Therapeutic Drug Monitoring and Methods of Quantitation for Carbamazepine
Abstract
:Introduction
Discussion
- General data
- 2.
- Therapeutic drug monitoring (TDM)
- -
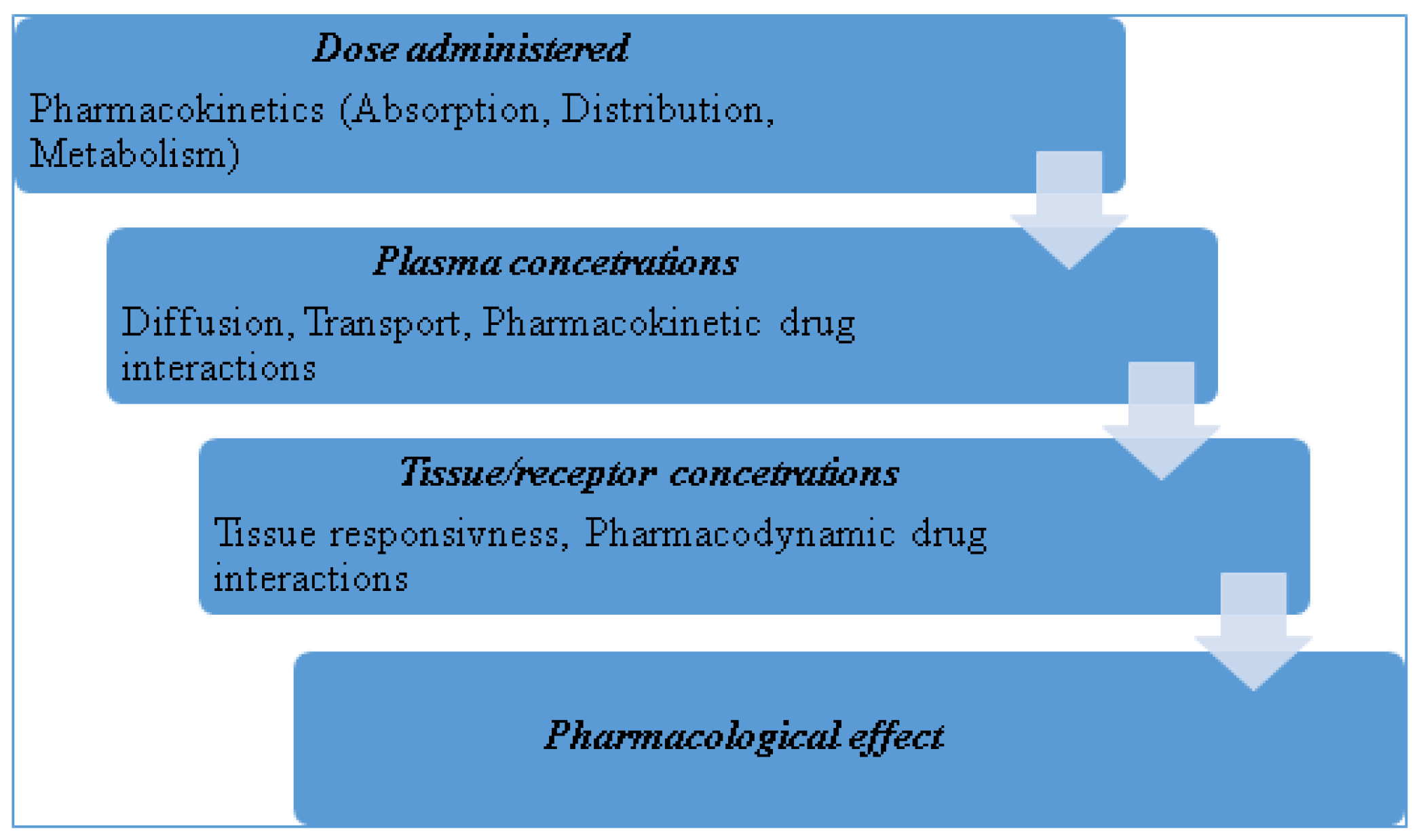
- The drug concentration in plasma must accurately reflect the concentration at the site of action (the receptor).
- -
- The drug concentration at the receptor should provide an accurate indication of the pharmacological response.
