Multi-Laboratory Evaluation of Prototype Dried Blood Spot Quality Control Materials for Creatine Kinase-MM Newborn Screening Assays


 , , ,
, , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Preparation of DBS-QC
2.2. Study Protocol and Data Analysis
3. Results
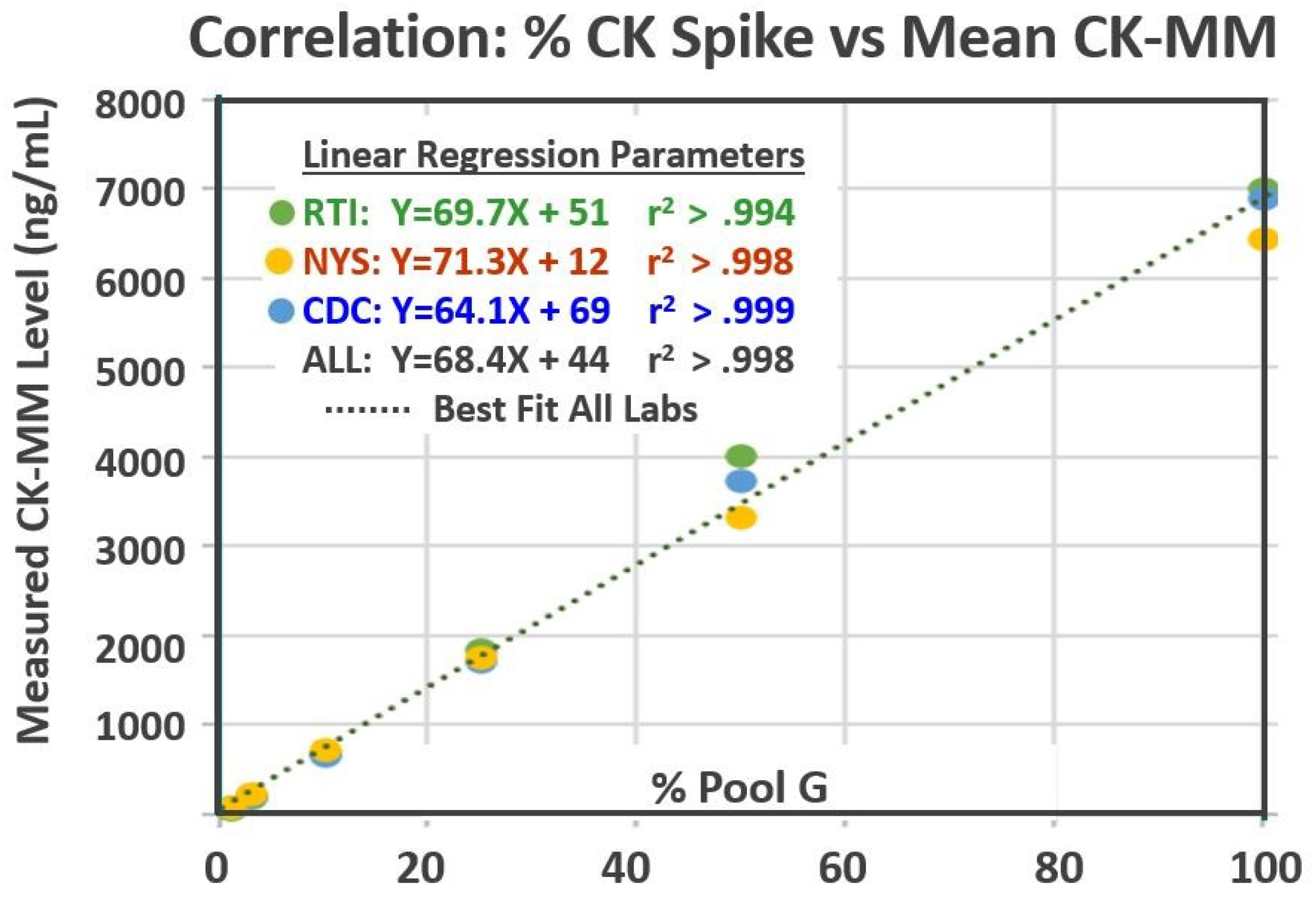
3.1. Range, Variances, and Comparability between Laboratories
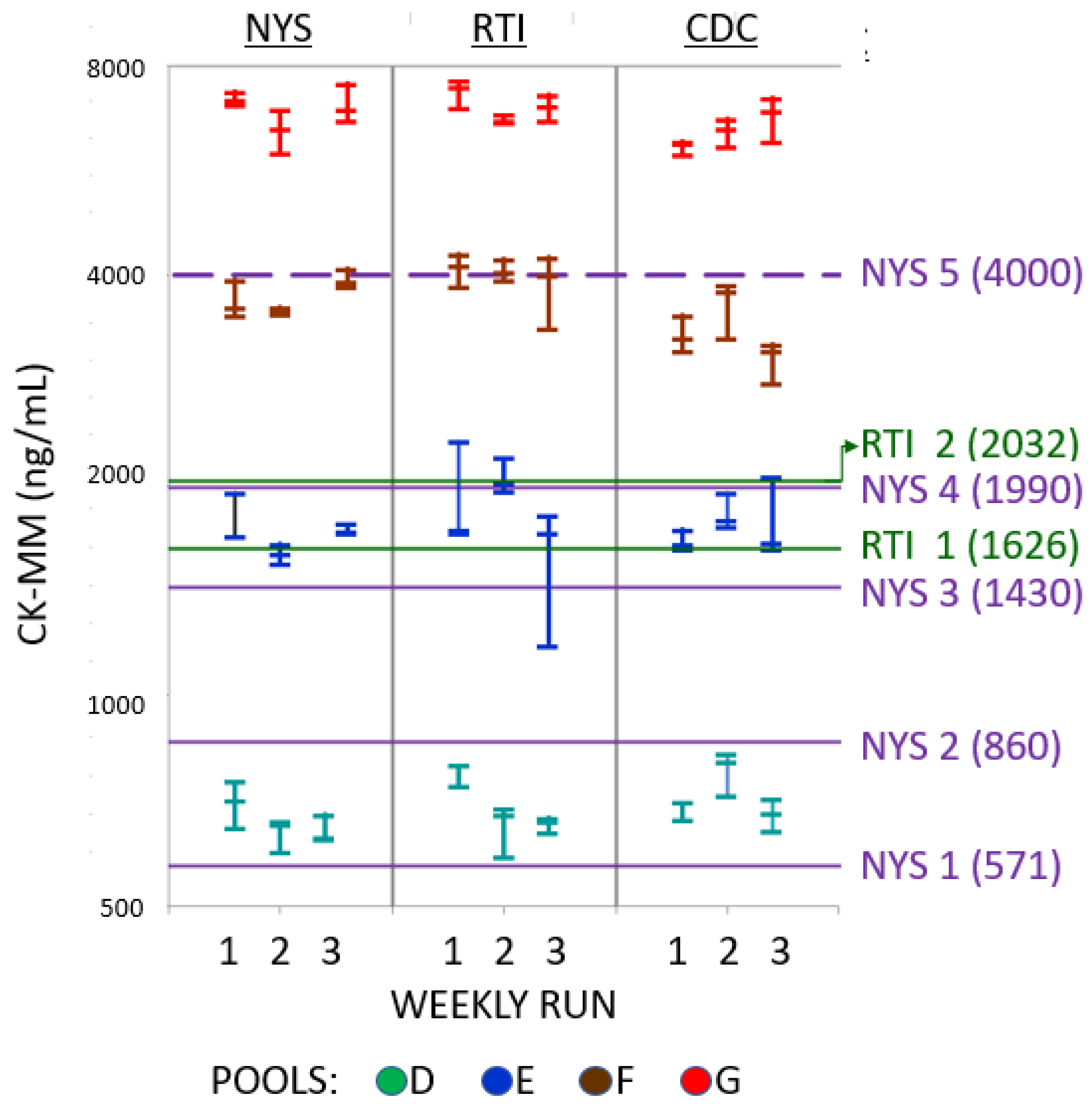
3.2. Categorical Interpretation of CK-MM Results from All Pools
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Salari, N.; Fatahi, B.; Valipour, E.; Kazeminia, M.; Fatahian, R.; Kiaei, A.; Shohaimi, S.; Mohammadi, M. Global prevalence of Duchenne and Becker muscular dystrophy: A systematic review and meta-analysis. J. Orthop. Surg. 2022, 17, 96–107. [Google Scholar] [CrossRef] [PubMed]
- Gatheridge, M.A.; Kwon, J.M.; Mendell, J.M.; Scheuerbrandt, G.; Moat, S.J.; Eyskens, F.; Rockman-Greenberg, C.; Drousiotou, A.; Griggs, R.C. Identifying Non-Duchenne Muscular Dystrophy-Positive and False Negative Results in Prior Duchenne Muscular Dystrophy Newborn Screening Programs: A Review. JAMA Neurol. 2016, 73, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Orfnos, A.P.; Naylor, E.W. A rapid screening test for Duchenne muscular dystrophy using dried blood specimens. Clin. Chim. Acta 1984, 138, 267–274. [Google Scholar] [CrossRef] [PubMed]
- Parad, R.B.; Sheldon, Y.; Bhattacharjee, A. Implementation of Hospital-Based Supplemental Duchenne Muscular Dystrophy Newborn Screening (sDMDNBS): A Pathway to Broadening Adoption. Int. J. Neonatal Screen. 2021, 7, 77. [Google Scholar] [CrossRef] [PubMed]
- Moat, S.J.; Korpimaki, T.; Furu, P.; Hakala, H.; Polari, H.; Merio, L.; Makinen, P.; Weeks, I. Characterization of a Blood Spot Creatine Kinase Skeletal Muscle Isoform Immunoassay for High-Throughput Newborn Screening of Duchenne Muscular Dystrophy. Clin. Chem. 2017, 63, 908–914. [Google Scholar] [CrossRef] [PubMed]
