
Biliary Leak after Pediatric Liver Transplantation Treated by Percutaneous Transhepatic Biliary Drainage—A Case Series

 ,
,  , and
, and
Abstract
1. Introduction
2. Material and Methods
2.1. Study Design
2.2. Procedure Technique
2.3. Definitions and Data
2.4. Statistical Analysis
3. Results
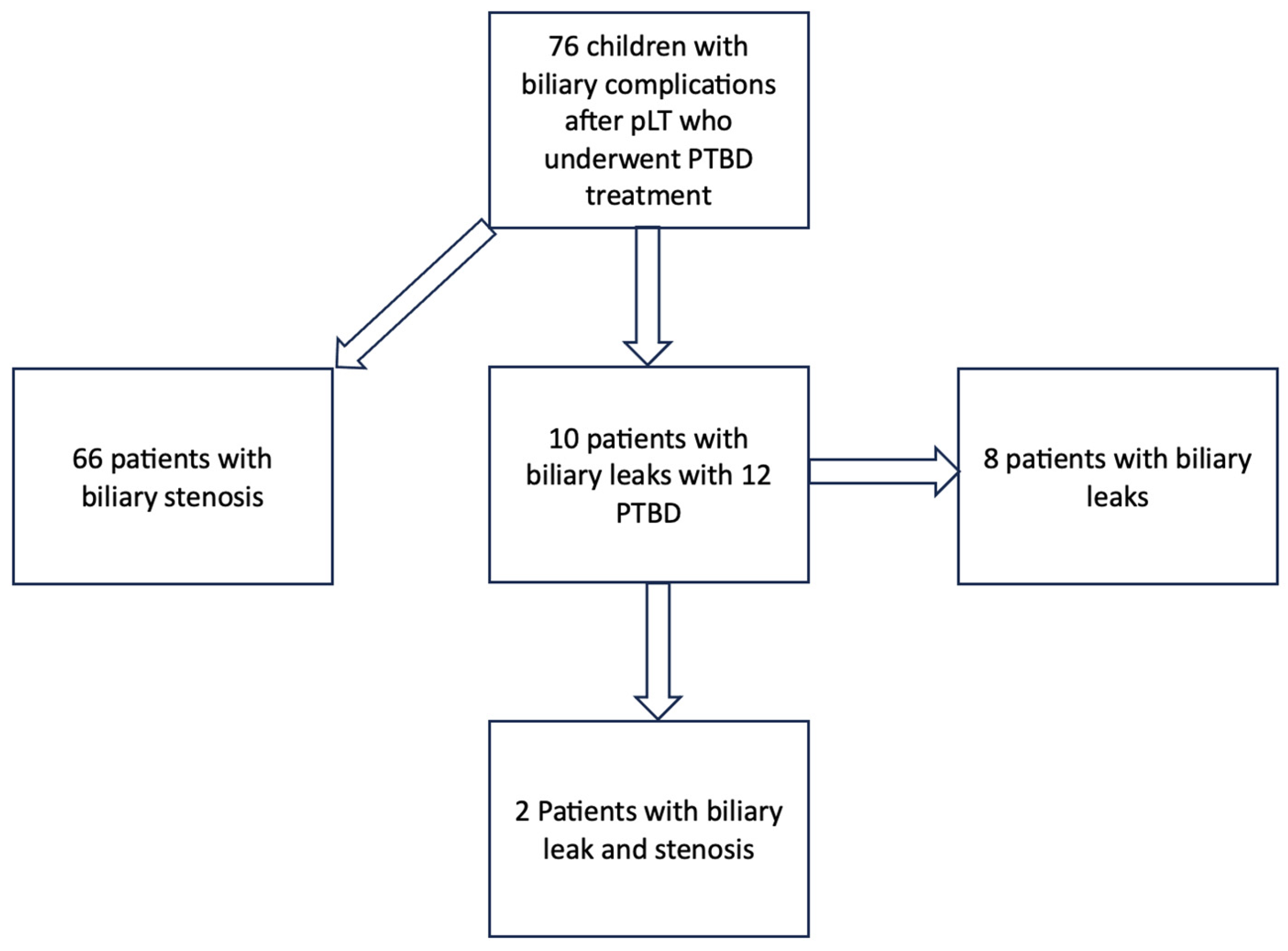
3.1. Study Cohort
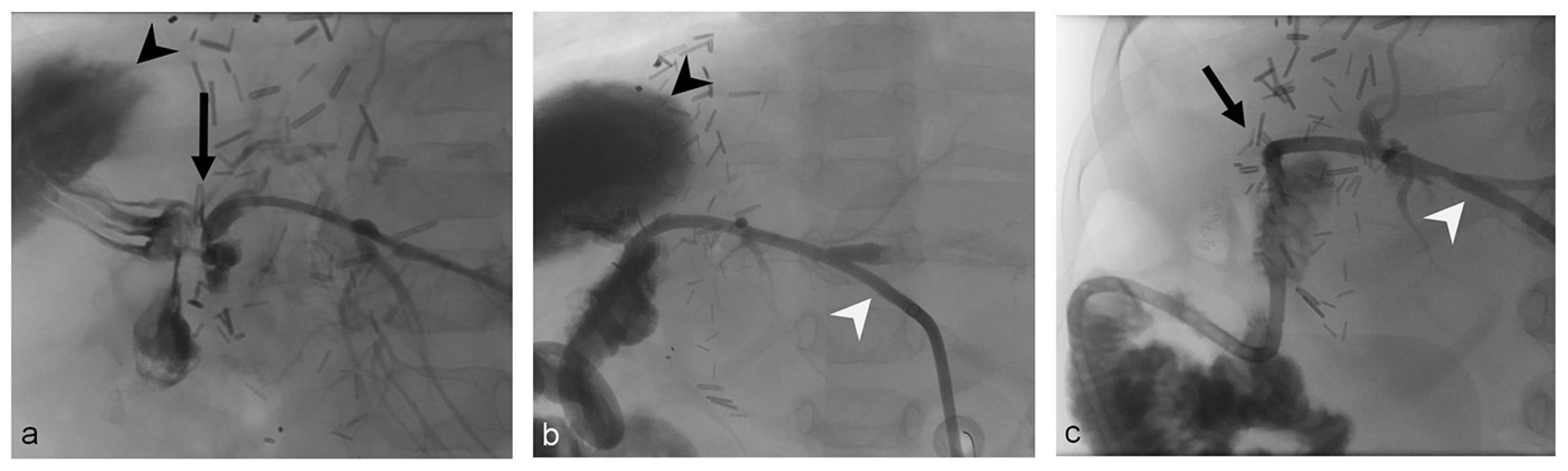
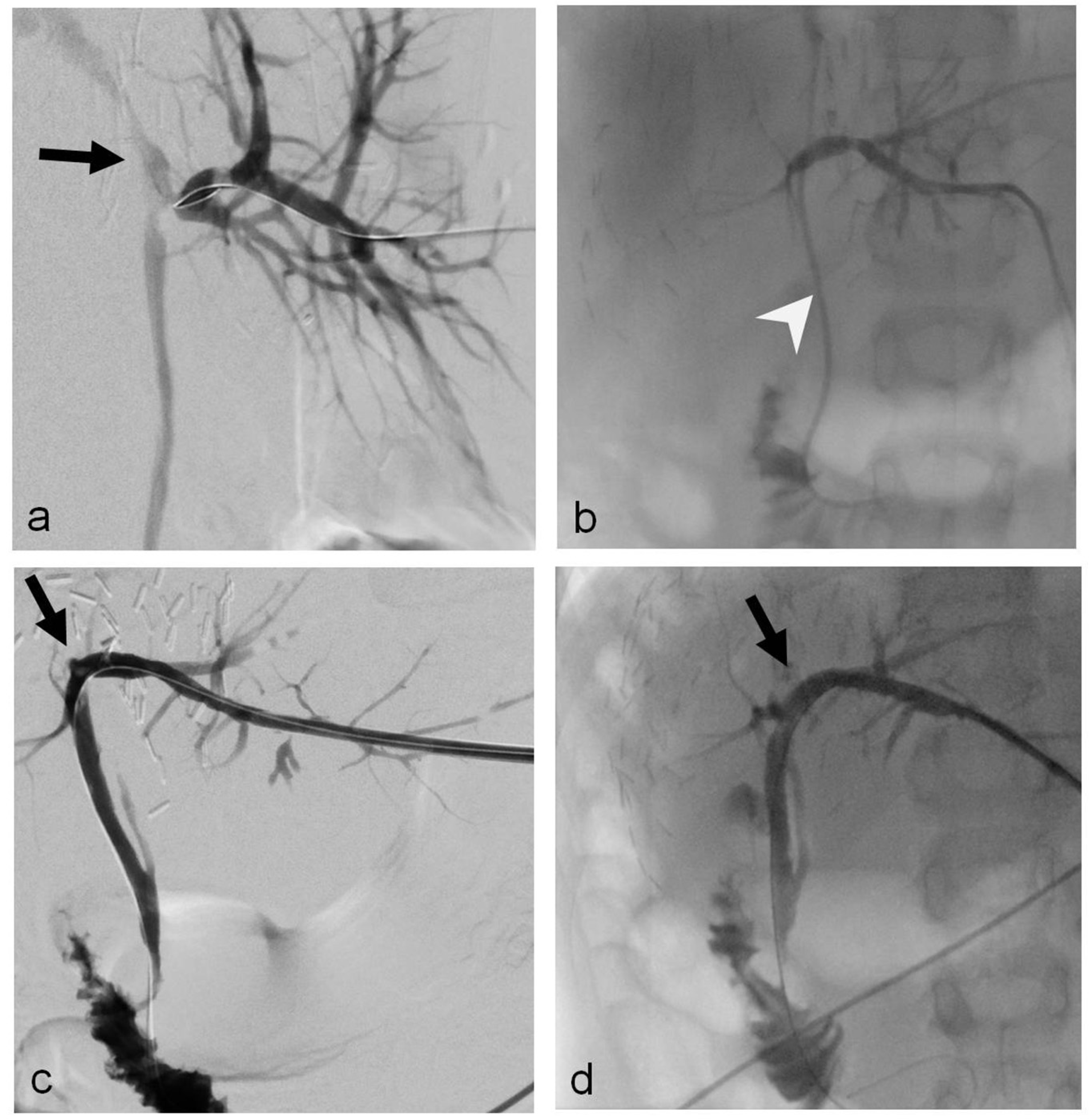
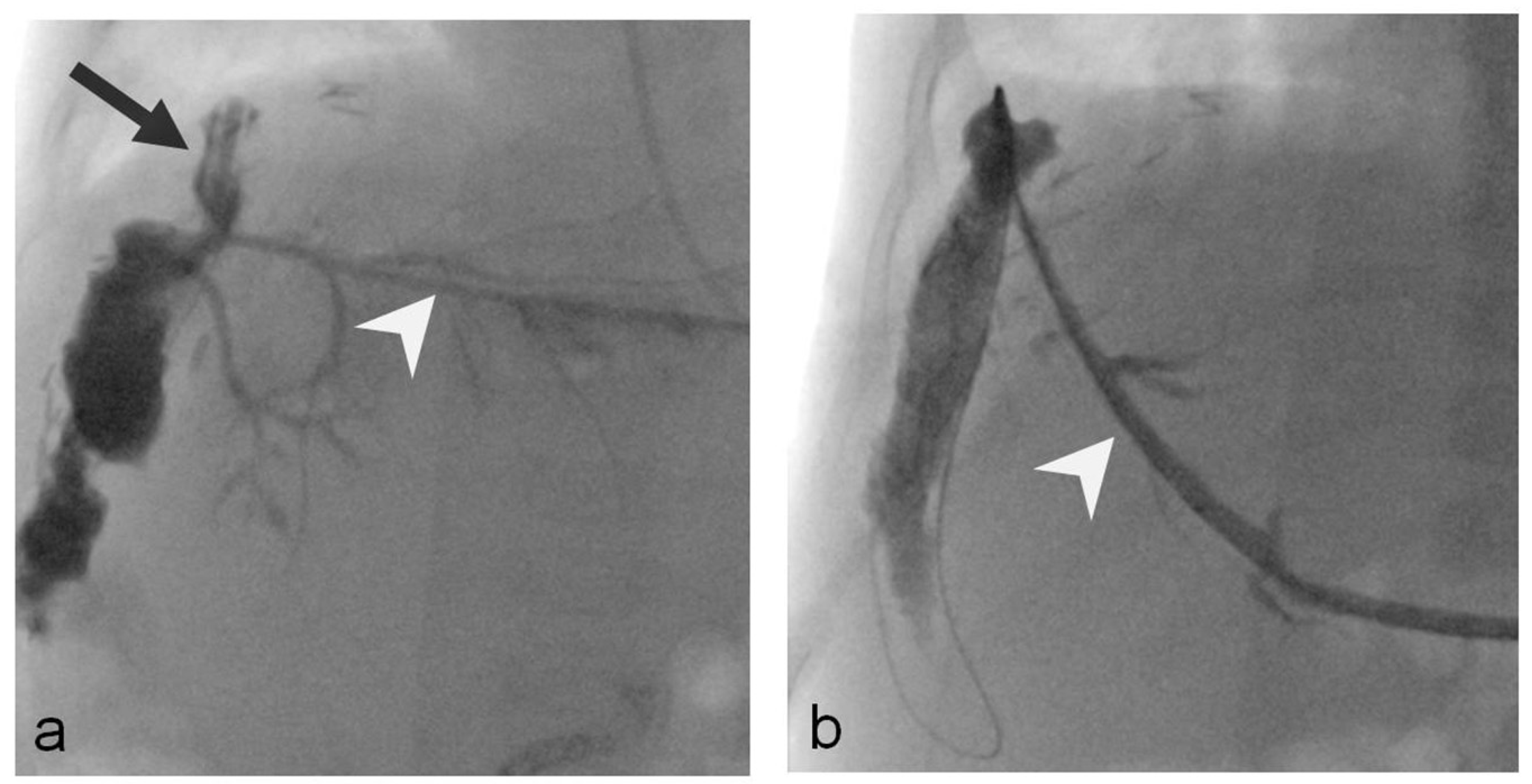
3.2. Biliary Leaks
3.3. Outcome
3.4. Inflammation Parameters
3.5. Cholestasis Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Deutsche Stiftung Organtransplantation. Jahresbericht Organspende und Transplantation in Deutschland 2020; Deutsche Stiftung Organtransplantation: Frankfurt, Germany, 2020. [Google Scholar]
- Hackl, C.; Schlitt, H.J.; Melter, M.; Knoppke, B.; Loss, M. Current developments in pediatric liver transplantation. World J. Hepatol. 2015, 7, 1509–1520. [Google Scholar] [CrossRef] [PubMed]
- Hackl, C.; Schmidt, K.M.; Susal, C.; Dohler, B.; Zidek, M.; Schlitt, H.J. Split liver transplantation: Current developments. World J. Gastroenterol. 2018, 24, 5312–5321. [Google Scholar] [CrossRef] [PubMed]
- Tran, L.T.; Carullo, P.C.; Banh, D.P.T.; Vitu, C.; Davis, P.J. Pediatric Liver Transplantation: Then and Now. J. Cardiothorac. Vasc. Anesth. 2020, 34, 2028–2035. [Google Scholar] [CrossRef] [PubMed]
- Dresske, B.; Schulze, M.; Braun, F.; Walter, J.; Kohl, M.; Schulz-Jurgensen, S.; Krause, M.; Schrappe, M.; Burdelski, M.; Broring, D.C. Living donation liver transplantation in children. Chirurg 2010, 81, 813–819. [Google Scholar] [CrossRef]
