
Is Our Newborn Screening Working Well? A Literature Review of Quality Requirements for Newborn Blood Spot Screening (NBS) Infrastructure and Procedures


Abstract
1. Introduction

{kind=link}
{kind=link}
| Metabolic Disorders: phenylketonuria (PKU) and hyperphenylalaninemia (HPA), maple syrup urine disease (MSUD), biotinidase deficiency, galactosemia, medium-chain acyl-CoA dehydrogenase deficiency (MCADD), long-chain 3-hydroxyacyl-CoA dehydrogenase deficiency (LCHADD), very-long-chain acyl-CoA dehydrogenase deficiency (VLCADD), carnitine cycle defects, glutaric acidemia type 1 (GA 1), isovaleric acidemia (IVA), and tyrosinemia type 1 Endocrine Disorders: congenital hypothyroidism (CH) and congenital adrenal hyperplasia (CAH) Hemoglobin and Immunodeficiency Disorders: sickle cell disease (SCD) and severe combined immunodeficiency (SCID) Neuromuscular Disorder: spinal muscular atrophy (SMA) Cystic Fibrosis (CF) |
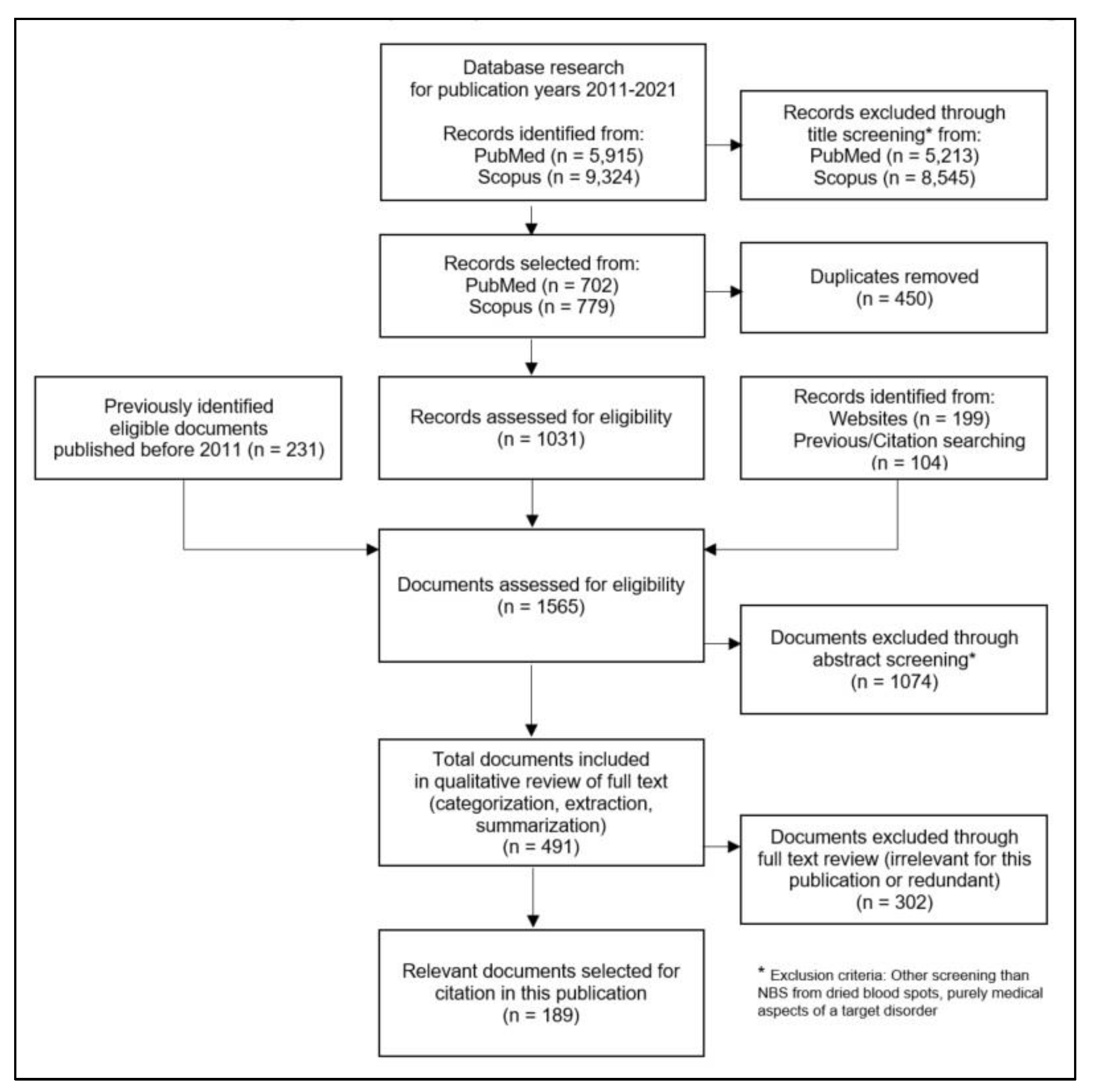
2. Materials and Methods
3. Results
3.1. Basic Principles
3.2. NBS Components
3.2.1. Parental Education about NBS and Informed Consent
3.2.2. Structure and Quality Assurance in the Screening Laboratory
3.2.3. Informing Parents about Abnormal (Positive) NBS Results
3.2.4. Confirmatory Diagnostics
3.2.5. Completeness of NBS Coverage
3.2.6. Follow-Up (Tracking) of Positive Results and Requested Repeat Screening Tests
3.2.7. Documentation and Evaluation of NBS
3.3. NBS Programme Governance and Quality Management
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hoffmann, G.F.; Lindner, M.; Loeber, J.G. 50 years of newborn screening. J. Inherit. Metab. Dis. 2014, 37, 163–164. [Google Scholar] [CrossRef] [PubMed]
- Jansen, M.E.; Lister, K.J.; van Kranen, H.J.; Cornel, M.C. Policy Making in Newborn Screening Needs a Structured and Transparent Approach. Front. Public Health 2017, 5, 53. [Google Scholar] [CrossRef] [PubMed]
- Bonham, J. NBS Is Pandora’s Box; New Techniques Make Anything Possible. Abstract. Int. J. Neonatal Screen. 2018, 4, 28. [Google Scholar] [CrossRef]
- Gramer, G.; Nennstiel-Ratzel, U.; Hoffmann, G.F. 50 Jahre Neugeborenenscreening in Deutschland. [50 years of newborn screening in Germany]. Monatsschr. Kinderheilkd. 2018, 166, 987–993. [Google Scholar] [CrossRef]
- González-Irazabal, Y.; Hernandez de Abajo, G.; Martínez-Morillo, E. Identifying and overcoming barriers to harmonize newborn screening programs through consensus strategies. Crit. Rev. Clin. Lab. Sci. 2021, 58, 29–48. [Google Scholar] [CrossRef]
- Dikow, N.; Ditzen, B.; Kölker, S.; Hoffmann, G.F.; Schaaf, C.P. From newborn screening to genomic medicine: Challenges and suggestions on how to incorporate genomic newborn screening in public health programs. Medgen 2022, 34, 13–20. [Google Scholar] [CrossRef]
- McCabe, E.R.B. Newborn screening: A complex system that requires a culture of safety. Mol. Genet. Metab. 2014, 113, 6–7. [Google Scholar] [CrossRef]
- Therrell, B.L.; Padilla, C.D.; Loeber, J.G.; Kneisser, I.; Saadallah, A.; Borrajo, G.J.C.; Adams, J. Current status of newborn screening worldwide: 2015. Semin. Perinatol. 2015, 39, 171–187. [Google Scholar] [CrossRef] [PubMed]
- Howson, C.P.; Cedergren, B.; Giugliani, R.; Huhtinen, P.; Padilla, C.D.; Palubiak, C.S.; Santos, M.D.; Schwartz, I.V.D.; Therrell, B.L.; Umemoto, A.; et al. Universal newborn screening: A roadmap for action. Mol. Genet. Metab. 2018, 124, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Kemper, A.R.; Boyle, C.A.; Brosco, J.P.; Grosse, S.D. Ensuring the Life-Span Benefits of Newborn Screening. Pediatrics 2019, 144, e20190904. [Google Scholar] [CrossRef]
- Deutsche Gesellschaft für Neugeborenenscreening e.V. (DGNS). Nationaler Screeningreport Deutschland. 2019. Available online: https://www.screening-dgns.de/Pdf/Screeningreports/DGNS-Screeningreport-e_2019.pdf (accessed on 13 April 2022).
