
Touch Imprint Intraoperative Flow Cytometry as a Complementary Tool for Detailed Assessment of Resection Margins and Tumor Biology in Liver Surgery for Primary and Metastatic Liver Neoplasms

 ,
, 
 ,
,  and
and
Abstract
:1. Introduction
2. Experimental Design
2.1. Materials
- Wipak Pouch Sterilization Steriking 11.75 In X 17.75 (Serfinity Medical Cat.No. SSU SS7);
- A total of 10 cc syringes for FNAs;
- Sterile single-pack CellTrics® filters (Sysmex, Cat.no. 04-004-2323);
- BD Pharmingen™ DNA stain buffer: 1X PBS, 2% FBS, 0.1% NaN3 (pH 7.1–7.4) (BD Biosciences, Cat.no. 554656);
- BD Pharmingen™ PI/RNase A staining buffer: 125 mM propidium iodine in DNA stain buffer (BD Biosciences, Cat.no.550825);
- Ficoll-Paque PREMIUM separation (GE Healthcare, Little Chalfont, Buckinghamshire, UK Cat.no. 95038-170);
- DNA QC particles (BD Biosciences Cat.no.349523).
2.2. Equipment
- BD FACSCaliBur Flow Cytometer (BD Biosciences)
3. Experimental Procedure
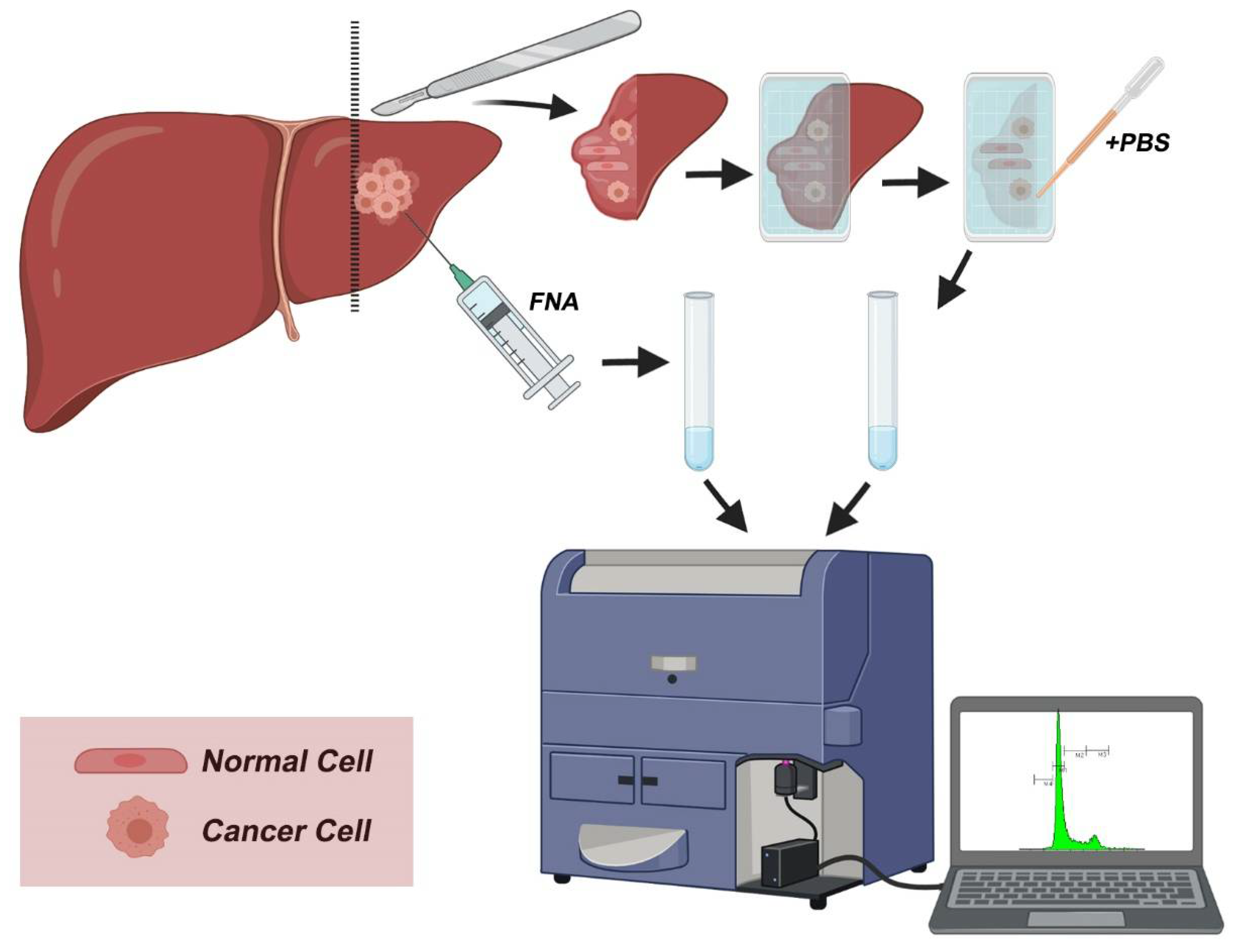
3.1. Preparing Cell Suspensions from Touch Imprints and Fine-Needle Aspirates for DNA Content
- Creating cell suspension from touch imprints
- 2.
- Creating cell suspension from fine-needle aspirates (FNAs)
- 3.
- Rake cell suspension for 10 s and pass through a sterilized filter.
 CRITICAL STEP The cell suspension should be minced thoroughly to obtain single cells but also gently to avoid disruption of cellular and nuclear membranes.
CRITICAL STEP The cell suspension should be minced thoroughly to obtain single cells but also gently to avoid disruption of cellular and nuclear membranes.- 4.
- Process the cell pellet immediately by adding DNA staining solution to obtain a final Propidium iodide concentration of 125 mM. Incubate for 3 min.
