Revascularization Impact: Quality of Life Enhancement in Chronic Limb-Threatening Ischemia
Abstract
:Introduction
Materials and Methods
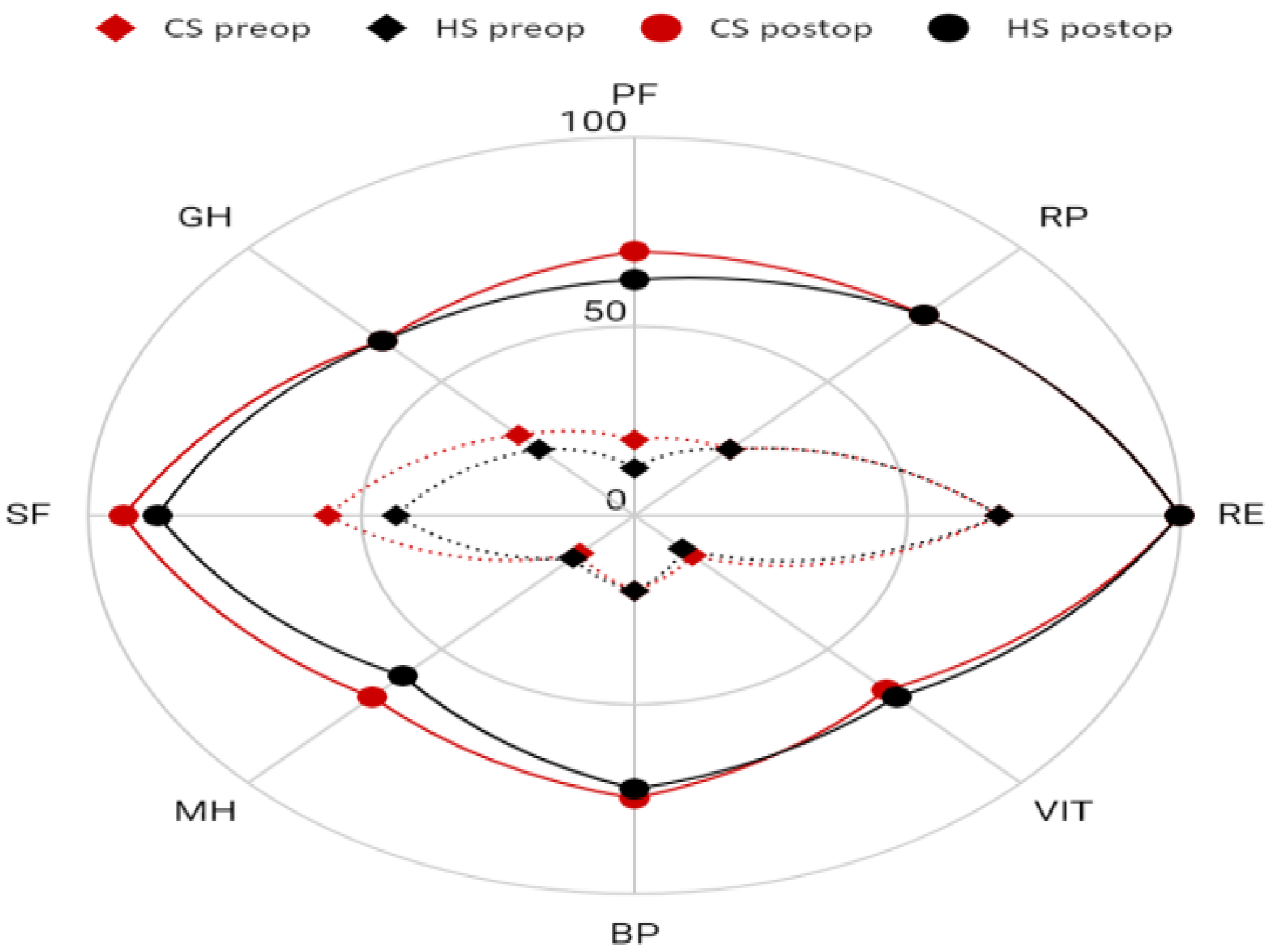
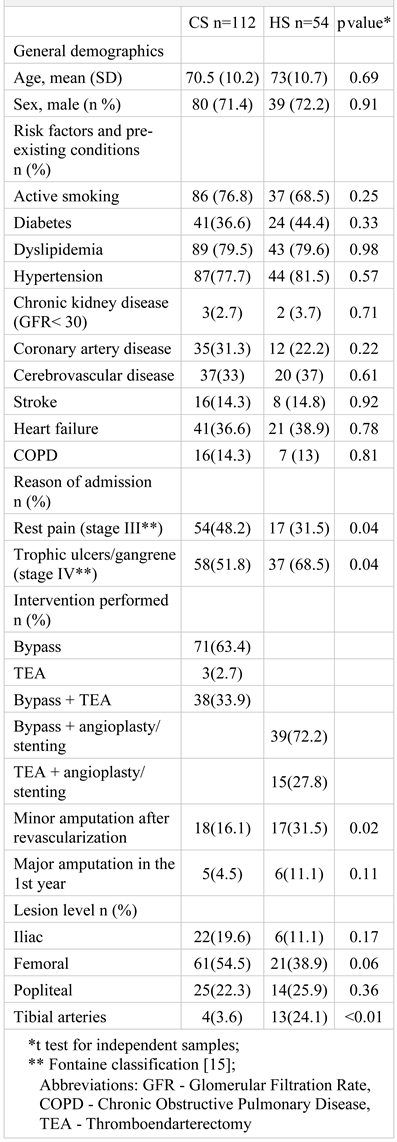
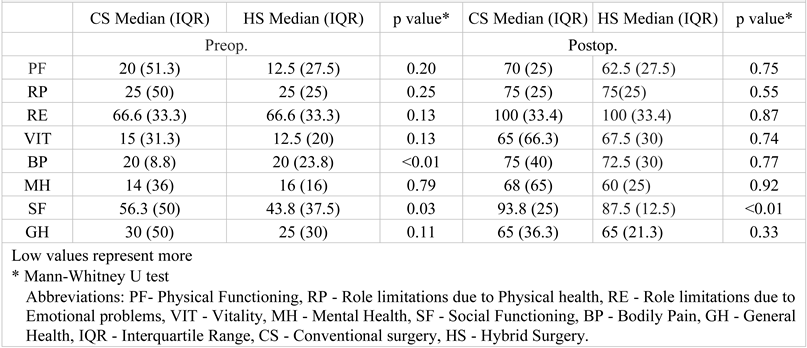
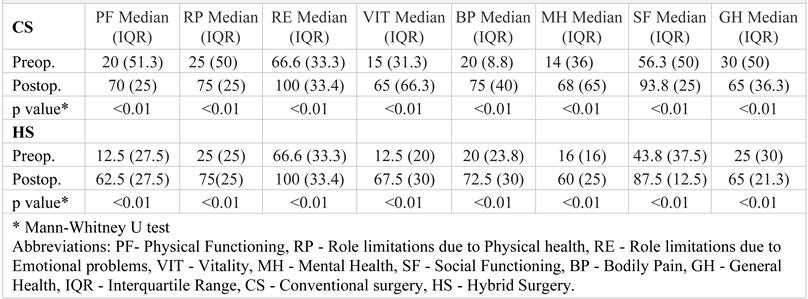
Results
Discussions
Conclusions
Highlights
- ✓
- Different methods of lower limb revascularization on the postoperative quality of life of CLTI patients highlights the multifaceted challenges they face, but underlines the significant improvement in QoL post-revascularization.
- ✓
- Despite the lack of a dedicated QoL measuring tool for CLTI patients, the study's findings suggest that both conventional surgery and hybrid procedures contribute to notable improvements in patients' QoL across various domains, underscoring the significance of tailored and comprehensive treatment approaches for these individuals.
