Abstract
Objectives. The experience accumulated in the last two years shows that the prevention of COVID-19 in people with comorbidities (protective measures, vaccination, etc.) still remains a public health priority. In this context, the aim of our study was to perform a retrospective, observational study in order to assess the time-to-death and risk factors of mortality among COVID-19 patients. Materials and Methods. The study was conducted on 177 patients admitted to Oradea Emergency County Hospital, Bihor, Romania, between October and December 2021. Inclusion criteria were patients over 18 years positive for COVID-19 in upper respiratory tract samples using real-time PCR test. Exclusion criteria were pregnant women, age <18 years, and patients with incomplete records at admission. Results. The mortality rate was assessed in correlation with the most prevalent comorbidities such as diabetes, cardiovascular diseases, hypertension, chronic kidney disease, and chronic pulmonary diseases, either alone or associated. During hospitalization, an aggravated health condition was noticed for 71 patients (40.11%). Among them, 47 patients were transferred to the intensive care unit (66.20%) due to severe respiratory failure, aggravation of associated diabetes and/or other associated comorbidities. Ventilation support was necessary in 122 cases (68.63%). The average survival time was 8.66 days. In conclusion, we found that the most prevalent comorbidities were cardiovascular diseases, being the major risk factor for mortality or aggravation after hospitalization. Its association with diabetes caused a risk of death 2.1 times higher than in patients without comorbidities. Based on Kaplan–Meier survival analysis, we found that the in-hospital survival rate was significantly higher in females compared to males (50.52% vs. 33.75%).
Introduction
Globally, based on the World Health Organization (WHO) daily report, the total number of infections during the COVID-19 pandemic reached in December 2021 640.395.651 confirmed cases, including 6.618.579 deaths [1]. In Europe, 265.511.765 cases were confirmed, and 2.137.157 deaths were reported to WHO. The overall infection fatality rate has been estimated to be around 0.5–1%, with higher rates among those aged 60 or older [2,3,4].
Previous studies revealed differences in rates of severe SARS-CoV-2 infection, depending on the prevalence of underlying medical conditions and comorbidities, clinical severity, access to care, and quality of care [5,6], being well-known that chronic diseases share several standard features with infectious disorders, such as the proinflammatory state, and the attenuation of the innate immune response. Based on these findings, it is generally accepted that risks increase with age, but nowadays there are strong pieces of evidence demonstrating increased risks associated with various health conditions, including chronic kidney disease (CKD), diabetes, lung and liver diseases, cardiovascular disease (CVD), hypertension, obesity, immunodeficiency, or certain disabilities [7,8,9,10]. The experience accumulated in the last two years provides sufficient arguments showing that preventing COVID-19 in populations with associated conditions must be a public health priority, along with conjugate efforts for the uptake of vaccines. Hence, careful evaluation and management of underlying conditions among patients with COVID-19 can help avoid the risk of severe illness. The predictive risk factors for critical illness and death might be very useful in the future, as the recent pandemic experience has shown us that while the number of cases increased, the admission and discharge criteria were changed to accommodate the service to those who need it most [11,12].
In Romania there is a lack of epidemiological studies related to the clinical progress of COVID-19 patients examining survival outcomes, patient’s socio-demographic characteristics, and predictive risk factors for critical illness and death causes. As reported on 21 August 2022, a total of 3.186.995 confirmed cases (2065 newly confirmed) and 66.490 deaths were recorded in Romania, the incidence cumulative rate/1000 inhabitants being 4.9. Better quantification of the relation between comorbidities and different outcomes is essential.
The aim of our study was to perform a retrospective, observational study based on medical records of confirmed COVID-19 cases hospitalized at Emergency County Hospital Oradea, Bihor, in NV Romania, over a period of three months, from October to December 2021. The socio-demographic data and clinical features including patients’ area of provenance (rural versus urban), age and gender, associated pathologies, health condition at admission time, vaccination status, average hospitalization time, ventilation support, and death rate are analyzed in order to assess the time-to-death and risk factors of mortality among COVID-19 patients.
Materials and Methods
Study design and participants
An observational cohort study was conducted on a total number of 177 patients, hospitalized at Emergency County Hospital Oradea, Bihor, in North West (NW) Romania, over three months from October to December 2021, which corresponds to a high incidence of COVID-19 infections. Inclusion criteria were: age >18 and patients positive for COVID-19 test based on virus detection for the RNA/antigen in the upper respiratory tract specimens (nasopharyngeal and oropharyngeal) using real-time PCR test. Exclusion criteria were: pregnant women, age<18 years, and patients with incomplete records at admission. All patient data were anonymized. The demographic characteristics examined included age, sex, urban and rural area of provenance, medical history, and vaccination status, all of this information being provided by the patients at admission.
Variables and data sources
In all subjects, data on baseline comorbidities and COVID-19–related complications were collected. Clinical data of patients were extracted from the hospital records. The prevalence of associated pathologies was assessed, along with the illness severity and health condition at admission time. Moreover, the ventilation support was evaluated in terms of hours (ranging between 24-96 hours). The severity of symptoms on admission was categorized (such as: mild, moderate, severe, or critical), while the patients’ evolution during hospitalization was recorded, along with the necessity for intensive care at admission or during hospitalization. The risk of death in unvaccinated patients was compared to vaccinated ones.