- Forman, J.; Coyle, F.; Levy-Fisch, J.; Roberts, P.; Terry, S.; Legge, M. Screening criteria: The need to deal with new developments and ethical issues in newborn metabolic screening. J. Community Genet. 2013, 4, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Gray, J.A.M.; Patnick, J.; Blanks, R.G. Maximising benefit and minimising harm of screening. BMJ 2008, 336, 480–483. [Google Scholar] [CrossRef]
- Wilcken, B. Expanded newborn screening: Reducing harm, assessing benefit. J. Inherit. Metab. Dis. 2010, 33, S205–S210. [Google Scholar] [CrossRef]
- Dans, L.F.; Silvestre, M.A.A.; Dans, A.L. Trade-off between benefit and harm is crucial in health screening recommendations. Part I: General principles. J. Clin. Epidemiol. 2011, 64, 231–239. [Google Scholar] [CrossRef] [PubMed]
- Nicholls, S.G.; Wilson, B.J.; Etchegary, H.; Brehaut, J.C.; Potter, B.K.; Hayeems, R.; Chakraborty, P.; Milburn, J.; Pullman, D.; Turner, L.; et al. Benefits and burdens of newborn screening: Public understanding and decision-making. Personalized Medicine 2014, 11, 593–607. [Google Scholar] [CrossRef] [PubMed]
- Wilcken, B.; Wiley, V. Fifty years of newborn screening. J. Paediatr. Child Health 2015, 51, 103–107. [Google Scholar] [CrossRef]
- Goldenberg, A.J.; Comeau, A.M.; Grosse, S.D.; Tanksley, S.; Prosser, L.A.; Ojodu, J.; Botkin, J.R.; Kemper, A.R.; Green, N.S. Evaluating Harms in the Assessment of Net Benefit: A Framework for Newborn Screening Condition Review. Matern. Child Health J. 2016, 20, 693–700. [Google Scholar] [CrossRef]
- Taylor-Phillips, S.; Stinton, C.; Di Ferrante Ruffano, L.; Seedat, F.; Clarke, A.; Deeks, J.J. Association between use of systematic reviews and national policy recommendations on screening newborn babies for rare diseases: Systematic review and meta-analysis. BMJ 2018, 361, k1612. [Google Scholar] [CrossRef]
- Goldenberg, A.J.; Lloyd-Puryear, M.; Brosco, J.P.; Therrell, B.; Bush, L.; Berry, S.; Brower, A.; Bonhomme, N.; Bowdish, B.; Chrysler, D.; et al. Including ELSI research questions in newborn screening pilot studies. Genet. Med. 2019, 21, 525–533. [Google Scholar] [CrossRef]
- WHO. Screening Programmes: A Short Guide: Increase Effectiveness, Maximize Benefits and Minimize Harm. Available online: https://apps.who.int/iris/bitstream/handle/10665/330829/9789289054782-eng.pdf (accessed on 12 November 2021).
- Andermann, A.; Blancquaert, I.; Beauchamp, S.; Déry, V. Revisiting Wilson and Jungner in the genomic age: A review of screening criteria over the past 40 years. Bull. World Health Organ. 2008, 86, 317–319. [Google Scholar] [CrossRef]
- Andermann, A.; Blancquaert, I.; Beauchamp, S.; Costea, I. Guiding policy decisions for genetic screening: Developing a systematic and transparent approach. Public Health Genom. 2011, 14, 9–16. [Google Scholar] [CrossRef]
- Bundesgesundheitsministerium. Gesetz über Genetische Untersuchungen bei Menschen (Gendiagnostikgesetz, GenDG). Available online: https://www.bundesgesundheitsministerium.de/service/begriffe-von-a-z/g/gendiagnostikgesetz.html (accessed on 9 February 2022).
- Gemeinsamer Bundesausschuss (G-BA). Richtlinie des Gemeinsamen Bundesausschusses über die Früherkennung von Krankheiten bei Kindern (Kinder-Richtlinie): Zuletzt Geändert am 16. September 2021, Veröffentlicht im Bundesanzeiger AT 03.11.2021 B4, in Kraft Getreten am. 1 January 2022. Available online: https://www.g-ba.de/richtlinien/15/ (accessed on 3 February 2022).
- Deutsche Gesellschaft für Neugeborenenscreening e.V. (DGNS). DGNS Screeningreports. Available online: https://www.screening-dgns.de/reports.php (accessed on 13 April 2022).
- Lüders, A.; Blankenstein, O.; Brockow, I.; Ensenauer, R.; Lindner, M.; Schulze, A.; Nennstiel, U. Neonatal Screening for Congenital Metabolic and Endocrine Disorders: Results From Germany for the Years 2006–2018. Dtsch. Arztebl. Int. 2021, 118, 101–108. [Google Scholar] [CrossRef]
- Zimmer, K.-P. Newborn Screening: Still Room for Improvement: Editorial. Dtsch. Arztebl. Int. 2021, 118, 99–100. [Google Scholar] [CrossRef] [PubMed]
- Wilson, J.; Jungner, G. Principles and Practice of Screening for Disease. WHO. 1968. Available online: https://apps.who.int/iris/handle/10665/37650 (accessed on 11 November 2021).
- Liebl, B.; Kries, R.v.; Nennstiel-Ratzel, U.; Muntau, A.C.; Röschinger, W.; Olgemöller, B.; Zapf, A.; Roscher, A.A. Ethisch-rechtliche Aspekte des Neugeborenenscreenings. Monatsschrift Kinderheilkunde 2001, 149, 1326–1335. [Google Scholar]
- Cornel, M.; Rigter, T.; Weinreich, S.; Burgard, P.; Hoffmann, G.F.; Lindner, M.; Loeber, J.G.; Rupp, K.; Taruscio, D.; Vittozzi, L. Newborn Screening in Europe: Expert Opinion Document. 2011. Available online: https://isns-neoscreening.org/wp-content/uploads/2018/11/Expert-opinion-document-on-NBS-FINAL.pdf (accessed on 15 October 2021).
