Abstract
Left ventricular non-compaction cardiomyopathy is a genetic disorder characterized by the presence of two myocardial layers with numerous prominent trabeculations and deep inter-trabecular recesses that communicate with the ventricular cavity. The diagnosis is often challenging because excessive trabeculations may also be a normal finding in performance athletes and black people. Echocardiography is the gold standard for diagnosis of this condition, but other useful diagnostic techniques may include cardiac magnetic resonance imaging, computed tomography, and contrast ventriculography. Moreover, newer echocardiographic methods such as three-dimensional imaging and speckle tracking analysis promise to improve the diagnosis of left ventricular non-compaction cardiomyopathy. The purpose of this paper is to review the pathogenesis, diagnosis, and management of this disease.
Introduction
Left ventricular non-compaction (LVNC) or ‘spongy myocardium’ is a congenital disorder characterized by the presence of a thin epicardial layer and an excessively trabeculated endocardial layer. This particular spongious aspect of the myocardium was first described more than eight decades ago in association with aortic atresia and coronary-to-chamber fistula during the autopsy of a newborn with complex congenital abnormalities [1]. The introduction of two-dimensional echocardiography facilitated the evaluation of left ventricle (LV) anatomy and continuously increased the number of cases diagnosed. In 1984 Engberding described the presence of ‘sinusoids’ within the LV, but it was not until 1990 that the first diagnostic echocardiographic criteria of LVNC were proposed and terminology was established [2,3].
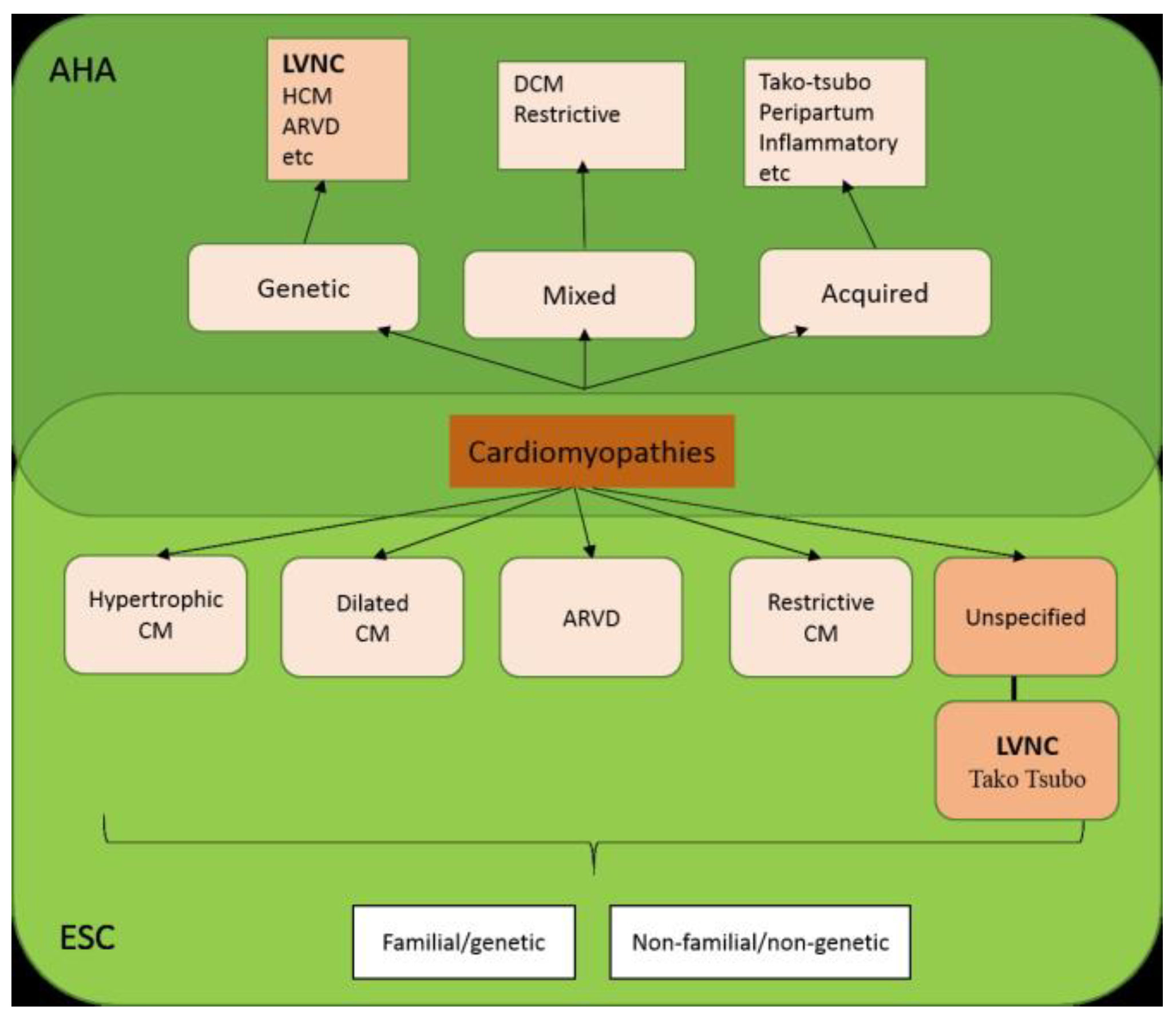
Despite current developments in cardiac imaging and genetic diagnostic techniques, it is yet controversial whether left ventricular non-compaction cardiomyopathy is a distinct cardiomyopathy or a morphologic feature shared by different types of cardiomyopathy [4]. Recent data, for example, have found that a significant proportion of asymptomatic individuals free from cardiovascular disease met all currently used magnetic resonance imaging (MRI) diagnostic criteria for LVNC, suggesting that the condition is an anatomical phenotype rather than a distinct cardiomyopathy [5]. To add to the controversy, non-compacted myocardium has been categorized as unclassified cardiomyopathy by the European Society of Cardiology (ESC) in the recently published report on the definition and classification of cardiomyopathies [6], whereas the American Heart Association (AHA) classifies it as a primary genetic cardiomyopathy [7] (Figure 1).
