
Performance Comparison of a Duplex Implementation of the CDC EUA 2019-nCoV Assay with the Seegene Allplex-SARS-CoV-2 Assay for the Detection of SARS-CoV-2 in Nasopharyngeal Swab Samples

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Processing
2.2. Amplification Design
2.3. Test Performance Evaluation
2.3.1. Determination of the Analytical Limit of Detection (LoD) of the Test
2.3.2. Verification of the Cross-Reactivity of the Test
2.4. Evaluation of the Clinical Performance of the Test
3. Results
3.1. Demographic Characteristics
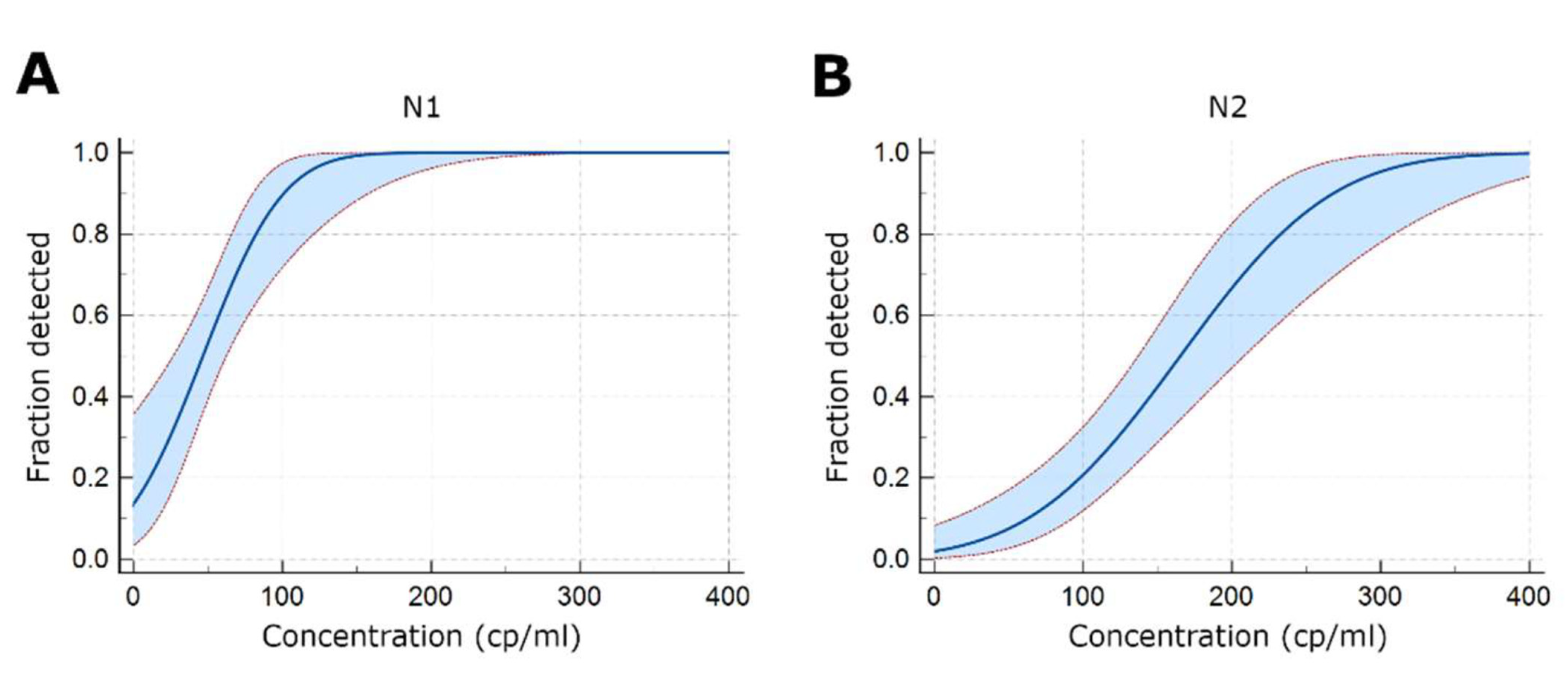
3.2. Determination of the Analytical Limit of Detection (LoD) of the Test
3.3. Determination of the Potential Cross-Reactivity of the Test
3.4. Evaluation of the Clinical Performance of the Test
3.5. Evaluation of Different SARS-CoV-2 Variants
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Harapan, H.; Itoh, N.; Yufika, A.; Winardi, W.; Keam, S.; Te, H.; Megawati, D.; Hayati, Z.; Wagner, A.L.; Mudatsir, M. Coronavirus disease 2019 (COVID-19): A literature review. J. Infect. Public Health 2020, 13, 667–673. [Google Scholar] [CrossRef] [PubMed]
- Lu, X.; Wang, L.; Sakthivel, S.K.; Whitaker, B.; Murray, J.; Kamili, S.; Lynch, B.; Malapati, L.; Burke, S.A.; Harcourt, J.; et al. US CDC Real-Time Reverse Transcription PCR Panel for Detection of Severe Acute Respiratory Syndrome Coronavirus 2. Emerg. Infect. Dis. 2020, 26, 1654–1665. [Google Scholar] [CrossRef] [PubMed]
- Mögling, R.; Meijer, A.; Berginc, N.; Bruisten, S.; Charrel, R.; Coutard, B.; Eckerle, I.; Enouf, V.; Hungnes, O.; Korukluoglu, G.; et al. Delayed Laboratory Response to COVID-19 Caused by Molecular Diagnostic Contamination. Emerg. Infect. Dis. 2020, 26, 1944–1946. [Google Scholar] [CrossRef] [PubMed]
- Huggett, J.F.; Benes, V.; Bustin, S.A.; Garson, J.A.; Harris, K.; Kammel, M.; Kubista, M.; McHugh, T.D.; Moran-Gilad, J.; Nolan, T.; et al. Cautionary Note on Contamination of Reagents Used for Molecular Detection of SARS-CoV-2. Clin. Chem. 2020, 66, 1369–1372. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. The United States badly bungled coronavirus testing—but things may soon improve. Science 2020. [Google Scholar] [CrossRef]