- Cornel, M.C.; Rigter, T.; Weinreich, S.S.; Burgard, P.; Hoffmann, G.F.; Lindner, M.; Gerard Loeber, J.; Rupp, K.; Taruscio, D.; Vittozzi, L. A framework to start the debate on neonatal screening policies in the EU: An Expert Opinion Document. EJHG 2013, 22, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Clinical and Laboratory Standards Institute (CLSI). NBS02-A2: Newborn Screening Follow-Up; Approved Guideline—Second Edition; Clinical and Laboratory Standards Institute (CLSI): Washington, DC, USA, 2013; ISBN 1-56238-876-2. [Google Scholar]
- Dobrow, M.J.; Hagens, V.; Chafe, R.; Sullivan, T.; Rabeneck, L. Consolidated principles for screening based on a systematic review and consensus process. Can. Med. Assoc. J. 2018, 190, E422–E429. [Google Scholar] [CrossRef]
- Cornel, M.C.; Rigter, T.; Jansen, M.E.; Henneman, L. Neonatal and carrier screening for rare diseases: How innovation challenges screening criteria worldwide. J. Community Genet. 2021, 12, 257–265. [Google Scholar] [CrossRef]
- Gramer, G.; Hoffmann, G.F.; Nennstiel-Ratzel, U. Das Erweiterte Neugeborenenscreening; Springer Fachmedien Wiesbaden: Wiesbaden, Germany, 2015; ISBN 978-3-658-10492-4. [Google Scholar]
- Wald, N.J. The definition of screening. J. Med. Screen 2001, 8, 1. [Google Scholar] [CrossRef] [PubMed]
- Beauchamp, T.L.; Childress, J.F. Principles of Biomedical Ethics; Oxford University Press: New York, NY, USA; Oxford, UK, 2019; ISBN 9780190640873. [Google Scholar]
- Potter, B.K.; Etchegary, H.; Nicholls, S.G.; Wilson, B.J.; Craigie, S.M.; Araia, M.H. Education and parental involvement in decision-making about newborn screening: Understanding goals to clarify content. J. Genet. Couns. 2015, 24, 400–408. [Google Scholar] [CrossRef]
- Ulph, F.; Wright, S.; Dharni, N.; Payne, K.; Bennett, R.; Roberts, S.; Walshe, K.; Lavender, T. Provision of information about newborn screening antenatally: A sequential exploratory mixed-methods project. Health Technol. Assess. 2017, 21, 1–240. [Google Scholar] [CrossRef]
- Ulph, F.; Dharni, N.; Bennett, R.; Lavender, T. Consent for newborn screening: Screening professionals’ and parents’ views. Public Health 2020, 178, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, L.E.; Fergus, K.A.; Ojeda, N.; Au, S.M. Parental attitudes toward ethical and social issues surrounding the expansion of newborn screening using new technologies. Public Health Genom. 2011, 14, 298–306. [Google Scholar] [CrossRef] [PubMed]
- Moyer, V.A.; Calonge, N.; Teutsch, S.M.; Botkin, J.R. Expanding newborn screening: Process, policy, and priorities. Hastings Cent. Rep. 2008, 38, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Orzalesi, M.; Danhaive, O. Ethical problems with neonatal screening. Ann. Ist. Super. Sanita 2009, 45, 325–330. [Google Scholar]
- Cragun, D.; DeBate, R.D.; Pal, T. Applying public health screening criteria: How does universal newborn screening compare to universal tumor screening for Lynch syndrome in adults with colorectal cancer? J. Genet. Couns. 2015, 24, 409–420. [Google Scholar] [CrossRef]
- Howell, R.R. Ethical Issues Surrounding Newborn Screening. Int. J. Neonatal Screen. 2021, 7, 3. [Google Scholar] [CrossRef]
- Zuckerman, S. Indifferent or Uninformed? Reflections of Health Professionals on Parental Education and Consent for Expanded Newborn Screening in Israel, 2008–2016. Int. J. Neonatal Screen. 2017, 3, 12. [Google Scholar] [CrossRef]
- Ficicioglu, C. New tools and approaches to newborn screening: Ready to open Pandora’s box? Cold Spring Harb. Mol. Case Stud. 2017, 3, a001842. [Google Scholar] [CrossRef]
- Loeber, J.G.; Platis, D.; Zetterström, R.H.; Almashanu, S.; Boemer, F.; Bonham, J.R.; Borde, P.; Brincat, I.; Cheillan, D.; Dekkers, E.; et al. Neonatal Screening in Europe Revisited: An ISNS Perspective on the Current State and Developments Since 2010. Int. J. Neonatal Screen. 2021, 7, 15. [Google Scholar] [CrossRef]
- Franková, V.; Driscoll, R.O.; Jansen, M.E.; Loeber, J.G.; Kožich, V.; Bonham, J.; Borde, P.; Brincat, I.; Cheillan, D.; Dekkers, E.; et al. Regulatory landscape of providing information on newborn screening to parents across Europe. EJHG 2021, 29, 67–78. [Google Scholar] [CrossRef]
- Nicholls, S.G.; Southern, K.W. Considering consent: A structural equation modelling analysis of factors influencing decisional quality when accepting newborn screening. J. Inherit. Metab. Dis. 2014, 37, 197–205. [Google Scholar] [CrossRef]
- Nicholls, S.G.; Southern, K.W. Informed choice for newborn blood spot screening in the United Kingdom: A survey of parental perceptions. Pediatrics 2012, 130, e1527-33. [Google Scholar] [CrossRef]
- Arnold, C.G. Two faces of patient advocacy: The current controversy in newborn screening. J. Med. Ethics 2014, 40, 558–562. [Google Scholar] [CrossRef] [PubMed]
- Botkin, J.R.; Rothwell, E.; Anderson, R.A.; Rose, N.C.; Dolan, S.M.; Kuppermann, M.; Stark, L.A.; Goldenberg, A.; Wong, B. Prenatal Education of Parents About Newborn Screening and Residual Dried Blood Spots: A Randomized Clinical Trial. JAMA Pediatr. 2016, 170, 543–549. [Google Scholar] [CrossRef] [PubMed]
- Powell, C.M. What is Newborn Screening? N. C. Med. J. 2019, 80, 32–36. [Google Scholar] [CrossRef]
- Dhondt, J.-L. Neonatal screening: From the ‘Guthrie age’ to the ‘genetic age’. J. Inherit. Metab. Dis. 2007, 30, 418–422. [Google Scholar] [CrossRef]
- Oerlemans, A.J.M.; Kluijtmans, L.A.J.; van der Burg, S. The Moral Life of Professionals in Newborn Screening in the Netherlands: A Qualitative Study. Public Health Ethics 2017, 10, 19–34. [Google Scholar] [CrossRef]
- Van Dijk, T.; Kater, A.; Jansen, M.; Dondorp, W.J.; Blom, M.; Kemp, S.; Langeveld, M.; Cornel, M.C.; van der Pal, S.M.; Henneman, L. Expanding Neonatal Bloodspot Screening: A Multi-Stakeholder Perspective. Front. Pediatr. 2021, 9, 706394. [Google Scholar] [CrossRef]
- Etchegary, H.; Nicholls, S.G.; Tessier, L.; Simmonds, C.; Potter, B.K.; Brehaut, J.C.; Pullman, D.; Hayeems, R.; Zelenietz, S.; Lamoureux, M.; et al. Consent for newborn screening: Parents’ and health-care professionals’ experiences of consent in practice. Eur. J. Hum. Genet. 2016, 24, 1530–1534. [Google Scholar] [CrossRef] [PubMed]
- Harrison, D.; Zhou, Y.; Mcarthur, L. Effectiveness of parents and clinicians working together to improve pain management in newborns. CMAJ 2018, 190, S26–S27. [Google Scholar] [CrossRef]