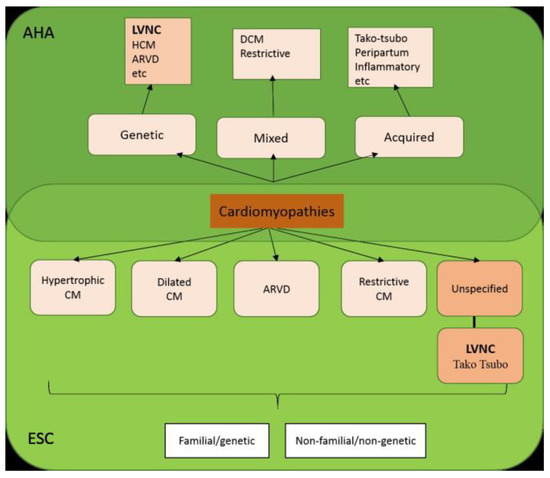
Figure 1.
Classification of primary (predominantly involving the heart) cardiomyopathies according to ESC and AHA. AHA, American Heart Association; ARVD, Arrythmogenic right ventricle dysplasia; CM, cardiomyopathy; DCM, dilated cardiomyopathy; ESC, European Society of Cardiology; HCM, hypertrophic cardiomyopathy; LVNC, left ventricle non- compaction.
Discussion
Prevalence
The prevalence of LVNC in the general population remains unknown, although in echocardiographic series it is reported around 0.14-1.3%. Isolated ventricular non- compaction has an incidence of 0.01-0.26% in observational studies [8,9]. In a pediatric population with any type of primary cardiomyopathy, LVNC was diagnosed in 9.2%, being the most frequent form after dilated and hypertrophic cardiomyopathy [10]. Left ventricular non-compaction in children is often associated with anatomical abnormalities such as septal or atrial defects, congenital aortic stenosis, and aortic coarctation, although studies have failed to demonstrate any direct relation among these conditions. Furthermore, non-compacted myocardium has been found in patients with neuromuscular diseases such as Becker muscular dystrophy, Friedrich ataxia, myotonic dystrophy, or mitochondrial diseases.
Nevertheless, published rates may well underestimate the prevalence of LVNC. Better echocardiographic imaging and LVNC awareness will likely lead to a better recognition of this pathology.
Pathogenesis
The mechanisms of non-compaction are not yet fully understood. The main morphogenetic anomaly is represented by the cessation of compaction of ventricular endomyocardium during intrauterine development. If this process does not progress normally, the LV develops as a two-layered structure, with a thick non- compacted endocardial layer and a thin compact epicardial layer, mostly observed in the inferior, lateral and apical segments.
During myocardial embryonic development, the muscular fibers lose their connections, resulting in a weak fiber network, with recesses that connect the myocardial wall with the ventricular cavity. Only in the 5th or 6th week of gestation does this fiber and intertrabecular recesses network begin the compaction process, starting from the base towards the apex and from the endocardium to the epicardium. This process implies the secretion of endothelial growth factors, such as neuregulins and angiopoietins. For reasons still unknown, this process ceases in patients with LVNC, resulting in a thick non-compacted endomyocardial layer with prominent trabeculae and deep recesses that communicate with the LV cavity and a thin compacted epicardial layer. This embryologic hypothesis is supported by the fact that LVNC is frequently associated with other congenital heart abnormalities [11]. Other theories suggest that ventricular non-compaction might be the consequence of a cardiac neuropathy or the result of a malfunction of gap junctions [12].
The trabecular phenotype in LVNC can also develop during adulthood as a response to left ventricular overload. In one large-scale study, excessive trabeculation of the LV was found in up to 18% of highly trained athletes. Nonetheless, only 0.9% of these athletes also presented with ECG changes and echocardiographic signs of systolic function depression [13]. Development of the ‘de novo’ hypertrabeculation has been observed in more than 25% of pregnant women and is related to LV overload and mechanisms of physiological adaptation to pregnancy. A similar anatomical aspect was described in patients suffering from sickle cell disease and chronic renal failure [14] due to an exaggerated response to the increase in preload. These examples challenge the embryogenesis theory and suggest involvement of acquired pathogenetic mechanisms or epigenetic factors. Given these considerations a recent review recommends cautious diagnostic labeling of LVNC as a cardiomyopathy [15].
Genetics
LVNC is a heterogeneous, familial, or sporadic genetic disorder. Genetic studies have strongly suggested that the disease has a pattern of inheritance (18% to 50% of cases are familial). The family form appears more frequently in adults with isolated LVNC than in the case of children, and it can be autosomal dominant, X-linked, or mitochondrial. Mutations of genes that code sarcomeric proteins (ACTC1 - cardiac alpha actinin, MYH7 - beta myosin heavy chain, TNNT2 - Troponin T, G4.5-tafazzin - responsible for Barth syndrome, TMP1-tropomyosin, MYBPC3 - binding protein C) [16,17,18], cytoskeletal and Z-line components (LDB3 - binding protein 3) [19], nuclear envelope proteins (LMNA-laminin A/C) [20] and ion-channels (SNC5A - RYR2) [21] have been identified in patients with ventricular non-compaction. Moreover, the hypertrabecular and non-compacted aspect of the left ventricle has also been associated with monogenic syndromes such as Danon disease [22] or, in a few cases, Anderson-Fabry disease [23]. Other genetic conditions that coexist with the spongious feature of the LV myocardium are Duchenne muscular dystrophy [24], mitochondrial myopathies [9], chromosomal disorders, and congenital heart disease. Specific mutations in genes of the Notch1 pathway (mindbomb homolog 1) in mice and humans leading to dysregulated signaling and hypertrabeculation and non-compaction [25], as well as mutations in the G4.5 gene that result in a severe, infantile, X-linked form of LVNC, suggest strongly that LVNC is a cardiomyopathy.
It is therefore both important and challenging to distinguish whether LVNC is an isolated cardiomyopathy or an anatomical characteristic associated with other cardiac disorders. Previous studies suggest that a detailed analysis of the family background in patients diagnosed with LVNC is justified.
Physiopathology
The two myocardial layers and the trabeculae are vascularized by the epicardial coronary arteries and the intertrabecular recesses receive blood from the ventricular cavity. Endocardial hypoperfusion arises because of a discrepancy between the number of capillaries and the myocardial mass. As a consequence of ischemia, fibrosis will expand progressively and will ultimately determine left ventricular systolic function depression which will predispose to ventricular arrhythmias. LVNC is a potential thromboembolic disease due to the blood stagnation in the intertrabecular recesses which predisposes to clot formation, which can embolize in systemic circulation.
