
Long-Term Follow-Up Cares and Check Initiative: A Program to Advance Long-Term Follow-Up in Newborns Identified with a Disease through Newborn Screening

 ,
,  , , , ,
, , , , 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Methods
2.1. Use Case
2.2. Program Goals
- Engage parents and families living with newborns, children, and adults with SMA to identify LTFU themes to prioritize for SMA;
- Design, implement, and evaluate data collection with input from at least five pediatric neurologists caring for NBS-identified SMA cases;
- Connect the clinical site with their respective state NBS program to foster LTFU collaboration;
- Design, implement, and evaluate data dashboards designed for clinical sites and state NBS programs;
- Design and disseminate LTFU data points that are important for the LTFU of SMA to all state NBS programs in the US;
- Increase the number of infants, children, and families who receive coordinated LTFU care through a medical home by 20 percent from baseline.
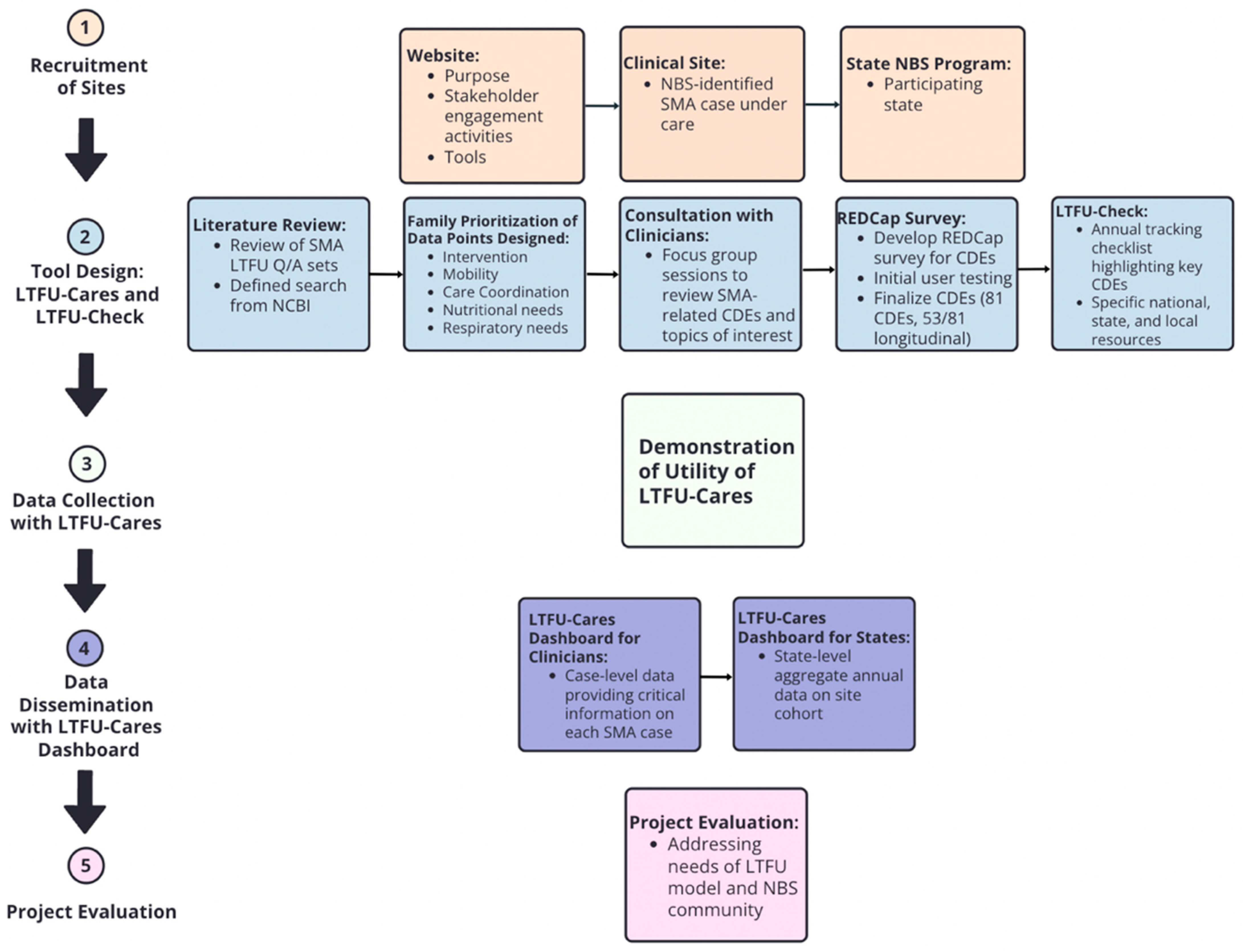
2.3. Workflow
- Recruitment of Sites
- Website
- Clinical Sites
- State NBS Programs
- 2.
