The Early History of PKU


{kind=link}
Abstract
1. Introduction
2. The Cause of Mental Retardation in PKU
3. First Ideas of a Phenylalanine-Restricted Diet
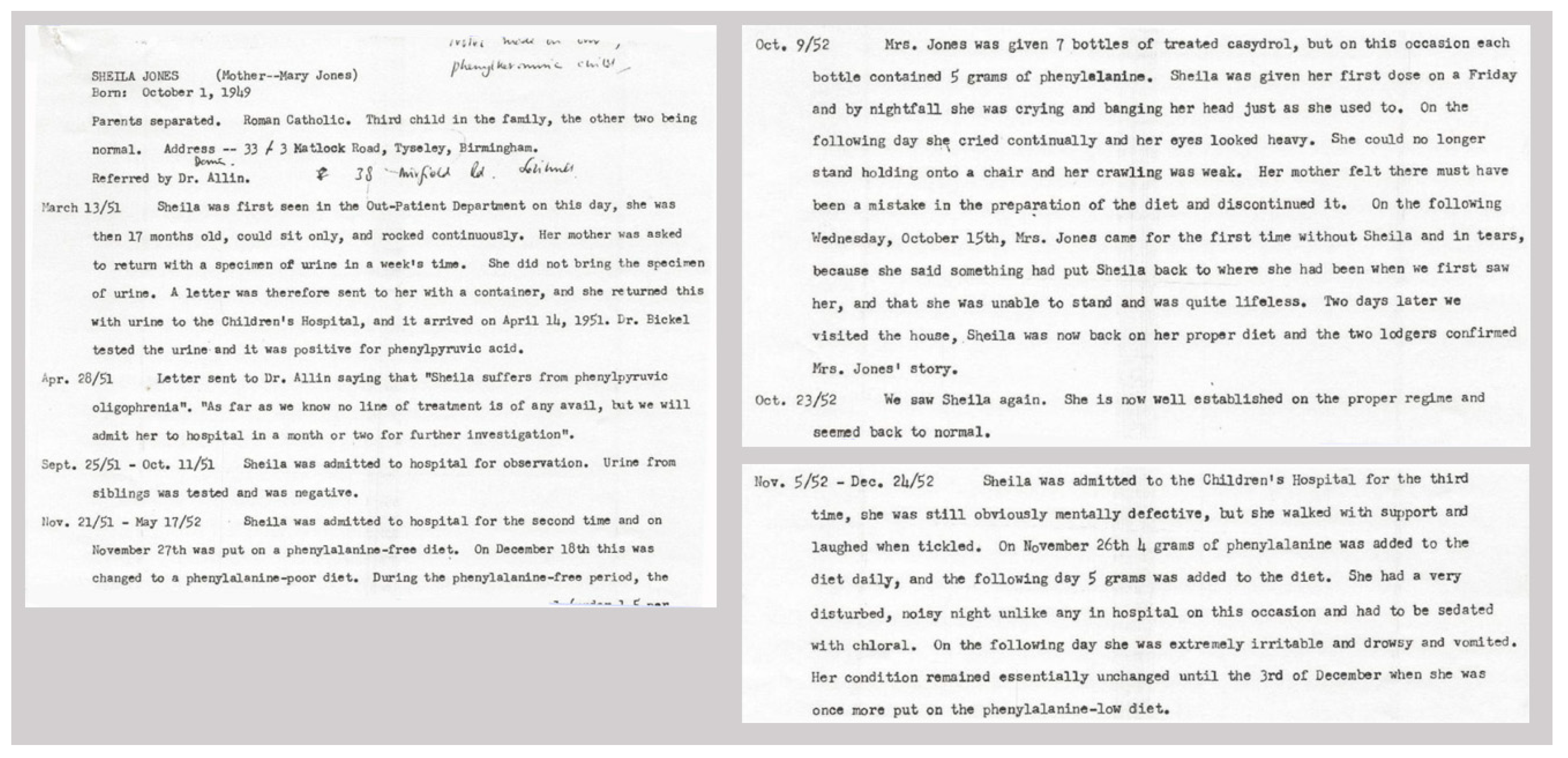
4. First Trials with a Phenylalanine-Restricted Diet
5. From Early Treatment to Newborn Screening
Funding
Conflicts of Interest
References
- Følling, A. Excretion of phenylpyruvic acid in urine as a metabolicnomaly in connection with imbecility. Nord. Med. Tidskr. 1934, 8, 1054–1059. [Google Scholar]
- Christ, S.E. Asbjørn Følling and the discovery of Phenylketonuria. J. Hist. Neurosci. 2003, 12, 44–54. [Google Scholar] [CrossRef] [PubMed]
- Centerwall, S.A.; Centerwall, W.R. The discovery of Phenylketonuria: The story of a young couple, two retarded children, and a scientist. Pediatrics 2000, 105, 89–103. [Google Scholar] [CrossRef] [PubMed]
- Jervis, G.A. Excretion of phenylalanine and derivatives in phenylpyruvic oligophrenia. Proc. Soc. Exp. Biol. Med. 1950, 75, 83–86. [Google Scholar] [CrossRef] [PubMed]
- Borek, E.; Brecher, A.; Jervis, G.A.; Waelsch, H. Oligophrenia phenylpyruvica. II. Constancy of the metabolic error. Proc. Soc. Exp. Biol. Med. 1950, 75, 86–89. [Google Scholar] [CrossRef] [PubMed]
- Gramer, G.; Haege, G.; Fang-Hoffmann, J.; Hoffmann, G.F.; Bartram, C.R.; Hinderhofer, K.; Burgard, P.; Lindner, M. Medium-Chain Acyl-CoA Dehydrogenase Deficiency: Evaluation of Genotype-Phenotype Correlation in Patients Detected by Newborn Screening. JIMD Rep. 2015, 23, 101–112. [Google Scholar] [PubMed]
- Laxova, R. Lionel Sharpless Penrose, 1898-1972: A Personal Memoir in Celebration of the Centenary of his birth. Genetics 1998, 150, 1333–1340. [Google Scholar] [PubMed]
- Woolf, L.I.; Vulliamy, D.G. Phenylketonuria with a study of the effect upon it of glutamic acid. Arch. Dis. Child. 1951, 26, 487–494. [Google Scholar] [CrossRef] [PubMed]
- Bickel, H.; Gerrard, J.; Hickmans, E.M. The influence of phenylalanine intake on phenylketonuria. Lancet 1953, 17, 812–813. [Google Scholar] [CrossRef]