- Timonen, A.; Lloyd-Puryear, M.; Hougaard, D.M.; Merio, L.; Makinen, P.; Laitala, V.; Polonen, T.; Skogstrand, K.; Kennedy, A.; Airenne, S.; et al. Duchenne Muscular Dystrophy Newborn Screening: Evaluation of a New GSP R Neonatal Creatine Kinase-MM Kit in a US and Danish Population. Int. J. Neonatal Screen. 2019, 5, 27. [Google Scholar] [CrossRef] [PubMed]
- Hartnett, M.J.; Lloyd-Puryear, M.A.; Tavakoli, N.P.; Wynn, J.; Koval-Burt, C.L.; Gruber, D.; Trotter, T.; Caggana, M.; Chung, W.K.; Armstrong, N.; et al. Newborn Screening for Duchenne Muscular Dystrophy: First Year Results of a Population-Based Pilot. Int. J. Neonatal Screen. 2022, 8, 50. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Maloney, B.; Caggana, M.; Tavakoli, N.P. Creatine Kinase-MM Concentration in Dried Blood Spots from Newborns and Implications for Newborn Screening for Duchenne Muscular Dystrophy. Muscle Nerve 2022, 65, 652–658. [Google Scholar] [CrossRef] [PubMed]
- Kucera, K. Early check implementation of newborn screening for Duchenne and related muscular dystrophies in North Carolina. In Proceedings of the 2021 APHL Newborn Screening Symposium, Silver Spring, MD, USA, 5–14 October 2021. [Google Scholar]
- Ke, Q.; Zhao, Z.Y.; Griggs, R.; Wiley, V.; Connolly, A.; Kwon, J.; Qi, M.; Sheehan, D.; Ciafaloni, E.; Howell, R.R.; et al. Newborn screening for Duchenne muscular dystrophy in China: Follow-up diagnosis and subsequent treatment. World J. Pediatr. 2017, 13, 197–201. [Google Scholar] [CrossRef] [PubMed]
- Jia, X.; Jiang, X.; Huang, Y. A Pilot Study of Newborn Screening for Duchenne muscular dystrophy in Guangzhou. Heliyon. 2022, 8, e11071. [Google Scholar] [CrossRef] [PubMed]
- Jia, C.; Zhao, D.; Yanru, L.; Gao, Y.; Zhang, X.; Li, X.; Lv, S.; Li, R.; Zhu, X.; Liu, S. Newborn screening and genomic analysis of duchenne muscular dystrophy in Henan, China. Clin. Chim. Acta 2023, 539, 90–96. [Google Scholar] [CrossRef] [PubMed]