- Diamond, I.R.; Fecteau, A.; Millis, J.M.; Losanoff, J.E.; Ng, V.; Anand, R.; Song, C.; Group, S.R. Impact of graft type on outcome in pediatric liver transplantation: A report From Studies of Pediatric Liver Transplantation (SPLIT). Ann. Surg. 2007, 246, 301–310. [Google Scholar] [CrossRef]
- D’Alessandro, A.M.; Knechtle, S.J.; Chin, L.T.; Fernandez, L.A.; Yagci, G.; Leverson, G.; Kalayoglu, M. Liver transplantation in pediatric patients: Twenty years of experience at the University of Wisconsin. Pediatr. Transpl. 2007, 11, 661–670. [Google Scholar] [CrossRef]
- Feier, F.H.; da Fonseca, E.A.; Seda-Neto, J.; Chapchap, P. Biliary complications after pediatric liver transplantation: Risk factors, diagnosis and management. World J. Hepatol. 2015, 7, 2162–2170. [Google Scholar] [CrossRef]
- Goss, J.A.; Shackleton, C.R.; McDiarmid, S.V.; Maggard, M.; Swenson, K.; Seu, P.; Vargas, J.; Martin, M.; Ament, M.; Brill, J.; et al. Long-term results of pediatric liver transplantation: An analysis of 569 transplants. Ann. Surg. 1998, 228, 411–420. [Google Scholar] [CrossRef]
- Heffron, T.G.; Pillen, T.; Welch, D.; Smallwood, G.A.; Redd, D.; Romero, R. Biliary complications after pediatric liver transplantation revisited. Transpl. Proc. 2003, 35, 1461–1462. [Google Scholar] [CrossRef]
- Tanaka, H.; Fukuda, A.; Shigeta, T.; Kuroda, T.; Kimura, T.; Sakamoto, S.; Kasahara, M. Biliary reconstruction in pediatric live donor liver transplantation: Duct-to-duct or Roux-en-Y hepaticojejunostomy. J. Pediatr. Surg. 2010, 45, 1668–1675. [Google Scholar] [CrossRef]