- Tool Design
- Literature Review
- Family Prioritization of Data Points
- Consultation with Clinicians
- LTFU-Cares Using REDCap®
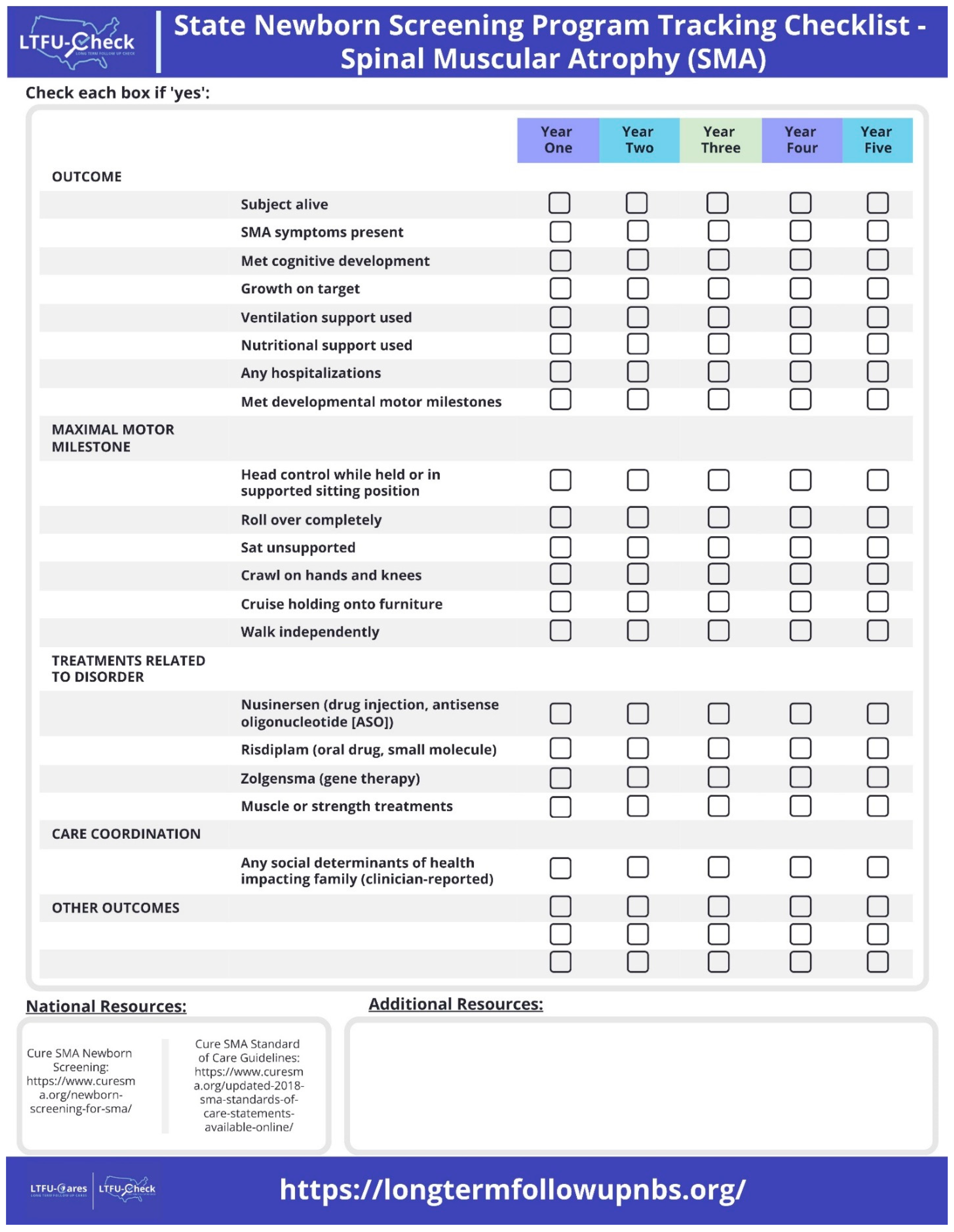
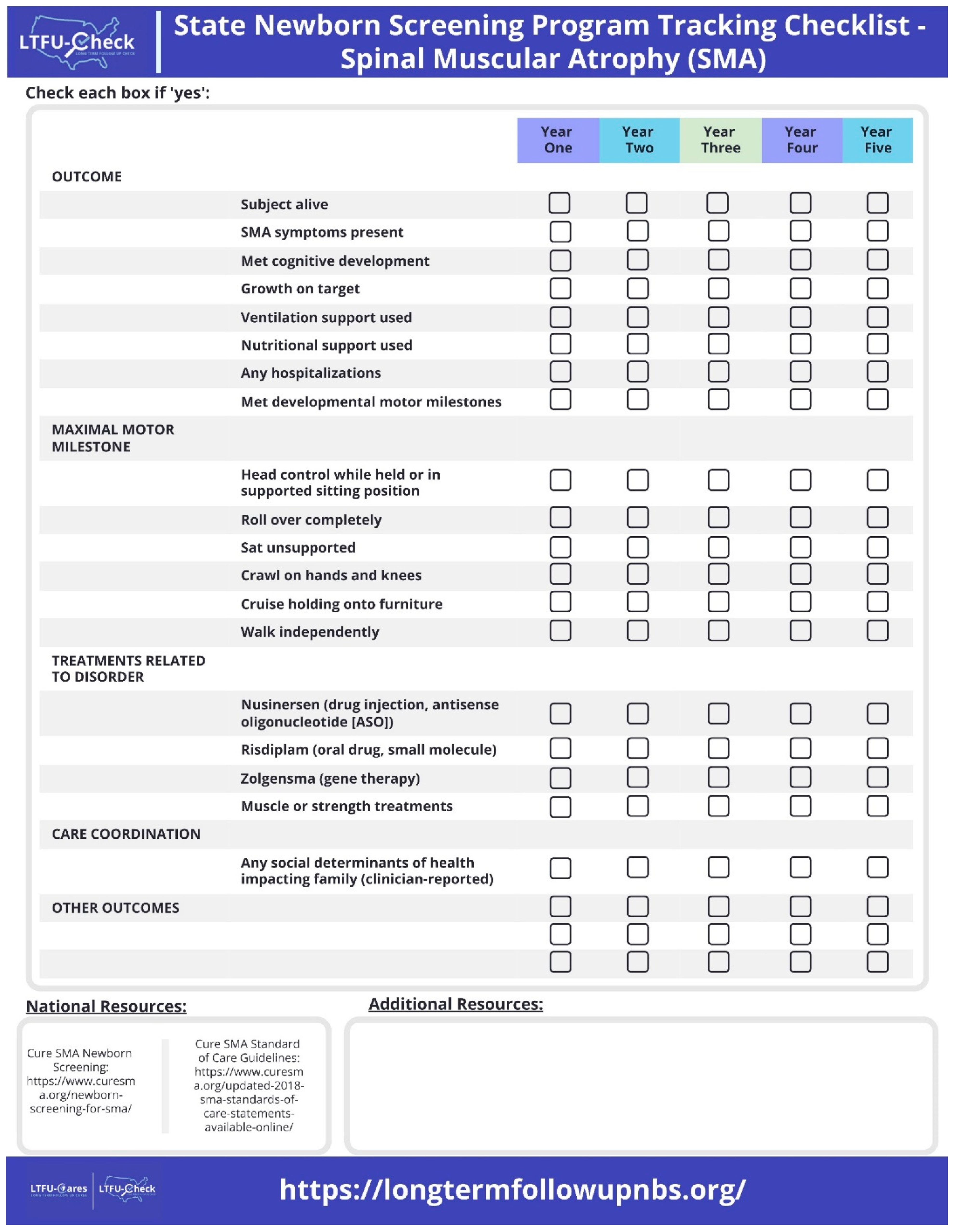
- LTFU-Check
- 3.