Imaging and Diagnosis
A multimodal diagnostic approach is the current recommendation for LVNC diagnosis. Echocardiography, although dependent on the echocardiographer’s skills and the echocardiographic window, remains the primary diagnostic method. Other imaging methods such as cardiac MRI can diagnose the pathology, when echocardiographic examination is suboptimal.
Echocardiographic diagnosis criteria
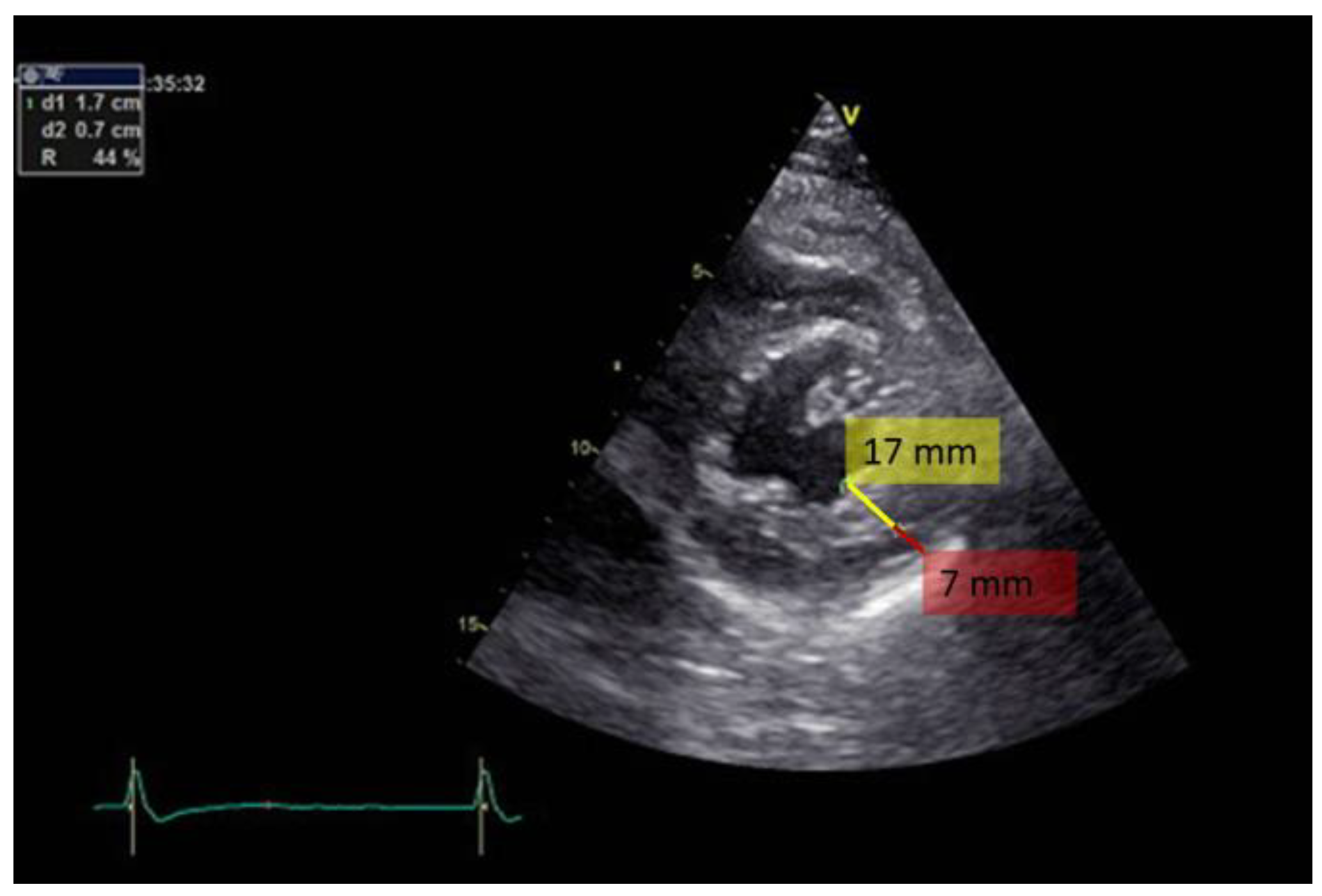
Transthoracic bidimensional echocardiography (2D- TTE) is the method of choice for diagnosing LVNC (Figure 2, Figure 3 and Figure 4). Three basic echocardiographic criteria have been proposed to define LVNC: a thick myocardium with a non-compacted layer and a compacted one; prominent trabeculations; and deep endomyocardial recesses.
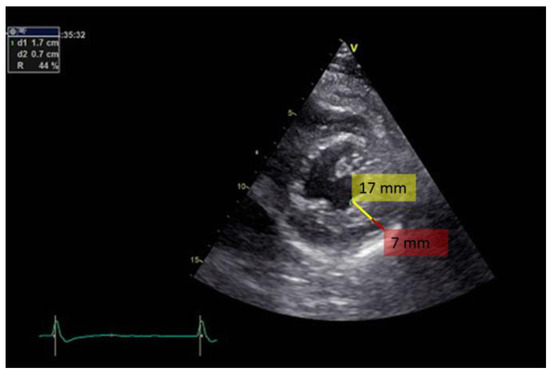
Figure 2.
Bidimensional transthoracic echo- cardiography, short axis view of the left ventricle apex. Note the excessive trabeculation in the infero-postero- lateral region. Red line indicates the distance from the epicardial line to the beginning of the trabeculae (7 mm) and yellow line marks the thickness of the trabeculae (17 mm).