- Lavin Venegas, C.; Taljaard, M.; Reszel, J.; Dunn, S.; Graham, I.D.; Harrold, J.; Larocque, C.; Nicholls, B.; Nicholls, S.; O’Flaherty, P.; et al. A Parent-Targeted and Mediated Video Intervention to Improve Uptake of Pain Treatment for Infants During Newborn Screening: A Pilot Randomized Controlled Trial. J. Perinat. Neonatal Nurs. 2019, 33, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Lavin Venegas, C.; Taljaard, M.; Reszel, J.; Harrison, D. Barriers and facilitators to using pain treatment during newborn screening blood tests at a mother-baby unit. J. Neonatal Nurs. 2019, 25, 139–144. [Google Scholar] [CrossRef]
- Harrison, D.; Reszel, J.; Dagg, B.; Aubertin, C.; Bueno, M.; Dunn, S.; Fuller, A.; Harrold, J.; Larocque, C.; Nicholls, S.; et al. Pain Management During Newborn Screening: Using YouTube to Disseminate Effective Pain Management Strategies. J. Perinat. Neonatal Nurs. 2017, 31, 172–177. [Google Scholar] [CrossRef] [PubMed]
- Toledo Gotor, C.; García Muro, C.; Pérez García, M.A.; Del Ruiz Prado, M.Y. Non-pharmacological analgesia during the heel lance procedure in newborns. Application in other painful procedures [Analgesia no farmacológica durante la realización del cribado metabólico. Aplicación en otros procedimientos dolorosos]. Pediatr. Atencion Prim. 2021, 23, e11–e16. [Google Scholar]
- Lan, H.-Y.; Yang, L.; Lin, C.-H.; Hsieh, K.-H.; Chang, Y.-C.; Yin, T. Breastmilk as a Multisensory Intervention for Relieving Pain during Newborn Screening Procedures: A Randomized Control Trial. Int. J. Environ. Res. Public Health 2021, 18, 13023. [Google Scholar] [CrossRef] [PubMed]
- Ganda, A.J.; Fara Ibrahim, L.; Natchimutu, K.; Ryan, C.A. No more tears? Maternal involvement during the newborn screening examination. Clin. Pediatr. 2011, 50, 753–756. [Google Scholar] [CrossRef]
- Marín Gabriel, M.Á.; Del Rey Hurtado de Mendoza, B.; Jiménez Figueroa, L.; Medina, V.; Iglesias Fernández, B.; Vázquez Rodríguez, M.; Escudero Huedo, V.; Medina Malagón, L. Analgesia with breastfeeding in addition to skin-to-skin contact during heel prick. Arch. Dis. Child. Fetal Neonatal Ed. 2013, 98, F499–F503. [Google Scholar] [CrossRef] [PubMed]
- Shah, P.S.; Aliwalas, L.I.; Shah, V. Breastfeeding or breast milk for procedural pain in neonates. Cochrane Database Syst. Rev. 2006, 3, CD004950. [Google Scholar] [CrossRef]
- Stevens, B.; Yamada, J.; Ohlsson, A. Sucrose for analgesia in newborn infants undergoing painful procedures. Cochrane Database Syst. Rev. 2004, 3, CD001069. [Google Scholar] [CrossRef]
- Fitzpatrick, P.; Fitzgerald, C.; Somerville, R.; Linnane, B. Parental awareness of newborn bloodspot screening in Ireland. Ir. J. Med. Sci. 2019, 188, 921–923. [Google Scholar] [CrossRef]
- Loeber, J.G.; Burgard, P.; Cornel, M.C.; Rigter, T.; Weinreich, S.S.; Rupp, K.; Hoffmann, G.F.; Vittozzi, L. Newborn screening programmes in Europe; arguments and efforts regarding harmonization. Part 1. From blood spot to screening result. J. Inherit. Metab. Dis. 2012, 35, 603–611. [Google Scholar] [CrossRef]
- Vass, C.M.; Georgsson, S.; Ulph, F.; Payne, K. Preferences for aspects of antenatal and newborn screening: A systematic review. BMC Pregnancy Childbirth 2019, 19, 131. [Google Scholar] [CrossRef] [PubMed]
- Ulph, F.; Lavender, D.T.; Bennett, R. Consent for newborn screening and storage of blood samples. Brit. J. Midwifery 2017, 25, 730–732. [Google Scholar] [CrossRef]
- Araia, M.H.; Wilson, B.J.; Chakraborty, P.; Gall, K.; Honeywell, C.; Milburn, J.; Ramsay, T.; Potter, B.K. Factors associated with knowledge of and satisfaction with newborn screening education: A survey of mothers. Genet. Med. 2012, 14, 963–970. [Google Scholar] [CrossRef] [PubMed]
- White, A.L.; Boardman, F.; McNiven, A.; Locock, L.; Hinton, L. Absorbing it all: A meta-ethnography of parents’ unfolding experiences of newborn screening. Soc. Sci. Med. 2021, 287, 114367. [Google Scholar] [CrossRef] [PubMed]
- Araia, M.H.; Potter, B.K. Newborn screening education on the internet: A content analysis of North American newborn screening program websites. J. Community Genet. 2011, 2, 127–134. [Google Scholar] [CrossRef]
- IJzebrink, A.; van Dijk, T.; Franková, V.; Loeber, G.; Kožich, V.; Henneman, L.; Jansen, M. Informing Parents about Newborn Screening: A European Comparison Study. Int. J. Neonatal Screen. 2021, 7, 13. [Google Scholar] [CrossRef]
- Hewlett, J.; Waisbren, S.E. A review of the psychosocial effects of false-positive results on parents and current communication practices in newborn screening. J. Inherit. Metab. Dis. 2006, 29, 677–682. [Google Scholar] [CrossRef]
- Anderson, R.; Rothwell, E.; Botkin, J.R. Newborn screening: Ethical, legal, and social implications. Annu. Rev. Nurs. Res. 2011, 29, 113–132. [Google Scholar] [CrossRef]
- Miller, B.C.; Goldenberg, A.J.; Bonhomme, N.F. Digital peer-to-peer information seeking and sharing: Opportunities for education and collaboration in newborn screening. Am. J. Med. Genet. C Semin. Med. Genet. 2021, 187, 64–69. [Google Scholar] [CrossRef]
- Bonham, J.R. Impact of new screening technologies: Should we screen and does phenotype influence this decision? J. Inherit. Metab. Dis. 2013, 36, 681–686. [Google Scholar] [CrossRef]
- Rothwell, E.; Johnson, E.; Wong, B.; Goldenberg, A.; Tarini, B.A.; Riches, N.; Stark, L.A.; Pries, C.; Langbo, C.; Langen, E.; et al. Comparison of Video, App, and Standard Consent Processes on Decision-Making for Biospecimen Research: A Randomized Controlled Trial. J. Empir. Res. Hum. Res. Ethics 2020, 15, 252–260. [Google Scholar] [CrossRef] [PubMed]
- Vittozzi, L.; Hoffmann, G.F.; Cornel, M.; Loeber, G. Evaluation of Population Newborn Screening Practices for Rare Disorders in Member States of the European Union. Available online: https://isns-neoscreening.org/wp-content/uploads/2016/06/Consensus-workshop-conclusions-FINAL.pdf (accessed on 15 December 2021).
- Chen, B.; Mei, J.; Kalman, L.; Shahangian, S.; Williams, I.; Gagnon, M.B.; Bosse, D.; Ragin, A.; Cuthbert, C.; Zehnbauer, B. Good laboratory practices for biochemical genetic testing and newborn screening for inherited metabolic disorders. Morb. Mortal. Wkly. Rep. 2012, 61, 1–37. [Google Scholar]