Contributions
Compliance with ethical standards
Conflict of interest disclosure
References
- Aday, A.W.; Matsushita, K. Epidemiology of Peripheral Artery Disease and Polyvascular Disease. Circ Res. 2021, 128, 1818–1832. [Google Scholar] [CrossRef] [PubMed]
- Dhaliwal, G.; Mukherjee, D. Peripheral arterial disease: Epidemiology, natural history, diagnosis and treatment. Int J Angiol. 2007, 16, 36–44. [Google Scholar] [CrossRef]
- Bencheikh, N.; Zarrintan, S.; Quatramoni, J.G.; Al-Nouri, O.; Malas, M.; Gaffey, A.C. Vascular Surgery in Low-Income and Middle-Income Countries: A State-of-the-Art Review. Ann Vasc Surg. 2023, 95, 297–306. [Google Scholar] [CrossRef] [PubMed]
- Conte, M.S.; Bradbury, A.W.; Kolh, P.; et al. Global vascular guidelines on the management of chronic limb-threatening ischemia. J Vasc Surg. 2019, 69, 3S–125S.e40. [Google Scholar] [CrossRef] [PubMed]
- Brouwers, J.; van Rijswijk, C.; Van Den Hoven, P.; Hamming, J.; van der Vorst, J.R. Chronic Limb-Threatening Ischemia: When is Enough Enough? J Endovasc Ther. 2023, 15266028231187604. [Google Scholar] [CrossRef]
- Corcoran, W.E.; Durham, C.F. Quality of life as an outcome-based evaluation of coronary artery bypass graft critical paths using the SF-36. Qual Manag Health Care. 2000, 8, 72–81. [Google Scholar] [CrossRef]
- Rasmussen, D.; Barnason, S.; Smith, J.; et al. Patient outcomes after peripheral revascularization surgery. J Vasc Nurs. 2001, 19, 108–116. [Google Scholar] [CrossRef]
- Tarlov, A.R.; Ware, J.E., Jr.; Greenfield, S.; Nelson, E.C.; Perrin, E.; Zubkoff, M. The Medical Outcomes Study. An application of methods for monitoring the results of medical care. JAMA. 1989, 262, 925–930. [Google Scholar] [CrossRef]
- Hunt, S.M.; McKenna, S.P. Validating the SF-36. BMJ. 1992, 305, 645–646. [Google Scholar] [CrossRef]
- Constantin, V.D.; Socea, B.; Gaspar, B.S.; Epistatu, D.; Paunica, I.; Dumitriu, A.S.; Paunica, S.; Silaghi, A. Limb amputations; etiopathogenesis, diagnosis and the multidisciplinary therapeutic approach. J Mind Med Sci. 2022, 9, 209–223. [Google Scholar] [CrossRef]
- Brazier, J.E.; Harper, R.; Jones, N.M.; et al. Validating the SF-36 health survey questionnaire: new outcome measure for primary care. BMJ. 1992, 305, 160–164. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E., Jr.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care. 1992, 30, 473–483. [Google Scholar] [CrossRef]
- Almasri, J.; Adusumalli, J.; Asi, N.; et al. A systematic review and meta-analysis of revascularization outcomes of infrainguinal chronic limb-threatening ischemia. J Vasc Surg. 2018, 68, 624–633. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.A.; Donegan, D.; Albert, T. The 36-item short form. J Am Acad Orthop Surg. 2007, 15, 126–134. [Google Scholar] [CrossRef]
- Conte, M.S.; Bradbury, A.W.; Kolh, P.; et al. Global Vascular Guidelines on the Management of Chronic Limb-Threatening Ischemia. Eur J Vasc Endovasc Surg. 2019, 58, S1–S109.e33. [Google Scholar] [CrossRef]
- Chong, P.F.; Garratt, A.M.; Golledge, J.; Greenhalgh, R.M.; Davies, A.H. The intermittent claudication questionnaire: a patient-assessed condition-specific health outcome measure. J Vasc Surg. 2002, 36, 764–864. [Google Scholar] [CrossRef]
- Regensteiner, J.G.; Steiner, J.F.; Panzer, R.J.; Hiatt, W.R. Evaluation of walking impairment by questionnaire in patients with peripheral arterial disease. J Vasc Med Biol. 1990, 2, 142–152. [Google Scholar]