- Poor correlation existing between the dose given and the plasma concentration obtained in different patients (wide inter-individual pharmacokinetic variability).
- Good correlation existing between plasma
- concentration and pharmacological effect in different patients (low inter-individual pharmacodynamic variability); this also implies an established therapeutic range of plasma concentrations or a good relationship between plasma concentration and effect.
- Clinically relevant only for drugs that show significant toxic or undesirable effects at plasma concentrations only slightly above those required for useful effect (low therapeutic index).
- TDM is redundant for drugs where there is a better
- clinical marker of both the desired effect and any associated adverse effects.
- Treatment is expected to be long-term.
- 3.
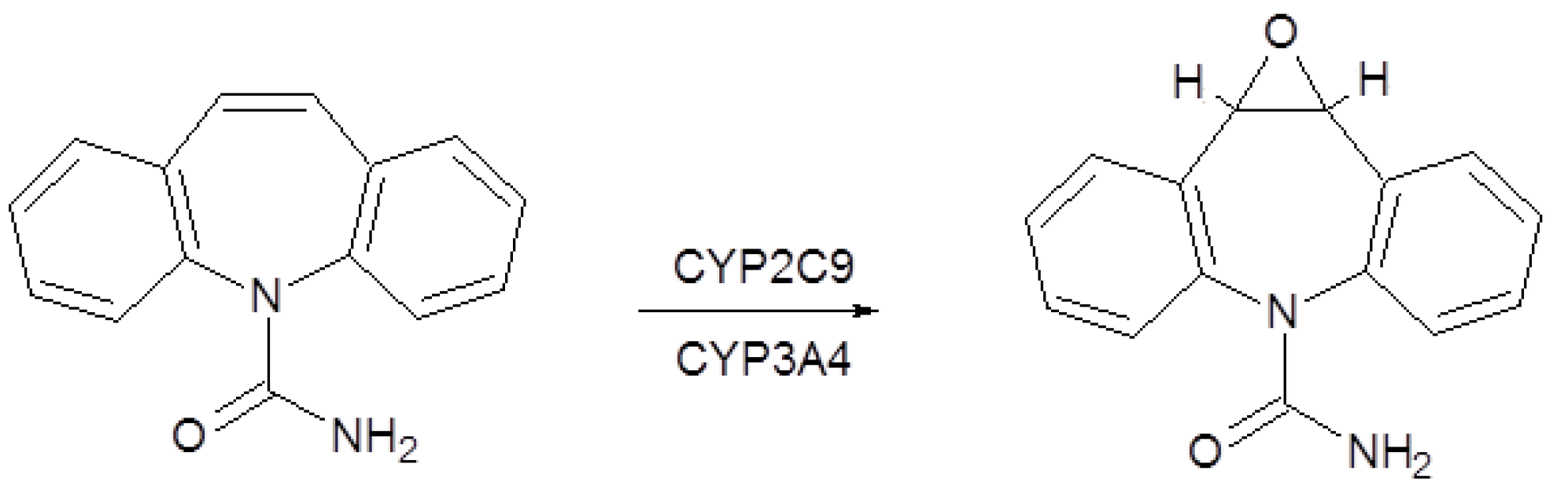
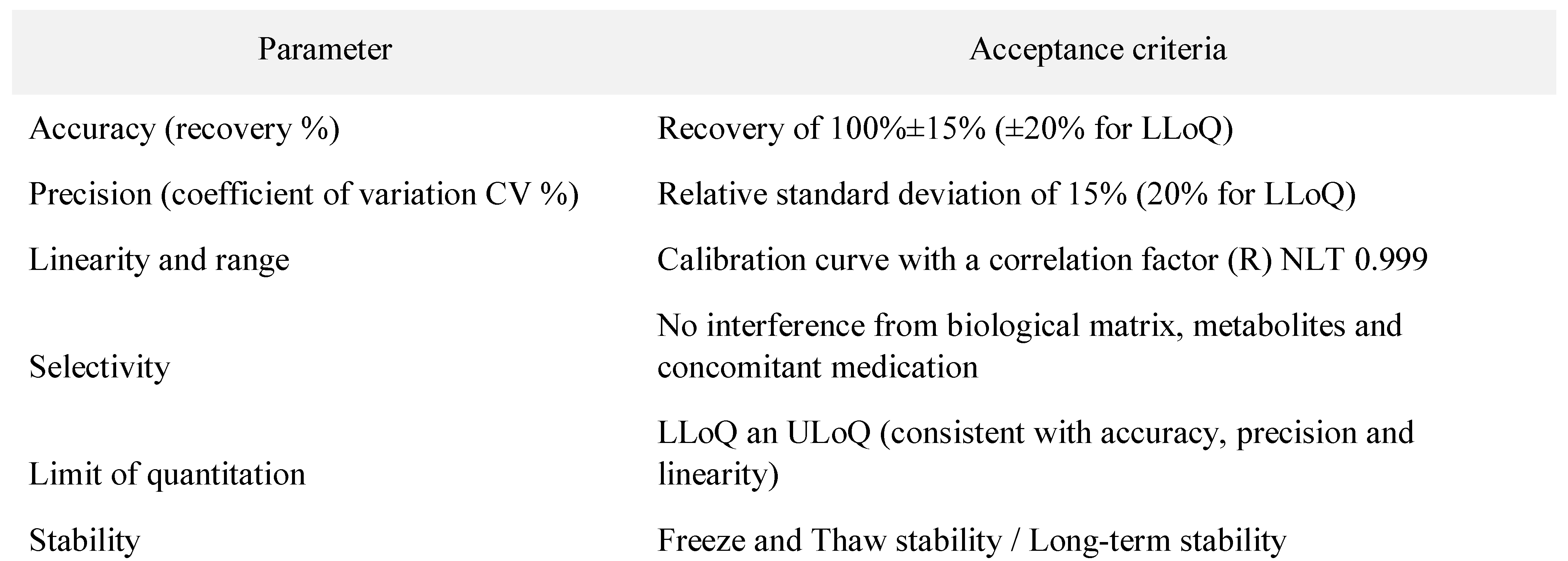
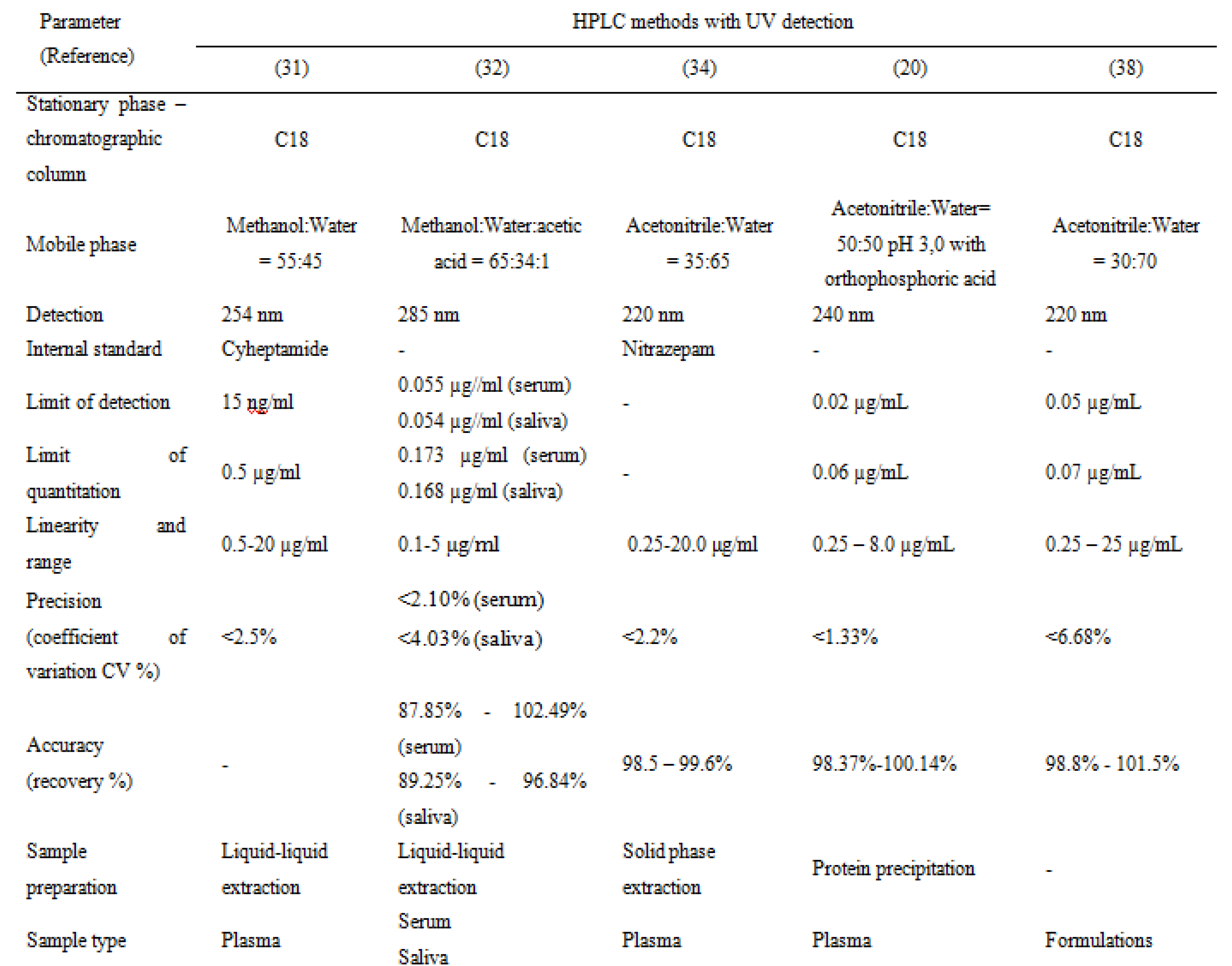
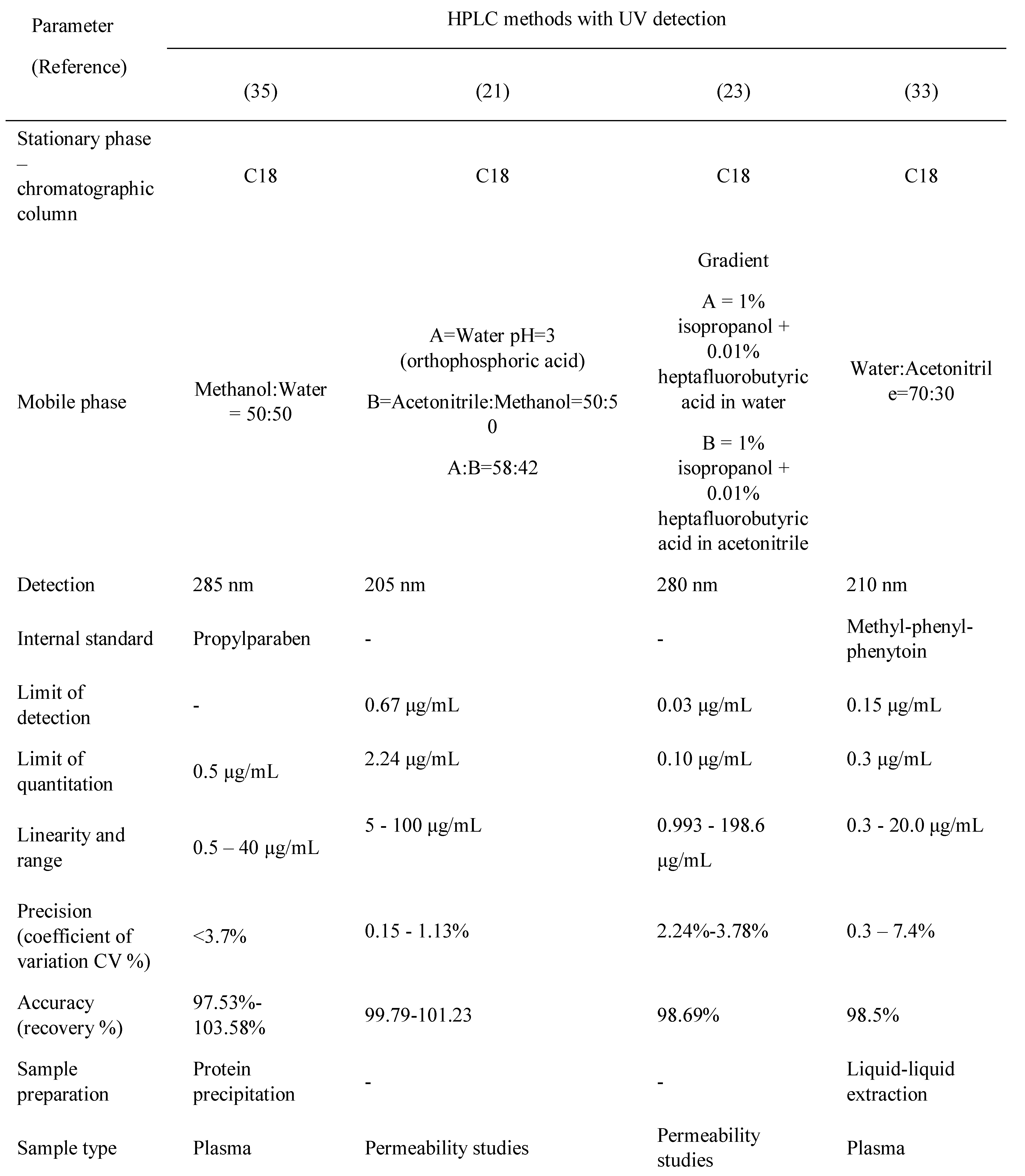
- Bioanalytical methods for determination of carbamazepine and metabolite
Conclusions
References