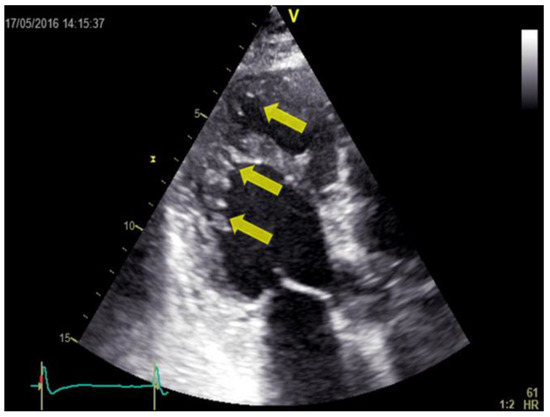
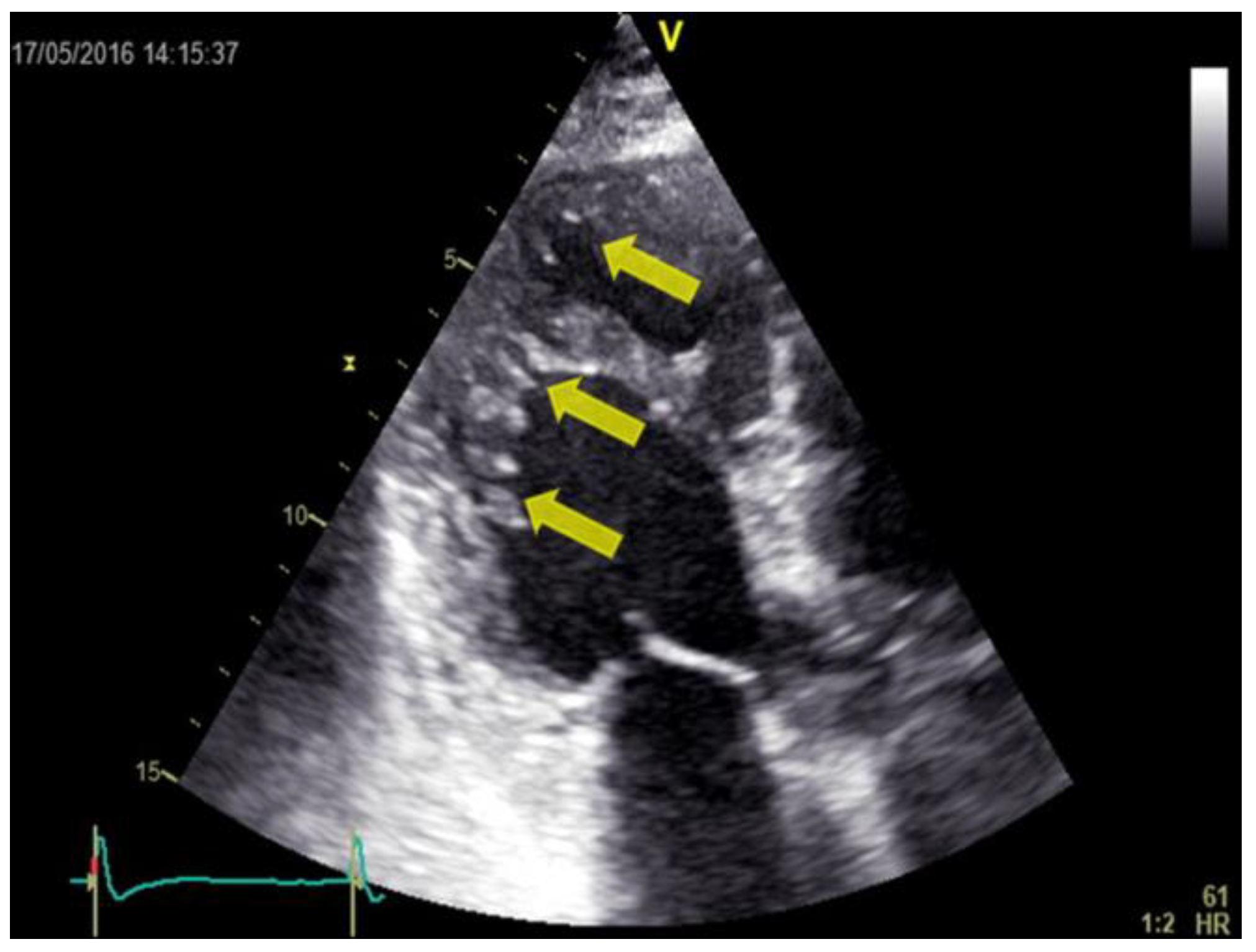
Figure 3.
Bidimensional transthoracic echo- cardiography, apical 3-chamber view (the same patient as in figure 2). The hypertrabeculation can be observed in the mid and apical region of the posterior wall (yellow arrows).
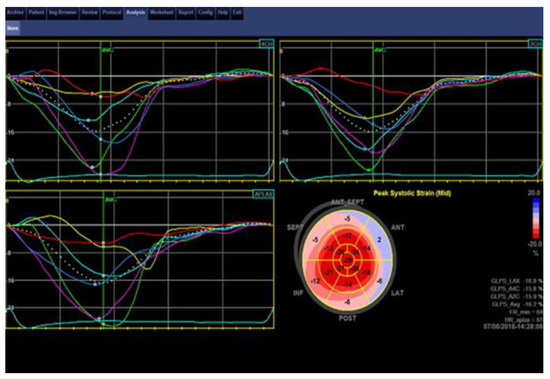
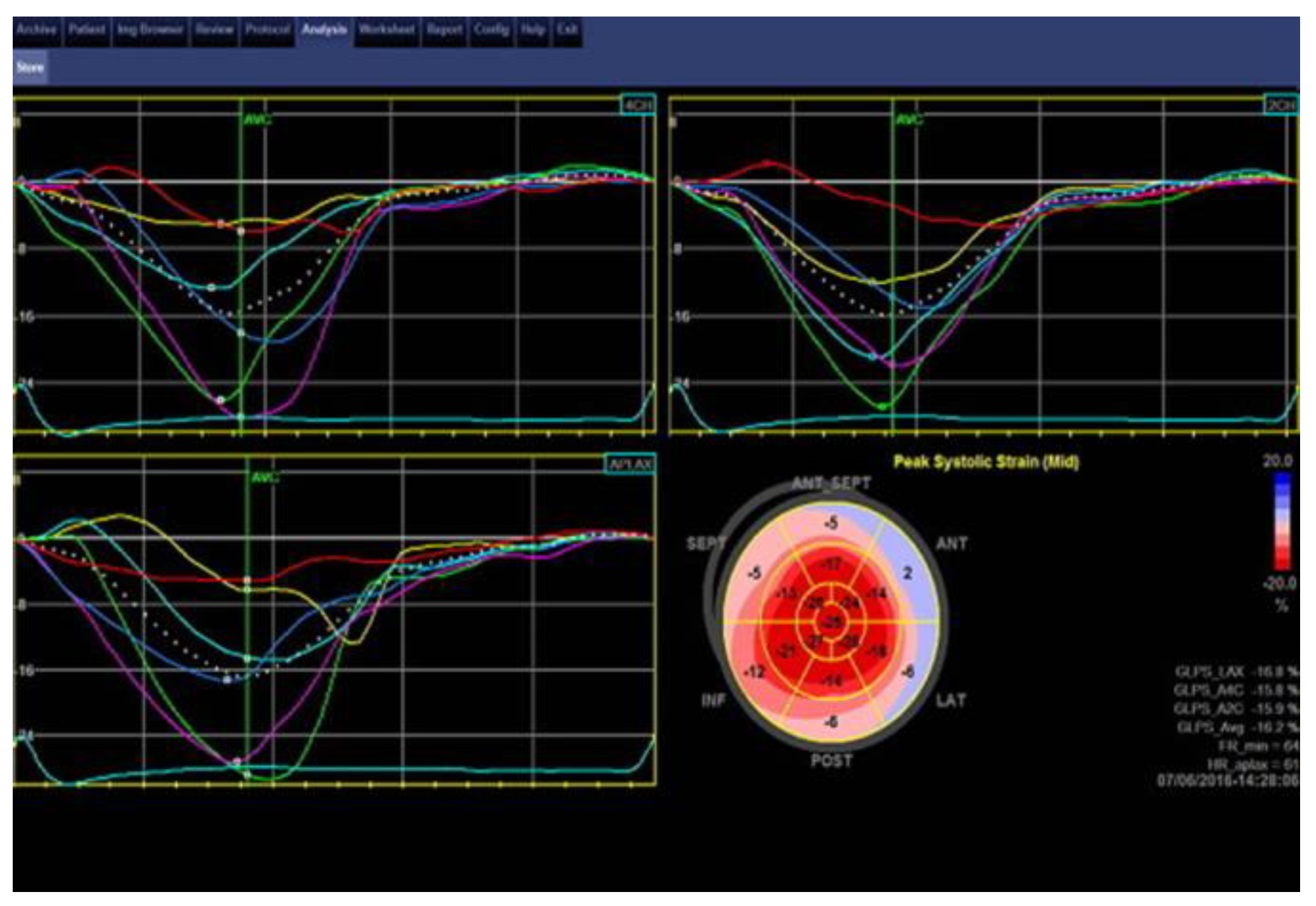
Figure 4.