- Why the CDC Botched Its Coronavirus Testing|MIT Technology Review. Available online: https://www.technologyreview.com/2020/03/05/905484/why-the-cdc-botched-its-coronavirus-testing/ (accessed on 24 January 2022).
- Vogels, C.B.F.; Brito, A.F.; Wyllie, A.L.; Fauver, J.R.; Ott, I.M.; Kalinich, C.C.; Petrone, M.E.; Casanovas-Massana, A.; Catherine Muenker, M.; Moore, A.J.; et al. Analytical sensitivity and efficiency comparisons of SARS-CoV-2 RT–qPCR primer–probe sets. Nat. Microbiol. 2020, 5, 1299–1305. [Google Scholar] [CrossRef] [PubMed]
- Nalla, A.K.; Casto, A.M.; Casto, A.M.; Huang, M.L.W.; Perchetti, G.A.; Sampoleo, R.; Shrestha, L.; Wei, Y.; Zhu, H.; Jerome, K.R.; et al. Comparative performance of SARS-CoV-2 detection assays using seven different primer-probe sets and one assay kit. J. Clin. Microbiol. 2020, 58, e00557-20. [Google Scholar] [CrossRef] [PubMed]
- Perchetti, G.A.; Nalla, A.K.; Huang, M.L.; Jerome, K.R.; Greninger, A.L. Multiplexing primer/probe sets for detection of SARS-CoV-2 by qRT-PCR. J. Clin. Virol. 2020, 129, 104499. [Google Scholar] [CrossRef] [PubMed]
- Lima, A.; Healer, V.; Vendrone, E.; Silbert, S. Validation of a modified CDC assay and performance comparison with the NeuMoDxTM and DiaSorin® automated assays for rapid detection of SARS-CoV-2 in respiratory specimens. J. Clin. Virol. 2020, 133, 104688. [Google Scholar] [CrossRef] [PubMed]
- Vogels, C.B.F.; Watkins, A.E.; Harden, C.A.; Brackney, D.; Shafer, J.; Wang, J.; Caraballo, C.; Kalinich, C.C.; Ott, I.; Fauver, J.R.; et al. SalivaDirect: Simple and sensitive molecular diagnostic test for SARS-CoV-2 surveillance. MedRxiv 2020. [Google Scholar] [CrossRef]
- Lineamientos para la Gestión de Muestras Durante la Pandemia del SARS-CoV-2 (COVID-19) en Colombia. Available online: psps02-lineamientos-gmuestras-pandemia-sars-cov-2-col.pdf (accessed on 20 March 2021).
