
Newborn Screening for Congenital Heart Disease: A Five-Year Study in Shanghai

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Procedures
2.3. Data Source
2.4. Defining Outcomes
2.5. Statistical Analyses
3. Results
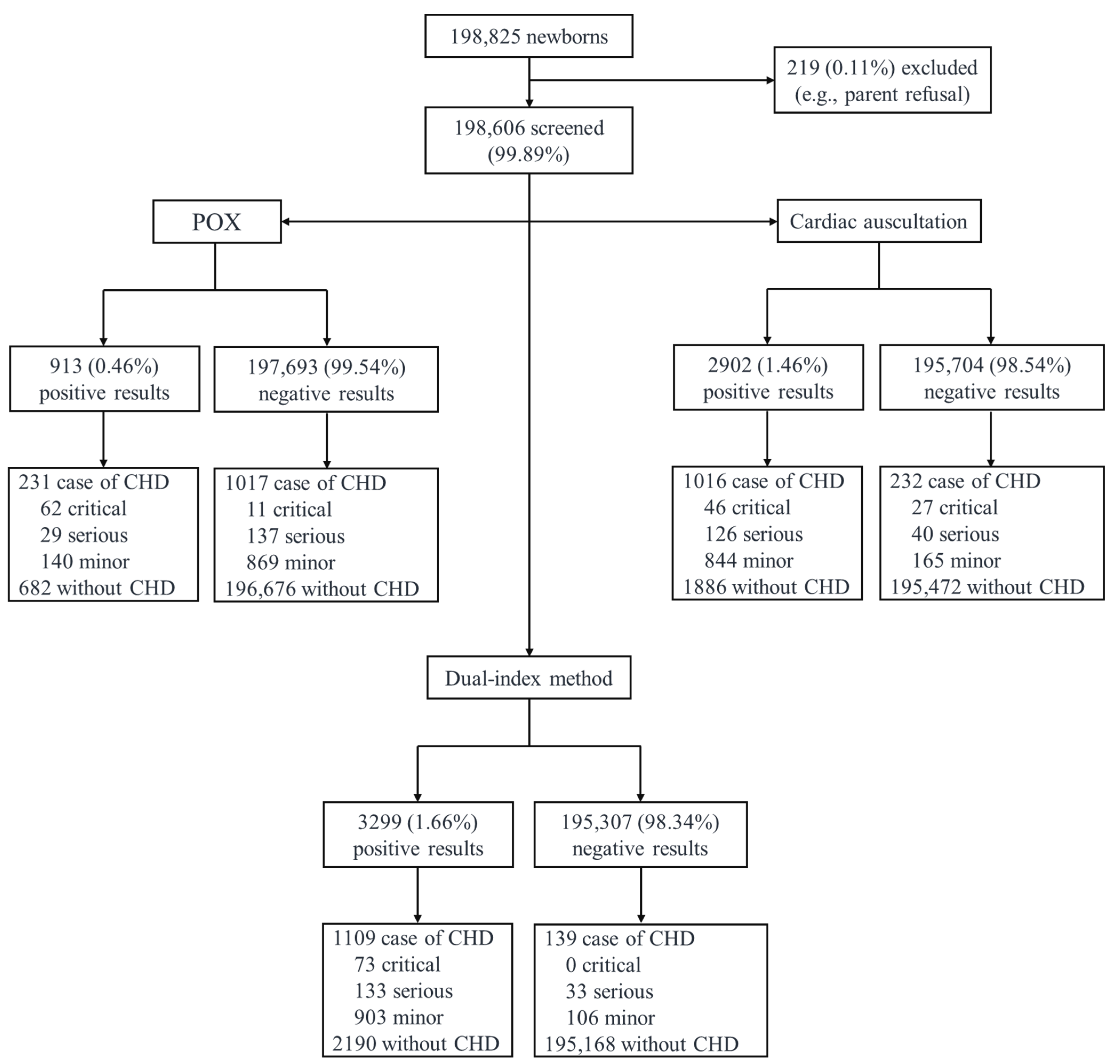
3.1. Results of Newborn Screening for CHD in South Shanghai
3.2. CHD in Infants with Negative Screening Results of the Dual-Index Method
3.3. Accuracy of Screening Methods for CCHD and Life-Threatening Major CHD
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CHD | Congenital heart disease |
| POX | Pulse oximetry |
| CCHD | Critical congenital heart disease |
| NICU | Neonatal intensive care unit |
| SpO2 | Pulse oximeter oxygen saturation |
| ASD | Atrial septal defect |
References
- Thoracic and Cardiovascular Surgery Branch of Chinese Medical Association. National consensus in China on perinatal diagnosis, evaluation and clinical disposal of cardiac birth defects. Chin. J. Pediatr. Surg. 2018, 39, 163–170. (In Chinese) [Google Scholar] [CrossRef]
- Tian, Y.; Hu, X.; Gu, Q.; Yang, M.; Jia, P.; Ma, X.; Ge, X.; Zhao, Q.; Liu, F.; Ye, M.; et al. Temporal trend in mortality due to congenital heart disease in China from 2008 to 2021. Chin. Med. J. 2025, 138, 693–701. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Q.M.; Liu, F.; Wu, L.; Ma, X.J.; Niu, C.; Huang, G.Y. Prevalence of Congenital Heart Disease at Live Birth in China. J. Pediatr. 2019, 204, 53–58. [Google Scholar] [CrossRef]
- Brown, K.L.; Ridout, D.A.; Hoskote, A.; Verhulst, L.; Ricci, M.; Bull, C. Delayed diagnosis of congenital heart disease worsens preoperative condition and outcome of surgery in neonates. Heart 2006, 92, 1298–1302. [Google Scholar] [CrossRef]
- Liberman, R.F.; Getz, K.D.; Lin, A.E.; Higgins, C.A.; Sekhavat, S.; Markenson, G.R.; Anderka, M. Delayed Diagnosis of Critical Congenital Heart Defects: Trends and Associated Factors. Pediatrics 2014, 134, E373–E381. [Google Scholar] [CrossRef]
- Plana, M.N.; Zamora, J.; Suresh, G.; Fernandez-Pineda, L.; Thangaratinam, S.; Ewer, A.K. Pulse oximetry screening for critical congenital heart defects. Cochrane Database Syst. Rev. 2018, 3, CD011912. [Google Scholar] [CrossRef] [PubMed]
- Abouk, R.; Grosse, S.D.; Ailes, E.C.; Oster, M.E. Association of US State Implementation of Newborn Screening Policies for Critical Congenital Heart Disease with Early Infant Cardiac Deaths. JAMA-J. Am. Med. Assoc. 2017, 318, 2111–2118. [Google Scholar] [CrossRef]
- Zhao, Q.M.; Ma, X.J.; Ge, X.L.; Liu, F.; Yan, W.L.; Wu, L.; Ye, M.; Liang, X.C.; Zhang, J.; Gao, Y.; et al. Pulse oximetry with clinical assessment to screen for congenital heart disease in neonates in China: A prospective study. Lancet 2014, 384, 747–754. [Google Scholar] [CrossRef]
