
Radiation Dose Management in Computed Tomography: Introduction to the Practice at a Single Facility


Abstract
1. Introduction
2. Management of Imaging Protocols
2.1. Significance of Protocol Management
2.2. Preparation of Subdivided Imaging Protocols
2.3. Preparation of the Protocol List
2.4. Tabulation of Imaging Parameters
3. Overview of CT Radiation Dose Management
3.1. Dose Indices Used for Radiation Dose Management
3.2. Automatic Exposure Control
3.3. The Need to Consider Body Size in Radiation Dose Management
3.4. Radiation Dose Management Considering Body Size
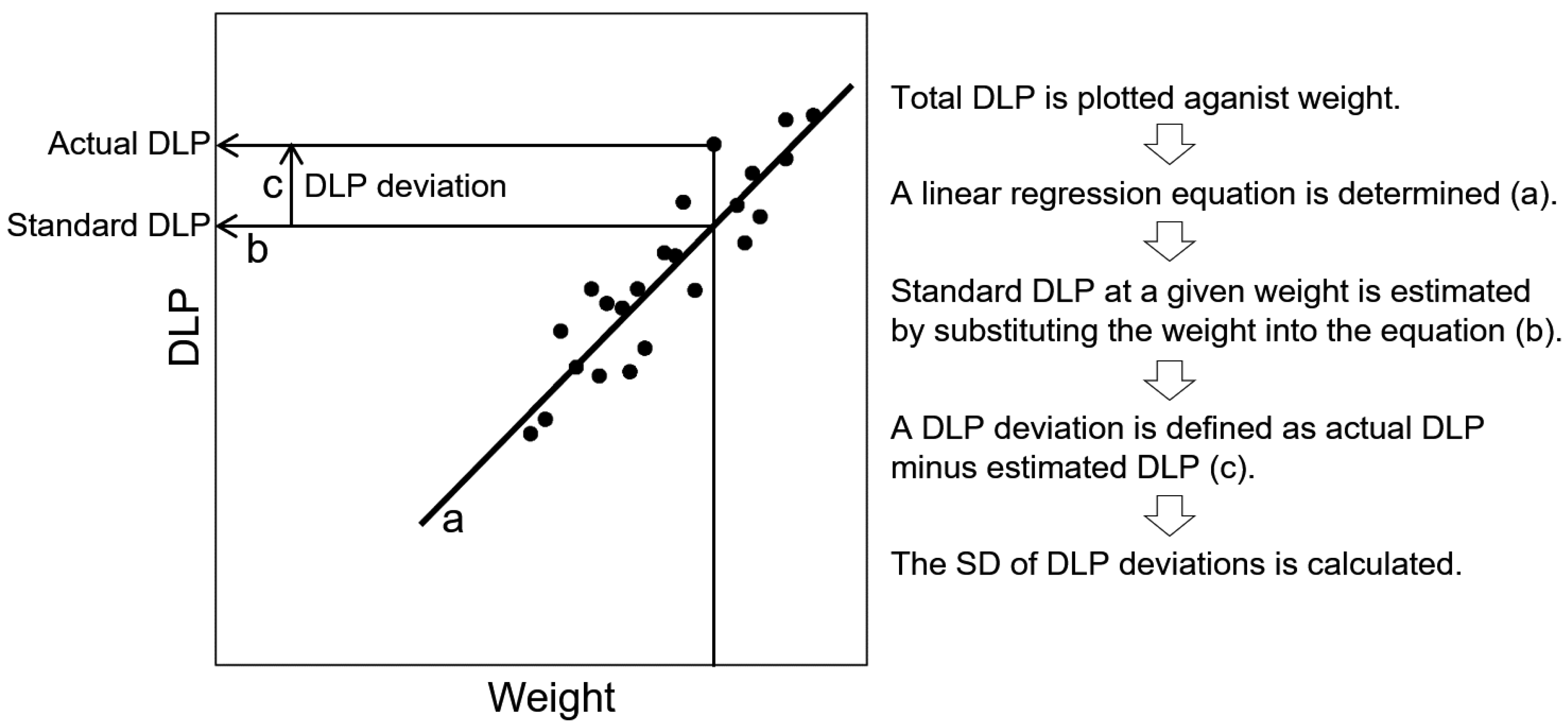
3.5. Standard Dose Tables for Radiation Dose Management
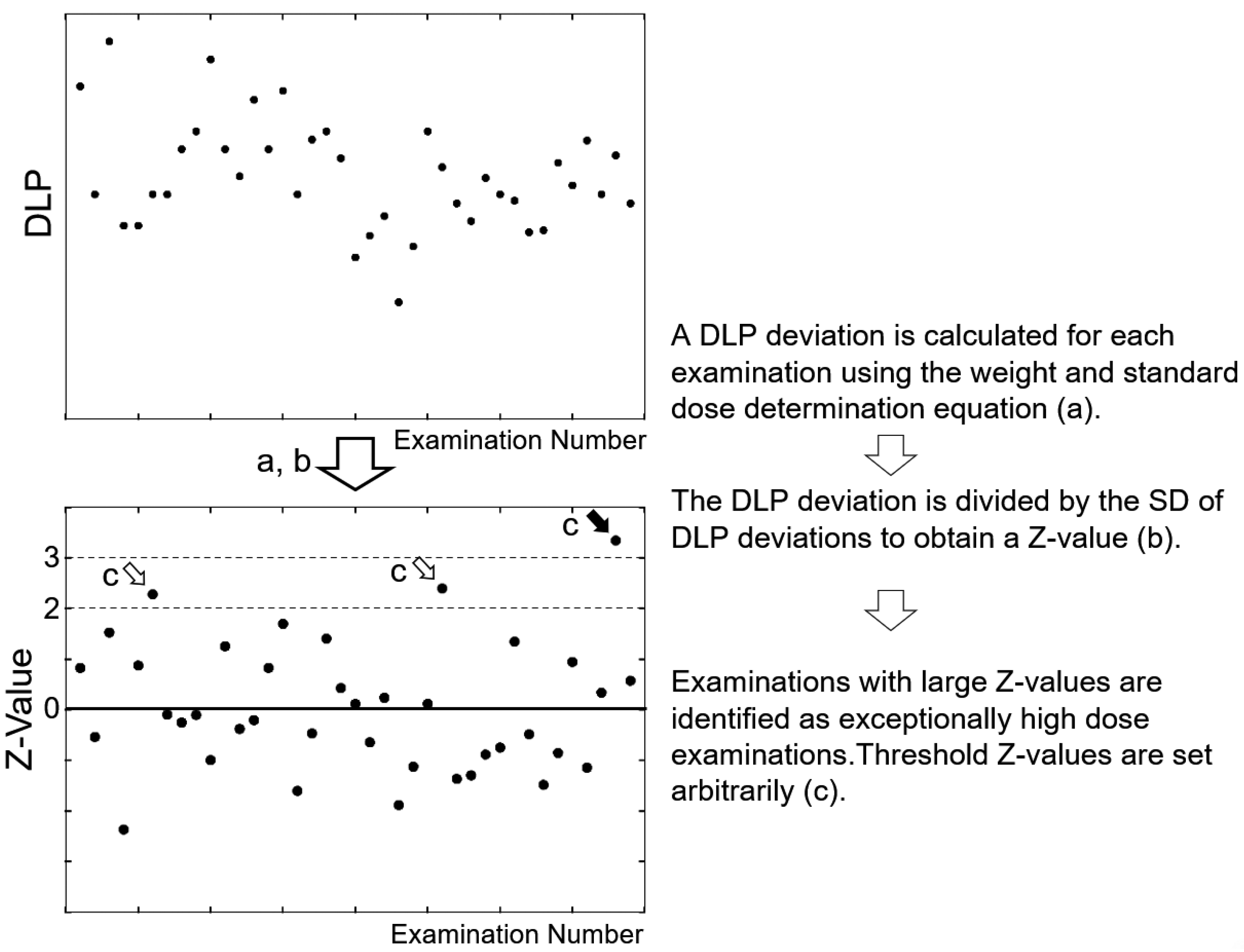
3.6. Identifying Examinations Delivering Exceptionally High Doses
3.7. Dose Reference Tables for Referring Physicians
4. Imaging Procedures Based on and toward Radiation Dose Management
4.1. Steps for Good CT Practice
4.2. Request for CT by the Referring Physician
4.3. Preparation on the Day before the Examination
4.4. Operation on the RIS during the Examination
4.5. Operation on the CT Console during the Examination
4.6. Recording at the End of the Examination
5. Daily Radiation Dose Management
5.1. Identification of Examinations to Be Investigated
5.2. Causes of Exceptionally High Doses
5.3. Problems with the Scan Range
5.4. Use of Water Equivalent Diameter
5.5. Problems with Weight Records
5.6. Limitation of the Analysis of DLP for Each Examination
5.7. Team Approach to Radiation Safety
6. Summary
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pearce, M.S.; Salotti, J.A.; Little, M.P.; McHugh, K.; Lee, C.; Kim, K.P.; Howe, N.L.; Ronckers, C.M.; Rajaraman, P.; Craft, A.W.; et al. Radiation exposure from CT scans in childhood and subsequent risk of leukaemia and brain tumours: A retrospective cohort study. Lancet 2012, 380, 499–505. [Google Scholar] [CrossRef]
- Mathews, J.D.; Forsythe, A.V.; Brady, Z.; Butler, M.W.; Goergen, S.K.; Byrnes, G.B.; Giles, G.G.; Wallace, A.B.; Anderson, P.R.; Guiver, T.A.; et al. Cancer risk in 680,000 people exposed to computed tomography scans in childhood or adolescence: Data linkage study of 11 million Australians. BMJ 2013, 346, f2360. [Google Scholar] [CrossRef]