- Data Collection using LTFU-Cares
- 4.
- Data Dissemination with LTFU-Cares Dashboard
- 5.
- Project Evaluation
3. Preliminary Results
3.1. Recruitment of Sites
3.1.1. Website
3.1.2. Clinical Sites
3.1.3. State NBS Programs
3.2. Tool Design
3.2.1. Parent and Family Engagement
3.2.2. LTFU-Cares Data Collection
3.2.3. LTFU-Cares Data Dashboard
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Motyl, A.A.L.; Gillingwater, T.H. Timing Is Everything: Clinical Evidence Supports Pre-Symptomatic Treatment for Spinal Muscular Atrophy. Cell Rep. Med. 2022, 3, 100725. [Google Scholar] [CrossRef] [PubMed]
- Brower, A.; Chan, K.; Williams, M.; Berry, S.; Currier, R.; Rinaldo, P.; Caggana, M.; Gaviglio, A.; Wilcox, W.; Steiner, R.; et al. Population-Based Screening of Newborns: Findings from the NBS Expansion Study (Part One). Front. Genet. 2022, 13, 867337. [Google Scholar] [CrossRef] [PubMed]
- The United Nations. Convention on the Rights of the Child; UN General Assembly: New York, NY, USA, 1989. [Google Scholar]
- Describing SMA—Cure SMA. Available online: https://www.curesma.org/describing-sma/ (accessed on 1 February 2024).
- Lee, B.H.; Waldrop, M.A.; Connolly, A.M.; Ciafaloni, E. Time Is Muscle: A Recommendation for Early Treatment for Preterm Infants with Spinal Muscular Atrophy. Muscle Nerve 2021, 64, 153–155. [Google Scholar] [CrossRef] [PubMed]
- Osterman, M.; Hamilton, B.; Martin, J.; Driscoll, A.; Valenzuela, C. Births: Final Data for 2020; National Center for Health Statistics (U.S.): Hyattsville, MA, USA, 2021. [CrossRef]
- Al-Zaidy, S.; Pickard, A.S.; Kotha, K.; Alfano, L.N.; Lowes, L.; Paul, G.; Church, K.; Lehman, K.; Sproule, D.M.; Dabbous, O.; et al. Health Outcomes in Spinal Muscular Atrophy Type 1 Following AVXS-101 Gene Replacement Therapy. Pediatr. Pulmonol. 2019, 54, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Aslesh, T.; Yokota, T. Restoring SMN Expression: An Overview of the Therapeutic Developments for the Treatment of Spinal Muscular Atrophy. Cells 2022, 11, 417. [Google Scholar] [CrossRef] [PubMed]
- Butterfield, R.J. Spinal Muscular Atrophy Treatments, Newborn Screening, and the Creation of a Neurogenetics Urgency. Semin. Pediatr. Neurol. 2021, 38, 100899. [Google Scholar] [CrossRef] [PubMed]
- Corsello, A.; Scatigno, L.; Pascuzzi, M.C.; Calcaterra, V.; Dilillo, D.; Vizzuso, S.; Pelizzo, G.; Zoia, E.; Mandelli, A.; Govoni, A.; et al. Nutritional, Gastrointestinal and Endo-Metabolic Challenges in the Management of Children with Spinal Muscular Atrophy Type 1. Nutrients 2021, 13, 2400. [Google Scholar] [CrossRef] [PubMed]
- Dangouloff, T.; Botty, C.; Beaudart, C.; Servais, L.; Hiligsmann, M. Systematic Literature Review of the Economic Burden of Spinal Muscular Atrophy and Economic Evaluations of Treatments. Orphanet J. Rare Dis. 2021, 16, 47. [Google Scholar] [CrossRef] [PubMed]
- Van Der Heul, A.M.B.; Cuppen, I.; Wadman, R.I.; Asselman, F.; Schoenmakers, M.A.G.C.; Van De Woude, D.R.; Gerrits, E.; Van Der Pol, W.L.; Van Den Engel-Hoek, L. Feeding and Swallowing Problems in Infants with Spinal Muscular Atrophy Type 1: An Observational Study. J. Neuromuscul. Dis. 2020, 7, 323–330. [Google Scholar] [CrossRef]
- De Holanda Mendonça, R.; Jorge Polido, G.; Ciro, M.; Jorge Fontoura Solla, D.; Conti Reed, U.; Zanoteli, E. Clinical Outcomes in Patients with Spinal Muscular Atrophy Type 1 Treated with Nusinersen. J. Neuromuscul. Dis. 2021, 8, 217–224. [Google Scholar] [CrossRef]