- Hu, X.J.; Ma, X.J.; Zhao, Q.M.; Yan, W.L.; Ge, X.L.; Jia, B.; Liu, F.; Wu, L.; Ye, M.; Liang, X.C.; et al. Pulse Oximetry and Auscultation for Congenital Heart Disease Detection. Pediatrics 2017, 140, e20171154. [Google Scholar] [CrossRef]
- Ma, X.J.; Tian, Y.P.; Ma, F.C.; Ge, X.L.; Gu, Q.; Huang, M.; Zhang, Y.Q.; Sun, K.; Hu, X.J.; Yang, M.; et al. Impact of Newborn Screening Programme for Congenital Heart Disease in Shanghai: A five-year observational study in 801,831 newborns. Lancet Reg. Health-West. Pac. 2023, 33, 100688. [Google Scholar] [CrossRef]
- Zhou, F.Y.; Li, C.; Qin, K.Z.; Luo, C.; Huang, H.F.; Wu, Y.T. Delivery and neonatal outcomes of pregnant women during the Shanghai lockdown: A retrospective analysis. Front. Pediatr. 2023, 11, 992908. [Google Scholar] [CrossRef] [PubMed]
- Deng, H.M.; Jin, Y.P.; Sheng, M.M.; Liu, M.; Shen, J.; Qian, W.; Zou, G.; Liao, Y.X.; Liu, T.F.; Ling, Y.; et al. Safety and efficacy of COVID-19 vaccine immunization during pregnancy in 1024 pregnant women infected with the SARS-CoV-2 Omicron virus in Shanghai, China. Front. Immunol. 2024, 14, 1303058. [Google Scholar] [CrossRef]
- Ewer, A.K.; Middleton, L.J.; Furmston, A.T.; Bhoyar, A.; Daniels, J.P.; Thangaratinam, S.; Deeks, J.J.; Khan, K.S.; Grp, P.S. Pulse oximetry screening for congenital heart defects in newborn infants (PulseOx): A test accuracy study. Lancet 2011, 378, 785–794. [Google Scholar] [CrossRef]
- Sun, S.Y.; Xie, Z.; Yu, K.T.; Jiang, B.Q.; Zheng, S.W.; Pan, X.T. COVID-19 and healthcare system in China: Challenges and progression for a sustainable future. Glob. Health 2021, 17, 14. [Google Scholar] [CrossRef] [PubMed]
- Singh, Y.; Chen, S.E. Impact of pulse oximetry screening to detect congenital heart defects: 5 years’ experience in a UK regional neonatal unit. Eur. J. Pediatr. 2022, 181, 813–821. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.H.; Sun, Y.; Zhu, J.J.; Zhu, Y.N.; Qiu, L.Q. Epidemiology, prenatal diagnosis, and neonatal outcomes of congenital heart defects in eastern China: A hospital-based multicenter study. BMC Pediatr. 2020, 20, 416. [Google Scholar] [CrossRef]
- Li, M.; Ye, B.; Chen, Y.; Gao, L.; Wu, Y.; Cheng, W. Analysis of genetic testing in fetuses with congenital heart disease of single atria and/or single ventricle in a Chinese prenatal cohort. BMC Pediatr. 2023, 23, 577. [Google Scholar] [CrossRef]
- Tomek, V.; Jicinska, H.; Pavlicek, J.; Kovanda, J.; Jehlicka, P.; Klaskova, E.; Mrazek, J.; Cutka, D.; Smetanova, D.; Brestak, M.; et al. Pregnancy Termination and Postnatal Major Congenital Heart Defect Prevalence After Introduction of Prenatal Cardiac Screening. JAMA Netw. Open 2023, 6, e2334069. [Google Scholar] [CrossRef]
- Liu, Y.J.; Chen, S.; Zühlke, L.; Black, G.C.; Choy, M.K.; Li, N.X.; Keavney, B.D. Global birth prevalence of congenital heart defects 1970-2017: Updated systematic review and meta-analysis of 260 studies. Int. J. Epidemiol. 2019, 48, 455–463. [Google Scholar] [CrossRef]