Speckle tracking echocardiography analysis, bull’s eye and regional strain curves (the same patient as in figure 2). Mildly decreased global longitudinal strain, with a value of -16.2%. Deformation is lower in the basal segments and normal in the midwall and apical segments. This may be explained by the globular shape of the LV and the presence of trabeculae in the apex.
Several echocardiographic derived algorithms for diagnosing LVNC have been proposed [3,26,27]. The first echocardiographic criterion has defined ventricular wall non-compaction as the ratio X / Y < 0.5, where X represents the distance from the epicardial surface to the trabecular recesses and Y is the distance from the epicardial surface to the peak of trabeculae, measured in parasternal short axis for the apex and apical sections for the left ventricular free wall [3]. Others have proposed a ratio between non-compacted and compacted myocardium greater than 2:1 at end systole, in apical short axis section, in the absence of other cardiac disorders [26] for the diagnosis of LVNC. The trabeculae are usually situated at the apex / lateral wall, medium wall / inferior wall of the left ventricle. Most of the non-compacted segments are hypokinetic. Stollberger et al. [27] defined LVNC as the presence of more than three trabeculae in the left ventricular wall, with trabeculae situated at the apex, visible in a single imaging plan. The flow between the inter-trabecular recesses can be identified by using the color Doppler method. A fourth criterion has been proposed by Belanger et al. [28], who diagnosed LVNC using planimetric echocardiography to measure the trabeculae in apical 4 chambers section. They divided the patients by the area of left ventricular non-compaction into 3 groups: mild (< 2.5 cm2), moderate (2.5-4.9 cm2) and severe (> 5 cm2). Based on a study on 380 patients, 15.8% were diagnosed with LVNC. However, their criteria have not been validated as there was no correlation with the modified Jenni et al. criteria.
Newer echocardiographic techniques such as tissue Doppler imaging, strain rate imaging, and speckle tracking imaging are now available for the diagnosis of LVNC. Global longitudinal strain was found to be lower in subjects with LVNC compared with healthy controls even in the presence of normal systolic/diastolic function [29]. A recent study also demonstrated that while in normal individuals and subjects with hypertrophic cardiomyopathy there is a significant increase in longitudinal deformation from base to apex, in subjects with LVNC, apical strain was only mildly and not significantly increased [30]. Three-dimensional echocardiography and contrast echocardiography may bring additional valuable data to the dimensional assessment in patients with LVNC by providing an accurate evaluation of the number of trabeculae, compacted segments, and intertrabecular recesses [31].
Cardiac Magnetic Resonance criteria
Cardiac magnetic resonance imaging is continually evolving and may contribute to a more accurate identification of LVNC. Cardiac MRI is particularly useful in patients in whom the apex is difficult to visualize with echocardiography. Two sets of MRI criteria proposed by Petersen in 2005 [32] and Jacquier in 2010 [33] are used for LVNC diagnosis. Petersen et al. defined a ratio between non-compacted/compacted layer > 2.3 measured in end-diastole as a cutoff for LVNC. Jacquier et al. calculated the LV trabecular mass in short axis views in end-diastole and concluded that a trabecular mass > 20% was predictive for LVNC.
Captur and al. [34] described a recent cardiac MRI technique, based on fractal analysis, which does not rely on ‘classical’ compacted/non-compacted ratio. A fractal dimension > 1.3 gave the optimal prediction for LVNC.
Late gadolinium enhancement (LGE) of trabeculae has also been observed in LVNC. LGE distributions in patients fulfilling LVNC criteria can be very heterogeneous, which may suggest several distinct cardiomyopathic processes that are responsible for LVNC. Small areas of myocardial fibrosis have also been observed in patients with preserved systolic function [35].
Other diagnostic imaging
Computed tomography (CT) is an alternative method of diagnosing LVNC if the echocardiogram is non-diagnostic or unavailable [36]. Positron emission tomography (PET), which quantitatively evaluates myocardial blood flow and coronary flow reserve, may be used to assess microcirculatory dysfunction ultimately responsible for the wall motion abnormalities [37].
Differential diagnosis
As there is no diagnostic gold standard, LVNC is frequently underdiagnosed or misdiagnosed as hypertrophic or dilated cardiomyopathy. The differential diagnosis should include: apical hypertrophic cardiomyopathy, left ventricular hypertrophy, dilated cardiomyopathy, arrhythmogenic left ventricular dysplasia, myocardial/endocardial fibroelastosis, cardiac tumors, left ventricular apical thrombus, normal heart with left ventricular prominent trabeculations (less than 3 trabeculations in echocardiography). Usually, a careful echocardiography study by a trained examiner will provide the diagnosis. A major challenge is to differentiate LVNC with dilated left ventricle from dilated cardiomyopathy.