- Chang, T.I.; Ho, M.C.; Wu, Y.M.; Lee, P.H.; Hu, R.H. Biliary complications after liver transplantation: An 18-year single-center experience. J. Formos. Med. Assoc. 2011, 110, 183–189. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Maguire, D.; Rela, M.; Heaton, N. Biliary complications after orthotopic liver transplantation. Transplant. Rev. 2002, 16, 220–240. [Google Scholar] [CrossRef]
- Miraglia, R.; Maruzzelli, L.; Caruso, S.; Marrone, G.; Carollo, V.; Spada, M.; Luca, A.; Gridelli, B. Interventional radiology procedures in pediatric patients with complications after liver transplantation. Radiographics 2009, 29, 567–584. [Google Scholar] [CrossRef] [PubMed]
- Buis, C.I.; Hoekstra, H.; Verdonk, R.C.; Porte, R.J. Causes and consequences of ischemic-type biliary lesions after liver transplantation. J. Hepatobiliary Pancreat. Surg. 2006, 13, 517–524. [Google Scholar] [CrossRef] [PubMed]
- Moench, C.; Moench, K.; Lohse, A.W.; Thies, J.; Otto, G. Prevention of ischemic-type biliary lesions by arterial back-table pressure perfusion. Liver Transpl. 2003, 9, 285–289. [Google Scholar] [CrossRef]
- Feier, F.H.; Chapchap, P.; Pugliese, R.; da Fonseca, E.A.; Carnevale, F.C.; Moreira, A.M.; Zurstrassen, C.; Santos, A.C.; Miura, I.K.; Baggio, V.; et al. Diagnosis and management of biliary complications in pediatric living donor liver transplant recipients. Liver Transpl. 2014, 20, 882–892. [Google Scholar] [CrossRef]
