Series 1: Impacts of COVID-19; Statistics Canada: Ottawa, ON, Canada, 2020. [Google Scholar]
- Williams, E.E.; Arant, K.R.; Leifer, V.P.; Balcom, M.C.; Levy-Carrick, N.C.; Lewis-O’Connor, A.; Katz, J.N. Provider perspectives on the provision of safe, equitable, trauma-informed care for intimate partner violence survivors during the COVID-19 pandemic: A qualitative study. BMC Women’s Health 2021, 21, e315. [Google Scholar] [CrossRef] [PubMed]
- Quintana-Domeque, C.; Carvalho, J.R.; de Oliveira, V.H. Zika virus incidence, preventive and reproductive behaviors: Correlates from new survey data. Econ. Hum. Biol. 2018, 30, 14–23. [Google Scholar] [CrossRef] [PubMed]
- Yasmin, S. The Ebola Rape Epidemic No One’s Talking About; Foreign Policy: Monrovia, Liberia, 2016. [Google Scholar]
- John, N.; Casey, S.E.; Carino, G.; McGovern, T. Lessons Never Learned: Crisis and gender-based violence. Dev. World Bioeth. 2020, 20, 65–68. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, R.A.; Genois, R.; Jin, J.; Vigo, D.; Rehm, J.; Rush, B. The early impact of COVID-19 on the incidence, prevalence, and severity of alcohol use and other drugs: A systematic review. Drug Alcohol Depend. 2021, 228, 109065. [Google Scholar] [CrossRef]
- Public Health Agency of Canada. Apparent Opioid and Stimulant Toxicity Deaths: Surveillance of Opioid and Stimulant-Related Harms in CANADA; Public Health Agency of Canada: Ottawa, ON, Canada, 2021. [Google Scholar]
- Leger. Mental Health and Substance Use during COVID-19: Summary Report 2-Spotlight on Gender and Household Size; Canadian Centre on Substance Use and Addiction & Mental Health Commission of Canada: Ottawa, ON, Canada, 2021. [Google Scholar]
- National Domestic Violence Hotline. COVID-19 Special Report; National Domestic Violence Hotline: Austin, TX, USA, 2020. [Google Scholar]
- Trudell, A.L.; Whitmore, E. Pandemic meets Pandemic: Understanding the Impacts of COVID19 on Gender-Based Violence Services and Survivors in Canada; Ending Violence Association of Canada & Anova: Ottawa, ON, Canada; London, ON, Canada, 2020. [Google Scholar]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef]
- Tricco, A.C.; Antony, J.; Zarin, W.; Strifler, L.; Ghassemi, M.; Ivory, J.; Perrier, L.; Hutton, B.; Moher, D.; Straus, S.E. A scoping review of rapid review methods. BMC Med. 2015, 13, 1–15. [Google Scholar] [CrossRef]
- Hong, Q.N.; Gonzalez-Reyes, A.; Pluye, P. Improving the usefulness of a tool for appraising the quality of qualitative, quantitative and mixed methods studies, the Mixed Methods Appraisal Tool (MMAT). J. Eval. Clin. Pract. 2018, 24, 459–467. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Sabri, B.; Hartley, M.; Saha, J.; Murray, S.; Glass, N.; Campbell, J.C. Effect of COVID-19 pandemic on women’s health and safety: A study of immigrant survivors of intimate partner violence. Health Care Women Int. 2020, 41, 1294–1312. [Google Scholar] [CrossRef]
- Anastario, M.; Shehab, N.; Lawry, L. Increased Gender-based Violence Among Women Internally Displaced in Mississippi 2 Years Post–Hurricane Katrina. Disaster Med. Public Health Prep. 2009, 3, 18–26. [Google Scholar] [CrossRef]
- Parkinson, D.; Zara, C. The hidden disaster: Domestic violence in the aftermath of natural disaster. Aust. J. Emerg. Manag. 2013, 28, 28–35. [Google Scholar]
- Schumacher, J.A.; Coffey, S.F.; Norris, F.H.; Tracy, M.; Clements, K.; Galea, S. Intimate Partner Violence and Hurricane Katrina: Predictors and Associated Mental Health Outcomes. Violence Vict. 2010, 25, 588–603. [Google Scholar] [CrossRef]