Outcomes
The major outcomes after admission were the discharges following recovery or death. The mortality rate was assessed in correlation with the most prevalent comorbidities such as diabetes, cardiovascular diseases, hypertension, chronic kidney disease, and chronic pulmonary diseases, either alone or in association. Kaplan–Meier survival analysis was applied to compare mortality rates between genders.
Statistical analysis
Statistical analysis was generated using the Statistical Package for the Social Sciences (SPPS), version 20. Descriptive statistic was performed including means, standard deviations, and tests of statistical significance by applying t-test and chi-square test. The statistical significance was considered for p-values < 0.05. In clinical trials, the investigator is often interested in the time until participants in a cohort study present a specific event such as death. The Kaplan-Meier curve is used to estimate the survival function from data that are censored, truncated, or have missing values. It shows the probability that a subject will survive up to time t. The curve is constructed by plotting the survival function against time. In order to calculate the relative risk, we used Med Calc Software (©2022 Med Calc Software Ltd.). Relative risk is a ratio of the probability of an event occurring in the exposed group versus the probability of the event occurring in the non-exposed group.
Ethical declaration
The study was approved by the institutional review board and Ethical Council of the Emergency County Hospital Oradea, Bihor (no. 33274/06.10.2022), and the research was conducted in compliance with the Declaration of the World Medical Association of Helsinki.
Results
Patients’ characteristics and health condition at admission time
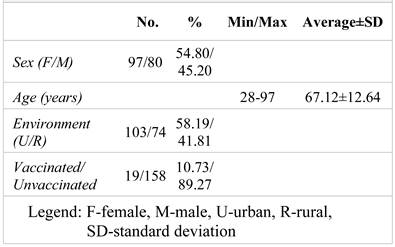
Among 177 individuals meeting our study criteria, 97 (54.80%) were female and 80 (45.20%) were male, with an average age of 67 (67.12±12.64), significantly higher for females compared to males (p=0,013). The patients’ age ranged between 28-97 years old, but the majority were within the age group of 51-70 years (50.85%). The overall characteristics of the study group are presented in Table 1.

Table 1.
The overall characteristics of the patients included in the study
In terms of area of provenance, the majority of hospitalized patients came from the rural area (58.19%), both males and females (56.70% vs 60.00%, p=0.002), as summarized in Table 2, along with the clinical details. In our study group, a very small percentage of patients were vaccinated against COVID-19 (10.73%), which corresponded to a much more severe evolution of them.
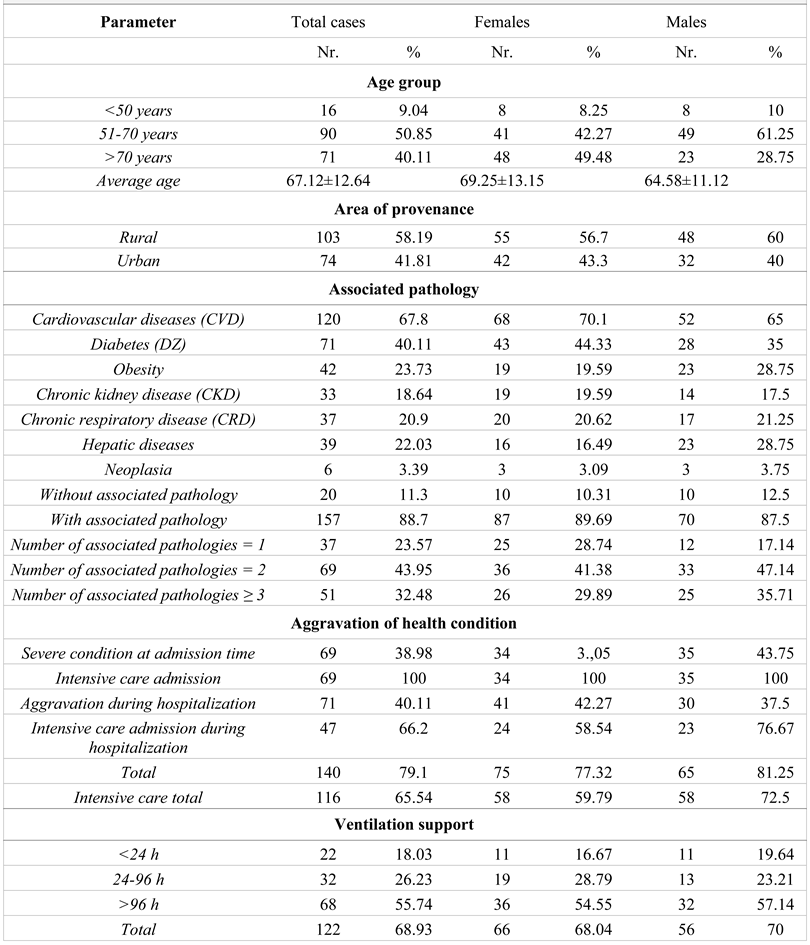
Table 2.