Management of LVNC
Currently no specific guidelines exist for the treatment of LVNC. Clinical management of LVNC depends on the presence or absence of cardiac dysfunction or arrhythmias. Patients with normal LV size and function will undergo clinical monitoring, whereas symptomatic patients with LV dilation and dysfunction or hypertrophy may be managed according to their clinical needs and corresponding guidelines. In later stages, recommendations for treatment follow the international guidelines of heart failure management. Treatment usually requires the combination of beta- blockers, ACE inhibitors/ARB, diuretics, and aldosterone antagonists.
The main complications related to LVNC are systemic thromboembolic events, arrhythmias, progressive heart failure, and sudden cardiac death. Oral anticoagulation is a debated issue in the prevention of thromboembolic complications. The question that arises is whether anticoagulation should be given independently of arrhythmias or LV dysfunction for primary prevention of embolic episodes, or only in the presence of LV dysfunction, arrhythmias, prior embolic events, or proven atrial or ventricular thrombi. Left ventricular clot and documented atrial fibrillation are clear situations when oral anticoagulation should be used. For patients that do not fall into either of these categories, Bennet et al. suggest a risk assessment using the CHADS2/CHA2DS2-Vasc scores as guidance and a discussion with the patient regarding the risks and benefits of anticoagulation [38].
Sudden cardiac death is another concerning complication of LVNC. Patients should be periodically evaluated by Holter ECG for ventricular arrhythmias. The incidence of ventricular arrhythmias rises from 2% to 62% in patients with LVNC. Those with sustained ventricular arrhythmia and those who have experienced an episode of cardiac arrest require ICD implantation.
Although data regarding anti-arrhythmic therapy are scant, recent research supports the idea of early aggressive therapy, including defibrillator and evaluation for cardiac transplant, for patients with bundle brunch block, increased left ventricle end-diastolic diameter, or permanent or persistent atrial fibrillation in III-IV NYHA functional class.
Echocardiographic screening is also recommended for family members, given that the symptoms are variable and the risks include heart failure and sudden cardiac death. Genetic testing for LVNC does not change clinical management of the disease; however, it may be helpful for confirming diagnosis in family members.
Prognosis
LVNC is associated with high morbidity and mortality rates although prognosis has significantly improved in recent years through earlier diagnosis and use of heart failure medications and device therapy. In one Swiss cohort, 35% of patients suffered early death, 53% required hospitalization for congestive heart failure, 41% had ventricular tachyarrhythmia, 12% required ICDs, and 12% required heart transplantation over 44 months of follow-up [39]. In another recent study, among 45 patients referred to a cardiomyopathy center, survival free of transplantation was 97% over 4 years of follow-up [40].
Conclusions
LVNC is a rare cardiomyopathy associated with significant morbidity and mortality. The diagnosis remains challenging and a multimodal diagnostic approach is currently recommended. The classical clinical presentation is the triad of heart failure, arrhythmias, and embolic events. There are no consensus guidelines for the management of these patients.
Acknowledgments
All authors contributed equally to the manuscript.
References
- Rooms, I.; Dujardin, K.; De Sutter, J. Non-compaction cardiomyopathy: a genetically and clinically heterogeneous disorder. Acta Cardiol. 2015, 70, 625–631. [Google Scholar] [CrossRef] [PubMed]
- Towbin, J.A.; Lorts, A.; Jefferies, J.L. Left ventricular non-compaction cardiomyopathy. Lancet 2015, 386, 813–825. [Google Scholar] [CrossRef] [PubMed]
- Chin, T.K.; Perloff, J.K.; Williams, R.G.; Jue, K.; Mohrmann, R. Isolated noncompaction of left ventricular myocardium. A study of eight cases. Circulation 1990, 82, 507–513. [Google Scholar] [CrossRef] [PubMed]
- Arbustini, E.; Weidemann, F.; Hall, J.L. Left ventricular noncompaction: A distinct cardiomyopathy or a trait shared by different cardiac diseases? J Am Coll Cardiol. 2014, 64, 1840–1850. [Google Scholar] [CrossRef] [PubMed]
- Weir-McCall, J.R.; Yeap, P.M.; Papagiorcopulo, C.; Fitzgerald, K.; Gandy, S.J.; Lambert, M.; Belch, J.J.; CavinI, *!!! REPLACE !!!*; Littleford, R.; Macfarlane, J.A.; Matthew, S.Z.; Nicholas, R.S.; Struthers, A.D.; Sullivan, F.; Waugh, S.A.; White, R.D.; Houston, J.G. Left ventricular noncompaction: Anatomical Phenotype or Distinct Cardiomyopathy? J Am Coll Cardiol. 2016, 68, 2157–2165. [Google Scholar] [CrossRef] [PubMed]
- Elliott, P.; Andersson, B.; Arbustini, E.; Bilinska, Z.; Cecchi, F.; Charron, P.; Dubourg, O.; Kühl, U.; Maisch, B.; McKenna, W.J.; Monserrat, L.; Pankuweit, S.; Rapezzi, C.; Seferovic, P.; Tavazzi, L.; Keren, A. Classification of the cardiomyopathies: A position statement from the european society of cardiology working group on myocardial and pericardial diseases. Eur Heart J. 2008, 29, 270–276. [Google Scholar] [CrossRef] [PubMed]