- Frasier, P.Y.; Belton, L.; Hooten, E.; Campbell, M.K.; DeVellis, B.; Benedict, S.; Carrillo, C.; Gonzalez, P.; Kelsey, K.; Meier, A. Disaster Down East: Using Participatory Action Research to Explore Intimate Partner Violence in Eastern North Carolina. Health Educ. Behav. 2004, 31, 69S–84S. [Google Scholar] [CrossRef]
- Parkinson, D. Investigating the Increase in Domestic Violence Post Disaster: An Australian Case Study. J. Interpers. Violence 2019, 34, 2333–2362. [Google Scholar] [CrossRef]
- Buttell, F.P.; Carney, M.M. Examining the impact of Hurricane Katrina on police responses to domestic violence. Traumatology 2009, 15, 6–9. [Google Scholar] [CrossRef]
- Harville, E.W.; Taylor, C.; Tesfai, H.; Xiong, X.; Buekens, P. Experience of Hurricane Katrina and Reported Intimate Partner Violence. J. Interpers. Violence 2010, 26, 833–845. [Google Scholar] [CrossRef]
- Taft, C.T.; Monson, C.M.; Schumm, J.A.; Watkins, L.E.; Panuzio, J.; Resick, P.A. Posttraumatic Stress Disorder Symptoms, Relationship Adjustment, and Relationship Aggression in a Sample of Female Flood Victims. J. Fam. Violence 2009, 24, 389–396. [Google Scholar] [CrossRef][Green Version]
- Lewis, M.W.; Cavanagh, P.K.; Ahn, G.; Yoshioka, M.R. Subjective effect of September 11, 2001 among pregnant women: Is cumulative history of interpersonal violence important? J. Interpers. Violence 2008, 23, 780–797. [Google Scholar] [CrossRef]
- Tedor, M.F.; Quinn, L.M.; Wilsnack, S.C.; Wilsnack, R.W.; Greenfield, T.K. Gender and Country Differences in Alcohol-Aggression Expectancy and Alcohol-Related Intimate Partner Violence. Deviant Behav. 2017, 39, 554–575. [Google Scholar] [CrossRef]
- Ahmadabadi, Z.; Najman, J.M.; Williams, G.M.; Clavarino, A.M.; D’Abbs, P.; Smirnov, A. Intimate partner violence in emerging adulthood and subsequent substance use disorders: Findings from a longitudinal study. Addiction 2019, 114, 1264–1273. [Google Scholar] [CrossRef]
- Bosch, J.; Weaver, T.L.; Arnold, L.D.; Clark, E.M. The Impact of Intimate Partner Violence on Women’s Physical Health: Findings from the Missouri Behavioral Risk Factor Surveillance System. J. Interpers. Violence 2015, 32, 3402–3419. [Google Scholar] [CrossRef]
- Suparare, L.; Watson, S.; Binns, R.; Frayne, J.; Galbally, M. Is intimate partner violence more common in pregnant women with severe mental illness? A retrospective study. Int. J. Soc. Psychiatry 2020, 66, 225–231. [Google Scholar] [CrossRef]
- Soccio, J.; Brown, M.; Comino, E.; Friesen, E. Pap smear screening, pap smear abnormalities and psychosocial risk factors among women in a residential alcohol and drug rehabilitation facility. J. Adv. Nurs. 2015, 71, 2858–2866. [Google Scholar] [CrossRef]
- Ullman, S.E.; Sigurvinsdottir, R. Intimate Partner Violence and Drinking among Victims of Adult Sexual Assault. J. Aggress. Maltreatment Trauma 2015, 24, 117–130. [Google Scholar] [CrossRef]
- Reichel, D. Determinants of Intimate Partner Violence in Europe: The Role of Socioeconomic Status, Inequality, and Partner Behavior. J. Interpers. Violence 2017, 32, 1853–1873. [Google Scholar] [CrossRef]
- Gobin, R.L.; Green, K.E.; Iverson, K.M. Alcohol Misuse Among Female Veterans: Exploring Associations with Interpersonal Violence and Mental Health. Subst. Use Misuse 2015, 50, 1765–1777. [Google Scholar] [CrossRef]
- Curtis, A.; Vadenberg, B.; Mayshak, R.; Coomber, K.; Hyder, S.; Walker, A.; Liknaitzky, P.; Miller, P.G. Alcohol use in family, domestic and other violence: Findings from a cross-sectional survey of the Australian population. Drug Alcohol Rev. 2019, 38, 349–358. [Google Scholar] [CrossRef]
- Crespo, M.; Soberón, C.; Fernández-Lansac, V. Alcohol and psychotropic substance use in female Spanish victims of intimate partner violence. Psicothema 2017, 29, 191–196. [Google Scholar] [CrossRef]