- Kang, J.Q. Defects at the crossroads of GABAergic signaling in generalized genetic epilepsies. Epilepsy Res. 2017, 137, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Magalhães, P.; Alves, G.; Llerena, A.; Falcão, A. Therapeutic Drug Monitoring of Fluoxetine, Norfluoxetine and Paroxetine: A New Tool Based on Microextraction by Packed Sorbent Coupled to Liquid Chromatography. J Anal Toxicol. 2017, 41, 631–638. [Google Scholar] [CrossRef] [PubMed]
- Pozzi, M.; Pineschi, R.; Bonanni, P.; Pellegri, A.; Clementi, E. Precipitation of Carbamazepine- Controlled Seizures Due to Low-Dose Risperidone in a Child: A Conspiracy to Unbalance Blood Electrolytes. J Clin Psychopharmacol. 2016, 36, 729–730. [Google Scholar] [CrossRef] [PubMed]
- Pohlmann-Eden, B.; Marson, A.G.; Noack-Rink, M.; Ramirez, F.; Tofighy, A.; Werhahn, K.J.; Wild, I.; Trinka, E. Comparative effectiveness of levetiracetam, valproate and carbamazepine among elderly patients with newly diagnosed epilepsy: subgroup analysis of the randomized, unblinded KOMET study. BMC Neurol. 2016, 16, 149. [Google Scholar] [CrossRef] [PubMed]