- Woolf, L.I.; Griffiths, R.; Moncrieff, A. Treatment of phenylketonuria with a diet low in phenylalanine. Br. Med. J. 1955, 1, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Alonso-Fernández, J.R.; Colón, C. The contribution of Louis I. Woolf to the treatment, early diagnosis and understanding of phenylketonuria. J. Med. Sceen. 2009, 16, 205–211. [Google Scholar]
- Armstrong, M.D.; Tyler, F.H. Studies on phenylketonuria. I. Restricted phenylalanine intake in phenylketonuria. J. Clin. Investig. 1955, 34, 565–580. [Google Scholar] [CrossRef] [PubMed]
- Woolf, L.I.; Griffiths, R.; Moncrieff, A.; Coates, S.; Dillistone, F. The dietary treatment of phenylketonuria. Arch. Dis. Child. 1958, 33, 31–45. [Google Scholar] [CrossRef] [PubMed]
- Woolf, L.I. Tests for phenylketonuria. Dev. Med. Child Neurol. 1961, 3, 249–254. [Google Scholar] [CrossRef] [PubMed]
- Berry, H.K.; Sutherland, B.; Guest, G.M.; Warkany, J. Simple method for detection of phenylketonuria. J. Am. Med. Assoc. 1958, 167, 2185–2190. [Google Scholar] [CrossRef] [PubMed]
- Guthrie, R.; Susi, A. A simple phenylalanine method for the detection of phenylketonuria in large populations of newborn infants. Pediatrics 1963, 32, 338–343. [Google Scholar] [PubMed]

© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Woolf, L.I.; Adams, J. The Early History of PKU. Int. J. Neonatal Screen. 2020, 6, 59. https://doi.org/10.3390/ijns6030059
Woolf LI, Adams J. The Early History of PKU. International Journal of Neonatal Screening. 2020; 6(3):59. https://doi.org/10.3390/ijns6030059
Chicago/Turabian StyleWoolf, Louis I., and John Adams. 2020. "The Early History of PKU" International Journal of Neonatal Screening 6, no. 3: 59. https://doi.org/10.3390/ijns6030059
APA StyleWoolf, L. I., & Adams, J. (2020). The Early History of PKU. International Journal of Neonatal Screening, 6(3), 59. https://doi.org/10.3390/ijns6030059