- 5.
- Proceed immediately to DNA content analysis.
3.2. Flow Cytometric DNA Content Analysis
- Evaluate instrument’s performance using DNA QC particles (BD Biosciences), using the manufacturer’s instructions.
 CRITICAL STEP. The instrument’s performance is based on the correct alignment of the cytometer. This step should not be omitted before every experiment.
CRITICAL STEP. The instrument’s performance is based on the correct alignment of the cytometer. This step should not be omitted before every experiment.- Prepare the internal control. Use ficoll-separated normal peripheral blood mononuclear cells (PBMCs). Stain 200 μL of ficoll-separated PBMCs for 3 min with PI/RNase A staining solution (125 mM of PI).
- 1.
- Use PBMC standard before every experiment, using freshly prepared ficoll-separated PBMCs, and determine their DNA content.
 CRITICAL STEP. A single peak is of non-dividing cells with normal diploid DNA (G0/G1 peak) is mostly visible. The normal G0/G1 peak should be accurately defined since the geo-mean of G0/G1 peak of PBMCs is the internal control for calculating both tumor and DNA index.
CRITICAL STEP. A single peak is of non-dividing cells with normal diploid DNA (G0/G1 peak) is mostly visible. The normal G0/G1 peak should be accurately defined since the geo-mean of G0/G1 peak of PBMCs is the internal control for calculating both tumor and DNA index.- 2.
- Process DNA content analysis in a flow cytometer with 488 nm excitation and 617 nm (or compatible) emission channel. Process 5000 cells. Repeat for FNA and individual touch imprints from individual patients.
- 3.