- Nemeth, J.M.; Bonomi, A.E.; Lu, B.; Lomax, R.G.; Wewers, M.E. Risk Factors for Smoking in Rural Women: The Role of Gender-Based Sexual and Intimate Partner Violence. J. Women’s Health 2016, 25, 1282–1291. [Google Scholar] [CrossRef]
- Alhusen, J.L.; Geller, R.; Jellig, J.; Budhathoki, C.; Decker, M. Intimate Partner Violence, Small for Gestational Age Birth and Cigarette Smoking in the Pregnancy Risk Assessment Monitoring System. J. Women’s Health 2018, 27, 458–465. [Google Scholar] [CrossRef]
- Mishra, G.; Chung, H.-F.; Gelaw, Y.A.; Loxton, D. The role of smoking in the relationship between intimate partner violence and age at natural menopause: A mediation analysis. Women’s Midlife Health 2018, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, T.P.; Flanagan, J.C.; Dudley, D.N.; Holt, L.J.; Mazure, C.M.; McKee, S.A. Correlates of smoking status among women experiencing intimate partner violence: Substance use, posttraumatic stress, and coping. Am. J. Addict. 2015, 24, 546–553. [Google Scholar] [CrossRef] [PubMed]
- Flanagan, J.C.; Hakes, J.K.; McClure, E.; Ma, A.L.S.; Back, S.E. Effects of intimate partner violence, PTSD, and alcohol use on cigarette smoking in a nationally representative sample. Am. J. Addict. 2016, 25, 283–290. [Google Scholar] [CrossRef]
- Decker, M.R.; Benning, L.; Webner, K.M.; Sherman, S.G.; Adedimeji, A.; Wilson, T.E.; Cohen, J.; Plankey, M.W.; Cohen, M.H.; Golub, E.T. Physical and sexual violence predictors: 20 years of the women’s interagency HIV study cohort. Am. J. Prev. Med. 2016, 51, 731–742. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Decker, M.R.; Park, J.N.; Allen, S.T.; Silberzahn, B.; Footer, K.; Huettner, S.; Galai, N.; Sherman, S.G. Inconsistent Condom Use Among Female Sex Workers: Partner-specific Influences of Substance Use, Violence, and Condom Coercion. AIDS Behav. 2019, 24, 762–774. [Google Scholar] [CrossRef] [PubMed]
- Caldentey, C.; Tirado-Munoz, J.; Ferrer, T.; Fonesca, F.; Rossi, P.; Mestre-Pinto, J.I. Intimate partner violence among female drug users admitted to the general hospital: Screening and prevalence. Adicciones 2017, 29, 172–179. [Google Scholar] [CrossRef] [PubMed]
- Low, S.; Tiberio, S.S.; Shortt, J.W.; Capaldi, D.M.; Eddy, J.M. Associations of couples’ intimate partner violence in young adulthood and substance use: A dyadic approach. Psychol. Violence 2017, 7, 120–127. [Google Scholar] [CrossRef]
- Kontautaite, A.; Matyushina-Ocheret, D.; Plotko, M.; Golichenko, M.; Kalvet, M.; Antonova, L. Study of human rights violations faced by women who use drugs in Estonia. Harm Reduct. J. 2018, 15, 54. [Google Scholar] [CrossRef]
- Sullivan, T.P.; Weiss, N.H.; Flanagan, J.C.; Willie, T.C.; Armeli, S.; Tennen, H. PTSD and Daily Co-Occurrence of Drug and Alcohol Use Among Women Experiencing Intimate Partner Violence. J. Dual Diagn. 2016, 12, 36–42. [Google Scholar] [CrossRef]
- Sherrill, A.M.; Bell, K.M.; Wyngarden, N. A Qualitative Examination of Situational Risk Recognition Among Female Victims of Physical Intimate Partner Violence. Violence Against Women 2015, 22, 966–985. [Google Scholar] [CrossRef]
- Cunradi, B.C.; Todd, M.; Mair, C. Discrepant patterns of heavy drinking, marijuana use, and smoking and intimate partner violence: Results from the California community health study of couples. J. Drug Educ. 2015, 45, 73–95. [Google Scholar] [CrossRef]
- Nydegger, L.A.; Claborn, K.R. Exploring patterns of substance use among highly vulnerable Black women at-risk for HIV through a syndemics framework: A qualitative study. PLoS ONE 2020, 15, e0236247. [Google Scholar] [CrossRef]