Demographic data of the patients, associated pathology, and evolution of health condition
The most prevalent comorbidity was CVD (67.80%), the percentage being higher (but insignificant) for females compared to males (70.10% vs 65.00%, p=0.471). Other associated conditions included diabetes (40.11%) with higher incidence for females than males (44.33% vs 35.00%, p=0.209), while obesity, chronic liver disease (CLD), and pulmonary diseases (CRD) revealed a lower prevalence, between 20-24% (23.73%, 22.03% and 20.90% respectively), more frequently present in males (28.75% vs 19.59%, p=0.155; 28.75% vs 16.49%, p=0.050; 21.25% vs 20.62%, p=0.919). Overall, by analyzing the presence of different associated pathologies, we noticed only 11.30% of patients lack any associated condition, the percentage being higher for males, but not significant (12.50% vs 10.31%, p=0.648). Among 157 patients with different comorbidities, most of them presented 2 associated diseases (43.95%), the most frequent association being diabetes and CVD (34.78%). More than 40% of all patients were admitted emergently or urgently, requiring intensive care facilities (38.98%), the percentage was higher for males (43.75% vs 35.05%, p=0.239). All of these patients presented with acute respiratory failure and met criteria for requiring ventilation with which they were subsequently treated. In 47 cases, the aggravation of the associated pathologies was noticed, especially related to CVD (23 cases), CVD associated with diabetes (17 cases), and diabetes alone (10 cases). Aggravation of CKD was also noticed in 7 cases.
Patient’s evolution and the most common acute complications
During hospitalization, an aggravated health condition was noticed for 71 patients (40,11%), with a higher value for females (42.27% vs 37.50%, p=0.521), but no risk for aggravation in the case of females (R2=0.127). Among them, 47 patients were transferred to the intensive care unit (66.20%) due to severe respiratory failure (11 cases), aggravation of diabetes associated with CVD (11 cases), aggravation of CVD (9 cases), unbalanced diabetes (8 cases), aggravation of CKD (5 cases) and advanced degradation of hepatic function (3 cases). The ventilation support was necessary in 122 cases (68.63%), the percent being insignificantly higher in males compared to females (70.00% vs 68.04%, p=0.780). Among these patients, 55.74 % were provided with ventilation support for more than 96 hours, the percentage being higher in males compared to females (57.14% vs 54.55%, p=0.731).
In-hospital mortality
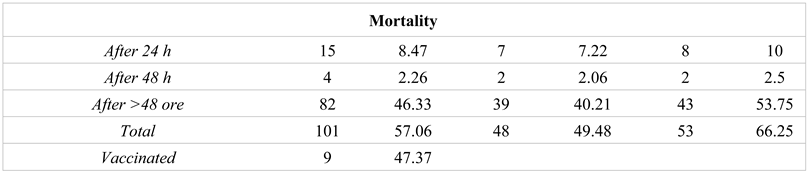
A percent of 57.06% for in-hospital mortality was calculated, significantly higher in males compared to females (66.25% vs 49.48%, p=0.025). At 24 hours after admission, the mortality was 8.47%, significantly higher in males (10.00% vs 7.22%, p=0.510). All 69 patients admitted with severe illness died during hospitalization, which means that 68.32% of deaths were due to delayed hospitalization. The average age of death was 67.83 years lower for males (66.53 vs 69.27, p=0.218), while the risk of mortality was 1.4 higher in males compared to females (R2=1.366, p=0.017). Mortality in vaccinated patients was 47.37%, lower but not significant percentage than in non-vaccinated ones (58.23%, p=0.368). The risk of death is 1.2 times higher in unvaccinated patients compared to vaccinated ones (R2=1.229, 95%CI: 0.752-2.011, z=0.822, p=0.411).
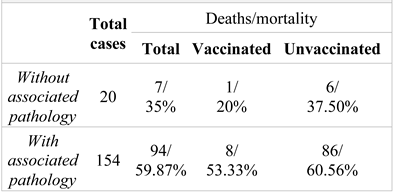
Among vaccinated patients without associated pathology, deaths represented 20.00%, which is lower than in the non-vaccinated ones (37.50%, p=0.648), while in those with associated pathology, the percentages were 53.33% vs 60.56% (p=0.588), as presented in Table 3. The risk of death in patients without associated pathology is 1.5 times higher for unvaccinated patients compared to vaccinated ones (R2=1.500, 95%CI: 0.245-9.179, z=0.439, p=0.661). In the patients with comorbidities, there is a higher risk of death for the unvaccinated ones compared to the vaccinated (R2=1.136, 95%CI: 0.695-1.857, z=0.507, p=0.613).
Table 3.
In-hospital mortality and vaccination status of patients with and without associated pathology
Comparing the mortality among the patients with and without any associated pathologies, a percent of 59.87% was noticed for the first ones, significantly higher compared to the patients without comorbidities (35.00%, p=0.035), as presented in Table 3 and Table 4. Overall, the risk of death was 1.7 times higher in patients with associated pathologies (R2=1.744, p=0.074).
