

A Review of Computer-Aided Breast Cancer Diagnosis Using Sequential Mammograms


Abstract
1. Introduction
2. Review Methodology
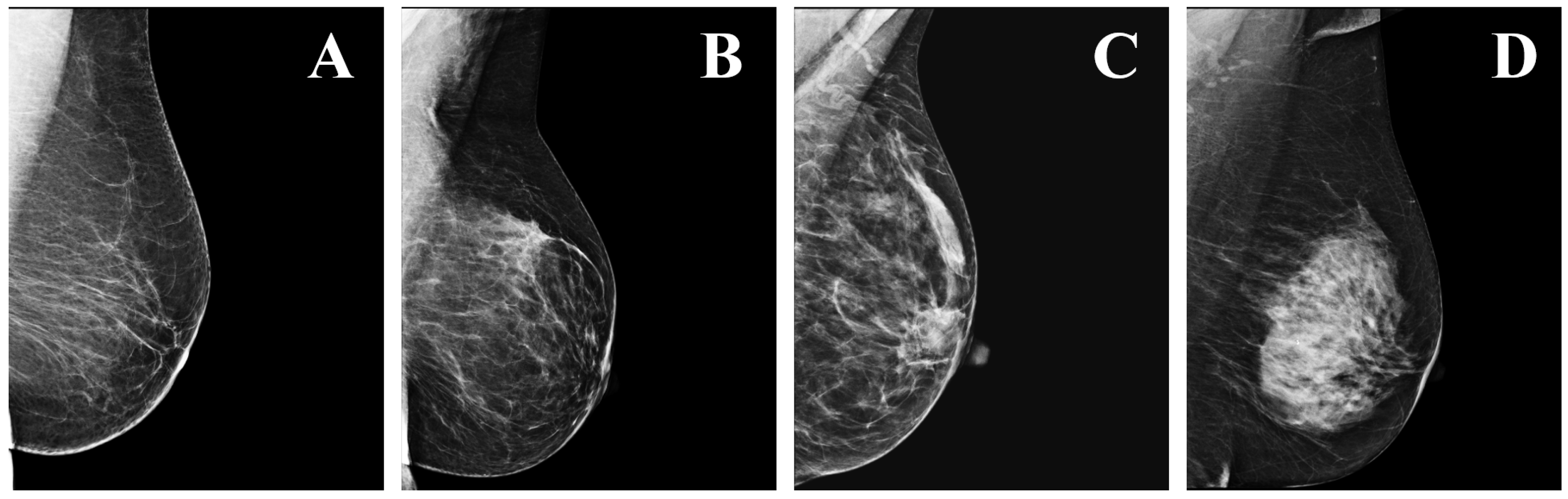
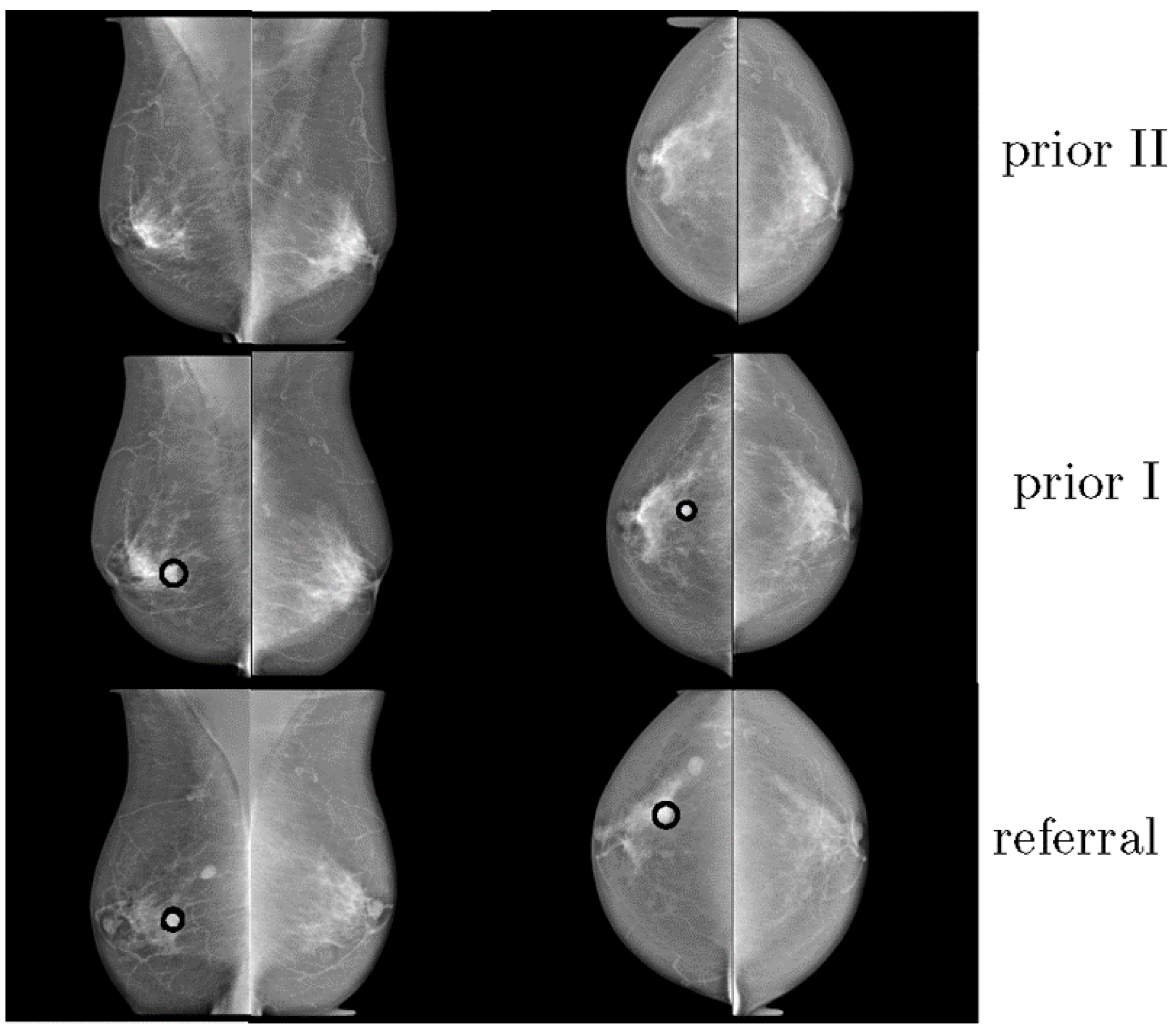
3. Importance of Prior Views
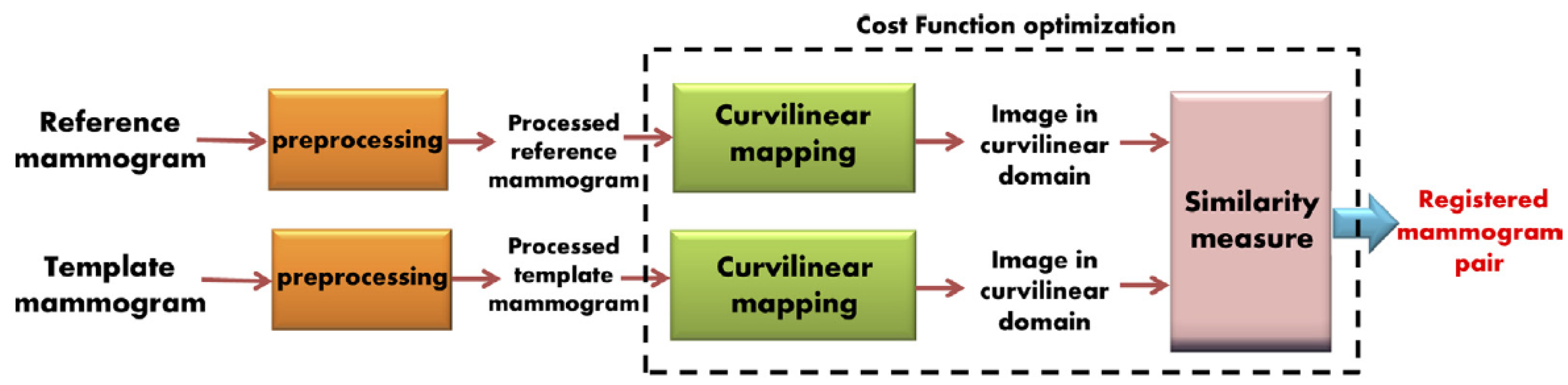
4. Registration
5. Temporal Analysis
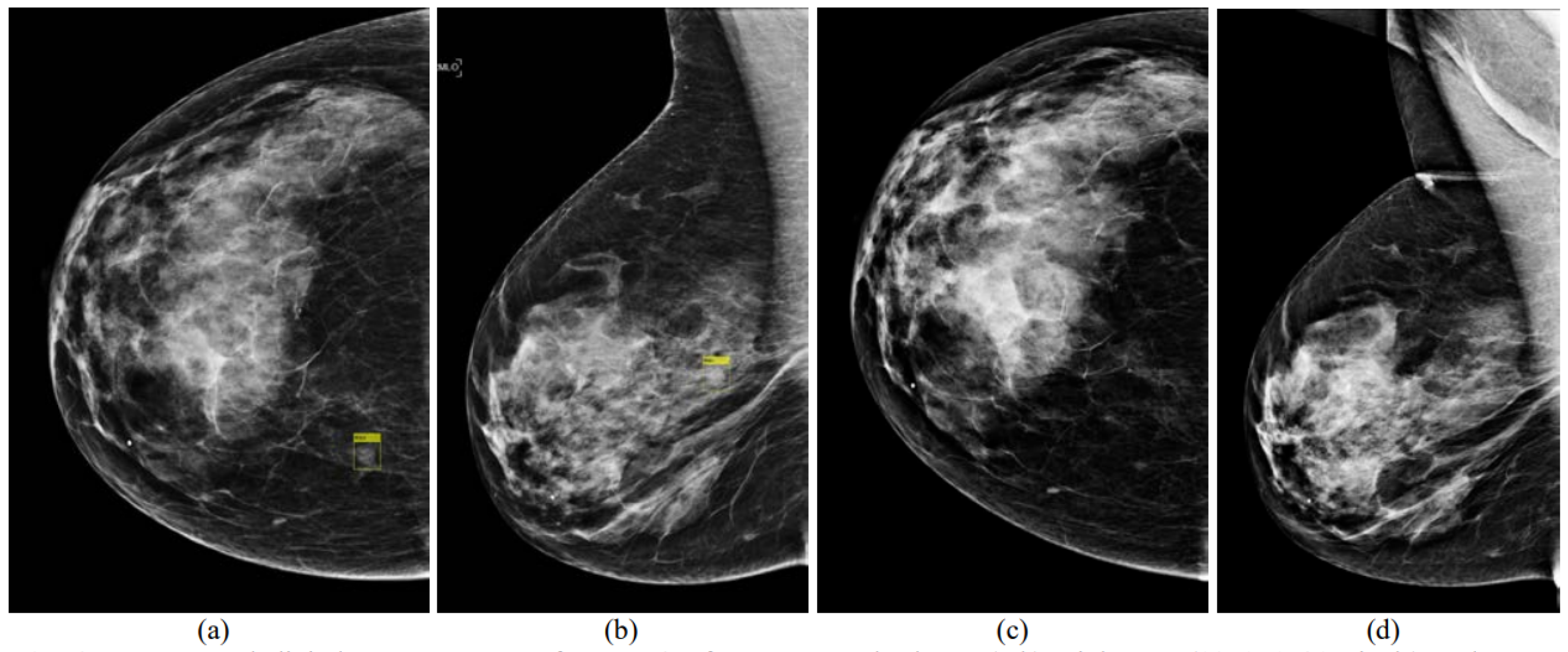
5.1. Detection of Breast Masses
5.2. Classification of Breast Masses
5.3. Detection of Micro-Calcifications (MCs)
5.4. Classification of Micro-Calcifications (MCs)
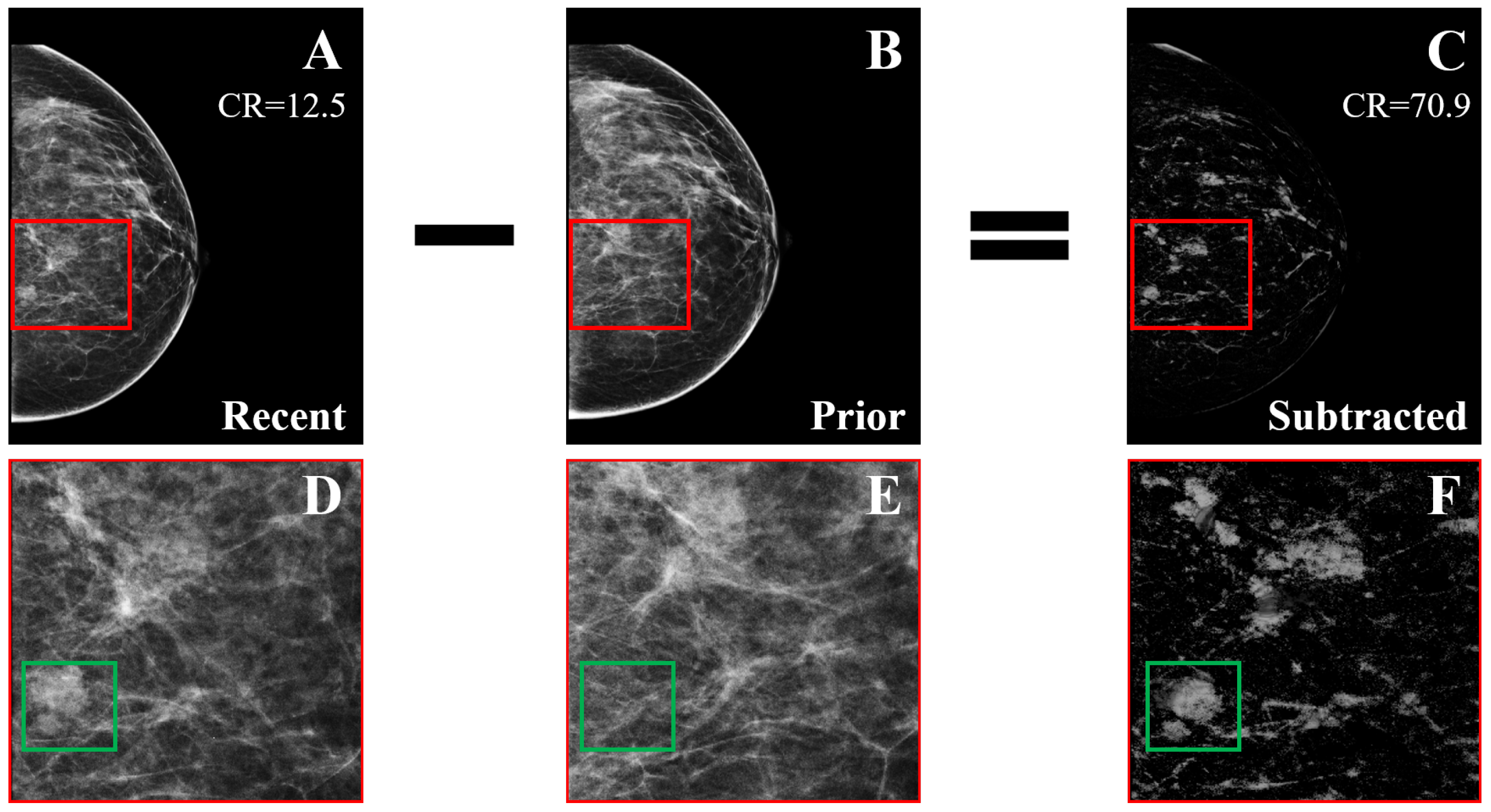
6. Temporal Subtraction
7. Open-Access Mammography Datasets
8. Discussion
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2022. CA Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Ganesan, K.; Acharya, U.R.; Chua, C.K.; Min, L.C.; Abraham, K.T.; Ng, K.H. Computer-aided breast cancer detection using mammograms: A review. IEEE Rev. Biomed. Eng. 2013, 6, 77–98. [Google Scholar] [CrossRef] [PubMed]
- Beura, S. Development of Features and Feature Reduction Techniques for Mammogram Classification. Ph.D. Thesis, Department of Computer Science and Engineering National Institute of Technology Rourkela, Odisha, India, 2016. [Google Scholar]
- Spak, D.A.; Plaxco, J.; Santiago, L.; Dryden, M.; Dogan, B. BI-RADS® fifth edition: A summary of changes. Diagn. Interv. Imaging 2017, 98, 179–190. [Google Scholar] [CrossRef] [PubMed]
- Breast Anatomy and How Cancer Starts. About Breast Cancer. Available online: https://nbcf.org.au/about-national-breast-cancer-foundation/about-breast-cancer/what-you-need-to-know/breast-anatomy-cancer-starts/ (accessed on 20 September 2020).