- Chien, Y.H.; Lee, N.C.; Weng, W.C.; Chen, L.C.; Huang, Y.H.; Wu, C.S.; Hwu, W.L. Duchenne muscular dystrophy newborn screening: The first 50,000 newborns screened in Taiwan. Neurolog. Sci. 2022, 43, 4563–4566. [Google Scholar] [CrossRef] [PubMed]
- CLSI. Using Proficiency Testing and Alternative Assessment to Improve Medical Laboratory Quality, 3rd ed.; CLSI guideline QMS24; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2016. [Google Scholar]
- Moat, S.J.; Bradley, D.M.; Salmon, R.; Clarke, A.; Hartley, L. Newborn bloodspot screening for Duchenne muscular dystrophy: 21 years experience in Wales (UK). Eur. J. Hum. Genet. 2013, 21, 1049–1053. [Google Scholar] [CrossRef] [PubMed]
- De Jesus, V.R.; Mei, J.V.; Cordovado, S.K.; Cuthbert, C.D. The Newborn Screening Quality Assurance Program at the Centers for Disease Control and Prevention: Thirty-five Year Experience Assuring Newborn Screening Laboratory Quality. Int. J. Neonatal Screen. 2015, 1, 13–26. [Google Scholar] [CrossRef] [PubMed]
- Hall, K. 12th ISNS European Regional Meeting Oral and Poster Abstracts. Int. J. Neonatal Screen. 2021, 7, 71. [Google Scholar] [CrossRef] [PubMed]
- Divisi, D.; Di Leonardo, G.; Zaccagna, G.; Crisci, R. Basic statistics with Microsoft Excel: A review. J. Thorac. Dis. 2017, 9, 1734–1740. [Google Scholar] [CrossRef] [PubMed]
- Thomas, S.; Conway, K.M.; Fapo, O.; Street, N.; Mathews, K.D.; Mann, J.R.; Romitti, P.A.; Soim, A.; Westfield, C.; Fox, D.J.; et al. Time to diagnosis of Duchenne muscular dystrophy remains unchanged: Findings from the Muscular Dystrophy Surveillance, Tracking, and Research Network, 2000–2015. Muscle Nerve 2022, 66, 193–197. [Google Scholar] [CrossRef] [PubMed]
- Migliore, B.A.; Zhou, L.; Duparc, M.; Robles, V.R.; Rehder, C.W.; Peay, H.L.; Kucera, K.S. Evaluation of the GSP Creatine Kinase-MM Assay and Assessment of CK-MM Stability in Newborn, Patient, and Contrived Dried Blood Spots for Newborn Screening for Duchenne Muscular Dystrophy. Int. J. Neonatal Screen. 2022, 8, 12. [Google Scholar] [CrossRef] [PubMed]