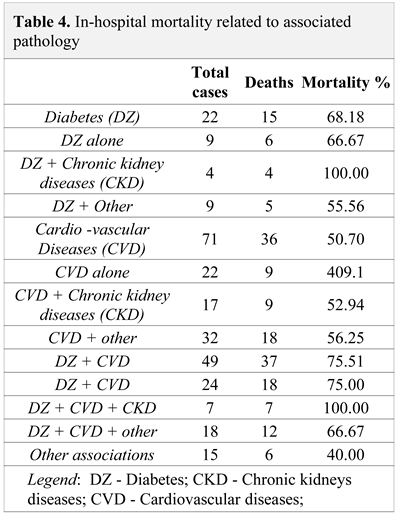
Table 4.
In-hospital mortality related to associated pathology
The highest mortality was recorded among the patients with diabetes associated with CVD (75.51%), but insignificantly higher compared to patients with diabetes without CVD (50.70%, p=0.006) or other associated diseases (40.00%, p=0.011). An important observation is the 100% mortality for the patients with CKD associated with diabetes, with or without CVD (Table 4). Compared to patients without any comorbidities, the risk of death is 1.9 times higher in patients with diabetes (R2=1.948, p=0.048), 1.5 times higher in those with CVD (R2=1.449, p=0.256) and 2.2 times higher in patients with diabetes associated with CVD. Also, we noticed a risk of death 1.2 times higher in patients with CVD compared to patients with no comorbidities (R2=1.169, p=0.695), while the association between CVD and CKD results in increasing the risk of death to 1.5 (R2=1.513, p=0.277). Moreover, the association between diabetes and CVD caused a risk of death 2.1 times higher than in patients without comorbidities R2=2.143, p=0.020), while the triple association between CVD, diabetes, and CKD resulted in a 2.9 times higher risk of mortality (R2=2.857, p=0.001).
In-hospital survival (40 days follow-up)
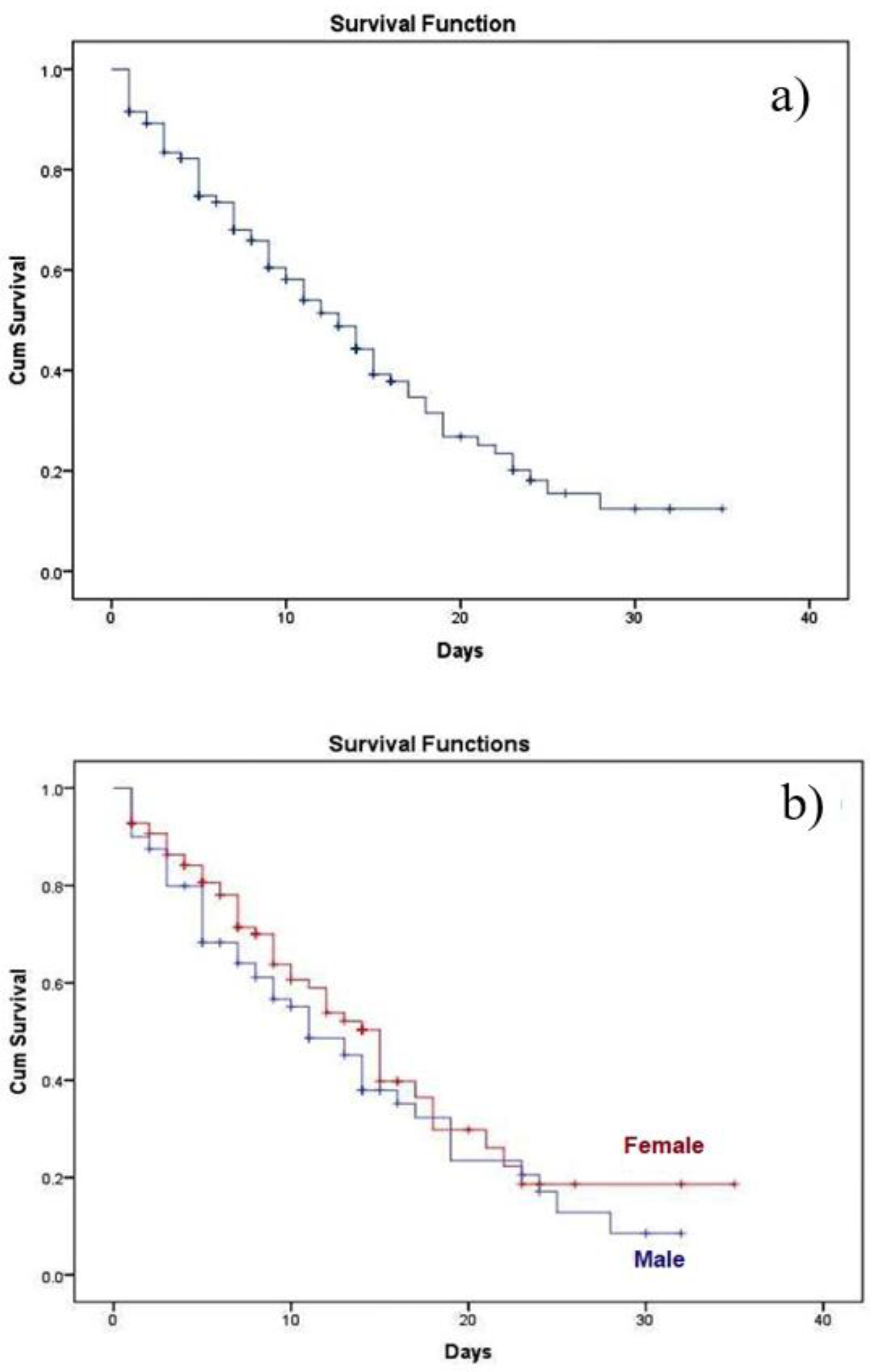
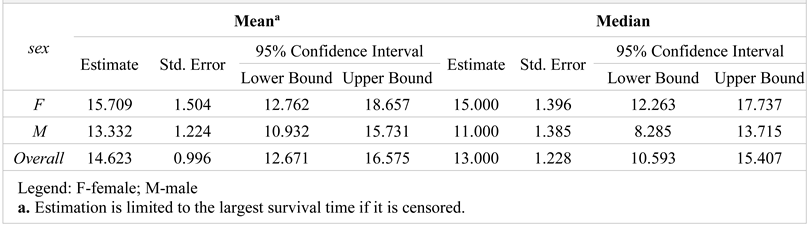
While the hospitalization time was between 1-35 days (average 9.66±7.33 days), we noticed 42.94% survival after 35 days, significantly higher in females compared to males (50.52% vs 33.75%). The average survival time was 8.66 days, insignificantly lower for females compared to males (8.54 days vs 8.77 days, p=0.861), as can be seen in Figure 1 (a, b), while means and medians for survival time are presented in Table 5, along with the calculated confidence interval.
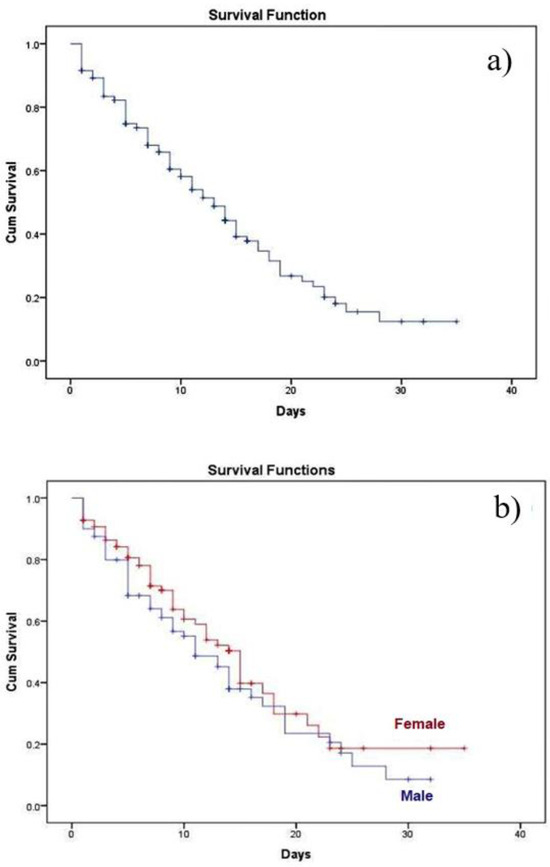
Figure 1.
Kaplan-Meier survival function: a) general; b) depending on the gender
Table 5.
Means and medians for survival time
Discussions
This retrospective study describes the basic demography, comorbidities, health condition at admission time, average hospitalization time, ventilation support, and death rate collected from a single center located in NW Romania, in order to assess the clinical outcome of COVID-19 patients focusing on the main risk factors of mortality, clinical-evolutionary particularities and survival analysis.