- Maron, B.J.; Towbin, J.A.; Thiene, G.; Antzelevitch, C.; Corrado, D.; Arnett, D.; Moss, A.J.; Seidman, C.E.; Young, J.B.; American Heart Association; Council on Clinical Cardiology, Heart Failure and Transplantation Committee; Quality of Care and Outcomes Research and Functional Genomics and Translational Biology Interdisciplinary Working Groups; Council on Epidemiology and Prevention. Contemporary definitions and classification of the cardiomyopathies: an American Heart Association Scientific Statement from the Council on Clinical Cardiology, Heart Failure and Transplantation Committee; Quality of Care and Outcomes Research and Functional Genomics and Translational Biology Interdisciplinary Working Groups; and Council on Epidemiology and Prevention. Circulation 2006, 113, 1807–1816. [Google Scholar] [CrossRef] [PubMed]
- Oechslin, E.N.; AttenhoferJost, C.H.; Rojas, J.R.; Kaufmann, P.A.; Jenni, R. Long-term follow-up of 34 adults with isolated left ventricular noncompaction: a distinct cardiomyopathy with poor prognosis. J Am Coll Cardiol. 2000, 36, 493–500. [Google Scholar] [CrossRef] [PubMed]
- Oechslin, E.; Jenni, R. Left ventricular non- compaction revisited: a distinct phenotype with genetic heterogeneity? Eur Heart J. 2011, 32, 1446–1456. [Google Scholar] [CrossRef] [PubMed]
- Nugent, A.W.; Daubeney, P.E.F.; Chondros, P.; Carlin, J.B.; Cheung, M.; Wilkinson, L.C.; Davis, A.M.; Kahler, S.G.; Chow, C.W.; Wilkinson, J.L.; Weintraub, R.G.; National Australian Childhood Cardiomyopathy Study. The epidemiology of childhood cardiomyopathy in Australia. N Engl J Med. 2003, 348, 1639–1646. [Google Scholar] [CrossRef] [PubMed]
- Stähli, B.E.; Gebhard, C.; Biaggi, P.; Klaassen, S.; ValsangiacomoBuechel, E.; AttenhoferJost, C.H.; Jenni, R.; Tanner, F.C.; Greutmann, M. Left ventricular non- compaction: Prevalence in congenital heart disease. Int J Cardiol. 2013, 167, 2477–81 PMID: 22704867. [Google Scholar] [CrossRef] [PubMed]
- Sleurs, E.; De Catte, L.; Benatar, A. Prenatal diagnosis of isolated ventricular noncompaction of the myocardium. J Ultrasound Med. 2005, 24, 1325–1329. [Google Scholar] [CrossRef] [PubMed]
- Gati, S.; Chandra, N.; Bennett, R.L.; Reed, M.; Kervio, G.; Panoulas, V.F.; Ghani, S.; Sheikh, N.; Zaidi, A.; Wilson, M.; Papadakis, M.; Carré, F.; Sharma, S. Increased left ventricular trabeculation in highly trained athletes: Do we need more stringent criteria for the diagnosis of left ventricular non-compaction in athletes? Heart 2013, 99, 401–408. [Google Scholar] [CrossRef] [PubMed]
- Markovic, N.S.; Dimkovic, N.; Damjanovic, T.; Loncar, G.; Dimkovic, S. Isolated ventricular noncompaction in patients with chronic renal failure. Clin Nephrol. 2008, 70, 72–76. [Google Scholar] [CrossRef] [PubMed]
- Arbustini, E.; Favalli, V.; Narula, N.; Serio, A.; Grasso, M. Left ventricular noncompaction: A Distinct Genetic Cardiomyopathy? J Am Coll Cardiol. 2016, 68, 949–966. [Google Scholar] [CrossRef] [PubMed]
- Klaassen, S.; Probst, S.; Oechslin, E.; Gerull, B.; Krings, G.; Schuler, P.; Greutmann, M.; Hürlimann, D.; Yegitbasi, M.; Pons, L.; Gramlich, M.; Drenckhahn, J.D.; Heuser, A.; Berger, F.; Jenni, R.; Thierfelder, L. Mutations in sarcomere protein genes in left ventricular noncompaction. Circulation 2008, 117, 2893–2901. [Google Scholar] [CrossRef] [PubMed]
- Arsene, A.L.; Uivarosi, V.; Mitrea, N.; Drăgoi, C.M.; Nicolae, A.C. In vitro studies regarding the interactions of some novel ruthenium (III) complexes with double stranded calf thymus deoxyribonucleic acid (DNA). Farmacia. 2016, 64, 712–716. [Google Scholar]
- Luedde, M.; Ehlermann, P.; Weichenhan, D.; Will, R.; Zeller, R.; Rupp, S.; Müller, A.; Steen, H.; Ivandic, B.T.; Ulmer, H.E.; Kern, M.; Katus, H.A.; Frey, N. Severe familial left ventricular non-compaction cardiomyopathy due to a novel troponin T (TNNT2) mutation. Cardiovasc Res. 2010, 86, 452–460. [Google Scholar] [CrossRef] [PubMed]
- Vatta, M.; Mohapatra, B.; Jimenez, S.; Sanchez, X.; Faulkner, G.; Perles, Z.; Sinagra, G.; Lin, J.H.; Vu, T.M.; Zhou, Q.; Bowles, K.R.; Di Lenarda, A.; Schimmenti, L.; Fox, M.; Chrisco, M.A.; Murphy, R.T.; McKenna, W.; Elliott, P.; Bowles, N.E.; Chen, J.; Valle, G.; Towbin, J.A. Mutations in Cypher/ZASP in patients with dilated cardiomyopathy and left ventricular non- compaction. J Am Coll Cardiol. 2003, 42, 2014–2027. [Google Scholar] [CrossRef] [PubMed]
- Rankin, J.; Auer-Grumbach, M.; Bagg, W.; Colclough, K.; Duong, N.T.; Fenton-May, J.; Hattersley, A.; Hudson, J.; Jardine, P.; Josifova, D.; Longman, C.; McWilliam, R.; Owen, K.; Walker, M.; Wehnert, M.; Ellard, S. Extreme phenotypic diversity and nonpenetrance in families with the LMNA gene mutation R644C. Am J Med Genet A. 2008, 146A(12), 1530–1542. [Google Scholar] [CrossRef] [PubMed]
- Shan, L.; Makita, N.; Xing, Y.; Watanabe, S.; Futatani, T.; Ye, F.; Saito, K.; Ibuki, K.; Watanabe, K.; Hirono, K.; Uese, K.; Ichida, F.; Miyawaki, T.; Origasa, H.; Bowles, N.E.; Towbin, J.A. SCN5A variants in Japanese patients with left ventricular noncompaction and arrhythmia. Mol Genet Metab. 2008, 93, 468–474. [Google Scholar] [CrossRef] [PubMed]
- Van Der Starre, P.; Deuse, T.; Pritts, C.; Brun, C.; Vogel, H.; Oyer, P. Late profound muscle weakness following heart transplantation due to Danon disease. Muscle Nerve. 2013, 47, 135–137. [Google Scholar] [CrossRef] [PubMed]