- Rudolph, N.; Gross, R.T. Creatine phosphokinase activity in serum of newborn infants as an indicator of fetal trauma during birth. Pediatrics 1966, 38, 1039–1046. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Pool | %Pool A | Pool G | Target CK-MM Conc (ng/mL) |
|---|---|---|---|
| A | 100 | 0 | 0 |
| B | 99 | 1 | 50 |
| C | 97 | 3 | 150 |
| D | 90 | 10 | 500 |
| E | 75 | 25 | 1250 |
| F | 50 | 50 | 2500 |
| G | 0 | 100 | 5000 |
| Pool | A | B | C | D | E | F | G | |
|---|---|---|---|---|---|---|---|---|
| Mean | 3.51 | 62.4 | 185 | 689 | 1846 | 4007 | 6992 | |
| SD | 1.48 | 3.8 | 9 | 63 | 331 | 283 | 363 | |
| RTI | CV (%) | 42 | 6 | 5 | 9 | 18 | 7 | 5 |
| Min. | 1.36 | 58 | 174 | 588 | 1178 | 3362 | 6618 | |
| Max. | 5.33 | 68 | 199 | 795 | 2313 | 4285 | 7584 | |
| Mean | 5.07 | 68.2 | 201 | 661 | 1701 | 3730 | 6887 | |
| SD | 0.98 | 5.4 | 17 | 48 | 116 | 219 | 466 | |
| NYS | CV (%) | 19 | 8 | 8 | 7 | 7 | 6 | 7 |
| Min. | 3.62 | 62.1 | 177 | 597 | 1541 | 3494 | 5984 | |
| Max. | 6.08 | 80.7 | 233 | 755 | 1954 | 4087 | 7537 | |
| Mean | 3.94 | 79 | 220 | 717 | 1757 | 3319 | 6432 | |
| SD | 2.17 | 5.4 | 19 | 61 | 153 | 343 | 404 | |
| CDC | CV (%) | 55 | 7 | 8 | 9 | 9 | 10 | 6 |
| Min. | 1.07 | 70.8 | 189 | 640 | 1618 | 2800 | 5957 | |
| Max. | 6.91 | 89.3 | 248 | 825 | 2053 | 3863 | 7181 | |
| Mean | 4.17 | 69.9 | 202 | 689 | 1768 | 3685 | 6771 | |
| SD | 1.32 | 4.2 | 12 | 61 | 285 | 330 | 369 | |
| All labs | CV (%) | 41 | 12 | 10 | 9 | 12 | 11 | 7 |
| Min. | 1.07 | 58 | 174 | 588 | 1178 | 2800 | 5957 | |
| Max. | 6.91 | 89.3 | 248 | 825 | 2313 | 4285 | 7584 |
| NBS Program | Newborn Population | Cutoff (ng/mL) | Reference |
|---|---|---|---|
| New York State Department of Health | ≥168 h 72–167 h 48–71 h ≤47 h | 571 (R) 571 (B) 860 (R) 1430 (B) 4000 (R) 1990 (B) 4000 (R) | [8] Park et al. 2022 |
| Early Check Program, RTI International | ≤72 h (Provisional) ≤72 h (Refined) | 1626 2032 | [9] Kucera 2021 |
| Supplemental Duchenne Muscular Dystrophy Newborn Screening | Males 24–48 h Females 24–48 h | 1080 958 | [4] Parad et al. 2021 |