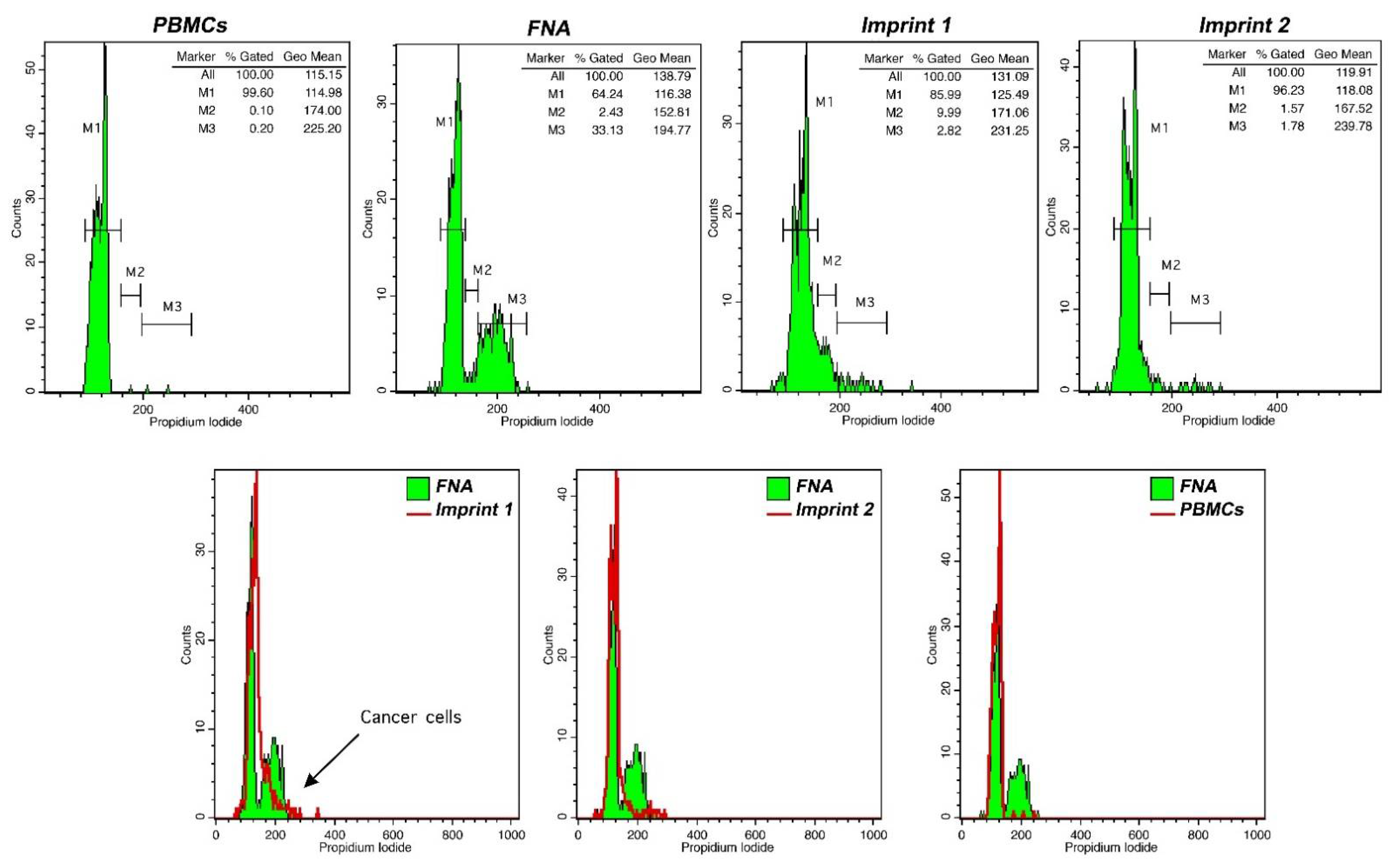
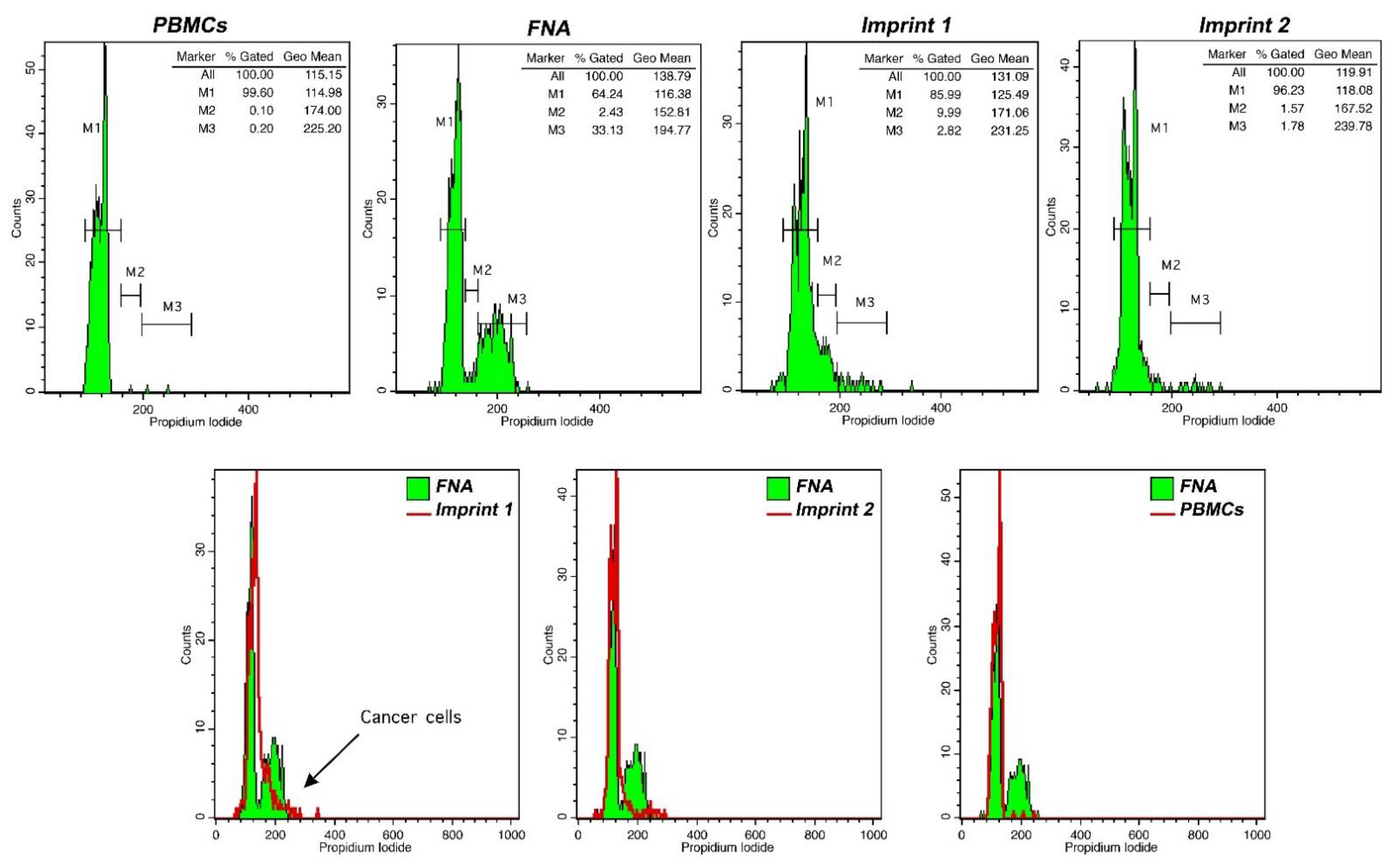
- Using flow cytometry analysis software, determine the G0/G1 geo-mean, based on PBMC fluorescence peak. Define respective areas corresponding to proliferating cells (S phase and G2/M cell cycle phases) and/or cells with altered DNA content. A typical flow cytometry analysis of FNA and touch imprint samples is presented in Figure 3.
3.3. Calculation of DNA Index and Tumor Index
- Calculate DNA index and tumor index in FNA-obtained sample as follows:
 CRITICAL STEP: The aforementioned calculations are critical for the characterization of cancer cells in FNA samples. In the next step, the detection of cancer cells in touch imprints is based on PBMC peak analysis and the calculations made in the FNA sample.