- Hsiao, C.Y.; Ho, C.M.; Wu, Y.M.; Ho, M.C.; Hu, R.H.; Lee, P.H. Biliary Complication in Pediatric Liver Transplantation: A Single-Center 15-Year Experience. J. Gastrointest. Surg. 2019, 23, 751–759. [Google Scholar] [CrossRef]
- Laurence, J.M.; Sapisochin, G.; DeAngelis, M.; Seal, J.B.; Miserachs, M.M.; Marquez, M.; Zair, M.; Fecteau, A.; Jones, N.; Hrycko, A.; et al. Biliary complications in pediatric liver transplantation: Incidence and management over a decade. Liver Transpl. 2015, 21, 1082–1090. [Google Scholar] [CrossRef]
- Darius, T.; Rivera, J.; Fusaro, F.; Lai, Q.; de Magnee, C.; Bourdeaux, C.; Janssen, M.; Clapuyt, P.; Reding, R. Risk factors and surgical management of anastomotic biliary complications after pediatric liver transplantation. Liver Transpl. 2014, 20, 893–903. [Google Scholar] [CrossRef]
- Zorger, N.; Feuerbach, S. Technik der Perkutanen Transhepatischen Cholangio-Drainage (PTCD). J. Gastroenterol. Hepatol. Erkr. 2010, 8, 21–26. [Google Scholar]
- Uller, W.; Wohlgemuth, W.A.; Hammer, S.; Knoppke, B.; Goessmann, H.; Loss, M.; Schlitt, H.J.; Stroszczynski, C.; Zorger, N.; Heiss, P. Percutaneous treatment of biliary complications in pediatric patients after liver transplantation. Rofo 2014, 186, 1127–1133. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Academic Press: Cambridge, MA, USA, 2013. [Google Scholar]
- Renzulli, M.; Brandi, N.; Brocchi, S.; Balacchi, C.; Lanza, C.; Pettinari, I.; Stefanini, B.; Carrafiello, G.; Piscaglia, F.; Golfieri, R.; et al. Association between anatomic variations of extrahepatic and intrahepatic bile ducts: Do look up! J. Anat. 2023, 242, 683–694. [Google Scholar] [CrossRef] [PubMed]