| California/Denmark Population Study | US 12–60 h Danish ≥ 48 h | 1190 675 | [6] Timonen et al. 2018 |
| National Taiwan University Hospital | All Newborns (Mean Age 2 Days) | 750 | [13] Chien et al. 2022 |
| Zhejiang Province China | Males 3–5 days | 700 | [10] Ke et al. 2017 |
| Guangzhou City China | Males and Females 48 h to 7 days | 800 | [11] Jia et al. 2022 |
| Henan Province China | Males 48–72 h | 472 | [12] Jia et al. 2023 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dantonio, P.; Tavakoli, N.P.; Migliore, B.; McCown, E.; Lim, T.; Park, S.; Caggana, M.; Kucera, K.S.; Phan, H.; Street, N.; et al. Multi-Laboratory Evaluation of Prototype Dried Blood Spot Quality Control Materials for Creatine Kinase-MM Newborn Screening Assays. Int. J. Neonatal Screen. 2023, 9, 13. https://doi.org/10.3390/ijns9010013
Dantonio P, Tavakoli NP, Migliore B, McCown E, Lim T, Park S, Caggana M, Kucera KS, Phan H, Street N, et al. Multi-Laboratory Evaluation of Prototype Dried Blood Spot Quality Control Materials for Creatine Kinase-MM Newborn Screening Assays. International Journal of Neonatal Screening. 2023; 9(1):13. https://doi.org/10.3390/ijns9010013
Chicago/Turabian StyleDantonio, Paul, Norma P. Tavakoli, Brooke Migliore, Elizabeth McCown, Timothy Lim, Sunju Park, Michele Caggana, Katerina S. Kucera, Han Phan, Natalie Street, and et al. 2023. "Multi-Laboratory Evaluation of Prototype Dried Blood Spot Quality Control Materials for Creatine Kinase-MM Newborn Screening Assays" International Journal of Neonatal Screening 9, no. 1: 13. https://doi.org/10.3390/ijns9010013
APA StyleDantonio, P., Tavakoli, N. P., Migliore, B., McCown, E., Lim, T., Park, S., Caggana, M., Kucera, K. S., Phan, H., Street, N., Petritis, K., & Vogt, R. F. (2023). Multi-Laboratory Evaluation of Prototype Dried Blood Spot Quality Control Materials for Creatine Kinase-MM Newborn Screening Assays. International Journal of Neonatal Screening, 9(1), 13. https://doi.org/10.3390/ijns9010013