- Abbas, A.; Ewer, A.K. New born pulse oximetry screening: A global perspective. Early Hum. Dev. 2021, 162, 105457. [Google Scholar] [CrossRef]
- Ailes, E.C.; Gilboa, S.M.; Honein, M.A.; Oster, M.E. Estimated Number of Infants Detected and Missed by Critical Congenital Heart Defect Screening. Pediatrics 2015, 135, 1000–1008. [Google Scholar] [CrossRef] [PubMed]
- Oddie, S.; Stenson, B.; Wyllie, J.; Ewer, A.K. UK consultation on pulse oximetry screening for critical congenital heart defects in newborns. Lancet 2019, 394, 103–104. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| District | Number of Newborns | Number of Newborns Screened | Screening Rate (%) | Number of Newborns Screened Positive | Screened Positive Rate (%) | Number of Echocardiography in Newborns Screened Positive | Echocardiography Examination Rate (%) | Number of Diagnosed CHD in Those Screened Positive | Diagnostic Rate of CHD in Newborns Screened Positive (%) | Number of False-Negative Cases | CHD Cases | Prevalence of CHD (‰) | Number of Treatments |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Xuhui | 84,884 | 84,783 | 99.88 | 1210 | 1.43 | 1103 | 91.16 | 463 | 38.26 | 26 | 489 | 5.76 | 60 |
| Qingpu | 10,304 | 10,301 | 99.97 | 193 | 1.87 | 180 | 93.26 | 56 | 29.02 | 4 | 60 | 5.82 | 15 |
| Jinshan | 17,925 | 17,891 | 99.81 | 459 | 2.57 | 420 | 91.50 | 110 | 23.97 | 27 | 137 | 7.64 | 27 |
| Minhang | 34,262 | 34,235 | 99.92 | 547 | 1.60 | 527 | 96.34 | 220 | 40.22 | 41 | 261 | 7.62 | 37 |
| Songjiang | 51,450 | 51,396 | 99.90 | 890 | 1.73 | 813 | 91.35 | 260 | 29.21 | 41 | 301 | 5.85 | 63 |
| Total | 198,825 | 198,606 | 99.89 | 3299 | 1.66 | 3043 | 92.24 | 1109 | 33.62 | 139 | 1248 | 6.28 | 202 |
| CHD in Infants with Positive Screening Results | CHD in Infants with Negative Screening Results | ||
|---|---|---|---|
| Critical CHD (N = 73) | Serious CHD (N = 33) | ||
| Pulmonary atresia | 20 | Patent ductus arteriosus | 17 |
| Total anomalous pulmonary venous drainage | 16 | Ventricular septal defect | 12 |
| Coarctation of the aorta | 11 | Atrioventricular septal defect | 1 |
| Transposition of the great arteries | 10 | Coarctation of the aorta | 1 |
| Critical pulmonary stenosis | 7 | Cor triatriatum | 1 |
| Interrupted aortic arch | 3 | Partial anomalous pulmonary venous connection | 1 |
| Double outlet right ventricle | 2 | ||
| Hypoplastic left heart syndrome | 2 | ||
| Single ventricle | 2 | ||
| Serious CHD (N = 133) | |||
| Ventricular septal defect | 71 | ||
| Tetralogy of Fallot | 20 | ||
| Pulmonary stenosis | 18 | ||
| Patent ductus arteriosus | 15 | ||
| Atrioventricular septal defect | 6 | ||
| Coarctation of the aorta | 2 | ||
| Partial anomalous pulmonary venous connection | 1 | ||