- Rangayyan, R.M.; Ayres, F.J.; Desautels, J.L. A review of computer-aided diagnosis of breast cancer: Toward the detection of subtle signs. J. Frankl. Inst. 2007, 344, 312–348. [Google Scholar] [CrossRef]
- Oliver, A.; Freixenet, J.; Marti, J.; Perez, E.; Pont, J.; Denton, E.R.; Zwiggelaar, R. A review of automatic mass detection and segmentation in mammographic images. Med. Image Anal. 2010, 14, 87–110. [Google Scholar] [CrossRef]
- Liu, X.; Zeng, Z. A new automatic mass detection method for breast cancer with false positive reduction. Neurocomputing 2015, 152, 388–402. [Google Scholar] [CrossRef]
- Xie, W.; Li, Y.; Ma, Y. Breast mass classification in digital mammography based on extreme learning machine. Neurocomputing 2016, 173, 930–941. [Google Scholar] [CrossRef]
- Zonderland, H.; Smithuis, R. BI-RADS for mammography and ultrasound 2013 updated version. Radiol. Assist. 2014. Available online: https://radiologyassistant.nl/breast/bi-rads/bi-rads-for-mammography-and-ultrasound-2013 (accessed on 1 December 2022).
- Castells, X.; Torá-Rocamora, I.; Posso, M.; Román, M.; Vernet-Tomas, M.; Rodríguez-Arana, A.; Domingo, L.; Vidal, C.; Baré, M.; Ferrer, J.; et al. Risk of breast cancer in women with false-positive results according to mammographic features. Radiology 2016, 280, 379–386. [Google Scholar] [CrossRef]
- Banik, S.; Rangayyan, R.M.; Desautels, J.L. Detection of architectural distortion in prior mammograms. IEEE Trans. Med. Imaging 2010, 30, 279–294. [Google Scholar] [CrossRef]
- Lehman, C.D.; Wellman, R.D.; Buist, D.S.; Kerlikowske, K.; Tosteson, A.N.; Miglioretti, D.L. Diagnostic accuracy of digital screening mammography with and without computer-aided detection. JAMA Intern. Med. 2015, 175, 1828–1837. [Google Scholar] [CrossRef]
- Nishikawa, R.M.; Kallergi, M.; Orton, C.G. Computer-aided detection, in its present form, is not an effective aid for screening mammography. Med. Phys. 2006, 33, 811–814. [Google Scholar] [CrossRef]
- Mohanty, F.; Rup, S.; Dash, B.; Majhi, B.; Swamy, M. A computer-aided diagnosis system using Tchebichef features and improved grey wolf optimized extreme learning machine. Appl. Intell. 2019, 49, 983–1001. [Google Scholar] [CrossRef]
- Al-Masni, M.A.; Al-Antari, M.A.; Park, J.M.; Gi, G.; Kim, T.Y.; Rivera, P.; Valarezo, E.; Choi, M.T.; Han, S.M.; Kim, T.S. Simultaneous detection and classification of breast masses in digital mammograms via a deep learning YOLO-based CAD system. Comput. Methods Programs Biomed. 2018, 157, 85–94. [Google Scholar] [CrossRef]
- Al-Antari, M.A.; Han, S.M.; Kim, T.S. Evaluation of deep learning detection and classification towards computer-aided diagnosis of breast lesions in digital X-ray mammograms. Comput. Methods Programs Biomed. 2020, 196, 105584. [Google Scholar] [CrossRef]
- Ma, F.; Bajger, M.; Williams, S.; Bottema, M.J. Improved detection of cancer in screening mammograms by temporal comparison. In Proceedings of the International Workshop on Digital Mammography; Springer: Girona, Catalonia, Spain, 2010; pp. 752–759. [Google Scholar]
- Hadjiiski, L.; Sahiner, B.; Chan, H.P.; Petrick, N.; Helvie, M.A.; Gurcan, M. Analysis of temporal changes of mammographic features: Computer-aided classification of malignant and benign breast masses. Med. Phys. 2001, 28, 2309–2317. [Google Scholar] [CrossRef]
- Doi, K. Computer-aided diagnosis in medical imaging: Historical review, current status and future potential. Comput. Med. Imaging Graph. 2007, 31, 198–211. [Google Scholar] [CrossRef]
- Cheng, H.D.; Cai, X.; Chen, X.; Hu, L.; Lou, X. Computer-aided detection and classification of microcalcifications in mammograms: A survey. Pattern Recognit. 2003, 36, 2967–2991. [Google Scholar] [CrossRef]
- Litjens, G.; Kooi, T.; Bejnordi, B.E.; Setio, A.A.A.; Ciompi, F.; Ghafoorian, M.; Van Der Laak, J.A.; Van Ginneken, B.; Sánchez, C.I. A survey on deep learning in medical image analysis. Med. Image Anal. 2017, 42, 60–88. [Google Scholar] [CrossRef]
- Abdelrahman, L.; Al Ghamdi, M.; Collado-Mesa, F.; Abdel-Mottaleb, M. Convolutional neural networks for breast cancer detection in mammography: A survey. Comput. Biol. Med. 2021, 131, 104248. [Google Scholar] [CrossRef]
- Timp, S.; Varela, C.; Karssemeijer, N. Computer-aided diagnosis with temporal analysis to improve radiologists’ interpretation of mammographic mass lesions. IEEE Trans. Inf. Technol. Biomed. 2010, 14, 803–808. [Google Scholar] [CrossRef]