- Meulepas, J.M.; Ronckers, C.M.; Smets, A.M.J.B.; Nievelstein, R.A.J.; Gradowska, P.; Lee, C.; Jahnen, A.; van Straten, M.; de Wit, M.Y.; Zonnenberg, B.; et al. Radiation exposure from pediatric CT scans and subsequent cancer risk in The Netherlands. J. Natl. Cancer Inst. 2019, 111, 256–263. [Google Scholar] [CrossRef] [PubMed]
- Brenner, D.J.; Hall, E.J. Computed tomography--an increasing source of radiation exposure. N. Engl. J. Med. 2007, 357, 2277–2284. [Google Scholar] [CrossRef]
- McCollough, C.H. The role of the medical physicist in managing radiation dose and communicating risk in CT. AJR Am. J. Roentgenol. 2016, 206, 1241–1244. [Google Scholar] [CrossRef] [PubMed]
- Caruana, C.J.; Tsapaki, V.; Damilakis, J.; Brambilla, M.; Martín, G.M.; Dimov, A.; Bosmans, H.; Egan, G.; Bacher, K.; McClean, B. EFOMP policy statement 16: The role and competences of medical physicists and medical physics experts under 2013/59/EURATOM. Phys. Med. 2018, 48, 162–168. [Google Scholar] [CrossRef] [PubMed]
- International Commission on Radiological Protection (ICRP). Diagnostic reference levels in medical imaging. ICRP Publication 135. Ann. ICRP 2017, 46, 1–144. [Google Scholar] [CrossRef]
- International Commission on Radiological Protection (ICRP). Radiological protection in paediatric diagnostic and interventional radiology. ICRP Publication 121. Ann. ICRP 2013, 42, 1–63. [Google Scholar] [CrossRef]
- International Commission on Radiological Protection (ICRP). Managing patient dose in multi-detector computed tomography(MDCT). ICRP Publication 102. Ann. ICRP 2007, 37, 1–79. [Google Scholar] [CrossRef]
- American Association of Physicists in Medicine (AAPM). Size-Specific Dose Estimates (SSDE) in Pediatric and Adult Body CT Examinations (Task Group 204); American Association of Physicists in Medicine: College Park, MD, USA, 2011. [Google Scholar]
- American Association of Physicists in Medicine (AAPM). Size Specific Dose Estimate (SSDE) for Head CT (Task Group 293); American Association of Physicists in Medicine: College Park, MD, USA, 2019. [Google Scholar]