- Bunker, N.; Woods, C.; Conway, J.; Barker, R.; Usher, K. Patterns of ‘at-home’ alcohol-related injury presentations to emergency departments. J. Clin. Nurs. 2016, 26, 157–169. [Google Scholar] [CrossRef]
- O’Brien, J.E.; Ermentrout, D.; Rizo, C.F.; Li, W.; Macy, R.J.; Dababnah, S. “I never knew which way he would swing…:” Exploring the Roles of Substances in the Lives of System-Involved Intimate Partner Violence Survivors. J. Fam. Violence 2015, 31, 61–73. [Google Scholar] [CrossRef]
- Bonomi, A.; Nichols, E.; Kammes, R.; Chugani, C.D.; De Genna, N.M.; Jones, K.; Miller, E. Alcohol Use, Mental Health Disability, and Violence Victimization in College Women: Exploring Connections. Violence Against Women 2018, 24, 1314–1326. [Google Scholar] [CrossRef]
- Yalch, M.M.; Levendosky, A.A. Main and moderating effects of temperament traits on the association between intimate partner violence and hazardous alcohol use in a sample of young adult women. Psychol. Trauma Theory Res. Pract. Policy 2018, 10, 611–618. [Google Scholar] [CrossRef]
- Sanz-Barbero, B.; Pereira, P.L.; Barrio, G.; Vives-Cases, C. Intimate partner violence against young women: Prevalence and associated factors in Europe. J. Epidemiol. Community Health 2018, 72, 611–616. [Google Scholar] [CrossRef]
- Mumford, E.A.; Liu, W.; Joseph, H. Postpartum Domestic Violence in Homes With Young Children: The Role of Maternal and Paternal Drinking. Violence Against Women 2016, 24, 144–162. [Google Scholar] [CrossRef]
- Wilson, I.M.; Eurenius, E.; Lindkvist, M.; Edin, K.; Edvardsson, K. Is there an association between pregnant women’s experience of violence and their partner’s drinking? A Swedish population-based study. Midwifery 2019, 69, 84–91. [Google Scholar] [CrossRef]
- Wilson, M.I.; Graham, K.; Taft, A. Living the cycle of drinking and violence: A qualitative study of women’s experience of alcohol-related intimate partner violence. Drug Alcohol Rev. 2017, 36, 115–124. [Google Scholar] [CrossRef]
- Fanslow, J.; Gulliver, P.; Janet, F.; Pauline, G. Exploring Risk and Protective Factors for Recent and Past Intimate Partner Violence Against New Zealand Women. Violence Vict. 2015, 30, 960–983. [Google Scholar] [CrossRef]
- Arpa, S. Women who Use Drugs: Issues, Needs, Responses, Challenges, and Implications for Policy and Practice; European Monitoring Centre for Drugs and Drug Addiction: Lisbon, Portugal, 2017. [Google Scholar]
- Canadian Women’s Foundation and BC Society of Transition Houses. Report on Violence Against Women, Mental Health and Substance Use; Canadian Women’s Foundation and BC Society of Transition Houses: Toronto, ON, Canada; Vancouver, BC, Canada, 2011. [Google Scholar]
- Drugscope and London Drug and Alcohol Network. Making the Connection: Developing Integrated Approaches to Domestic Violence and Substance Use; Drugscope and London Drug and Alcohol Network: London, UK, 2013. [Google Scholar]
- Moyser, M. Gender Differences in Mental Health during the COVID-19 Pandemic; Statistics Canada: Ottawa, ON, Canada, 2020. [Google Scholar]
- Machisa, M.; Shamu, S. Mental ill health and factors associated with men’s use of intimate partner violence in Zimbabwe. BMC Public Health 2018, 18, 376. [Google Scholar] [CrossRef]
- De Mattos Russo Rafael, R.; Miranda Soares de Moura, A.T. Relationship between alcohol consumption and violence between intimate partners: A sectional study. Online Braz. J. Nurs. 2016, 15, 617–623. [Google Scholar]