- Gelig Thurfjell, M.; Vitak, B.; Azavedo, E.; Svane, G.; Thurfjell, E. Effect on sensitivity and specificity of mammography screening with or without comparison of old mammograms. Acta Radiol. 2000, 41, 52–56. [Google Scholar] [CrossRef]
- Varela, C.; Karssemeijer, N.; Hendriks, J.H.; Holland, R. Use of prior mammograms in the classification of benign and malignant masses. Eur. J. Radiol. 2005, 56, 248–255. [Google Scholar] [CrossRef] [PubMed]
- Hadjiiski, L.; Sahiner, B.; Helvie, M.A.; Chan, H.P.; Roubidoux, M.A.; Paramagul, C.; Blane, C.; Petrick, N.; Bailey, J.; Klein, K.; et al. Breast masses: Computer-aided diagnosis with serial mammograms. Radiology 2006, 240, 343–356. [Google Scholar] [CrossRef] [PubMed]
- Marias, K.; Behrenbruch, C.; Parbhoo, S.; Seifalian, A.; Brady, M. A registration framework for the comparison of mammogram sequences. IEEE Trans. Med. Imaging 2005, 24, 782–790. [Google Scholar] [CrossRef] [PubMed]
- Zitova, B.; Flusser, J. Image registration methods: A survey. Image Vis. Comput. 2003, 21, 977–1000. [Google Scholar] [CrossRef]
- Guo, Y.; Sivaramakrishna, R.; Lu, C.C.; Suri, J.S.; Laxminarayan, S. Breast image registration techniques: A survey. Med. Biol. Eng. Comput. 2006, 44, 15–26. [Google Scholar] [CrossRef]
- Oliveira, F.P.; Tavares, J.M.R. Medical image registration: A review. Comput. Methods Biomech. Biomed. Eng. 2014, 17, 73–93. [Google Scholar] [CrossRef]
- Díez, Y.; Oliver, A.; Lladó, X.; Martí, R. Comparison of registration methods using mamographic images. In Proceedings of the 2010 IEEE International Conference on Image Processing, Hong Kong, China, 26–29 September 2010; pp. 4421–4424. [Google Scholar]
- Rueckert, D.; Sonoda, L.I.; Hayes, C.; Hill, D.L.; Leach, M.O.; Hawkes, D.J. Nonrigid registration using free-form deformations: Application to breast MR images. IEEE Trans. Med. Imaging 1999, 18, 712–721. [Google Scholar] [CrossRef]
- Arsigny, V.; Pennec, X.; Ayache, N. Polyrigid and polyaffine transformations: A novel geometrical tool to deal with non-rigid deformations–application to the registration of histological slices. Med. Image Anal. 2005, 9, 507–523. [Google Scholar] [CrossRef]
- Thirion, J.P. Image matching as a diffusion process: An analogy with Maxwell’s demons. Med. Image Anal. 1998, 2, 243–260. [Google Scholar] [CrossRef]
- van Engeland, S.; Snoeren, P.; Hendriks, J.; Karssemeijer, N. A comparison of methods for mammogram registration. IEEE Trans. Med. Imaging 2003, 22, 1436–1444. [Google Scholar] [CrossRef]
- Vujovic, N.; Brzakovic, D. Establishing the correspondence between control points in pairs of mammographic images. IEEE Trans. Image Process. 1997, 6, 1388–1399. [Google Scholar] [CrossRef][Green Version]
- Marti, R.; Zwiggelaar, R.; Rubin, C. Automatic mammographic registration: Towards the detection of abnormalities. In Proceedings of the S T1U Conference on Medical Image Understanding and Analysis, Birmingham, UK, 16–17 July 2001; pp. 149–152. [Google Scholar]
- Sanjay-Gopal, S.; Chan, H.P.; Wilson, T.; Helvie, M.; Petrick, N.; Sahiner, B. A regional registration technique for automated interval change analysis of breast lesions on mammograms. Med. Phys. 1999, 26, 2669–2679. [Google Scholar] [CrossRef]
- Filev, P.; Hadjiiski, L.; Chan, H.P.; Sahiner, B.; Ge, J.; Helvie, M.A.; Roubidoux, M.; Zhou, C. Automated regional registration and characterization of corresponding microcalcification clusters on temporal pairs of mammograms for interval change analysis. Med. Phys. 2008, 35, 5340–5350. [Google Scholar] [CrossRef]
- Ma, F.; Yu, L.; Bajger, M.; Bottema, M.J. Incorporation of fuzzy spatial relation in temporal mammogram registration. Fuzzy Sets Syst. 2015, 279, 87–100. [Google Scholar] [CrossRef]
- Wirth, M.A.; Narhan, J.; Gray, D.W. Nonrigid mammogram registration using mutual information. In Proceedings of the Medical Imaging 2002: Image Processing, San Diego, CA, USA, 24–28 February 2002; International Society for Optics and Photonics: Bellingham, WA, USA, 2002; Volume 4684, pp. 562–573. [Google Scholar]
- Timp, S.; Karssemeijer, N. Interval change analysis to improve computer aided detection in mammography. Med. Image Anal. 2006, 10, 82–95. [Google Scholar] [CrossRef]