- De Jesús, V.R.; Mei, J.V.; Cordovado, S.K.; Cuthbert, C.D. The Newborn Screening Quality Assurance Program at the Centers for Disease Control and Prevention: Thirty-five Year Experience Assuring Newborn Screening Laboratory Quality. Int. J. Neonatal Screen. 2015, 1, 13–26. [Google Scholar] [CrossRef] [PubMed]
- Pickens, C.A.; Sternberg, M.; Seeterlin, M.; de Jesús, V.R.; Morrissey, M.; Manning, A.; Bhakta, S.; Held, P.K.; Mei, J.; Cuthbert, C.; et al. Harmonizing Newborn Screening Laboratory Proficiency Test Results Using the CDC NSQAP Reference Materials. Int. J. Neonatal Screen. 2020, 6, 75. [Google Scholar] [CrossRef]
- Bonham, J.R. The organisation of training for laboratory scientists in inherited metabolic disease, newborn screening and paediatric clinical chemistry. Clin. Biochem. 2014, 47, 763–764. [Google Scholar] [CrossRef]
- Wilcken, B. Screening for disease in the newborn: The evidence base for blood-spot screening. Pathology 2012, 44, 73–79. [Google Scholar] [CrossRef]
- Prosser, L.A.; Grosse, S.D.; Kemper, A.R.; Tarini, B.A.; Perrin, J.M. Decision analysis, economic evaluation, and newborn screening: Challenges and opportunities. Genet. Med. 2013, 14, 703–712. [Google Scholar] [CrossRef]
- Streetly, A.; Madden, V. Public health for paediatricians: Population screening. Arch. Dis. Child. Educ. Pract. Ed. 2016, 101, 304–310. [Google Scholar] [CrossRef]
- Malvagia, S.; Forni, G.; Ombrone, D.; La Marca, G. Development of Strategies to Decrease False Positive Results in Newborn Screening. Int. J. Neonatal Screen. 2020, 6, 84. [Google Scholar] [CrossRef]
- Peng, G.; Tang, Y.; Cowan, T.M.; Enns, G.M.; Zhao, H.; Scharfe, C. Reducing False-Positive Results in Newborn Screening Using Machine Learning. Int. J. Neonatal Screen. 2020, 6, 16. [Google Scholar] [CrossRef] [PubMed]
- Webster, D. Quality performance of newborn screening systems: Strategies for improvement. J. Inherit. Metab. Dis. 2007, 30, 576–584. [Google Scholar] [CrossRef]
- Bhattacharya, K.; Wotton, T.; Wiley, V. The evolution of blood-spot newborn screening. Transl. Pediatr. 2014, 3, 63–70. [Google Scholar] [PubMed]
- Gramer, G.; Hoffmann, G.F. Second-tier strategies in newborn screening–Potential and limitations. Medgen 2022, 34, 21–28. [Google Scholar] [CrossRef]
- Ombrone, D.; Giocaliere, E.; Forni, G.; Malvagia, S.; La Marca, G. Expanded newborn screening by mass spectrometry: New tests, future perspectives. Mass Spectrom. Rev. 2016, 35, 71–84. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Schultz, N.; Sant, D.; Norcross, S.; Dansithong, W.; Hart, K.; Asay, B.; Little, J.; Chung, K.; Oakeson, K.F.; Young, E.L.; et al. Methods and feasibility study for exome sequencing as a universal second-tier test in newborn screening. Genet. Med. 2021, 23, 767–776. [Google Scholar] [CrossRef]
- McHugh, D.M.S.; Cameron, C.A.; Abdenur, J.E.; Abdulrahman, M.; Adair, O.; Al Nuaimi, S.A.; Åhlman, H.; Allen, J.J.; Antonozzi, I.; Archer, S.; et al. Clinical validation of cutoff target ranges in newborn screening of metabolic disorders by tandem mass spectrometry: A worldwide collaborative project. Genet. Med. 2011, 13, 230–254. [Google Scholar] [CrossRef]
- Marquardt, G.; Currier, R.; McHugh, D.M.S.; Gavrilov, D.; Magera, M.J.; Matern, D.; Oglesbee, D.; Raymond, K.; Rinaldo, P.; Smith, E.H.; et al. Enhanced interpretation of newborn screening results without analyte cutoff values. Genet. Med. 2012, 14, 648–655. [Google Scholar] [CrossRef]
- Fleischman, A.; Thompson, J.D.; Glass, M. Systematic Data Collection to Inform Policy Decisions: Integration of the Region 4 Stork (R4S) Collaborative Newborn Screening Database to Improve MS/MS Newborn Screening in Washington State. JIMD Rep. 2014, 13, 15–21. [Google Scholar] [CrossRef]
- Hall, P.L.; Marquardt, G.; McHugh, D.M.S.; Currier, R.J.; Tang, H.; Stoway, S.D.; Rinaldo, P. Postanalytical tools improve performance of newborn screening by tandem mass spectrometry. Genet. Med. 2014, 16, 889–895. [Google Scholar] [CrossRef]
- Maase, R.; Bouva, M.; Rinaldo, P.; Visser, G.; Monique de Sain-van der Velden; Schielen, P. Striving towards a Better Predictive Value from the Dutch Newborn Screening Results. Abstract. Int. J. Neonatal Screen. 2018, 4, 28. [Google Scholar] [CrossRef]
- Gavrilov, D.K.; Piazza, A.L.; Pino, G.; Turgeon, C.; Matern, D.; Oglesbee, D.; Raymond, K.; Tortorelli, S.; Rinaldo, P. The Combined Impact of CLIR Post-Analytical Tools and Second Tier Testing on the Performance of Newborn Screening for Disorders of Propionate, Methionine, and Cobalamin Metabolism. Int. J. Neonatal Screen. 2020, 6, 33. [Google Scholar] [CrossRef] [PubMed]
- Sörensen, L.; von Döbeln, U.; Åhlman, H.; Ohlsson, A.; Engvall, M.; Naess, K.; Backman-Johansson, C.; Nordqvist, Y.; Wedell, A.; Zetterström, R.H. Expanded Screening of One Million Swedish Babies with R4S and CLIR for Post-Analytical Evaluation of Data. Int. J. Neonatal Screen. 2020, 6, 42. [Google Scholar] [CrossRef]
- Tangeraas, T.; Sæves, I.; Klingenberg, C.; Jørgensen, J.; Kristensen, E.; Gunnarsdottir, G.; Hansen, E.V.; Strand, J.; Lundman, E.; Ferdinandusse, S.; et al. Performance of Expanded Newborn Screening in Norway Supported by Post-Analytical Bioinformatics Tools and Rapid Second-Tier DNA Analyses. Int. J. Neonatal Screen. 2020, 6, 51. [Google Scholar] [CrossRef]
- Rowe, A.D.; Stoway, S.D.; Åhlman, H.; Arora, V.; Caggana, M.; Fornari, A.; Hagar, A.; Hall, P.L.; Marquardt, G.C.; Miller, B.J.; et al. A Novel Approach to Improve Newborn Screening for Congenital Hypothyroidism by Integrating Covariate-Adjusted Results of Different Tests into CLIR Customized Interpretive Tools. Int. J. Neonatal Screen. 2021, 7, 23. [Google Scholar] [CrossRef]
- Rinaldo, P. Precision Newborn Screening Driven by Results Adjustments for Multiple Covariates. Abstract. Int. J. Neonatal Screen. 2018, 4, 28. [Google Scholar] [CrossRef]
- Hall, P.L.; Wittenauer, A.; Hagar, A. Post-Analytical Tools for the Triage of Newborn Screening Results in Follow-up Can Reduce Confirmatory Testing and Guide Performance Improvement. Int. J. Neonatal Screen. 2020, 6, 20. [Google Scholar] [CrossRef] [PubMed]
- Jones, D.; Garcia, S.; Ruiz-Schultz, N.; Gaviglio, A.; Cuthbert, C. A Strong Start: Enhancing Newborn Screening for Precision Public Health|Blogs|CDC. Available online: https://blogs.cdc.gov/genomics/2020/10/13/a-strong-start/ (accessed on 15 November 2021).