- Zhang, C.; Li, X.; Su, S.; Hong, Y.; Zhou, Y.; Tang, Z.; Shen, Z. Violence against Chinese female sex workers from their stable partners: A hierarchical multiple regression analysis. Health Care Women Int. 2013, 36, 797–815. [Google Scholar] [CrossRef] [PubMed]
- Adjah, E.S.O.; Agbemafle, I. Determinants of domestic violence against women in Ghana. BMC Public Health 2016, 16, 368. [Google Scholar] [CrossRef] [PubMed]
- Zipursky, J.S.; Stall, N.M.; Silverstein, W.K.; Huang, M.Q.; Chau, B.J.; Hillmer, M.M.P.; Redelmeier, D.A. Alcohol Sales and Alcohol-Related Emergencies During the COVID-19 Pandemic. Ann. Intern. Med. 2021, 174, 1029–1032. [Google Scholar] [CrossRef] [PubMed]
- Enarson, E. Violence against women in disasters: A study of domestic violence programs in the United States and Canada. Violence Against Women 1999, 5, 742–768. [Google Scholar] [CrossRef]
- Nguyen, H.T. Gendered Vulnerabilities in Times of Natural Disasters: Male-to-Female Violence in the Philippines in the Aftermath of Super Typhoon Haiyan. Violence Against Women 2018, 25, 421–440. [Google Scholar] [CrossRef]
- Massetti, G.M.; Townsend, J.S.; Thomas, C.C.; Basile, K.C.; Richardson, L.C. Healthcare Access and Cancer Screening Among Victims of Intimate Partner Violence. J. Women’s Health 2018, 27, 607–614. [Google Scholar] [CrossRef]
- Gearhart, S.; Perez-Patron, M.; Hammond, T.A.; Goldberg, D.W.; Klein, A.; Horney, J.A. The Impact of Natural Disasters on Domestic Violence: An Analysis of Reports of Simple Assault in Florida (1999–2007). Violence Gend. 2018, 5, 87–92. [Google Scholar] [CrossRef]
- Lira, M.C.; Xuan, Z.; Coleman, S.M.; Swahn, M.H.; Heeren, T.C.; Naimi, T.S. Alcohol Policies and Alcohol Involvement in Intimate Partner Homicide in the U.S. Am. J. Prev. Med. 2019, 57, 172–179. [Google Scholar] [CrossRef]
- Centre of Excellence for Women’s Health. COVID-19, Intimate Partner Violence and Substance Use-Connections and Implications; Centre of Excellence for Women’s Health: Vancouver, BC, Canada, 2021. [Google Scholar]
- Centre of Excellence for Women’s Health. Action on Intimate Partner Violence and Substance Use in the COVID-19 Context; Centre of Excellence for Women’s Health: Vancouver, BC, Canada, 2021. [Google Scholar]
- Centre of Excellence for Women’s Health. Linking Practices on Intimate Partner Violence and Substance Use during COVID-19; Centre of Excellence for Women’s Health: Vancouver, BC, Canada, 2021. [Google Scholar]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brabete, A.C.; Wolfson, L.; Stinson, J.; Poole, N.; Allen, S.; Greaves, L. Exploring the Linkages between Substance Use, Natural Disasters, Pandemics, and Intimate Partner Violence against Women: A Rapid Review in the Context of COVID-19. Sexes 2021, 2, 509-522. https://doi.org/10.3390/sexes2040040
Brabete AC, Wolfson L, Stinson J, Poole N, Allen S, Greaves L. Exploring the Linkages between Substance Use, Natural Disasters, Pandemics, and Intimate Partner Violence against Women: A Rapid Review in the Context of COVID-19. Sexes. 2021; 2(4):509-522. https://doi.org/10.3390/sexes2040040
Chicago/Turabian StyleBrabete, Andreea C., Lindsay Wolfson, Julie Stinson, Nancy Poole, Sarah Allen, and Lorraine Greaves. 2021. "Exploring the Linkages between Substance Use, Natural Disasters, Pandemics, and Intimate Partner Violence against Women: A Rapid Review in the Context of COVID-19" Sexes 2, no. 4: 509-522. https://doi.org/10.3390/sexes2040040
APA StyleBrabete, A. C., Wolfson, L., Stinson, J., Poole, N., Allen, S., & Greaves, L. (2021). Exploring the Linkages between Substance Use, Natural Disasters, Pandemics, and Intimate Partner Violence against Women: A Rapid Review in the Context of COVID-19. Sexes, 2(4), 509-522. https://doi.org/10.3390/sexes2040040