- Moagar-Poladian, S.; Folea, V.; Paunica, M. Competitiveness of EU member states in attracting EU funding for research and innovation. Romanian Journal of Economic Forecasting. 2017, 20, 150–167. [Google Scholar]
- Tolbert, D.; Cloyd, J.; Biton, V.; Bekersky, I.; Walzer, M.; Wesche, D.; Drummond, R.; Lee, D. Bioequivalence of oral and intravenous carbamazepine formulations in adult patients with epilepsy. Epilepsia 2015, 56, 915–923. [Google Scholar] [CrossRef] [PubMed]
- Gierbolini, J.; Giarratano, M.; Benbadis, S.R. Carbamazepine-related antiepileptic drugs for the treatment of epilepsy - a comparative review. Expert Opin Pharmacother. 2016, 17, 885–888. [Google Scholar] [CrossRef] [PubMed]
- Sitges, M.; Chiu, L.M.; Reed, R.C. Effects of Levetiracetam, Carbamazepine, Phenytoin, Valproate, Lamotrigine, Oxcarbazepine, Topiramate, Vinpocetine and Sertraline on Presynaptic Hippocampal Na(+) and Ca(2+) Channels Permeability. Neurochem Res. 2016, 41, 758–769. [Google Scholar] [CrossRef] [PubMed]
- Acikgoz, M.; Paksu, M.S.; Guzel, A.; Alacam, A.; Alacam, F. Severe Carbamazepine Intoxication in Children: Analysis of a 40-Case Series. Med Sci Monit 2016, 22, 4729–4735. [Google Scholar] [CrossRef] [PubMed]