- Gaviglio, A.; Cuthbert, C. Enhancing Data-Driven Disease Detection in Newborns: A National Data Platform for Modernizing Newborn Screening Data Analytics and Interpretation. Abstract. Int. J. Neonatal Screen. 2021, 7, 71. [Google Scholar] [CrossRef]
- Lin, B.; Yin, J.; Shu, Q.; Deng, S.; Li, Y.; Jiang, P.; Yang, R.; Pu, C. Integration of Machine Learning Techniques as Auxiliary Diagnosis of Inherited Metabolic Disorders: Promising Experience with Newborn Screening Data. Lecture Notes Inst. Comp. Sci. Social-Inf. Telecommun. Eng. LNICST 2019, 292, 334–349. [Google Scholar] [CrossRef]
- Chudleigh, J.; Chinnery, H. Psychological impact of NBS for CF. Int. J. Neonatal Screen. 2020, 6, 27. [Google Scholar] [CrossRef]
- Franková, V.; Hermánková, R.; Dohnalová, A.; Dragomirecká, E.; Pešková, K.; Oliveriusová; Votava, F.; Holubová, A.; Kožich, V. The Maternal Stress of False Positive Newborn Screening Results. Abstract. Int. J. Neonatal Screen. 2021, 7, 71. [Google Scholar] [CrossRef]
- Rosettenstein, K.R.; Lain, S.J.; Wormleaton, N.; Jack, M.M. A systematic review of the outcomes of false-positive results on newborn screening for congenital hypothyroidism. Clin. Endocrinol. 2021, 95, 766–781. [Google Scholar] [CrossRef] [PubMed]
- Rueegg, C.S.; Barben, J.; Hafen, G.M.; Moeller, A.; Jurca, M.; Fingerhut, R.; Kuehni, C.E. Newborn screening for cystic fibrosis-The parent perspective. J. Cyst. Fibros. 2016, 15, 443–451. [Google Scholar] [CrossRef] [PubMed]
- Moody, L.; Atkinson, L.; Kehal, I.; Bonham, J.R. Healthcare professionals’ and parents’ experiences of the confirmatory testing period: A qualitative study of the UK expanded newborn screening pilot. BMC Pediatr. 2017, 17, 121. [Google Scholar] [CrossRef] [PubMed]
- Tangeraas, T. What Happens after Recall, Who Should Give the Results to Families? Abstract. Int. J. Neonatal Screen. 2021, 7, 71. [Google Scholar] [CrossRef]
- O’Connor, K.; Jukes, T.; Goobie, S.; DiRaimo, J.; Moran, G.; Potter, B.K.; Chakraborty, P.; Rupar, C.A.; Gannavarapu, S.; Prasad, C. Psychosocial impact on mothers receiving expanded newborn screening results. Eur. J. Hum. Genet. 2018, 26, 477–484. [Google Scholar] [CrossRef]
- Karaceper, M.D.; Chakraborty, P.; Coyle, D.; Wilson, K.; Kronick, J.B.; Hawken, S.; Davies, C.; Brownell, M.; Dodds, L.; Feigenbaum, A.; et al. The health system impact of false positive newborn screening results for medium-chain acyl-CoA dehydrogenase deficiency: A cohort study. Orphanet. J. Rare Dis. 2016, 11, 12. [Google Scholar] [CrossRef]
- Schmidt, J.L.; Castellanos-Brown, K.; Childress, S.; Bonhomme, N.; Oktay, J.S.; Terry, S.F.; Kyler, P.; Davidoff, A.; Greene, C. The impact of false-positive newborn screening results on families: A qualitative study. Genet. Med. 2012, 14, 76–80. [Google Scholar] [CrossRef]
- Finan, C.; Nasr, S.Z.; Rothwell, E.; Tarini, B.A. Primary care providers’ experiences notifying parents of cystic fibrosis newborn screening results. Clin. Pediatr. 2015, 54, 67–75. [Google Scholar] [CrossRef]
- Howell, R.R. The high price of false positives. Mol. Genet. Metab. 2006, 87, 180–183. [Google Scholar] [CrossRef]
- Tu, W.-J.; He, J.; Chen, H.; Shi, X.-D.; Li, Y. Psychological effects of false-positive results in expanded newborn screening in China. PLoS ONE 2012, 7, e36235. [Google Scholar] [CrossRef] [PubMed]
- Brockow, I.; Nennstiel, U. Parents’ experience with positive newborn screening results for cystic fibrosis. Eur. J. Pediatr. 2019, 178, 803–809. [Google Scholar] [CrossRef] [PubMed]
- Barben, J.; Chudleigh, J. Processing Newborn Bloodspot Screening Results for CF. Int. J. Neonatal Screen. 2020, 6, 25. [Google Scholar] [CrossRef]
- Chudleigh, J.; Ren, C.L.; Barben, J.; Southern, K.W. International approaches for delivery of positive newborn bloodspot screening results for CF. J. Cyst. Fibros. 2019, 18, 614–621. [Google Scholar] [CrossRef]
- Salm, N.; Yetter, E.; Tluczek, A. Informing parents about positive newborn screen results: Parents’ recommendations. J. Child Health Care 2012, 16, 367–381. [Google Scholar] [CrossRef] [PubMed]
- Advisory Committee on Heritable Disorders in Newborns and Children. Communication Guide for Clinicians and Providers to Help Frame the Initial Notification and Discussion with Parents about Positive/Abnormal/Out-Of-Range Newborn Screening Results. Available online: https://www.hrsa.gov/sites/default/files/hrsa/advisory-committees/heritable-disorders/reports-recommendations/reports/achdnc-communication-guide-newborn.pdf (accessed on 17 November 2022).
- Summar, M.; Kirmse, B.; Monaco, J. Mind the Gap. Mol. Genet. Metab. 2014, 113, 1. [Google Scholar] [CrossRef]
- Viall, S.; Jain, S.; Chapman, K.; Mew, N.A.; Summar, M.; Kirmse, B. Short-term follow-up systems for positive newborn screens in the Washington Metropolitan Area and the United States. Mol. Genet. Metab. 2015, 116, 226–230. [Google Scholar] [CrossRef]
- Chudleigh, J.; Holder, P.; Moody, L.; Simpson, A.; Southern, K.; Morris, S.; Fusco, F.; Ulph, F.; Bryon, M.; Bonham, J.R.; et al. Process evaluation of co-designed interventions to improve communication of positive newborn bloodspot screening results. BMJ Open 2021, 11, e050773. [Google Scholar] [CrossRef]
- Buchbinder, M.; Timmermans, S. Newborn screening for metabolic disorders: Parental perceptions of the initial communication of results. Clin. Pediatr. 2012, 51, 739–744. [Google Scholar] [CrossRef]
- Moody, L.; Choudhry, K. Parental views on informed consent for expanded newborn screening. Health Expect. 2013, 16, 239–250. [Google Scholar] [CrossRef]
- DeLuca, J.M.; Kearney, M.H.; Norton, S.A.; Arnold, G.L. Internet use by parents of infants with positive newborn screens. J. Inherit. Metab. Dis. 2012, 35, 879–884. [Google Scholar] [CrossRef]
- Bellcross, C.A.; Harmond, L.; Floyd-Browning, P.; Singh, R. Infrastructure and educational needs of newborn screening short-term follow-up programs within the southeast regional newborn screening & genetics collaborative: A pilot survey. Healthcare 2015, 3, 964–972. [Google Scholar] [CrossRef] [PubMed]
- Newborn Screening Ontario. Screen Positive Results. Available online: https://www.newbornscreening.on.ca/en/screening-results/screen-positive-results (accessed on 9 November 2022).
- Chudleigh, J.; Chinnery, H.; Holder, P.; Carling, R.S.; Southern, K.; Olander, E.; Moody, L.; Morris, S.; Ulph, F.; Bryon, M.; et al. Processing of positive newborn screening results: A qualitative exploration of current practice in England. BMJ Open 2020, 10, e044755. [Google Scholar] [CrossRef] [PubMed]
- Vernooij-van Langen, A.M.M.; van der Pal, S.M.; Reijntjens, A.J.T.; Loeber, J.G.; Dompeling, E.; Dankert-Roelse, J.E. Parental knowledge reduces long term anxiety induced by false-positive test results after newborn screening for cystic fibrosis. Mol. Genet. Metab. Rep. 2014, 1, 334–344. [Google Scholar] [CrossRef] [PubMed]
- Deutsche Gesellschaft für Kinder- und Jugendmedizin (DGKJ). AWMF-S1-Leitlinie 027-021 “Konfirmationsdiagnostik bei Verdacht auf Angeborene Stoffwechselkrankheiten aus dem Neugeborenenscreening”. Available online: https://www.awmf.org/leitlinien/detail/ll/027-021.html (accessed on 20 April 2022).
- Nationales Aktionsbündnis für Menschen mit Seltenen Erkrankungen (NAMSE). Nationaler Aktionsplan für Menschen mit Seltenen Erkrankungen: Handlungsfelder, Empfehlungen und Maßnahmenvorschläge. 2013. Available online: https://www.namse.de/ (accessed on 3 February 2022).
- Council of the European Union. Council Recommendation of 8 June 2009 on an Action in the Field of Rare Diseases. Available online: https://eur-lex.europa.eu/legal-content/DE/TXT/?uri=uriserv%3AOJ.C_.2009.151.01.0007.01.DEU&toc=OJ%3AC%3A2009%3A151%3ATOC (accessed on 17 February 2022).
- Deutscher Ethikrat. Herausforderungen im Umgang mit seltenen Erkrankungen: AD-HOC-EMPFEHLUNG. Berlin 2018. Available online: https://www.ethikrat.org/publikationen/publikationsdetail/?tx_wwt3shop_detail%5Bproduct%5D=116&tx_wwt3=&cHash=b3e78fc99b523a5226a74aca8f971b95 (accessed on 13 December 2021).