- Dir Redes en Salud Publica, D.V. y A. del R. Protocolo de Verificación (Validación Secundaria) para Pruebas Moleculares de PCR en Tiempo Real (RT-qPCR) para la Detección del SARS-CoV-2. Inst. Nac. Salud. 1–8. Available online: http://www.saludcapital.gov.co/CTDLab/Publicaciones/2021/Protocolo_verifi_RT_PCR_SARS_CoV-2.pdf (accessed on 15 July 2021).
- INSTRUCTION MANUAL Luna ® Universal Probe One-Step RT-qPCR Kit NEB #E3006S/L/X/E 200/500/1,000/2,500 Reactions. Available online: https://international.neb.com/-/media/nebus/files/manuals/manuale3006.pdf?rev=389c4c496bba40a2ad7e0171c37c8658&hash=B1948A5B6DDC71B2ED2DAACD2FBF93F2 (accessed on 15 February 2021).
- Burki, T. COVID-19 in Latin America. Lancet Infect. Dis. 2020, 20, 547–548. [Google Scholar] [CrossRef]
- AVISO DE LA OMS PARA LOS USUARIOS DE PRODUCTOS DE DIAGNÓSTICO IN VITRO. Available online: https://www.who.int/es/news/item/20-01-2021-who-information-notice-for-ivd-users-2020-05 (accessed on 24 January 2022).
- ALERTA SANITARIA Dirección de Dispositivos Médicos y Otras Tecnologías Invima Alerta Fuente de la Alerta: Organización Mundial de la Salud. Available online: https://app.invima.gov.co/alertas/ckfinder/userfiles/files/ALERTAS%20SANITARIAS/Dispositivos_Medicos/2020/Diciembre/Alerta%20No_%20%23194-2020%20-%20%20.pdf (accessed on 19 December 2020).



{kind=link}
{kind=link}
| Assay | Primer/Probe Name | Sequence 5′→3′ |
|---|---|---|
| 1 | 2019-nCov_N1 Forward | GACCCCAAAATCAGCGAAAT |
| 2019-nCov_N1 Reverse | TCTGGTTACTGCCAGTTGAATCTG | |
| 2019-nCov_N1 probe | FAM-ACCCCGCATTACGTTTGGTGGACC-BHQ1 | |
| Human Rnase P Forward | AGATTTGGACCTGCGAGCG | |
| Human Rnase P Reverse | GAGCGGCTGTCTCCACAAGT | |
| Human Rnase P Probe | Quasar 670-TTCTGACCTGAAGGCTCTGCGCG-BHQ2 | |
| 2 | 2019-nCov_N2 Forward | TTACAAACATTGGCCGCAAA |
| 2019-nCov_N2 Reverse | GCGCGACATTCCGAAGAA | |
| 2019-nCov_N2 probe | FAM-ACAATTTGCCCCCAGCGCTTCAG-BHQ1 |
| Variable | N (%) | Mean Age (S.D.) |
|---|---|---|
| Positive cases | ||
| Gender | ||
| Female | 74 (50.7) | |
| Male | 72 (49.3) | |
| Age | ||
| <18 years | 5 (3.4) | 3 years (±5 years) |
| 18–60 years | 92 (63.0) | 37 years (±12 years) |
| >60 years | 49 (33.6) | 74 years (±10 years) |
| Clinical presentation | ||
| Symptomatic | 133 (91.1) | |
| Asymptomatic | 13 (8.9) | |
| Total cases | 146 | |
| Negative cases | ||
| Gender | ||
| Female | 43 (58.1) | |
| Male | 31 (41.9) | |
| Age | ||
| <18 years | 14 (18.9) | 5 years (±4 years) |
| 18–60 years | 43 (58.1) | 28 years (±9 years) |
| >60 years | 17 (23.0) | 75 years (±10 years) |
| Clinical presentation | ||
| Symptomatic | 54 (73) | |
| Asymptomatic | 20 (27) | |
| Total cases | 74 |
| Sample | Respiratory Pathogen | Multiplex PCR Result | SARS-CoV-2 RT-PCR Result | ||
|---|---|---|---|---|---|
| N1 | RP (Ct) | N2 | |||
| 1 | RSV | Pos | Neg | Pos (27.30) | Neg |
| 2 | RHINO/ENTE | Pos | Neg | Pos (24.84) | Neg |
| 3 | 229E | Pos | Neg | Pos (36.75) | Neg |