- Marino, S.; Birnbaum, A.; Leppik, I.; Conway, J.M.; Musib, L.C.; Brundage, R.C.; Ramsay, R.E.; Pennell, P.B.; White, J.R.; Gross, C.R.; Rarick, J.O.; Mishra, U.; Cloyd, J.C. Steady-state Carbamazepine Pharmacokinetics following Oral and Stable-Labeled Intravenous Administration in Epilepsy Patients: Effect of Race and Sex. Clin Pharmacol Ther. 2012, 91, 483–488. [Google Scholar] [CrossRef] [PubMed]
- Baumann, P.; Hiemke, C.; Ulrich, S.; Gaertner, I.; Rao, M.; Eckermann, G.; Zernig, G. Therapeutic Monitoring of Psychotropic Drugs - An Outline of the AGNP- TDM Expert Group Consensus Guideline. Ther Drug Monit. 2004, 26, 167–170. [Google Scholar] [CrossRef] [PubMed]
- Bârcă, M.; Ilie, M.; Baconi, D.L.; Ciobanu, A.M.; Bălălău, D.; Burcea, G.T. Spectrofluorimetric methotrexate assay in human plasma. Farmacia 2010, 58, 95–10. [Google Scholar]
- Bălălău, C.; Voiculescu, Ș.; Motofei, I.; Scăunașu, R.V.; Negrei, C. Low Dose Tamoxifen as Treatment of Benign Breast Proliferative Lesions. Farmacia 2015, 63, 371–375. [Google Scholar]