- Spengel, F.A.; Brown, T.M.; Dietze, S.; Kirchberger, I.; Comte, S. The Claudication Scale (CLAU-S). A new disease-specific quality of life instrument in intermittent claudication. Disease Management & Health Outcomes. 1997, 2, 65–70. [Google Scholar]
- Rutherford, R.B.; Baker, J.D.; Ernst, C.; et al. Recommended standards for reports dealing with lower extremity ischemia: revised version. J Vasc Surg. 1997, 26, 517–538. [Google Scholar] [CrossRef]
- Kutsenko, O.; Sommerset, J.; Chandra, V.; Bryce, Y. Techniques Providing Endpoints for Revascularization in Chronic Limb-Threatening Ischemia. Semin Intervent Radiol. 2023, 40, 177–182, Published 2023 Jun 16. [Google Scholar] [CrossRef]
- Hata, Y.; Iida, O.; Okamoto, S.; et al. Japanese real-world population with chronic limb-threatening ischemia who meet the criteria of the BEST-CLI trial. Vasc Med. 2023, 1358863X231205229. [Google Scholar] [CrossRef]
- Iancu, G.; Serban, D.; Badiu, C.D.; Tanasescu, C.; Tudosie, M.S.; Tudor, C.; Costea, D.O.; Zgura, A.; Iancu, R.; Vasile, D. Tyrosine kinase inhibitors in breast cancer (Review). Exp Ther Med. 2022, 23, 114. [Google Scholar] [CrossRef]
- Serban, D.; Popa Cherecheanu, A.; Dascalu, A.M.; et al. Hypervirulent Klebsiella pneumoniae Endogenous Endophthalmitis-A Global Emerging Disease. Life (Basel). 2021, 11, 676. [Google Scholar] [CrossRef]
- Davie-Smith, F.; Coulter, E.; Kennon, B.; Wyke, S.; Paul, L. Factors influencing quality of life following lower limb amputation for peripheral arterial occlusive disease: A systematic review of the literature. Prosthet Orthot Int. 2017, 41, 537–547. [Google Scholar] [CrossRef]
- Yagshyyev, S.; Hausmann, P.; Li, Y.; et al. Intermittent negative pressure therapy in patients with no-option chronic limb-threatening ischemia. Vasa 2023, 10.1024/0301-1526/a001098. [Google Scholar] [CrossRef]
- Nylaende, M.; Abdelnoor, M.; Stranden, E.; et al. The Oslo balloon angioplasty versus conservative treatment study (OBACT)--the 2-years results of a single centre, prospective, randomised study in patients with intermittent claudication. Eur J Vasc Endovasc Surg. 2007, 33, 3–12. [Google Scholar] [CrossRef]
- Beach, J.M. Revascularization Strategies for Acute and Chronic Limb Ischemia. Cardiol Clin. 2021, 39, 483–494. [Google Scholar] [CrossRef]
- Berchiolli, R.; Bertagna, G.; Adami, D.; Canovaro, F.; Torri, L.; Troisi, N. Chronic Limb-Threatening Ischemia and the Need for Revascularization. J Clin Med. 2023, 12, 2682. [Google Scholar] [CrossRef]
- Khalil, E.; Ozcan, S. Health-related quality of life after vascular surgery and endovascular treatment in subjects with critical limb ischemia. Pak J Med Sci. 2020, 36, 877–883. [Google Scholar] [CrossRef]
- Vlajinac, H.; Marinkovic, J.; Tanaskovic, S.; et al. Quality of life after peripheral bypass surgery: a 1 year follow-up. Wien Klin Wochenschr. 2015, 127, 210–217. [Google Scholar] [CrossRef]
- Alexandrescu, V.; Hubermont, G.; Coessens, V.; et al. Why a multidisciplinary team may represent a key factor for lowering the inferior limb loss rate in diabetic neuro-ischaemic wounds: application in a departmental institution. Acta Chir Belg. 2009, 109, 694–700. [Google Scholar] [CrossRef] [PubMed]