CRITICAL STEP: The aforementioned calculations are critical for the characterization of cancer cells in FNA samples. In the next step, the detection of cancer cells in touch imprints is based on PBMC peak analysis and the calculations made in the FNA sample.- 2.
- Perform DNA index and tumor index calculations for individual FNA samples. The presence of cancer cells in imprint samples is based on the characterization made for the respective FNA sample.
4. Results and Discussion
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Anastasopoulos, N.-A.T.; Lianos, G.D.; Tatsi, V.; Karampa, A.; Goussia, A.; Glantzounis, G.K. Clinical heterogeneity in patients with non-alcoholic fatty liver disease-associated hepatocellular carcinoma. Expert Rev. Gastroenterol. Hepatol. 2020, 14, 1025–1033. [Google Scholar] [CrossRef]
- Glantzounis, G.K.; Karampa, A.; Peristeri, D.; Pappas-Gogos, G.; Tepelenis, K.; Tzimas, P.; Cyrochristos, D. Recent advances in the surgical management of hepatocellular carcinoma. Ann. Gastroenterol. 2021, 34, 1–13. [Google Scholar] [CrossRef]
- Glantzounis, G.; Paliouras, A.; Stylianidi, M.-C.; Milionis, H.; Tzimas, P.; Roukos, D.; Pentheroudakis, G.; Felekouras, E. The role of liver resection in the management of intermediate and advanced stage hepatocellular carcinoma. A systematic review. Eur. J. Surg. Oncol. 2018, 44, 195–208. [Google Scholar] [CrossRef] [PubMed]
- Kyrochristos, I.D.; Ziogas, D.E.; Goussia, A.; Glantzounis, G.K.; Roukos, D.H. Bulk and single-cell next-generation sequencing: Individualizing treatment for colorectal cancer. Cancers 2019, 11, 1809. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ethun, C.G.; Kooby, D.A. The importance of surgical margins in pancreatic cancer. J. Surg. Oncol. 2016, 113, 283–288. [Google Scholar] [CrossRef]
- Schlageter, M.; Terracciano, L.M.; D’Angelo, S.; Sorrentino, P. Histopathology of hepatocellular carcinoma. World J. Gastroenterol. WJG 2014, 20, 15955. [Google Scholar] [CrossRef]
- Rastogi, A. Changing role of histopathology in the diagnosis and management of hepatocellular carcinoma. World J. Gastroenterol. 2018, 24, 4000. [Google Scholar] [CrossRef]
- Shapiro, H.M. Practical Flow Cytometry; John Wiley & Sons: Hoboken, NJ, USA, 2005. [Google Scholar]
- Horan, P.K.; Wheeless, L.L. Quantitative single cell analysis and sorting. Science 1977, 198, 149–157. [Google Scholar] [CrossRef]
- Vartholomatos, E.; Vartholomatos, G.; Alexiou, G.A.; Markopoulos, G.S. The Past, Present and Future of Flow Cytometry in Central Nervous System Malignancies. Methods Protoc. 2021, 4, 11. [Google Scholar] [CrossRef]
- Alexiou, G.A.; Vartholomatos, G.; Goussia, A.; Batistatou, A.; Tsamis, K.; Voulgaris, S.; Kyritsis, A.P. Fast cell cycle analysis for intraoperative characterization of brain tumor margins and malignancy. J. Clin. Neurosci. 2015, 22, 129–132. [Google Scholar] [CrossRef]