- Li, C.; Chen, Z.; Zhang, H. Multi-Individual Mammographic Image Registration Based on Global-Local Integrated Transformations. In Proceedings of the 2018 IEEE 9th International Conference on Software Engineering and Service Science (ICSESS), Beijing, China, 23–25 November 2018; pp. 983–986. [Google Scholar]
- Abdel-Nasser, M.; Moreno, A.; Puig, D. Temporal mammogram image registration using optimized curvilinear coordinates. Comput. Methods Programs Biomed. 2016, 127, 1–14. [Google Scholar] [CrossRef]
- M.N. Kumar, A.; M.N. Kumar, A.; S. Sheshadri, H. Computer Aided Detection of Clustered Microcalcification: A Survey. Curr. Med. Imaging 2019, 15, 132–149. [Google Scholar] [CrossRef]
- Mendel, K.; Li, H.; Tayob, N.; El-Zein, R.; Bedrosian, I.; Giger, M. Temporal mammographic registration for evaluation of architecture changes in cancer risk assessment. In Proceedings of the Medical Imaging 2019: Computer-Aided Diagnosis. International Society for Optics and Photonics, San Diego, CA, USA, 17–20 February 2019; Volume 10950, p. 1095041. [Google Scholar]
- Sharma, M.K.; Jas, M.; Karale, V.; Sadhu, A.; Mukhopadhyay, S. Mammogram Segmentation using Multi-atlas Deformable Registration. Comput. Biol. Med. 2019, 110, 244–253. [Google Scholar] [CrossRef]
- Shanmugavadivu, P.; Sivakumar, V.; Sudhir, R. Fractal dimension-bound spatio-temporal analysis of digital mammograms. Eur. Phys. J. Spec. Top. 2016, 225, 137–146. [Google Scholar] [CrossRef]
- Zheng, B.; Good, W.F.; Armfield, D.R.; Cohen, C.; Hertzberg, T.; Sumkin, J.H.; Gur, D. Performance change of mammographic CAD schemes optimized with most-recent and prior image databases. Acad. Radiol. 2003, 10, 283–288. [Google Scholar] [CrossRef] [PubMed]
- Ma, F.; Yu, L.; Liu, G.; Niu, Q. Computer Aided Mass Detection in Mammography with temporal change analysis. Comput. Sci. Inf. Syst. 2015, 12, 1255–1272. [Google Scholar] [CrossRef]
- Zheng, Y.; Yang, C.; Merkulov, A. Breast cancer screening using convolutional neural network and follow-up digital mammography. In Proceedings of the Computational Imaging III, International Society for Optics and Photonics, Orlando, FL, USA; 2018; Volume 10669, p. 1066905. [Google Scholar]
- Kooi, T.; Karssemeijer, N. Classifying symmetrical differences and temporal change for the detection of malignant masses in mammography using deep neural networks. J. Med. Imaging 2017, 4, 044501. [Google Scholar] [CrossRef] [PubMed]
- Timp, S.; Varela, C.; Karssemeijer, N. Temporal change analysis for characterization of mass lesions in mammography. IEEE Trans. Med. Imaging 2007, 26, 945–953. [Google Scholar] [CrossRef] [PubMed]
- Bozek, J.; Kallenberg, M.; Grgic, M.; Karssemeijer, N. Use of volumetric features for temporal comparison of mass lesions in full field digital mammograms. Med. Phys. 2014, 41, 021902. [Google Scholar] [CrossRef]
- Hadjiiski, L.M.; Chan, H.P.; Sahiner, B.; Petrick, N.; Helvie, M.A.; Roubidoux, M.A.; Gurcan, M.N. Computer-aided characterization of malignant and benign microcalcification clusters based on the analysis of temporal change of mammographic features. In Proceedings of the Medical Imaging 2002: Image Processing SPIE, San Diego, CA, USA, 24–28 February 2002; Volume 4684, pp. 749–753. [Google Scholar]
- Loizidou, K.; Skouroumouni, G.; Nikolaou, C.; Pitris, C. An automated breast micro-calcification detection and classification technique using temporal subtraction of mammograms. IEEE Access 2020, 8, 52785–52795. [Google Scholar] [CrossRef]
- Loizidou, K.; Skouroumouni, G.; Pitris, C.; Nikolaou, C. Digital subtraction of temporally sequential mammograms for improved detection and classification of microcalcifications. Eur. Radiol. Exp. 2021, 5, 1–12. [Google Scholar] [CrossRef]
- Breast Micro-Calcifications Dataset with Precisely Annotated Sequential Mammograms|Zenodo, 2021. Available online: https://doi.org/10.5281/zenodo.5036062 (accessed on 20 September 2022).
- Loizidou, K.; Skouroumouni, G.; Nikolaou, C.; Pitris, C. Automatic Breast Mass Segmentation and Classification Using Subtraction of Temporally Sequential Digital Mammograms. IEEE J. Transl. Eng. Health Med. 2022, 10, 1–11. [Google Scholar] [CrossRef]
- Breast Masses Dataset with Precisely Annotated Sequential Mammograms|Zenodo, 2022. Available online: https://doi.org/10.5281/zenodo.7179856 (accessed on 13 October 2022).