- Kennedy, R.A.; Carroll, K.; McGinley, J.L.; Paterson, K.L. Walking and Weakness in Children: A Narrative Review of Gait and Functional Ambulation in Paediatric Neuromuscular Disease. J. Foot Ankle Res. 2020, 13, 10. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.H.; Collins, E.; Lewis, L.; Guntrum, D.; Eichinger, K.; Voter, K.; Abdel-Hamid, H.Z.; Ciafaloni, E. Combination Therapy with Nusinersen and AVXS-101 in SMA Type 1. Neurology 2019, 93, 640–641. [Google Scholar] [CrossRef] [PubMed]
- Markati, T.; Fisher, G.; Ramdas, S.; Servais, L. Risdiplam: An Investigational Survival Motor Neuron 2 (SMN2) Splicing Modifier for Spinal Muscular Atrophy (SMA). Expert. Opin. Investig. Drugs 2022, 31, 451–461. [Google Scholar] [CrossRef] [PubMed]
- Matesanz, S.E.; Curry, C.; Gross, B.; Rubin, A.I.; Linn, R.; Yum, S.W.; Kichula, E.A. Clinical Course in a Patient with Spinal Muscular Atrophy Type 0 Treated with Nusinersen and Onasemnogene Abeparvovec. J. Child. Neurol. 2020, 35, 717–723. [Google Scholar] [CrossRef] [PubMed]
- Salmin, F.; Albamonte, E.; Morettini, V.; Gagliano, N.; Mercuri, E.; Sansone, V.A. Resolution of Skin Necrosis after Nusinersen Treatment in an Infant with Spinal Muscular Atrophy. Muscle Nerve 2019, 59, E42–E44. [Google Scholar] [CrossRef] [PubMed]
- Vega, P.; Glisser, C.; Castiglioni, C.; Amézquita, M.V.; Quirola, M.; Barja Yañez, S. Calidad de Vida En Niños y Adolescentes Con Atrofia Muscular Espinal. Rev. Chil. Pediatr. 2020, 91, 512–520. [Google Scholar] [CrossRef] [PubMed]
- Waldrop, M.A.; Elsheikh, B.H. Spinal Muscular Atrophy in the Treatment Era. Neurol. Clin. 2020, 38, 505–518. [Google Scholar] [CrossRef] [PubMed]
- Wurster, C.; Petri, S. Progress in Spinal Muscular Atrophy Research. Curr. Opin. Neurol. 2022, 35, 693–698. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research Electronic Data Capture (REDCap)—A Metadata-Driven Methodology and Workflow Process for Providing Translational Research Informatics Support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap Consortium: Building an International Community of Software Platform Partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef]
- Brower, A.; Chan, K.; Hartnett, M.; Taylor, J. The Longitudinal Pediatric Data Resource: Facilitating Longitudinal Collection of Health Information to Inform Clinical Care and Guide Newborn Screening Efforts. Int. J. Neonatal. Screen. 2021, 7, 37. [Google Scholar] [CrossRef] [PubMed]
- Chan, K.; Hu, Z.; Bush, L.W.; Cope, H.; Holm, I.A.; Kingsmore, S.F.; Wilhelm, K.; Scharfe, C.; Brower, A. NBSTRN Tools to Advance Newborn Screening Research and Support Newborn Screening Stakeholders. Int. J. Neonatal. Screen. 2023, 9, 63. [Google Scholar] [CrossRef] [PubMed]
- Berry, S.A.; Leslie, N.D.; Edick, M.J.; Hiner, S.; Justice, K.; Cameron, C. Inborn Errors of Metabolism Collaborative: Large-Scale Collection of Data on Long-Term Follow-up for Newborn-Screened Conditions. Genet. Med. 2016, 18, 1276–1281. [Google Scholar] [CrossRef] [PubMed]
- Tartaglia, N.; Howell, S.; Davis, S.; Kowal, K.; Tanda, T.; Brown, M.; Boada, C.; Alston, A.; Crawford, L.; Thompson, T.; et al. Early neurodevelopmental and medical profile in children with sex chromosome trisomies: Background for the prospective eXtraordinarY babies study to identify early risk factors and targets for intervention. Am. J. Med. Genet. C 2020, 184, 428–443. [Google Scholar] [CrossRef] [PubMed]
- Beyond Health Care: The Role of Social Determinants in Promoting Health and Health Equity|KFF. Available online: https://www.kff.org/racial-equity-and-health-policy/issue-brief/beyond-health-care-the-role-of-social-determinants-in-promoting-health-and-health-equity/ (accessed on 26 October 2023).