- Caetano, A.P.; Conde Vasco, I.; Veloso Gomes, F.; et al. Successful Revascularization has a Significant Impact on Limb Salvage Rate and Wound Healing for Patients with Diabetic Foot Ulcers: Single-Centre Retrospective Analysis with a Multidisciplinary Approach. Cardiovasc Intervent Radiol. 2020, 43, 1449–1459. [Google Scholar] [CrossRef]
- Tanasescu, D.; Moisin, A.; Fleaca, R.; et al. Modern therapeutic options in diabetic foot ulcer. J Mind Med Sci. 2022, 9, 285–293. [Google Scholar] [CrossRef]
- Liistro, F.; Porto, I.; Angioli, P.; et al. Drug-eluting balloon in peripheral intervention for below the knee angioplasty evaluation (DEBATE-BTK): a randomized trial in diabetic patients with critical limb ischemia. Circulation. 2013, 128, 615–621. [Google Scholar] [CrossRef]
- Liistro, F.; Grotti, S.; Porto, I.; et al. Drug-eluting balloon in peripheral intervention for the superficial femoral artery: the DEBATE-SFA randomized trial (drug eluting balloon in peripheral intervention for the superficial femoral artery). JACC Cardiovasc Interv. 2013, 6, 1295–1302. [Google Scholar] [CrossRef]
- Castro-Dominguez, Y.; Shishehbor, M.H. Team-Based Care in Patients with Chronic Limb-Threatening Ischemia. Curr Cardiol Rep. 2022, 24, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Lozano Navarro, L.V.; Chen, X.; Giratá Viviescas, L.T.; et al. Mesenchymal stem cells for critical limb ischemia: their function, mechanism, and therapeutic potential. Stem Cell Res Ther. 2022, 13, 345, Published 2022 Jul 26. [Google Scholar] [CrossRef]
- Huerta, C.T.; Voza, F.A.; Ortiz, Y.Y.; Liu, Z.J.; Velazquez, O.C. Mesenchymal stem cell-based therapy for non-healing wounds due to chronic limb-threatening ischemia: A review of preclinical and clinical studies. Front Cardiovasc Med. 2023, 10, 1113982, Published 2023 Feb 1. [Google Scholar] [CrossRef] [PubMed]
- Shirbaghaee, Z.; Hassani, M.; Heidari Keshel, S.; Soleimani, M. Emerging roles of mesenchymal stem cell therapy in patients with critical limb ischemia. Stem Cell Res Ther. 2022, 13, 462. [Google Scholar] [CrossRef]
- Babtan, A.M.; Ilea, A.; Feurdean, C.N.; et al. Biostimulation with low-level laser therapy and its effects on soft and hard tissue regeneration. Literature review. J Mind Med Sci. 2022, 9, 28–37. [Google Scholar] [CrossRef]
- Adamičková, A.; Gažová, A.; Adamička, M.; et al. Molecular basis of the effect of atorvastatin pretreatment on stem cell therapy in chronic ischemic diseases - critical limb ischemia. Physiol Res. 2021, 70, S527–S533. [Google Scholar] [CrossRef] [PubMed]
- Arango-Rodríguez, M.L.; Mateus, L.C.; Sossa, C.L.; et al. A novel therapeutic management for diabetes patients with chronic limb-threatening ischemia: comparison of autologous bone marrow mononuclear cells versus allogenic Wharton jelly-derived mesenchymal stem cells. Stem Cell Res Ther. 2023, 14, 221, Published 2023 Aug 25. [Google Scholar] [CrossRef]
- Shan, L.L.; Wang, J.; Westcott, M.J.; et al. A Systematic Review of Cost-Utility Analyses in Chronic Limb-Threatening Ischemia. Ann Vasc Surg. 2022, 85, 9–21. [Google Scholar] [CrossRef]
- Bensley, R.P.; Beck, A.W. Using the Vascular Quality Initiative to improve quality of care and patient outcomes for vascular surgery patients. Semin Vasc Surg. 2015, 28, 97–102. [Google Scholar] [CrossRef]
- Li, Q.; Birmpili, P.; Johal, A.S.; et al. Delays to revascularization for patients with chronic limb-threatening ischaemia. Br J Surg. 2022, 109, 717–726. [Google Scholar] [CrossRef]