- Azevedo, O.; Gaspar, P.; Sá Miranda, C.; Cunha, D.; Medeiros, R.; Lourenço, A. Left ventricular noncompaction in a patient with Fabry disease: Overdiagnosis, morphological manifestation of Fabry disease or two unrelated rare conditions in the same patient? Cardiology 2011, 119, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Stöllberger, C.; Finsterer, J.; Blazek, G. Left ventricular hypertrabeculation / noncompaction and association with additional cardiac abnormalities and neuromuscular disorders. Am J Cardiol. 2002, 90, 899–902. [Google Scholar] [CrossRef] [PubMed]
- Luxán, G.; Casanova, J.C.; Martínez-Poveda, B.; Prados, B.; D’Amato, G.; MacGrogan, D.; Gonzalez-Rajal, A.; Dobarro, D.; Torroja, C.; Martinez, F.; Izquierdo-García, J.L.; Fernández-Friera, L.; Sabater-Molina, M.; Kong, Y.Y.; Pizarro, G.; Ibañez, B.; Medrano, C.; García-Pavía, P.; Gimeno, J.R.; Monserrat, L.; Jiménez-Borreguero, L.J.; de la Pompa, J.L. Mutations in the NOTCH pathway regulator MIB1 cause left ventricular noncompaction cardiomyopathy. Nat Med. 2013, 19, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Jenni, R.; Oechslin, E.; Schneider, J.; Attenhofer Jost, C.; Kaufmann, P.A. Echocardiographic and pathoanatomical characteristics of isolated left ventricular non-compaction: a step towards classification as a distinct cardiomyopathy. Heart 2001, 86, 666–671. [Google Scholar] [CrossRef] [PubMed]
- Stöllberger, C.; Finsterer, J. Left ventricular hypertrabeculation/noncompaction. J Am Soc Echocardiogr. 2004, 17, 91–100. [Google Scholar] [CrossRef] [PubMed]
- Belanger, A.R.; Miller, M.A.; Donthireddi, U.R.; Najovits, A.J.; Goldman, M.E. New classification scheme of left ventricular noncompaction and correlation with ventricular performance. Am J Cardiol. 2008, 102, 92–96. [Google Scholar] [CrossRef] [PubMed]
- Cortés, M.; Oliva, M.R.; Orejas, M.; Navas, M.A.; Rábago, R.M.; Martínez, M.E.; Taibo, M.; Palfy, J.; Rey, M.; Farré, J. Usefulness of speckle myocardial imaging modalities for differential diagnosis of left ventricular non-compaction of the myocardium. Int J Cardiol. 2016, 223, 813–818. [Google Scholar] [CrossRef] [PubMed]
- Haland, T.F.; Saberniak, J.; Leren, I.S.; Edvardsen, T.; Haugaa, K.H. Echocardiographic comparison between left ventricular non-compaction and hypertrophic cardiomyopathy. Int J Cardiol. 2017, 228, 900–905. [Google Scholar] [CrossRef] [PubMed]
- Petersen, S.E.; Selvanayagam, J.B.; Wiesmann, F.; Robson, M.D.; Francis, J.M.; Anderson, R.H.; Watkins, H.; Neubauer, S. Left ventricular non-compaction. J Am Coll Cardiol. 2005, 46, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Bodiwala, K.; Miller, A.P.; Nanda, N.C.; Patel, V.; Vengala, S.; Mehmood, F.; Upendram, S.; Frans, E. Live three-dimensional transthoracic echocardiographic assessment of ventricular noncompaction. Echocardiography 2005, 22, 611–620. [Google Scholar] [CrossRef] [PubMed]
- Jacquier, A.; Thuny, F.; Jop, B.; Giorgi, R.; Cohen, F.; Gaubert, J.Y.; Vidal, V.; Bartoli, J.M.; Habib, G.; Moulin, G. Measurement of trabeculated left ventricular mass using cardiac magnetic resonance imaging in the diagnosis of left ventricular non-compaction. Eur Heart J. 2010, 31, 1098–1104. [Google Scholar] [CrossRef] [PubMed]
- Captur, G.; Muthurangu, V.; Cook, C.; Flett, A.S.; Wilson, R.; Barison, A.; Sado, D.M.; Anderson, S.; McKenna, W.J.; Mohun, T.J.; Elliott, P.M.; Moon, J.C. Quantification of left ventricular trabeculae using fractal analysis. J Cardiovasc Magn Reson. 2013, 15, 36. [Google Scholar] [CrossRef] [PubMed]
- Nucifora, G.; Aquaro, G.D.; Masci, P.G.; Pingitore, A.; Lombardi, M. Magnetic resonance assessment of prevalence and correlates of right ventricular abnormalities in isolated left ventricular noncompaction. Am J Cardiol. 2014, 113, 142–146. [Google Scholar] [CrossRef] [PubMed]
- Sidhu, M.S.; Uthamalingam, S.; Ahmed, W.; Engel, L.-C.; Vorasettakarnkij, Y.; Lee, A.M.; Hoffmann, U.; Brady, T.; Abbara, S.; Ghoshhajra, B.B. Defining left ventricular noncompaction using cardiac computed tomography. J Thorac Imaging. 2014, 29, 60–66. [Google Scholar] [CrossRef] [PubMed]
- Jenni, R.; Wyss, C.A.; Oechslin, E.N.; Kaufmann, P.A. Isolated ventricular voncompaction is associated with coronary microcirculatory dysfunction. J Am Coll Cardiol. 2002, 39, 450–454. [Google Scholar] [CrossRef] [PubMed]
- Bennett, C.E.; Freudenberger, R. The current approach to diagnosis and management of left ventricular noncompaction cardiomyopathy: review of the literature. Cardiol Res Pract. 2016, 2016, 5172308. [Google Scholar] [CrossRef] [PubMed]
- Hussein, A.; Karimianpour, A.; Collier, P.; Krasuski, R.A. Isolated noncompaction of the left ventricle in adults. J Am Coll Cardiol. 2015, 66, 578–585. [Google Scholar] [CrossRef] [PubMed]
- Murphy, R.T.; Thaman, R.; Blanes, J.G.; Ward, D.; Sevdalis, E.; Papra, E.; Kiotsekoglou, A.; Tome, M.T.; Pellerin, D.; McKenna, W.J.; Elliott, P.M. Natural history and familial characteristics of isolated left ventricular non-compaction. Eur Heart J. 2005, 26, 187–192. [Google Scholar] [CrossRef] [PubMed]
© 2017 by the author. 2017 Oana Mirea1, Mihaela Berceanu, Anca Constantin, Mirela Mănescu, Georgică C. Târtea, Ionuț Donoiu1, Constantin Militaru1, Octavian Istrătoaie