- Kisanga, E.R.; Gjerde, J.; Guerrieri-Gonzaga, A.; Pigatto, F.; Pesci-Feltri, A.; Robertson, C.; Serrano, D.; Pelosi, G.; Decensi, A.; Lien, E.A. Tamoxifen and metabolite concentrations in serum and breast cancer tissue during three dose regimens in a randomized preoperative trial. Clin Cancer Res. 2004, 10, 2336–2343. [Google Scholar] [CrossRef] [PubMed]
- Vasile, R.D.; Baconi, D.; Hudiţă, C.; Bârcă, M.; Bălălău, C.; Ciobanu, A.M. Methadone plasma levels in heroin addict patients during substitution therapy. Farmacia; 2014, 62, 1202–1212. [Google Scholar]
- Baconi, D.L.; Stan, M.; Ebrahim, Z.A.J.; Tuchila, C.; Balalau, C. Determination of Tramadol in human plasma by HPLC with fluorescence detection. Journal of Mind and Medical Sciences 2016, 3, 55–64. [Google Scholar] [CrossRef]
- Vlăsceanu, A.M.; Petraru, C.; Baconi, D.; Ghica, M.; Arsene, A.; Popa, L.; Nicolae, A.; Drăgoi, C.; Pavalache, G. Quantitative relationships of urinary cotinine levels in smoking diabetic patients. Farmacia 2015, 63, 349–356. [Google Scholar]
- FDA Guidance for Industry - Bioanalytical Method Validation, 2013, Retrieved from FDA Guidances: http://www.fda.gov/Drugs/GuidanceComplianceReg ulatoryInformation/Guidances/default.htm.