- Sontag, M.K.; Sarkar, D.; Comeau, A.M.; Hassell, K.; Botto, L.D.; Parad, R.; Rose, S.R.; Wintergerst, K.A.; Smith-Whitley, K.; Singh, S.; et al. Case Definitions for Conditions Identified by Newborn Screening Public Health Surveillance. Int. J. Neonatal Screen. 2018, 4, 16. [Google Scholar] [CrossRef] [PubMed]
- Heather, N.; Webster, D. It All Depends What You Count-The Importance of Definitions in Evaluation of CF Screening Performance. Int. J. Neonatal Screen. 2020, 6, 47. [Google Scholar] [CrossRef] [PubMed]
- Blom, M.; Zetterström, R.H.; Stray-Pedersen, A.; Gilmour, K.; Gennery, A.R.; Puck, J.M.; van der Burg, M. Recommendations for uniform definitions used in newborn screening for severe combined immunodeficiency. J. Allergy Clin. Immunol. 2021, 149, 1428–1436. [Google Scholar] [CrossRef]
- Kronn, D.; Mofidi, S.; Braverman, N.; Harris, K. Diagnostic guidelines for newborns who screen positive in newborn screening. Genet. Med. 2010, 12, S251–S255. [Google Scholar] [CrossRef]
- Bräuer, P. Rechtsfragen des Neugeborenen-Screenings unter besonderer Beachtung des Datenschutzrechts; Eberhard Karls Universität Tübingen: Tübingen, Germany, 2020. [Google Scholar]
- Spady; Saunders; Bamforth. Who gets lost: Follow-up of suspect results in a newborn screening program. Pediatrics 1998, 102, E21A. [Google Scholar] [CrossRef]
- Darby, E.; Thompson, J.; Johnson, C.; Singh, S.; Ojodu, J. Establishing a National Community of Practice for Newborn Screening Follow-Up. Int. J. Neonatal Screen. 2021, 7, 49. [Google Scholar] [CrossRef]
- Percenti, L.; Vickery, G. Newborn Screening Follow-up. N. C. Med. J. 2019, 80, 37–41. [Google Scholar] [CrossRef] [PubMed]
- Robert Koch-Institut (RKI). Richtlinie der Gendiagnostik-Kommission (GEKO) für die Anforderungen an die Durchführung genetischer Reihenuntersuchungen gemäß § 23 Abs. 2 Nr. 6 GenDG: Revidierte Fassung vom 26.06.2020, veröffentlicht und in Kraft getreten am 16.07.2020, ersetzt die Fassung vom 16.11.2012. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2020, 63, 1311–1317. [Google Scholar] [CrossRef]
- Liebl, B.; Nennstiel-Ratzel, U.; von Kries, R.; Fingerhut, R.; Olgemöller, B.; Zapf, A.; Roscher, A.A. Expanded newborn screening in Bavaria: Tracking to achieve requested repeat testing. Prev. Med. 2002, 34, 132–137. [Google Scholar] [CrossRef] [PubMed]
- Gramer, G.; Brockow, I.; Labitzke, C.; Fang-Hoffmann, J.; Beivers, A.; Feyh, P.; Hoffmann, G.F.; Nennstiel, U.; Sommerburg, O. Implementing a tracking system for confirmatory diagnostic results after positive newborn screening for cystic fibrosis-implications for process quality and patient care. Eur. J. Pediatr. 2021, 180, 1145–1155. [Google Scholar] [CrossRef]
- Nennstiel, U.; Lüders, A.; Brockow, I. Newborn-screening in Germany [Neugeborenen-Screening-Programme]. Public Health Forum 2019, 27, 317–319. [Google Scholar] [CrossRef]
- Gramer, G.; Hauck, F.; Lobitz, S.; Sommerburg, O.; Speckmann, C.; Hoffmann, G.F. Neugeborenenscreening 2020. Monatsschr Kinderheilkd 2017, 165, 216–225. [Google Scholar] [CrossRef]
- Lajic, S.; Karlsson, L.; Zetterström, R.H.; Falhammar, H.; Nordenström, A. The Success of a Screening Program Is Largely Dependent on Close Collaboration between the Laboratory and the Clinical Follow-Up of the Patients. Int. J. Neonatal Screen. 2020, 6, 68. [Google Scholar] [CrossRef]
- Burgard, P.; Rupp, K.; Lindner, M.; Haege, G.; Rigter, T.; Weinreich, S.S.; Loeber, J.G.; Taruscio, D.; Vittozzi, L.; Cornel, M.C.; et al. Newborn screening programmes in Europe; arguments and efforts regarding harmonization. Part 2. From screening laboratory results to treatment, follow-up and quality assurance. J. Inherit. Metab. Dis. 2012, 35, 613–625. [Google Scholar] [CrossRef]
- Mütze, U.; Garbade, S.F.; Gramer, G.; Lindner, M.; Freisinger, P.; Grünert, S.C.; Hennermann, J.; Ensenauer, R.; Thimm, E.; Zirnbauer, J.; et al. Long-term Outcomes of Individuals With Metabolic Diseases Identified Through Newborn Screening. Pediatrics 2020, 146, e20200444. [Google Scholar] [CrossRef]
- Powell, C.M. Newborn Screening and Long-term Outcomes. Pediatrics 2020, 146, e2020023663. [Google Scholar] [CrossRef]
- Hinman, A.R.; Mann, M.Y.; Singh, R.H. Newborn dried bloodspot screening: Mapping the clinical and public health components and activities. Genet. Med. 2009, 11, 418–424. [Google Scholar] [CrossRef]
- Hinton, C.F.; Mai, C.T.; Nabukera, S.K.; Botto, L.D.; Feuchtbaum, L.; Romitti, P.A.; Wang, Y.; Piper, K.N.; Olney, R.S. Developing a public health-tracking system for follow-up of newborn screening metabolic conditions: A four-state pilot project structure and initial findings. Genet. Med. 2014, 16, 484–490. [Google Scholar] [CrossRef]
- Deutsche Gesellschaft für Epidemiologie (DGEpi). Leitlinien und Empfehlungen zur Sicherung von Guter Epidemiologischer Praxis (GEP). Available online: https://www.dgepi.de/de/berichte-und-publikationen/leitlinien-und-empfehlungen/ (accessed on 2 March 2022).
- Sheller, R.; Ojodu, J.; Griffin, E.; Edelman, S.; Yusuf, C.; Pigg, T.; Huston, A.; Fitzek, B.; Boyle, J.G.; Singh, S. The Landscape of Severe Combined Immunodeficiency Newborn Screening in the United States in 2020: A Review of Screening Methodologies and Targets, Communication Pathways, and Long-Term Follow-Up Practices. Front. Immunol. 2020, 11, 577853. [Google Scholar] [CrossRef]
- Brower, A.; Chan, K.; Hartnett, M.; Taylor, J. The Longitudinal Pediatric Data Resource: Facilitating Longitudinal Collection of Health Information to Inform Clinical Care and Guide Newborn Screening Efforts. Int. J. Neonatal Screen. 2021, 7, 37. [Google Scholar] [CrossRef] [PubMed]
- Wilcken, B.; Rinaldo, P.; Matern, D. Newborn Screening for Inborn Errors of Metabolism. In Inborn Metabolic Diseases; Saudubray, J.-M., van den Berghe, G., Walter, J.H., Eds.; Springer Berlin Heidelberg: Berlin/Heidelberg, Germany, 2012; pp. 75–86. ISBN 978-3-642-15719-6. [Google Scholar]
- Wright, E.L.; van Hove, J.L.K.; Thomas, J. Mountain States Genetics Regional Collaborative Center’s Metabolic Newborn Screening Long-term Follow-up Study: A collaborative multi-site approach to newborn screening outcomes research. Genet. Med. 2010, 12, S228–S241. [Google Scholar] [CrossRef]
- Kölker, S. The Value of European Registries and Networks for Changing Practice and Informing Guidelines. Abstract. Int. J. Neonatal Screen. 2021, 7, 71. [Google Scholar] [CrossRef]
- Kölker, S. Long-Term Outcome Studies, the (Often) Neglected Part of Newborn Screening Programs. Abstract. Int. J. Neonatal Screen. 2018, 4, 28. [Google Scholar] [CrossRef]
- Wasserstein, M.P. Long-term follow-up in newborn screening: The role of collaboration. Genet. Med. 2016, 1–2. [Google Scholar] [CrossRef]
- Vittozzi, L.; Burgard, P.; Cornel, M.; Hoffmann, G.F.; Lindner, M.; Loeber, J.G.; Rigter, T.; Rupp, K.; Taruscio, D.; Weinreich, S. Executive Report to the European Commission on Newborn Screening in the European Union. Available online: https://isns-neoscreening.org/wp-content/uploads/2016/06/Executive-Report-to-EC-FINAL.pdf (accessed on 15 December 2021).