- Loizidou, K.; Skouroumouni, G.; Savvidou, G.; Constantinidou, A.; Nikolaou, C.; Pitris, C. Identification and Classification of Benign and Malignant Masses based on Subtraction of Temporally Sequential Digital Mammograms. In Proceedings of the 2022 44th Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Glasgow, UK, 11–15 July 2022; pp. 1667–1670. [Google Scholar]
- PUB, M.H.; Bowyer, K.; Kopans, D.; Moore, R.; Kegelmeyer, P. The digital database for screening mammography. In Proceedings of the Third International Workshop on Digital Mammography, Chicago, IL, USA, 9–12 June 1996; Volume 58, p. 27. [Google Scholar]
- Suckling J, P. The mammographic image analysis society digital mammogram database. Digit. Mammo 1994, 375–386. [Google Scholar]
- Moreira, I.C.; Amaral, I.; Domingues, I.; Cardoso, A.; Cardoso, M.J.; Cardoso, J.S. Inbreast: Toward a full-field digital mammographic database. Acad. Radiol. 2012, 19, 236–248. [Google Scholar] [CrossRef]
- Lopez, M.G.; Posada, N.; Moura, D.C.; Pollán, R.R.; Valiente, J.M.F.; Ortega, C.S.; Solar, M.; Diaz-Herrero, G.; Ramos, I.; Loureiro, J.; et al. BCDR: A breast cancer digital repository. In Proceedings of the 15th International Conference on Experimental Mechanics, Porto, Portugal, 22–27 July 2012; Volume 1215. [Google Scholar]
- CBIS-DDSM—The Cancer Imaging Archive (TCIA) Public Access—Cancer Imaging Archive Wiki. 2021. Available online: https://wiki.cancerimagingarchive.net/display/Public/CBIS-DDSM (accessed on 27 January 2022).
- DoD BCRP Spiculated Mass Detection Evaluation Data. Available online: http://www.eng.usf.edu/cvprg/mammography/DDSM/BCRP/bcrp_mass_01.html (accessed on 27 January 2022).
- Halling-Brown, M.D.; Warren, L.M.; Ward, D.; Lewis, E.; Mackenzie, A.; Wallis, M.G.; Wilkinson, L.S.; Given-Wilson, R.M.; McAvinchey, R.; Young, K.C. OPTIMAM mammography image database: A large-scale resource of mammography images and clinical data. Radiol. Artif. Intell. 2020, 3, e200103. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Registration Category | Reference | Details |
|---|---|---|
| Global | van Engeland et al. (2003) [36] | joint probability intensity distribution |
| Local | Vujovic and Brzakovic (1997) [37] Sanjay-Gopal et al. (1999) [39] Marti et al. (2001) [38] Hadjiiski et al. (2001) [19] Filev et al. (2008) [40] Ma et al. (2015) [41] | modified monotony operator and accumulator matrix associated information between regions correspondence between linear structures affine transformation and nonlinear optimization corresponding local search spatial relationships and graph matching |
| Hybrid | Wirth et al. (2002) [42] Timp and Karssemeijer (2006) [43] Abdel-Nasser et al. (2016) [45] Li et al. (2018) [44] Sharma et al. (2019) [48] Mendel et al. (2019) [47] | similarity and point-based spatial transformation center of mass alignment and feature space mapping curvilinear coordinates; global/local deformations global coarse and local fine registration data-driven clustering and deformable registration B-splines and multi-resolution registration |
| Reference | Database | Type of Images | Dataset | Classifier | Validation Method | Result: ACC (%) | Result: SEN/SPEC (%) | Result: AUC | Result: Other |
|---|---|---|---|---|---|---|---|---|---|
| Zheng et al. (2003) [50] | Restricted | Digitized | 134 pairs | ANN | 75–25% (per image) | - | - | 0.89 temporal 0.68 single | - |
| Timp and Karssemeijer (2006) [43] | Restricted | Digitized | 2873 pairs | ANN | 10-fold CV (per patient) | - | - | 0.72 temporal 0.71 single | - |
| Ma et al. (2015) [51] | Restricted | Digitized | 95 pairs | SMV LDA | 5-fold CV (per ???) | - | - | 0.9 temporal 0.88 single | - |
| Reference | Database | Type of Images | Dataset | Data Augmentation | Classifier | Validation Method | Result: ACC (%) | Result: SEN/SPEC (%) | Result: AUC | Result: Other |
|---|---|---|---|---|---|---|---|---|---|---|
| Kooi and Karssemeijer (2017) [53] | Restricted | Digital | 18366 pairs | YES | CNN (shallow gradient boosted tree) | 16-fold CV (per patient) | - | - | 0.88 temporal 0.87 single | - |
| Zheng et al. (2018) [52] | Restricted | Digital | 96 pairs | NO | CNN (VGG-19) | 10 × 75–25% (per image) | - | 92.8/99.1 | - | 0.004 FPi |
| Reference | Database | Type of Images | Dataset | Classifier | Validation Method | Result: ACC (%) | Result: SEN/SPEC (%) | Result: AUC | Result: Other |
|---|---|---|---|---|---|---|---|---|---|
| Hadjiiski et al. (2001) [19] | Restricted | Digitized | 140 pairs | LDA | leave-one-out (per patient) | - | - | 0.88 temporal 0.82 single | - |
| Timp et al. (2007) [54] | Restricted | Digitized | 465 pairs | SVM | 20-fold CV (per ???) | - | - | 0.77 temporal 0.74 single | - |