- Mortelé, K.J.; Ros, P.R. Anatomic variants of the biliary tree: MR cholangiographic findings and clinical applications. Am. J. Roentgenol. 2001, 177, 389–394. [Google Scholar] [CrossRef] [PubMed]
- Dulcetta, L.; Marra, P.; Carbone, F.S.; Bonaffini, P.A.; Sallemi, C.; Sansotta, N.; Colledan, M.; D’Antiga, L.; Sironi, S. Biliary complications in pediatric liver transplantation: Findings of percutaneous transhepatic cholangiography in a large single-center cohort. Pediatr. Radiol. 2022, 52, 1061–1074. [Google Scholar] [CrossRef] [PubMed]
- Mastier, C.; Valette, P.J.; Adham, M.; Mabrut, J.Y.; Glehen, O.; Ponchon, T.; Rousset, P.; Rode, A. Complex Biliary Leaks: Effectiveness of Percutaneous Radiological Treatment Compared to Simple Leaks in 101 Patients. Cardiovasc. Interv. Radiol. 2018, 41, 1566–1572. [Google Scholar] [CrossRef] [PubMed]
- Lorenz, J.M.; Funaki, B.; Leef, J.A.; Rosenblum, J.D.; Van Ha, T. Percutaneous Transhepatic Cholangiography and Biliary Drainage in Pediatric Liver Transplant Patients. Am. J. Roentgenol. 2001, 176, 761–765. [Google Scholar] [CrossRef] [PubMed]
- Mosconi, C.; Calandri, M.; Mirarchi, M.; Vara, G.; Breatta, A.D.; Cappelli, A.; Brandi, N.; Paccapelo, A.; De Benedittis, C.; Ricci, C.; et al. Percutaneous management of postoperative Bile leak after hepato-pancreato-biliary surgery: A multi-center experience. HPB 2021, 23, 1518–1524. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Weight | Sex | Age at the Start of PTBD | Duration of PTBD Treatment | Duration of Follow-Up | Drain for Bilioma | Site of Bile Leak | Target Size of PTBD | Additional Bile Duct Stenosis | Type of Transplant | Living Donor |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 48.9 kg | m | 16 y 8 m | 7 m (200 d) | 63 m (1929 d) | Yes | End-to-side hepaticojejunostomy | 10 F | No | Right liver lobe | No |
| 2 | 9.5 kg | m | 1 y 5 m | 2 m (57 d) | 92 m (2809 d) | Yes | End-to-side hepaticojejunostomy | 8 F | Yes | Left lat. split | No |
| 3 | 5.1 kg | f | 5 m | 10 m (304 d) | 3 m (79 d) | Yes | End-to-side hepaticojejunostomy (Double bile duct anastomosis) | 10 F | Yes | Left lat. split | Yes |
| 4 | 35.9 kg | m | 9 y 9 m | 8 m (244 d) | 24 m (732 d) | Yes | End-to-end choledochcholedochostomy | 12 F | Yes | Left liver lobe | Yes |
| 5 | 6.8 kg | f | 8 m | 3 m (89 d) | 73 m (2216 d) | Yes | End-to-side hepaticojejunostomy (Double bile duct anastomosis) | 6 F | No | Left lat. split | No |
| 6 | 47 kg | f | 11 y 7 m | 1 m (20 d) | 21 m (632 d) | No | End-to-side hepaticojejunostomy | 8.5 F | No | Left liver lobe | Yes |
| 7 | 12 kg | f | 3 y 5 m | 1 m (25 d) | 66 m (1999 d) | Yes | End-to-side hepaticojejunostomy (Double bile duct anastomosis) | 10 F | No | Left lat. split | No |
| 8 | 6 kg | f | 6 m | 1 m (37 d) | 33 m (1002 d) | Yes | End-to-side hepaticojejunostomy (Double bile duct anastomosis) | 8.5 F | No | Left lat. split | Yes |
| 9 | 70.9 kg | f | 14 y 8 m | 3 m (106 d) | 28 m (865 d) | Yes | End-to-end choledochcholedochostomy | 10 F | No | Full size | No |