- Zuckerman, A.E.; Badawi, D.; Brosco, J.P.; Brower, A.; Finitzo, T.; Flannery, D.; Green, N.; Greene, C.; Hassell, K.; Leslie, N.D.; et al. The Role of Quality Measures to Promote Long-Term Follow-Up of Children Identified by Newborn Screening Programs: Presented by the Follow-Up and Treatment Workgroup to the Advisory Committee on Heritable Disorders in Newborns and Children on 8 February 2018. Available online: https://www.hrsa.gov/sites/default/files/hrsa/advisory-committees/heritable-disorders/reports-recommendations/reports/role-of-quality-measures-in-nbs-sept2018-508c.pdf (accessed on 12 October 2021).
- Hinton, C.F.; Feuchtbaum, L.; Kus, C.A.; Kemper, A.R.; Berry, S.A.; Levy-Fisch, J.; Luedtke, J.; Kaye, C.; Boyle, C.A. What questions should newborn screening long-term follow-up be able to answer? A statement of the US Secretary for Health and Human Services’ Advisory Committee on Heritable Disorders in Newborns and Children. Genet. Med. 2011, 13, 861–865. [Google Scholar] [CrossRef] [PubMed]
- Opladen, T.; Gleich, F.; Kozich, V.; Scarpa, M.; Martinelli, D.; Schaefer, F.; Jeltsch, K.; Juliá-Palacios, N.; García-Cazorla, Á.; Dionisi-Vici, C.; et al. U-IMD: The first Unified European registry for inherited metabolic diseases. Orphanet J. Rare Dis. 2021, 16, 95. [Google Scholar] [CrossRef] [PubMed]
- Boyle, C.A.; Bocchini, J.A., Jr.; Kelly, J. Reflections on 50 years of newborn screening. Pediatrics 2014, 133, 961–963. [Google Scholar] [CrossRef]
- Andermann, A. Presentation: Revisiting Wilson and Jungner in the genomic age: A review of screening criteria over the past 40 years. VHPB Budapest. Bull. World Health Organ. 2008, 86, 317–319. [Google Scholar]
- Andermann, A.; Blancquaert, I. Genetic screening: A primer for primary care. Can. Family Physician 2010, 56, 333–339. [Google Scholar]
- Martz, M.P.; Humble, W.; Nabor, C.; Waddell, V. Applying transparency and quality measurement to improve newborn screening: Lessons learned from arizona’s transit time project. J. Public Health Manag. Pract. 2015, 21, 217–219. [Google Scholar] [CrossRef] [PubMed]
- Viall, S.; Calhoun, A.; Mew, N.A.; Tarini, B.A. How a baby with classic galactosemia was nearly missed: When the test succeeds but system fails. Am. J. Med. Genet. A 2020, 182, 1750–1753. [Google Scholar] [CrossRef]
- Sontag, M.K.; Miller, J.I.; McKasson, S.; Sheller, R.; Edelman, S.; Yusuf, C.; Singh, S.; Sarkar, D.; Bocchini, J.; Scott, J.; et al. Newborn screening timeliness quality improvement initiative: Impact of national recommendations and data repository. PLoS ONE 2020, 15, e0231050. [Google Scholar] [CrossRef]
- Marsden, D.; Larson, C.; Levy, H.L. Newborn screening for metabolic disorders. J. Pediatr. 2006, 148, 577–584. [Google Scholar] [CrossRef]
- Miller, F.A.; Cressman, C.; Hayeems, R. Governing population screening in an age of expansion: The case of newborn screening. Can. J. Public Health 2015, 106, e244–e248. [Google Scholar] [CrossRef]
- Kellar-Guenther, Y.; Sontag, M.K.; Linder, E.; Singh, S.; Sheller, R.; Ojodu, J. Analyzing Patterns in NewSTEPs Site Review Recommendations: Practical Applications for Newborn Screening Programs. Int. J. Neonatal Screen. 2019, 5, 13. [Google Scholar] [CrossRef]
- Torresani, T. Quality control requirements in neonatal screening. Eur. J. Pediatr. 2003, 162, S54–S56. [Google Scholar] [CrossRef] [PubMed]
- Busse, R.; Klazinga, N.; Panteli, D.; Quentin, W. (Eds.) Improving Healthcare Quality in Europe: Characteristics, Effectiveness and Implementation of Different Strategies; WHO Regional Office for Europe: Copenhagen, Denmark, 2019; ISBN 9789289051750. [Google Scholar]
- Ruckstuhl, B.; Somaini, B.; Twisselmann, W. Förderung der Qualität in Gesundheitsprojekten: Der Public Health Action Cycle als Arbeitsinstrument. Zürich. 2008. Available online: http://www.quint-essenz.ch/de/files/Foerderung_der_Qualitaet.pdf (accessed on 3 December 2021).
- Pluscauskas, M.; Henderson, M.; Milburn, J.; Chakraborty, P. Building a Newborn Screening Information Management System from Theory to Practice. Int. J. Neonatal Screen. 2019, 5, 9. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.H.; Brown, S.J.; Hale, P.M.; Narlow, K.; Gurung, S.; Salvatore, M.L.; Tchamako, J.K. Using Informatics to Build a Digital Health Footprint of Patients Living With Inherited Metabolic Disorders Identified by Newborn Screening. J. Public Health Manag. Pract. 2020, 28, E340–E344. [Google Scholar] [CrossRef] [PubMed]
- Watkins, M.; Au, A.; Vuong, T.; Wallis, H.; Hart, K.; Rohrwasser, A.; Eilbeck, K. ResultsMyWay: Combining Fast Healthcare Interoperability Resources (FHIR), Clinical Quality Language (CQL), and informational resources to create a newborn screening application. AMIA Jt. Summits Trans. Sci. Proc. 2021, 2021, 615–623. [Google Scholar]
- Loeber, J.G. European Union Should Actively Stimulate and Harmonise Neonatal Screening Initiatives. Int. J. Neonatal Screen. 2018, 4, 32. [Google Scholar] [CrossRef] [PubMed]


Wilson and Jungner’s classic screening criteria (1968) [29]
|
Andermann’s Synthesis of emerging screening criteria (2008) [22]
|
Specific recommendations for parental education about NBS Setting:
|
Specific recommendations for informing parents about abnormal (positive) NBS results [32,105,116,120,124,125,127,128,131,133,134]
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Odenwald, B.; Brockow, I.; Hanauer, M.; Lüders, A.; Nennstiel, U. Is Our Newborn Screening Working Well? A Literature Review of Quality Requirements for Newborn Blood Spot Screening (NBS) Infrastructure and Procedures. Int. J. Neonatal Screen. 2023, 9, 35. https://doi.org/10.3390/ijns9030035
Odenwald B, Brockow I, Hanauer M, Lüders A, Nennstiel U. Is Our Newborn Screening Working Well? A Literature Review of Quality Requirements for Newborn Blood Spot Screening (NBS) Infrastructure and Procedures. International Journal of Neonatal Screening. 2023; 9(3):35. https://doi.org/10.3390/ijns9030035
Chicago/Turabian StyleOdenwald, Birgit, Inken Brockow, Marianne Hanauer, Anja Lüders, and Uta Nennstiel. 2023. "Is Our Newborn Screening Working Well? A Literature Review of Quality Requirements for Newborn Blood Spot Screening (NBS) Infrastructure and Procedures" International Journal of Neonatal Screening 9, no. 3: 35. https://doi.org/10.3390/ijns9030035
APA StyleOdenwald, B., Brockow, I., Hanauer, M., Lüders, A., & Nennstiel, U. (2023). Is Our Newborn Screening Working Well? A Literature Review of Quality Requirements for Newborn Blood Spot Screening (NBS) Infrastructure and Procedures. International Journal of Neonatal Screening, 9(3), 35. https://doi.org/10.3390/ijns9030035