The most prevalent comorbidity in our cohort was cardiovascular disease (67.80%), being the major risk factor for mortality or aggravation after hospitalization, requiring intensive care facilities. The second associated condition in our cohort was diabetes (40.1%), the result being not surprising as it is well-known that the risk of infections is further increased with poorer glycemic values, as hyperglycemia, including the resulting glycosuria, increases the virulence of certain pathogens [13].
According to Landstra et al. [14], severe SARS-CoV-2 infection and its associated hyperinflammation present an indirect negative effect on insulin target tissues, and a direct negative effect on pancreatic b-cells resulting in hyperglycemia. On the one hand, diabetes and its associated comorbidities increase the risk of a more severe course of COVID-19 and increase mortality [15]. According to a study published by Wu Z et al [16] which included a total of 72.314 patients from China, the mortality rate was 7.3% among the diabetic patients (both type 1 and type 2 diabetes) infected with SARS-CoV-2 virus. In our study, the most frequent association among COVID-19 patients was between diabetes and CVD (34.78%). Actually, The American Heart Association (AHA) considers diabetes one of the seven major controllable risk factors for cardiovascular disease (CVD). A close link exists between diabetes and CVD, and cardiovascular risk factors such as obesity, hypertension, and dyslipidemia are common in patients with DM, placing them at increased risk for cardiac events [17]. In related literature and earlier research studies underlying diseases that increase the mortality rate in patients who acquired COVID-19, it was noticed that cardiac disease and diabetes were the most significant risk factors [18,19]. In our study, more than 40% of patients from this category required intensive care facilities and ventilation support, the main clinical manifestation being acute respiratory distress syndrome, while some of the clinical manifestations that are not typical might appear first, predicting COVID-19 [20].