| CCHD | Major CHD | All Type of CHD | ||||
|---|---|---|---|---|---|---|
| POX Alone | Dual-Index Method | POX Alone | Dual-Index Method | POX Alone | Dual-Index Method | |
| True-positives | 62 | 73 | 91 | 206 | 231 | 1109 |
| False-negatives | 11 | 0 | 148 | 33 | 1017 | 139 |
| False-positives | 851 | 3226 | 822 | 3093 | 682 | 2190 |
| True-negatives | 197,682 | 195,307 | 197,545 | 195,274 | 196,676 | 195,168 |
| False-positive rate (%) | 0.43 | 1.62 | 0.41 | 1.56 | 0.34 | 1.11 |
| Sensitivity (%) | 84.93 (75.00, 91.37) | 100.00 (95.00, 100.00) * | 38.08 (32.15, 44.37) | 86.19 (81.24, 90.00) * | 18.51 (16.45, 20.76) | 88.86 (87.00, 90.49) * |
| Specificity (%) | 99.57 (99.54, 99.60) | 98.38 (98.32, 98.43) | 99.59 (99.56, 99.61) | 98.44 (98.39, 98.49) | 99.65 (99.63, 99.68) | 98.89 (98.84, 98.94) |
| Positive predictive value (%) | 6.79 (5.33, 8.61) | 2.21 (1.76, 2.77) | 9.97 (8.19, 12.08) | 6.24 (5.47, 7.12) | 25.30 (22.59, 28.22) | 33.62 (32.02, 35.25) |
| Negative predictive value (%) | 99.99 (99.99, 100.00) | 100.00 (100.00, 100.00) | 99.93 (99.91, 99.94) | 99.98 (99.98, 99.99) | 99.49 (99.45, 99.52) | 99.93 (99.92, 99.94) |
| Consistency rate (%) | 99.57 (99.54, 99.59) | 98.38 (98.32, 98.43) | 99.51 (99.48, 99.54) | 98.43 (98.37, 98.48) | 99.14 (99.1, 99.18) | 98.83 (98.78, 98.87) |
| Youden’s index | 0.85 | 0.98 | 0.38 | 0.85 | 0.18 | 0.88 |
| Positive likelihood ratio | 197.91 | 61.54 | 91.88 | 55.28 | 53.56 | 80.08 |
| Negative likelihood ratio | 15.13 | 0.00 | 62.18 | 14.03 | 81.77 | 11.26 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the International Society for Neonatal Screening. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tian, Y.; Gu, Q.; Hu, X.; Ge, X.; Ma, X.; Yang, M.; Jia, P.; Zhang, J.; Yang, L.; Zhao, Q.; et al. Newborn Screening for Congenital Heart Disease: A Five-Year Study in Shanghai. Int. J. Neonatal Screen. 2025, 11, 38. https://doi.org/10.3390/ijns11020038
Tian Y, Gu Q, Hu X, Ge X, Ma X, Yang M, Jia P, Zhang J, Yang L, Zhao Q, et al. Newborn Screening for Congenital Heart Disease: A Five-Year Study in Shanghai. International Journal of Neonatal Screening. 2025; 11(2):38. https://doi.org/10.3390/ijns11020038
Chicago/Turabian StyleTian, Youping, Qing Gu, Xiaojing Hu, Xiaoling Ge, Xiaojing Ma, Miao Yang, Pin Jia, Jing Zhang, Lulu Yang, Quming Zhao, and et al. 2025. "Newborn Screening for Congenital Heart Disease: A Five-Year Study in Shanghai" International Journal of Neonatal Screening 11, no. 2: 38. https://doi.org/10.3390/ijns11020038
APA StyleTian, Y., Gu, Q., Hu, X., Ge, X., Ma, X., Yang, M., Jia, P., Zhang, J., Yang, L., Zhao, Q., Liu, F., Ye, M., Yang, Y., & Huang, G. (2025). Newborn Screening for Congenital Heart Disease: A Five-Year Study in Shanghai. International Journal of Neonatal Screening, 11(2), 38. https://doi.org/10.3390/ijns11020038