- McMillin, G.A.; Juenke, J.M.; Tso, G.; Dasgupta, A. Estimation of Carbamazepine and Carbamazepine- 10,11-Epoxide Concentrations in Plasma Using Mathematical Equations Generated With Two Carbamazepine Immunoassays. Am J Clin Pathol. 2010, 133, 728–736. [Google Scholar] [CrossRef] [PubMed]
- Sultana, N.; Arayne, M.S.; Ali, S.N. An Ultra-Sensitive LC Method for the Simultaneous Determination of Paracetamol, Carbamazepine, Losartan and Ciprofloxacin in Bulk Drug, Pharmaceutical Formulation and Human Serum by Programming the Detector. Am J Anal Chem, 2013; 4, 24–33. [Google Scholar]
- Patil, S.; Kumar, L.; Kohli, G.; Bansal, A. Validated HPLC Method for Concurrent Determination of Antipyrine, Carbamazepine, Furosemide and Phenytoin and its Application in Assessment of Drug Permeability through Caco-2 Cell Monolayers. Sci Pharm. 2012, 80, 89–100. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.A.; Abd Al Haleem, E.N.; Khaleel, S.A.; Sallam, A.S. Protective effect of cardamonin against acetic acid-induced ulcerative colitis in rats. Pharmacol Rep. 2017, 69, 268–275. [Google Scholar] [CrossRef] [PubMed]
- Xie, W.; Qin, X.; Teraoka, I.; Gross, R.A. Comparison of retention behavior of oligolysine and oligoarginine in ion-pairing chromatography using heptafluorobutyric acid. Anal Bioanal Chem. 2013, 405, 9739–9746. [Google Scholar] [CrossRef] [PubMed]
- Yin, L.; Wang, T.; Shi, M.; Zhang, Y.; Zhao, X.; Yang, Y.; Gu, J. Simultaneous determination of ten antiepileptic drugs in human plasma by liquid chromatography and tandem mass spectrometry with positive/negative ion-switching electrospray ionization and its application in therapeutic drug monitoring. J Sep Sci. 2016, 39, 964–972. [Google Scholar] [CrossRef] [PubMed]
- Dzodic, P.; Zivanovic, L.; Protic, A.; Ivanovic, I.; Velickovic-Radovanovic, M.; Spasic, M.; Zivanovic, S. Development and validation of a solid phase extraction-HPLC method for the determination of carbamazepine and its metabolites, carbamazepine epoxide and carbamazepine trans-diol, in plasma. J Serb Chem Soc. 2012, 77, 1–21. [Google Scholar] [CrossRef]
- Powell, G.; Saunders, M.; Marson, A.G. Immediate- release versus controlled-release carbamazepine in the treatment of epilepsy. Cochrane Database Syst Rev 2010, 1, CD007124. [Google Scholar] [CrossRef] [PubMed]
- Mashayekhi, H.; Abroomand-Azar, P.; Saber-Tehrani, M.; Husain, S. Rapid Determination of Carbamazepine in Human Urine, Plasma Samples and Water Using DLLME followed by RP-LC. Chromatographia 2010, 71, 517–521. [Google Scholar] [CrossRef]
- Borowicz-Reutt, K.K.; Banach, M.; Piskorska, B. Mexiletine and its Interactions with Classical Antiepileptic Drugs: An Isobolographic Analysis. Neurochem Res. 2016, 41, 1185–1191. [Google Scholar] [CrossRef] [PubMed]
- Oh, E.K.; Ban, E.; Woo, J.S.; Kim, C.K. Analysis of carbamazepine and its active metabolite, carbamazepine-10,11-epoxide, in human plasma using high-performance liquid chromatography. Anal Bioanal Chem. 2006, 386, 1931–1936. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, A.; Rodrigues, M.; Falcao, A.; Alves, G. HPLC–DAD Method for the Quantification of Carbamazepine, Oxcarbazepine and their Active Metabolites in HepaRG Cell Culture Samples. Chromatographia 2016, 79, 581–590. [Google Scholar] [CrossRef]
- Mihaly, W.G.; Phillips, J.A.; Louis, W.J.; Vajda, F.J. Measurement of Carbamazepine and Its Epoxide Metabolite by High-Performance Liquid Chromatography, and a Comparison of Assay Techniques for the Analysis of Carbamazepine. Clin Chem. 1977, 23, 2283–2287. [Google Scholar] [CrossRef] [PubMed]
- Nicolae, A.C.; Arsene, A.L.; Vuță, V.; Popa, D.E.; Sîrbu, C.A.; Burcea Dragomiroiu, G.T.A.; Dumitrescu, I.B.; Velescu, B.Ș.; Gofiță, E.; Drăgoi, C.M. In vitro P-GP expression after administration of CNS active drugs. Farmacia. 2016, 64, 844–850. [Google Scholar]