| 10 | 8.3 kg | f | 1 y 6 m | 0.5 m (15 d) | 60 m (1830 d) | No | Non-anastomosed bile duct of segment II | 6 F | No | Left lat. split | Yes |
| Parameter | Before PTBD | After PTBD | Last Annual Follow-Up | |||||
|---|---|---|---|---|---|---|---|---|
| Median | Mean | Median | Mean | p | Median | Mean | p | |
| Alkaline Phosphatase (ALP) | 519 U/L | 494.7 ± 148 U/L | 256 U/L | 369.1 ± 94.9 U/L | 0.5 | 282 U/L | 297.9 ± 47.4 U/L | 0.06 |
| Bilirubin Total Direct Indirect | 1.3 mg/dL 1.2 mg/dL 0.3 mg/dL | 1.7 ± 0.5 mg/dL 1.6 ± 0.5 mg/dL 0.4 ± 0.2 mg/dL | 0.5 mg/dL 0.2 mg/dL 0.1 mg/dL | 0.46 ± 0.04 mg/dL 0.2 ± 0.03 mg/dL 0.2 ± 0.07 mg/dL | 0.006 0.03 0.11 | 0.53 mg/dL 0.2 mg/dL 0.3 mg/dL | 0.5 ± 0.07 mg/dL 0.2 ± 0.02 mg/dL 0.4 ± 0.06 mg/dL | 0.12 0.08 0.11 |
| Choline esterase (CHE) | 10,638 U/L | 10,349 ± 799 U/L | 9588 U/L | 8744 ± 1118 U/L | 0.5 | 10,376 U/L | 10,498 ± 806 U/L | 0.12 |
| Gamma-glutamyl transferase (GGT) | 104 U/L | 177 ± 56.2 U/L | 94.5 U/L | 121.5 ± 29.3 U/L | 0.009 | 26 U/L | 66.8 ± 21.6 U/L | 0.016 |
| Glutamate dehydrogenase (GLDH) | 4.1 U/L | 7 ± 2.3 U/L | 4.3 U/L | 4.9 ± 0.92 U/L | 0.23 | 4.0 U/L | 27.8 ± 23.8 U/L | 0.917 |
| Aspartate transaminase (AST) | 20 U/L | 48.9 ± 19.1 U/L | 32.5 U/L | 42.9 ± 9 U/L | 0.15 | 31 U/L | 54.9 ± 25.8 U/L | 0.43 |
| Alanine transaminase (ALT) | 42 U/L | 79.7 ± 37.8 U/L | 33.5 U/L | 45.2 ± 12.8 U/L | 0.25 | 30.5 U/L | 40.2 ± 9.2 U/L | 0.42 |
| Albumin | 24.1 g/L | 24.3 ± 2.3 g/L | 31.7 g/L | 31.8 ± 3.3 g/L | 0.14 | 36.6 g/L | 36.8 ± 1.2 g/L | 0.29 |
| INR | 1.1 | 1.1 ± 0.04 | 1.1 | 1.1 ± 0.02 | 0.36 | 1.0 | 0.9 ± 0.02 | 0.11 |