- Lee, C.H.; Goo, J.M.; Ye, H.J.; Ye, S.J.; Park, C.M.; Chun, E.J.; Im, J.G. Radiation dose modulation techniques in the multidetector CT era: From basics to practice. Radiographics 2008, 28, 1451–1459. [Google Scholar] [CrossRef]
- Kalra, M.K.; Maher, M.M.; Toth, T.L.; Schmidt, B.; Westerman, B.L.; Morgan, H.T.; Saini, S. Techniques and applications of automatic tube current modulation for CT. Radiology 2004, 233, 649–657. [Google Scholar] [CrossRef]
- Inoue, Y. Radiation dose modulation of computed tomography component in positron emission tomography/computed tomography. Semin. Nucl. Med. 2022, 52, 157–166. [Google Scholar] [CrossRef]
- Granata, C.; Origgi, D.; Palorini, F.; Matranga, D.; Salerno, S. Radiation dose from multidetector CT studies in children: Results from the first Italian nationwide survey. Pediatr. Radiol. 2015, 45, 695–705. [Google Scholar] [CrossRef] [PubMed]
- Célier, D.; Roch, P.; Etard, C.; Ducou Le Pointe, H.; Brisse, H.J. Multicentre survey on patient dose in paediatric imaging and proposal for updated diagnostic reference levels for France. Part 1: Computed tomography. Eur. Radiol. 2020, 30, 1156–1165. [Google Scholar] [CrossRef]
- Inoue, Y.; Itoh, H.; Miyatake, H.; Hata, H.; Sasa, R.; Shiibashi, N.; Mitsui, K. Automatic exposure control attains radiation dose modulation matched with the head size in pediatric brain CT. Tomography 2022, 8, 2929–2938. [Google Scholar] [CrossRef] [PubMed]
- Yu, L.; Li, H.; Fletcher, J.G.; McCollough, C.H. Automatic selection of tube potential for radiation dose reduction in CT: A general strategy. Med. Phys. 2010, 37, 234–243. [Google Scholar] [CrossRef] [PubMed]
- Frellesen, C.; Stock, W.; Kerl, J.M.; Lehnert, T.; Wichmann, J.L.; Nau, C.; Geiger, E.; Wutzler, S.; Beeres, M.; Schulz, B.; et al. Topogram-based automated selection of the tube potential and current in thoraco-abdominal trauma CT—A comparison to fixed kV with mAs modulation alone. Eur. Radiol. 2014, 24, 1725–1734. [Google Scholar] [CrossRef]