Other comorbidities noticed in our cohort were obesity (23.73%), chronic liver disease (CLD) (22.03%), chronic respiratory diseases (CRD) (20.90%), and chronic kidney diseases (CKD) (18.64%). The potential mechanisms for the effect of obesity on COVID-19 length of hospitalization or severity have been extensively studied reporting that obesity altered lung physiology, reduced lung volumes, and subsequently induced abnormal ventilation and perfusion distribution. Moreover, it could induce hyperinsulinemia and insulin resistance [21]. On the other hand, according to a meta-analysis conducted by Ramya Nagarajan et al [22], the risk of COVID-19 severity and death was twice as high among CLD patients than among non-CLD patients. The impact of CRD on severe COVID-19 and the risk of death is considered controversial according to a Nationwide Retrospective Cohort Study of 39.420 cases conducted by Wei-jie Guan et al [23]. In this study, patients with CRD were not associated with a higher risk of mortality for COVID-19 compared with those without CRD. Moreover, neither chronic obstructive pulmonary disease nor asthma was significantly associated with the risk of death within 30 days after hospitalization.
There are related studies showing that dialysis, organ transplantation, and CKD represent three of the four comorbidities associated with the highest mortality risk from COVID-19 [24,25]. They highlighted that hypertension is not an independent risk factor for COVID-19 death, in contrast to renal disease. To date, it is unclear if there is a direct mechanism of kidney involvement in COVID-19, but however, it includes a cytokine storm syndrome either through sepsis pathways or direct damage of renal tubular cells [26]. A meta-analysis with a pooled subject of 18.822 patients showed that the presence of diabetes in CKD patients with COVID-19 was associated with an increased risk of mortality [27]. It was concluded that patients with CKD are more susceptible to bacterial and viral infections due to the alterations of the immune system [28] caused by excessive levels of proinflammatory cytokines and oxidative stress.
We observed in our research that the association between diabetes and CVD caused a risk of death 2.1 times higher than in patients without comorbidities, while the association between CVD, diabetes, and chronic kidney diseases resulted in a 2.9 times higher risk of mortality. A percent of 100% in-hospital mortality related to CVD, diabetes, and CKD-associated pathology was recorded. Overall, the mortality among the patients with associated pathologies was 59.87% compared to 35.00% for the patients without comorbidities. In a similar study, conducted by Irawaty Djaharuddin et al [29], more than half of patient’s death (52.56%) due to COVID-19 presented more than two comorbidities, while the rest had only one.
In our study group, a very small percentage of patients were vaccinated against COVID-19 (10.73%). Considering the discrepancy, we also noticed an important difference between the mortality among unvaccinated versus vaccinated patients, with or without associated pathology, respectively 60.56% versus only 53.33% (patients with comorbidities) and 37.50% versus 20% (without comorbidities). An explanation resides from the clinical features of the admitted patients [30], especially those with aggravated status requiring direct admission to intensive care units, as a consequence of tardive presentation at the emergency unit. Another particular feature of our study population is represented by the high number of patients (68.63%) requiring ventilation support for more than 96 h (55.74%).
Overall, the novelty of our study consists in describing the patients’ profile, starting with clinical status at admission time, and following the clinical-evolutionary particularities and survival analysis during hospitalization. While the standard medical care and treatment were adequately applied, an aggravated health condition progressed for 40.11% of the total of admitted patients. Thus, another advantage of our study is the evaluation of the COVID-19 severity for the unvaccinated.
Our study has some limitations, the data being collected from a single hospital, within a relatively narrow time frame and may not represent be generalized for the entire population. In addition, it is based on a retrospective analysis of patient records, and hence, it may lack some additional factors that may predict variation in survival probabilities (such as treatment-related factors). Medications were not included in the dataset, and hence, we could not evaluate the specific effects on patient outcomes or any influence over the received antiviral-tailored therapy during hospitalization.
The explanation for the small size population included in our study is related to the fact that, during the pandemic, only a few hospitals in Bihor County were dedicated to the treatment of COVID patients. In this context, Oradea County Emergency Clinical Hospital decided to dedicate 20 beds for emergency admission and treatment of adults COVID-19 positive, with severe forms, requiring admission in the intensive care unit. Besides them, this special COVID-19-section admitted also patients already hospitalized in all the clinical departments (neurology, neurosurgery, cardiology, diabetology, orthopedics, surgery, urology, maxillofacial, otorhinolaryngology, ophthalmology) infected with the SARS-COV 2 virus during hospitalization, which explains the severity of the associated infection.