- Saito, T.; Muragaki, Y.; Shioyama, T.; Komori, T.; Maruyama, T.; Nitta, M.; Yasuda, T.; Hosono, J.; Okamoto, S.; Kawamata, T. Malignancy index using intraoperative flow cytometry is a valuable prognostic factor for glioblastoma treated with radiotherapy and concomitant temozolomide. Neurosurgery 2019, 84, 662–672. [Google Scholar] [CrossRef] [PubMed]
- Vartholomatos, G.; Alexiou, G.A.; Lianos, G.D.; Harissis, H.; Voulgaris, S.; Kyritsis, A.P. Intraoperative cell cycle analysis for tumor margins evaluation: The future is now? Int. J. Surg. 2018, 53, 380–381. [Google Scholar] [CrossRef] [PubMed]
- Vartholomatos, G.; Basiari, L.; Kastanioudakis, I.; Psichogios, G.; Alexiou, G.A. The Role of Intraoperative Flow Cytometry in Surgical Margins of Head and Neck Malignancies. Ear Nose Throat J. 2020, 10, 145561320931989. [Google Scholar] [CrossRef]
- Vartholomatos, G.; Basiari, L.; Exarchakos, G.; Kastanioudakis, I.; Komnos, I.; Michali, M.; Markopoulos, G.S.; Batistatou, A.; Papoudou-Bai, A.; Alexiou, G.A. Intraoperative flow cytometry for head and neck lesions. Assessment of malignancy and tumour-free resection margins. Oral Oncol. 2019, 99, 104344. [Google Scholar] [CrossRef]
- Andreou, M.; Vartholomatos, E.; Harissis, H.; Markopoulos, G.S.; Alexiou, G.A. Past, Present and Future of Flow Cytometry in Breast Cancer—A Systematic Review. EJIFCC 2019, 30, 423–437. [Google Scholar]
- Vartholomatos, G.; Stefanaki, K.; Alexiou, G.A.; Batistatou, A.; Markopoulos, G.S.; Tzoufi, M.; Sfakianos, G.; Prodromou, N. Pediatric brain tumor grading based on CD56 quantification. J. Pediatr. Neurosci. 2018, 13, 524. [Google Scholar]
- Alexiou, G.A.; Vartholomatos, G.; Stefanaki, K.; Markopoulos, G.S.; Kyritsis, A.P. Intraoperative Flow Cytometry for Diagnosis of Central Nervous System Lesions. J. Cytol. 2019, 36, 134–135. [Google Scholar] [CrossRef] [PubMed]
- Valdes, E.K.; Boolbol, S.K.; Cohen, J.M.; Feldman, S.M. Intra-operative touch preparation cytology; does it have a role in re-excision lumpectomy? Ann. Surg. Oncol. 2007, 14, 1045–1050. [Google Scholar] [CrossRef]
- Hashmi, A.A.; Naz, S.; Ahmed, O.; Yaqeen, S.R.; Afzal, A.; Asghar, I.A.; Irfan, M.; Faridi, N. Diagnostic Accuracy of Intraoperative Touch Imprint Cytology for the Diagnosis of Axillary Sentinel Lymph Node Metastasis of Breast Cancer: Comparison With Intraoperative Frozen Section Evaluation. Cureus 2021, 13, e12960. [Google Scholar] [CrossRef]
- Turoldo, A.; Pascuali, A.; Bortul, M.; Silvestri, M.; Dobrinja, C.; Zanconati, F.; di Meo, N.; Zalaudek, I.; De Manzini, N. Touch Imprinting Cytology may be useful in the intraoperative evaluation of the sentinel lymph node in melanoma. Ann. Ital. Chir. 2019, 90, 491–496. [Google Scholar] [PubMed]
- Huang, S.C.; Liang, J.D.; Hsu, S.J.; Hong, T.C.; Yang, H.C.; Kao, J.H. Direct Comparison of Biopsy Techniques for Hepatic Malignancies. Clin. Mol. Hepatol. 2020, 27, 305–312. [Google Scholar] [CrossRef]
- Baltagiannis, E.G.; Kyrochristos, I.D.; Ziogas, D.E.; Goussia, A.; Mitsis, M.; Roukos, D.H. From personalized to precision cancer medicine. Per. Med. 2020, 17, 245–250. [Google Scholar] [CrossRef] [PubMed]