- Inoue, Y.; Nagahara, K.; Hayakawa, N.; Hanawa, H.; Hata, H. Monitoring dose-length product in computed tomography of the chest considering sex and body weight. Radiat. Prot. Dosim. 2016, 171, 375–381. [Google Scholar] [CrossRef]
- Iball, G.R.; Tout, D. Computed tomography automatic exposure control techniques in 18F-FDG oncology PET-CT scanning. Nucl. Med. Commun. 2014, 35, 372–381. [Google Scholar] [CrossRef]
- Inoue, Y.; Takahashi, K.; Miyatake, H.; Nagahara, K.; Iwasaki, R. Factors affecting dose-length product of computed tomography component in whole-body positron emission tomography/computed tomography. J. Radiol. Prot. 2022, 42. in press. [Google Scholar] [CrossRef]
- Kanda, R.; Akahane, M.; Koba, Y.; Chang, W.; Akahane, K.; Okuda, Y.; Hosono, M. Developing diagnostic reference levels in Japan. Jpn. J. Radiol. 2021, 39, 307–314. [Google Scholar] [CrossRef]
- Kanal, K.M.; Butler, P.F.; Sengupta, D.; Bhargavan-Chatfield, M.; Coombs, L.P.; Morin, R.L. U.S. diagnostic reference levels and achievable doses fo 10 adult CT examinations. Radiology 2017, 284, 120–133. [Google Scholar] [CrossRef] [PubMed]
- Inoue, Y.; Itoh, H.; Waga, A.; Sasa, R.; Mitsui, K. Radiation dose management in pediatric brain CT according to age and weight as continuous variables. Tomography 2022, 82, 985–998. [Google Scholar] [CrossRef]
- Inoue, Y.; Nagahara, K.; Tanaka, Y.; Miyatake, H.; Hata, H.; Hara, T. Methods of CT dose estimation in whole-body ¹⁸F-FDG PET/CT. J. Nucl. Med. 2015, 56, 695–700. [Google Scholar] [CrossRef] [PubMed]
- Inoue, Y.; Nagahara, K.; Kudo, H.; Itoh, H. Effects of the scan range on radiation dose in the computed tomography component of oncology positron emission tomography/computed tomography. Radiat. Prot. Dosim. 2019, 185, 1–6. [Google Scholar] [CrossRef]
- Inoue, Y.; Ohkubo, Y.; Nagahara, K.; Uehara, A.; Takano, M. Conversion from dose length product to effective dose for the CT component of whole-body PET/CT. Ann. Nucl. Med. 2022, 36, 411–419. [Google Scholar] [CrossRef]