Conclusions
The most prevalent comorbidity in COVID-19 patients admitted to a tertiary center in North West Romania was cardiovascular disease. Also, it is the major risk factor for mortality or aggravation after hospitalization, requiring intensive care facilities. The association between diabetes and CVD caused a risk of death 2.1 times higher than in patients without comorbidities. In patients with comorbidities, we observed a higher risk of death for the unvaccinated ones, which represent the majority of our study population. Based on Kaplan–Meier survival analysis, we found that the in-hospital survival rate was significantly higher in females compared to males (50.52% vs 33.75%).
Our data might help the healthcare sector to guide and target the vulnerable populations assessing the risk of deterioration in the future, in the event of similar respiratory viruses. As the prevalence of chronic diseases is increasing year by year, targeted public health vaccination interventions must be adopted to protect this vulnerable group, prioritizing them for future antiviral interventions.
Contributions
M.S.P. and S.C. collected and analyzed the data and drafted the manuscript. M.S.P. designed the project. M.S.P., L.P., R.A.S, A.P.S., C.T., and S.C. revised the manuscript. All authors have read and agreed to the published version of the manuscript.
Compliance with ethical standards
Any aspect of the work covered in this manuscript has been conducted with the ethical approval of all relevant bodies and that such approvals are acknowledged within the manuscript. The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (Ethics Committee) of Emergency County Hospital Oradea, Bihor (no. 33274/06.10.2022). The data supporting the reported results can be found in the medical archive of Emergency County Hospital Oradea, Bihor.
Conflict of interest disclosure
There are no known conflicts of interest in the publication of this article. The manuscript was read and approved by all authors.
Funding
This research was funded by the University of Oradea, Romania.
References
- Allan, M.; Lièvre, M.; Laurenson-Schafer, H.; et al. The World Health Organization COVID-19 surveillance database. Int J Equity Health. 2022, 21, 167, Published 2022 Nov 23. [Google Scholar] [CrossRef]
- Mallapaty, S. How deadly is the coronavirus? Scientists are close to an answer. Nature. 2020, 582, 467–468. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, A.; Nardi, C.; Oberije, C.; Lambin, P. Knowledge Graphs for COVID-19: An Exploratory Review of the Current Landscape. J Pers Med. 2021, 11, 300. [Google Scholar] [CrossRef]
- Nagarajan, P.; Vetrivel, A.; Kumar, J.; Howlader, A.; Rangarajalu, K.; Sabapathy, S.K.; Gopal, M.; Kumar, S. SARSCoV-2 Omicron (B.1.1.529) variant: structural features, biological characteristics, impact on scientific research, general precautions and protective procedures; a systematic review. J Mind Med Sci. 2022, 9, 224–235. [Google Scholar] [CrossRef]
- Yang, J.; Zheng, Y.; Gou, X.; Pu, K.; Chen, Z.; et al. Prevalence of comorbidities and its effects in patients infected with SARS-CoV-2: a systematic review and meta-analysis. Int J Infect Dis. 2020, 94, 91–95. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020, 395, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Adab, P.; Haroon, S.; O'Hara, M.E.; Jordan, R.E. Comorbidities and covid-19. BMJ. 2022, 377, o1431, Published 2022 Jun 15. [Google Scholar] [CrossRef]
- Kaso, A.W.; Agero, G.; Hurissa, Z.; et al. Survival analysis of COVID-19 patients in Ethiopia: A hospital-based study. PLoS One. 2022, 17, e0268280, Published 2022 May 9. [Google Scholar] [CrossRef]
- Rasmi, Y.; Saavedra, L.P.J.; Cozma, M.A.; et al. Laboratory findings in COVID-19-alterations of hematological, immunological, biochemical, hormonal and other lab panels: a narrative review. J Mind Med Sci. 2022, 9, 38–55. [Google Scholar] [CrossRef]
- Rosenthal, N.; Cao, Z.; Gundrum, J.; Sianis, J.; Safo, S. Risk Factors Associated With In-Hospital Mortality in a US National Sample of Patients With COVID-19. JAMA Netw Open. 2020, 3, e2029058, Published 2020 Dec 1. [Google Scholar] [CrossRef]
- Kompaniyets, L.; Pennington, A.F.; Goodman, A.B.; et al. Underlying Medical Conditions and Severe Illness Among 540,667 Adults Hospitalized With COVID-19, March 2020-March 2021. Prev Chronic Dis. 2021, 18, E66. [Google Scholar] [CrossRef] [PubMed]