- Shatnawi, N.J.; Al-Zoubi, N.A.; Al-Bakkar, L.A.; et al. Chronic Limb-Threatening Ischemia in Patients with Type 2 Diabetes: Revascularization Index as a Predictor for Primary Endovascular Intervention Outcome. Vasc Health Risk Manag. 2023, 19, 495–504, Published 2023 Jul 31. [Google Scholar] [CrossRef] [PubMed]
- Belowski, A.; Partyka, Ł.; Krzanowski, M.; et al. Clinical and linguistic validation of the Polish version of VascuQol: a disease-specific quality-of-life questionnaire assessing patients with chronic limb ischemia. Pol Arch Intern Med. 2019, 129, 167–174. [Google Scholar] [CrossRef]
- Serna Santos, J.; Söderström, M.; Helminen, R.; Aho, P.; Halmesmäki, K.; Venermo, M. Outcome after Hybrid Outflow Interventions for Chronic Limb-threatening Ischemia. Scand J Surg. 2021, 110, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Terabe, Y.; Kaneko, N.; Ando, H. Three years progress chronic limb-threatening ischemia case with simultaneous surgery. Int J Surg Case Rep. 2022, 95, 107212. [Google Scholar] [CrossRef]
- Kobayashi, T.; Kodama, A.; Okazaki, T.; et al. Prognostic Significance of Preoperative Functional Independence Measure (FIM) on Long-Term Outcomes in Patients with Chronic Limb-Threatening Ischemia (CLTI). Ann Vasc Surg. 2022, 83, 275–283. [Google Scholar] [CrossRef]
- Secară, C.A.; Cinteză, O.L.; Popescu, D.; Popa, C.V.; Hîrjeu, C.A.; Voinea, O.C.; Șerbănescu, L.G.; Păuna, A.M.; Tudosie, M.S. Innovative therapeutic approach to chemical burns produced by vesicants; an experimental study. J Mind Med Sci. 2022, 9, 294–303. [Google Scholar] [CrossRef]
- Simon, F.; Duran, M.; Garabet, W.; Schelzig, H.; Jacobs, M.; Gombert, A. Gene Therapy of Chronic Limb-Threatening Ischemia: Vascular Medical Perspectives. J Clin Med. 2022, 11, 1282, Published 2022 Feb 26. [Google Scholar] [CrossRef]
- Vaidya, A.; Kleinegris, M.C.; Severens, J.L.; et al. Comparison of EQ-5D and SF-36 in untreated patients with symptoms of intermittent claudication. J Comp Eff Res. 2018, 7, 535–548. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
 |
 |
 |
 |
© 2023 by the author. 2023 Cristian Traian Paius, Vlad Denis Constantin, Alexandru Carap, Andrei Tarus, Grigore Tinica
Share and Cite
Paius, C.T.; Constantin, V.D.; Carap, A.; Tarus, A.; Tinica, G. Revascularization Impact: Quality of Life Enhancement in Chronic Limb-Threatening Ischemia. J. Mind Med. Sci. 2023, 10, 321-329. https://doi.org/10.22543/2392-7674.1441
Paius CT, Constantin VD, Carap A, Tarus A, Tinica G. Revascularization Impact: Quality of Life Enhancement in Chronic Limb-Threatening Ischemia. Journal of Mind and Medical Sciences. 2023; 10(2):321-329. https://doi.org/10.22543/2392-7674.1441
Chicago/Turabian StylePaius, Cristian Traian, Vlad Denis Constantin, Alexandru Carap, Andrei Tarus, and Grigore Tinica. 2023. "Revascularization Impact: Quality of Life Enhancement in Chronic Limb-Threatening Ischemia" Journal of Mind and Medical Sciences 10, no. 2: 321-329. https://doi.org/10.22543/2392-7674.1441
APA StylePaius, C. T., Constantin, V. D., Carap, A., Tarus, A., & Tinica, G. (2023). Revascularization Impact: Quality of Life Enhancement in Chronic Limb-Threatening Ischemia. Journal of Mind and Medical Sciences, 10(2), 321-329. https://doi.org/10.22543/2392-7674.1441