| Bozek et al. (2014) [55] | Restricted | Digital | 60 pairs | LDA | leave-one-out CV (per ???) | - | - | 0.90 temporal 0.77 single | - |
| Reference | Database | Type of Images | Dataset | Classifier | Validation Method | Result: ACC (%) | Result: SEN/SPEC (%) | Result: AUC | Result: Other |
|---|---|---|---|---|---|---|---|---|---|
| Detection | |||||||||
| Filev et al. (2008) [40] | Restricted | Digitized | 261 pairs | LDA | leave-one-out (per patient) | 91.2 | - | - | 0.72 FPs per image |
| Classification | |||||||||
| Hadjiiski et al. (2002) [56] | Restricted | Digitized | 65 pairs | LDA | leave-one-out (per patient) | - | - | 0.87 temporal 0.81 single | - |
| Filev et al. (2008) [40] | Restricted | Digitized | 261 pairs | LDA | leave-one-out (per patient) | - | - | 0.81 temporal 0.72 single | - |
| Reference | Database | Type of Images | Dataset | Classifier | Validation Method | Result: ACC (%) | Result: SEN/SPEC (%) | Result: AUC | Result: Other |
|---|---|---|---|---|---|---|---|---|---|
| Detection | |||||||||
| Loizidou et al. (2021) [58] | Open access | Digital | 100 pairs | Voting | leave-one-out (per patient) | 94.1 | 81.4/95.5 | 0.88 | - |
| Classification | |||||||||
| Loizidou et al. (2021) [58] | Open access | Digital | 100 pairs | ANN | leave-one-out (per patient) | 90.3 | 81.6/92.2 | 0.87 | - |
| Reference | Database | Type of Images | Dataset | Classifier | Validation Method | Result: ACC (%) | Result: SEN/SPEC (%) | Result: AUC | Result: Other |
|---|---|---|---|---|---|---|---|---|---|
| Detection | |||||||||
| Loizidou et al. (2022) [60] | Open access | Digital | 80 pairs | ANN | leave-one-out (per patient) | 99.9 | 96.6/99.9 | 0.98 | - |
| Classification | |||||||||
| Loizidou et al. (2022) [60] | Open access | Digital | 80 pairs | ANN | leave-one-out (per patient) | 98 | 99/96.1 | 0.98 | - |
| Name | Origin | Year | File Access | Number of Cases | Number of Images | Resolution (bits/pixel) | Image Mode | Type of Abnormality | Image Categories | Annotation |
|---|---|---|---|---|---|---|---|---|---|---|
| DDSM [63] | USA | 1999 | Open | 2620 | 10480 | 8 or 16 | Digitized | ALL | Normal Benign Malignant | Contour points of the ROI |
| MIAS [64] | UK | 2003 | Open | 161 | 322 | 8 | Digitized | ALL | Normal Benign Malignant | Center and radius of a circle around ROI |
| INbreast [65] | Portugal | 2011 | Approval from authors | 115 | 410 | 14 | Digital | Masses Calcifications Distortions Asymmetries | Normal Benign Malignant | Contour points of the ROI |
| BCDR-FM [66] | Portugal | 2012 | Open (requires registration) | 1125 | 3703 | 8 | Digitized | ALL | Normal Cancer | Precise lesion locations and mass coordinates, detailed segmentation outlines |
| BCDR-DM [66] | Portugal | 2012 | Open (requires registration) | 1042 | 3612 | 14 | Digital | ALL | Normal Cancer | Precise lesion locations and mass coordinates, detailed segmentation outlines |
| CBIS-DDSM [67] | USA | 2017 | Open | 1566 | 10239 | 8 or 16 | Digitized | Mass Calcifications | Benign Malignant | ROI segmentation and bounding boxes |
| DDSM-BCRP [68] | USA | 2000 | Open | 179 | 716 | 12 | Digitized | Masses Calcifications | Benign Malignant | Contour points of the ROI |
| OPTIMAM [69] | UK | 2020 | Approval from authors | - | 2889312 | 12 or 16 | Digital | ALL | Normal Benign Malignant | Rectangular around the boundaries of the ROI |
| SDM-MCs [59] | Cyprus | 2021 | Open | 100 | 400 | 12 | Digital | Calcifications | Normal Benign Suspicious | Precise annotation of each micro-calcification |
| SDM-Masses [61] | Cyprus | 2022 | Open | 80 | 320 | 12 | Digital | Masses | Normal Benign Malignant | Precise annotation of each mass |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Loizidou, K.; Skouroumouni, G.; Nikolaou, C.; Pitris, C. A Review of Computer-Aided Breast Cancer Diagnosis Using Sequential Mammograms. Tomography 2022, 8, 2874-2892. https://doi.org/10.3390/tomography8060241
Loizidou K, Skouroumouni G, Nikolaou C, Pitris C. A Review of Computer-Aided Breast Cancer Diagnosis Using Sequential Mammograms. Tomography. 2022; 8(6):2874-2892. https://doi.org/10.3390/tomography8060241
Chicago/Turabian StyleLoizidou, Kosmia, Galateia Skouroumouni, Christos Nikolaou, and Costas Pitris. 2022. "A Review of Computer-Aided Breast Cancer Diagnosis Using Sequential Mammograms" Tomography 8, no. 6: 2874-2892. https://doi.org/10.3390/tomography8060241
APA StyleLoizidou, K., Skouroumouni, G., Nikolaou, C., & Pitris, C. (2022). A Review of Computer-Aided Breast Cancer Diagnosis Using Sequential Mammograms. Tomography, 8(6), 2874-2892. https://doi.org/10.3390/tomography8060241