- Emanuel, E.J.; Persad, G.; Upshur, R.; et al. Fair Allocation of Scarce Medical Resources in the Time of Covid-19. N Engl J Med. 2020, 382, 2049–2055. [Google Scholar] [CrossRef] [PubMed]
- Critchley, J.A.; Carey, I.M.; Harris, T.; DeWilde, S.; Hosking, F.J.; Cook, D.G. Glycemic Control and Risk of Infections Among People With Type 1 or Type 2 Diabetes in a Large Primary Care Cohort Study. Diabetes Care. 2018, 41, 2127–2135. [Google Scholar] [CrossRef]
- Landstra, C.P.; de Koning, E.J.P. COVID-19 and Diabetes: Understanding the Interrelationship and Risks for a Severe Course. Front Endocrinol (Lausanne). 2021, 12, 649525. [Google Scholar] [CrossRef] [PubMed]
- Barron, E.; Bakhai, C.; Kar, P.; et al. Associations of type 1 and type 2 diabetes with COVID-19-related mortality in England: a whole-population study. Lancet Diabetes Endocrinol. 2020, 8, 813–822. [Google Scholar] [CrossRef]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases From the Chinese Center for Disease Control and Prevention. JAMA. 2020, 323, 1239–1242. [Google Scholar] [CrossRef]
- Leon, B.M.; Maddox, T.M. Diabetes and cardiovascular disease: Epidemiology, biological mechanisms, treatment recommendations and future research. World J Diabetes. 2015, 6, 1246–1258. [Google Scholar] [CrossRef]
- Sanyaolu, A.; Okorie, C.; Marinkovic, A.; et al. Comorbidity and its Impact on Patients with COVID-19. SN Compr Clin Med. 2020, 2, 1069–1076. [Google Scholar] [CrossRef]
- Alkhemeiri, A.; Al Zaabi, S.; Lakshmanan, J.; El-Khatib, Z.; Awofeso, N. COVID-19 Case Management Outcomes Amongst Diabetes and Hypertensive Patients in the United Arab Emirates: A Prospective Study. Int J Environ Res Public Health. 2022, 19, 15967, Published 2022 Nov 30. [Google Scholar] [CrossRef]
- Baj, J.; Karakuła-Juchnowicz, H.; Teresiński, G.; et al. COVID-19: Specific and Non-Specific Clinical Manifestations and Symptoms: The Current State of Knowledge. J Clin Med. 2020, 9, 1753, Published 2020 Jun 5. [Google Scholar] [CrossRef]
- Yu, P.; Tan, Z.; Li, Z.; et al. Obesity and clinical outcomes in COVID-19 patients without comorbidities, a post-hoc analysis from ORCHID trial. Front Endocrinol (Lausanne). 2022, 13, 936976, Published 2022 Jul 29. [Google Scholar] [CrossRef]
- Nagarajan, R.; Krishnamoorthy, Y.; Rajaa, S.; Hariharan, V.S. COVID-19 Severity and Mortality Among Chronic Liver Disease Patients: A Systematic Review and Meta-Analysis. Prev Chronic Dis. 2022, 19, E53, Published 2022 Aug 25. [Google Scholar] [CrossRef]
- Guan, W.J.; Liang, W.H.; Shi, Y.; et al. Chronic Respiratory Diseases and the Outcomes of COVID-19: A Nationwide Retrospective Cohort Study of 39,420 Cases. J Allergy Clin Immunol Pract. 2021, 9, 2645–2655.e14. [Google Scholar] [CrossRef] [PubMed]
- ERA-EDTA Council; ERACODA Working Group. Chronic kidney disease is a key risk factor for severe COVID-19: a call to action by the ERA-EDTA. Nephrol Dial Transplant. 2021, 36, 87–94. [Google Scholar] [CrossRef]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature. 2020, 584, 430–436. [Google Scholar] [CrossRef] [PubMed]
- D'Marco, L.; Puchades, M.J.; Romero-Parra, M.; Gorriz, J.L. Diabetic Kidney Disease and COVID-19: The Crash of Two Pandemics. Front Med (Lausanne). 2020, 7, 199, Published 2020 May 6. [Google Scholar] [CrossRef] [PubMed]
- Iryaningrum, M.R.; Supriyadi, R.; Lawrensia, S.; Henrina, J.; Soetedjo, N.N.M. Diabetes and Mortality among Patients with Chronic Kidney Disease and COVID-19: A Systematic Review, Meta-analysis, and Meta-regression. Indian J Nephrol. 2022, 32, 327–333. [Google Scholar] [CrossRef]
- Anca, P.S.; Toth, P.P.; Kempler, P.; Rizzo, M. Gender differences in the battle against COVID-19: Impact of genetics, comorbidities, inflammation and lifestyle on differences in outcomes. Int J Clin Pract. 2021, 75, e13666. [Google Scholar] [CrossRef]
- Djaharuddin, I.; Munawwarah, S.; Nurulita, A.; Ilyas, M.; Tabri, N.A.; Lihawa, N. Comorbidities and mortality in COVID-19 patients. Gac Sanit. 2021, 35, S530–S532. [Google Scholar]
- Gheorghe, G.; Ilie, M.; Bungau, S.; Stoian, A.M.P.; Bacalbasa, N.; Diaconu, C.C. Is There a Relationship between COVID-19 and Hyponatremia? Medicina (Kaunas). 2021, 57, 55. [Google Scholar] [CrossRef]
© 2023 by the author. 2023 Mihaela-Simona Popoviciu, Lorena Păduraru, Roxana Adriana Stoica, Anca Pantea Stoian, Claudiu Teodorescu, Simona Cavalu