- Inoue, Y.; Itoh, H.; Nagahara, K.; Takahashi, Y. Estimation of radiation dose in ct venography of the lower extremities: Phantom experiments using different automatic exposure control settings and scan ranges. Radiat. Prot. Dosim. 2020, 188, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Inoue, Y.; Yonekura, Y.; Nagahara, K.; Uehara, A.; Ikuma, H. Conversion from dose-length product to effective dose in computed tomography venography of the lower extremities. J. Radiol. Prot. 2022, 42. in press. [Google Scholar] [CrossRef]
- American Association of Physicists in Medicine (AAPM). Use of Water Equivalent Diameter for Calculating Patient Size and Size-Specific Dose Estimates (SSDE) in CT (Task Group 220); American Association of Physicists in Medicine: College Park, MD, USA, 2014. [Google Scholar]
- Inoue, Y.; Nagahara, K.; Inoki, Y.; Hara, T.; Miyatake, H. Clinical evaluation of CT radiation dose in whole-body 18F-FDG PET/CT in relation to scout imaging direction and arm position. Ann. Nucl. Med. 2019, 33, 169–176. [Google Scholar] [CrossRef]
- Inoue, Y.; Adachi, M.; Shimizu, H.; Nagahara, K.; Itoh, H.; Takano, M.; Jinguji, K. Suboptimal modulation of radiation dose in the computed tomography component of whole-body positron emission tomography/computed tomography. Radiat. Prot. Dosim. 2020, 192, 69–74. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
|
|
Planned variance at pre-check
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Inoue, Y. Radiation Dose Management in Computed Tomography: Introduction to the Practice at a Single Facility. Tomography 2023, 9, 955-966. https://doi.org/10.3390/tomography9030078
Inoue Y. Radiation Dose Management in Computed Tomography: Introduction to the Practice at a Single Facility. Tomography. 2023; 9(3):955-966. https://doi.org/10.3390/tomography9030078
Chicago/Turabian StyleInoue, Yusuke. 2023. "Radiation Dose Management in Computed Tomography: Introduction to the Practice at a Single Facility" Tomography 9, no. 3: 955-966. https://doi.org/10.3390/tomography9030078
APA StyleInoue, Y. (2023). Radiation Dose Management in Computed Tomography: Introduction to the Practice at a Single Facility. Tomography, 9(3), 955-966. https://doi.org/10.3390/tomography9030078