| Quick | 88% | 87.7 ± 5.3% | 86% | 84.8 ± 3.8% | 0.36 | 101% | 99.6 ± 2.8% | 0.11 |
| CRP | 16.6 mg/L | 47.2 ± 16.4 mg/L | 7.5 mg/L | 14.3 ± 4.8 mg/L | 0.05 | 2.8 mg/L | 4.8 ± 1.8 mg/L | 0.11 |
| Leucocytes | 10.3 × 103/μL | 9.6 ± 1.3 × 103/μL | 6.4 × 103/μL | 6.7 ± 0.8 × 103/μL | 0.05 | 6.6 × 103/μL | 7.4 ± 1.1 × 103/μL | 0.14 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Doppler, M.; Fürnstahl, C.; Hammer, S.; Melter, M.; Verloh, N.; Schlitt, H.J.; Uller, W. Biliary Leak after Pediatric Liver Transplantation Treated by Percutaneous Transhepatic Biliary Drainage—A Case Series. Tomography 2023, 9, 1965-1975. https://doi.org/10.3390/tomography9050153
Doppler M, Fürnstahl C, Hammer S, Melter M, Verloh N, Schlitt HJ, Uller W. Biliary Leak after Pediatric Liver Transplantation Treated by Percutaneous Transhepatic Biliary Drainage—A Case Series. Tomography. 2023; 9(5):1965-1975. https://doi.org/10.3390/tomography9050153
Chicago/Turabian StyleDoppler, Michael, Christin Fürnstahl, Simone Hammer, Michael Melter, Niklas Verloh, Hans Jürgen Schlitt, and Wibke Uller. 2023. "Biliary Leak after Pediatric Liver Transplantation Treated by Percutaneous Transhepatic Biliary Drainage—A Case Series" Tomography 9, no. 5: 1965-1975. https://doi.org/10.3390/tomography9050153
APA StyleDoppler, M., Fürnstahl, C., Hammer, S., Melter, M., Verloh, N., Schlitt, H. J., & Uller, W. (2023). Biliary Leak after Pediatric Liver Transplantation Treated by Percutaneous Transhepatic Biliary Drainage—A Case Series. Tomography, 9(5), 1965-1975. https://doi.org/10.3390/tomography9050153