| 4 | RSV | Pos | Neg | Pos (25.17) | Neg |
| 5 | RHINO/ENTE | Pos | Neg | Pos (21.33) | Neg |
| 6 | HKU1 | Pos | Neg | Pos (30.12) | Neg |
| 7 | RSV | Pos | Neg | Pos (27.36) | Neg |
| 8 | ADV | Pos | Neg | Pos (26.54) | Neg |
| Parameter | Result | 95% CI |
|---|---|---|
| Sensitivity (%) | 100 | 97.50–100 |
| Specificity (%) | 100 | 95.14–100 |
| False positive rate | 0 | |
| False negative rate | 0 | |
| PPV (%) | 100 | 97.50–100 |
| NPV (%) | 100 | 95.14–100 |
| Kappa Index | 1 | 0.98–1.00 |
| Sample | Allplex-SARS-CoV-2 Assay | Modified CDC Test | |||||
|---|---|---|---|---|---|---|---|
| Target | Target | ||||||
| E | RdRP/S | N | Result | N1 | N2 | Result | |
| 1 | 36.12 | 37.13 | 38.54 | Positive | 39.07 | 39.49 | Positive * |
| 2 | NA | 38.72 | NA | Positive | 37.76 | NA | Positive * |
| 3 | 37.49 | 39.21 | 35.64 | Positive | 36.45 | 39.02 | Positive * |
| 4 | 36.17 | 37.65 | 39.42 | Positive | 37.33 | 39.03 | Positive * |
| 5 | 38.59 | 38.88 | 37.57 | Positive | 37.15 | 39.31 | Positive * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiménez, K.M.; Fonseca-Mendoza, D.J.; Morel, A.; Ortega-Recalde, O.; Contreras Bravo, N.C.; Velandia-Piedrahita, C.A.; Steevens, A.; Caldas, L.D.; Ribón, J.P.; Sánchez, M.; et al. Performance Comparison of a Duplex Implementation of the CDC EUA 2019-nCoV Assay with the Seegene Allplex-SARS-CoV-2 Assay for the Detection of SARS-CoV-2 in Nasopharyngeal Swab Samples. Methods Protoc. 2022, 5, 73. https://doi.org/10.3390/mps5050073
Jiménez KM, Fonseca-Mendoza DJ, Morel A, Ortega-Recalde O, Contreras Bravo NC, Velandia-Piedrahita CA, Steevens A, Caldas LD, Ribón JP, Sánchez M, et al. Performance Comparison of a Duplex Implementation of the CDC EUA 2019-nCoV Assay with the Seegene Allplex-SARS-CoV-2 Assay for the Detection of SARS-CoV-2 in Nasopharyngeal Swab Samples. Methods and Protocols. 2022; 5(5):73. https://doi.org/10.3390/mps5050073
Chicago/Turabian StyleJiménez, Karen Marcela, Dora Janeth Fonseca-Mendoza, Adrien Morel, Oscar Ortega-Recalde, Nora Constanza Contreras Bravo, Camilo Andres Velandia-Piedrahita, Adriana Steevens, Luisa Daniela Caldas, Juan Pablo Ribón, Martha Sánchez, and et al. 2022. "Performance Comparison of a Duplex Implementation of the CDC EUA 2019-nCoV Assay with the Seegene Allplex-SARS-CoV-2 Assay for the Detection of SARS-CoV-2 in Nasopharyngeal Swab Samples" Methods and Protocols 5, no. 5: 73. https://doi.org/10.3390/mps5050073
APA StyleJiménez, K. M., Fonseca-Mendoza, D. J., Morel, A., Ortega-Recalde, O., Contreras Bravo, N. C., Velandia-Piedrahita, C. A., Steevens, A., Caldas, L. D., Ribón, J. P., Sánchez, M., Restrepo, C. M., & Cabrera, R. (2022). Performance Comparison of a Duplex Implementation of the CDC EUA 2019-nCoV Assay with the Seegene Allplex-SARS-CoV-2 Assay for the Detection of SARS-CoV-2 in Nasopharyngeal Swab Samples. Methods and Protocols, 5(5), 73. https://doi.org/10.3390/mps5050073