- Baltagiannis, E.G.; Ziogas, D.E.; Cho, W.C.; Mitsis, M.; Roukos, D.H. Tumor heterogeneity-driven individualized therapy. Future Med. 2021, 17. [Google Scholar] [CrossRef]
- Thomas, R.M.; Berman, J.J.; Yetter, R.A.; William Moore, G.; Hutchins, G.M. Liver cell dysplasia: A DNA aneuploid lesion with distinct morphologic features. Hum. Pathol. 1992, 23, 496–503. [Google Scholar] [CrossRef]
- Roncalli, M.; Borzio, M.; Brando, B.; Colloredo, G.; Servida, E. Abnormal DNA content in liver-cell dysplasia: A flow cytometric study. Int. J. Cancer 1989, 44, 204–207. [Google Scholar] [CrossRef]
- Fidler, I.J. The pathogenesis of cancer metastasis: The’seed and soil’hypothesis revisited. Nat. Rev. Cancer 2003, 3, 453–458. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| # | DNA Index | Tumor Index | TI-IFC 1 | Pathologic Diagnosis 2,3 | Microscopic Evaluation 4 |
|---|---|---|---|---|---|
| 1 | 1 | 15 | + | HCC, Grade 2 | U (<1 mm) |
| 2 | 1 | 10 | − | HCC, Grade 2 | U (>10 mm) |
| 3 | 1,5 | 20 | + | CRC *, Grade 2 | U (7 mm) |
| 4 | 1 | 13 | − | CRC *, Grade 2 | U (5 mm) |
| 5 | 1,6 | 12 | + | CRC *, Grade 2 | U (4 mm) |
| 6 | 1 | 13 | − | CRC *, Grade 2 | U (>10 mm) |
| 7 | 1,9 | 4 | − | GEA *, Grade 2 | U (4 mm) |
| 8 | 1 | 7 | − | CRC *, Grade 3 | U (>10 mm) |
| 9 | 1 | 25 | − | HCC, Grade 2 | U (>10 mm) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Markopoulos, G.S.; Glantzounis, G.K.; Goussia, A.C.; Lianos, G.D.; Karampa, A.; Alexiou, G.A.; Vartholomatos, G. Touch Imprint Intraoperative Flow Cytometry as a Complementary Tool for Detailed Assessment of Resection Margins and Tumor Biology in Liver Surgery for Primary and Metastatic Liver Neoplasms. Methods Protoc. 2021, 4, 66. https://doi.org/10.3390/mps4030066
Markopoulos GS, Glantzounis GK, Goussia AC, Lianos GD, Karampa A, Alexiou GA, Vartholomatos G. Touch Imprint Intraoperative Flow Cytometry as a Complementary Tool for Detailed Assessment of Resection Margins and Tumor Biology in Liver Surgery for Primary and Metastatic Liver Neoplasms. Methods and Protocols. 2021; 4(3):66. https://doi.org/10.3390/mps4030066
Chicago/Turabian StyleMarkopoulos, Georgios S., Georgios K. Glantzounis, Anna C. Goussia, Georgios D. Lianos, Anastasia Karampa, George A. Alexiou, and George Vartholomatos. 2021. "Touch Imprint Intraoperative Flow Cytometry as a Complementary Tool for Detailed Assessment of Resection Margins and Tumor Biology in Liver Surgery for Primary and Metastatic Liver Neoplasms" Methods and Protocols 4, no. 3: 66. https://doi.org/10.3390/mps4030066
APA StyleMarkopoulos, G. S., Glantzounis, G. K., Goussia, A. C., Lianos, G. D., Karampa, A., Alexiou, G. A., & Vartholomatos, G. (2021). Touch Imprint Intraoperative Flow Cytometry as a Complementary Tool for Detailed Assessment of Resection Margins and Tumor Biology in Liver Surgery for Primary and Metastatic Liver Neoplasms. Methods and Protocols, 4(3), 66. https://doi.org/10.3390/mps4030066