- Newborn Screening for SMA—Cure SMA. Available online: https://www.curesma.org/newborn-screening-for-sma/ (accessed on 21 February 2024).
- Updated 2018 SMA Standards of Care Statements Available Online—Cure SMA. Available online: https://www.curesma.org/updated-2018-sma-standards-of-care-statements-available-online/ (accessed on 21 February 2024).
- Kemper, A.; Lam, K.; Comeau, A.; Kwon, J.; Green, N.; Ojodu, J.; Grosse, S.; Prosser, L.; Jones, E.; Tanksley, S. Evidence-Based Review of Newborn Screening for Spinal Muscular Atrophy (SMA): Final Report (v5.2); Maternal and Child Health Bureau. 2018. Available online: https://www.hrsa.gov/sites/default/files/hrsa/advisory-committees/heritable-disorders/reports-recommendations/sma-final-report.pdf (accessed on 26 February 2024).
- AAP Motor Delay Tool. Available online: https://www.healthychildren.org/English/MotorDelay/Pages/default.aspx (accessed on 9 July 2019).
- CDC. What Is a Developmental Milestone? Centers for Disease Control and Prevention: Atlanta, GA, USA. Available online: https://www.cdc.gov/ncbddd/actearly/milestones/index.html (accessed on 26 February 2024).


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lietsch, M.; Chan, K.; Taylor, J.; Lee, B.H.; Ciafaloni, E.; Kwon, J.M.; Waldrop, M.A.; Butterfield, R.J.; Rathore, G.; Veerapandiyan, A.; et al. Long-Term Follow-Up Cares and Check Initiative: A Program to Advance Long-Term Follow-Up in Newborns Identified with a Disease through Newborn Screening. Int. J. Neonatal Screen. 2024, 10, 34. https://doi.org/10.3390/ijns10020034
Lietsch M, Chan K, Taylor J, Lee BH, Ciafaloni E, Kwon JM, Waldrop MA, Butterfield RJ, Rathore G, Veerapandiyan A, et al. Long-Term Follow-Up Cares and Check Initiative: A Program to Advance Long-Term Follow-Up in Newborns Identified with a Disease through Newborn Screening. International Journal of Neonatal Screening. 2024; 10(2):34. https://doi.org/10.3390/ijns10020034
Chicago/Turabian StyleLietsch, Mei, Kee Chan, Jennifer Taylor, Bo Hoon Lee, Emma Ciafaloni, Jennifer M. Kwon, Megan A. Waldrop, Russell J. Butterfield, Geetanjali Rathore, Aravindhan Veerapandiyan, and et al. 2024. "Long-Term Follow-Up Cares and Check Initiative: A Program to Advance Long-Term Follow-Up in Newborns Identified with a Disease through Newborn Screening" International Journal of Neonatal Screening 10, no. 2: 34. https://doi.org/10.3390/ijns10020034
APA StyleLietsch, M., Chan, K., Taylor, J., Lee, B. H., Ciafaloni, E., Kwon, J. M., Waldrop, M. A., Butterfield, R. J., Rathore, G., Veerapandiyan, A., Kapil, A., Parsons, J. A., Gibbons, M., & Brower, A. (2024). Long-Term Follow-Up Cares and Check Initiative: A Program to Advance Long-Term Follow-Up in Newborns Identified with a Disease through Newborn Screening. International Journal of Neonatal Screening, 10(2), 34. https://doi.org/10.3390/ijns10020034