- Sanches, C.; Lopez, K.; Omosako, C.; Bertoline, M.; Pereira, M.; Santos, S. Micromethod for Quantification of Carbamazepine, Phenobartital and Phenytoin in Human Plasma by HPLC-UV Detection for Therapeutic Drug Monitoring Application. Latin American Journal of Pharmacy. 2008, 27, 485–491. [Google Scholar]
- Zhu, Y.; Chiang, H.; Wulster-Radcliffe, M.; Hilt, R.; Wong, P.; Kissinger, C.B.; Kissinger, P.T. Liquid chromatography/tandem mass spectrometry for the determination of carbamazepine and its main metabolite in rat plasma utilizing an automated blood sampling system. J Pharm Biomed Anal. 2005, 38, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Mowafy, H.A.; Alanazi, F.K.; El Maghraby, G.M. Development and validation of an HPLC–UV method for the quantification of carbamazepine in rabbit plasma. Saudi Pharm J. 2012, 20, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Devandla, A.; Yamasani, M. Development and Validation of and UPLC Method for the Quantification of Carbamazepine in Intestinal Sac Samples. International Journal of Pharmacy and Biological Science. 2015, 5, 145–152. [Google Scholar]
- Guerrero Garduño, Ó.; González-Esquivel, D.F.; Escalante-Membrillo, C.; Fernández, Á.; Rojas-Tomé, I.S.; Jung Cook, H.; Castro, N. Comparison of a high- performance liquid chromatography method for quantification of carbamazepine with chemiluminescent microparticle immunoassay. Biomed Chromatogr. 2016, 30, 933–937. [Google Scholar] [CrossRef] [PubMed]
- Dzodić, P.L.j.; Zivanović, L.J.; Protić, A.D.; Zećević, M.L.; Jocić, B.M. Determination of carbamazepine and its impurities iminostilbene and iminodibenzyl in solid dosage form by column high-performance liquid chromatography. J AOAC Int. 2010, 93, 1059–1068. [Google Scholar] [CrossRef] [PubMed]
- Borhade, V.B.; Nair, H.A.; Hegde, D.D.; Barhate, C.R. Development and validation of HPTLC method for estimation of tacrolimus in formulations. Drug Dev Ind Pharm. 2009, 35, 440–448. [Google Scholar] [CrossRef]
- Zadbuke, N.; Shahi, S.; Jadhav, A.; Borde, S. Development and Validation of UV-Visible Spectrophotometric Method for Estimation of Carbamazepine in Bulk and Tablet Dosage Form. Int J Pharmacy and Pharmaceutical Sci. 2016, 8, 234–238. [Google Scholar]
- Tambe, H.; Mulgund, S. UV Spectrophotometric Estimation of Carbamazepine in Bulk and Tablet Dosage Form Using Area Under Curve Method. World Journal of Pharmacy and Pharmaceutical Sciences. 2015, 4, 1200–1206. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
 |
 |
 |
 |
 |
© 2017 by the author. 2017 Cristian Tuchila, Daniela L. Baconi, Cristina D. Pirvu, Denisa O. Balalau, Ana M. Vlasceanu, Miriana Stan, Cristian Balalau
Share and Cite
Tuchila, C.; Baconi, D.L.; Pirvu, C.D.; Balalau, D.O.; Vlasceanu, A.M.; Stan, M.; Balalau, C. Therapeutic Drug Monitoring and Methods of Quantitation for Carbamazepine. J. Mind Med. Sci. 2017, 4, 100-114. https://doi.org/10.22543/7674.42.P100114
Tuchila C, Baconi DL, Pirvu CD, Balalau DO, Vlasceanu AM, Stan M, Balalau C. Therapeutic Drug Monitoring and Methods of Quantitation for Carbamazepine. Journal of Mind and Medical Sciences. 2017; 4(2):100-114. https://doi.org/10.22543/7674.42.P100114
Chicago/Turabian StyleTuchila, Cristian, Daniela L. Baconi, Cristina D. Pirvu, Denisa O. Balalau, Ana M. Vlasceanu, Miriana Stan, and Cristian Balalau. 2017. "Therapeutic Drug Monitoring and Methods of Quantitation for Carbamazepine" Journal of Mind and Medical Sciences 4, no. 2: 100-114. https://doi.org/10.22543/7674.42.P100114
APA StyleTuchila, C., Baconi, D. L., Pirvu, C. D., Balalau, D. O., Vlasceanu, A. M., Stan, M., & Balalau, C. (2017). Therapeutic Drug Monitoring and Methods of Quantitation for Carbamazepine. Journal of Mind and Medical Sciences, 4(2), 100-114. https://doi.org/10.22543/7674.42.P100114