

Evaluation of the Effects of R-CHOP Chemotherapy on Brain Glucose Metabolism in Patients with Diffuse Large B Cell Lymphoma: A Baseline, Interim, and End-of-Treatment PET/CT Study


Abstract
1. Background
2. Methods
2.1. Patients
2.2. PET/CT Scans
2.3. PET/CT Data Analysis
3. Results
3.1. Patients and Characteristics
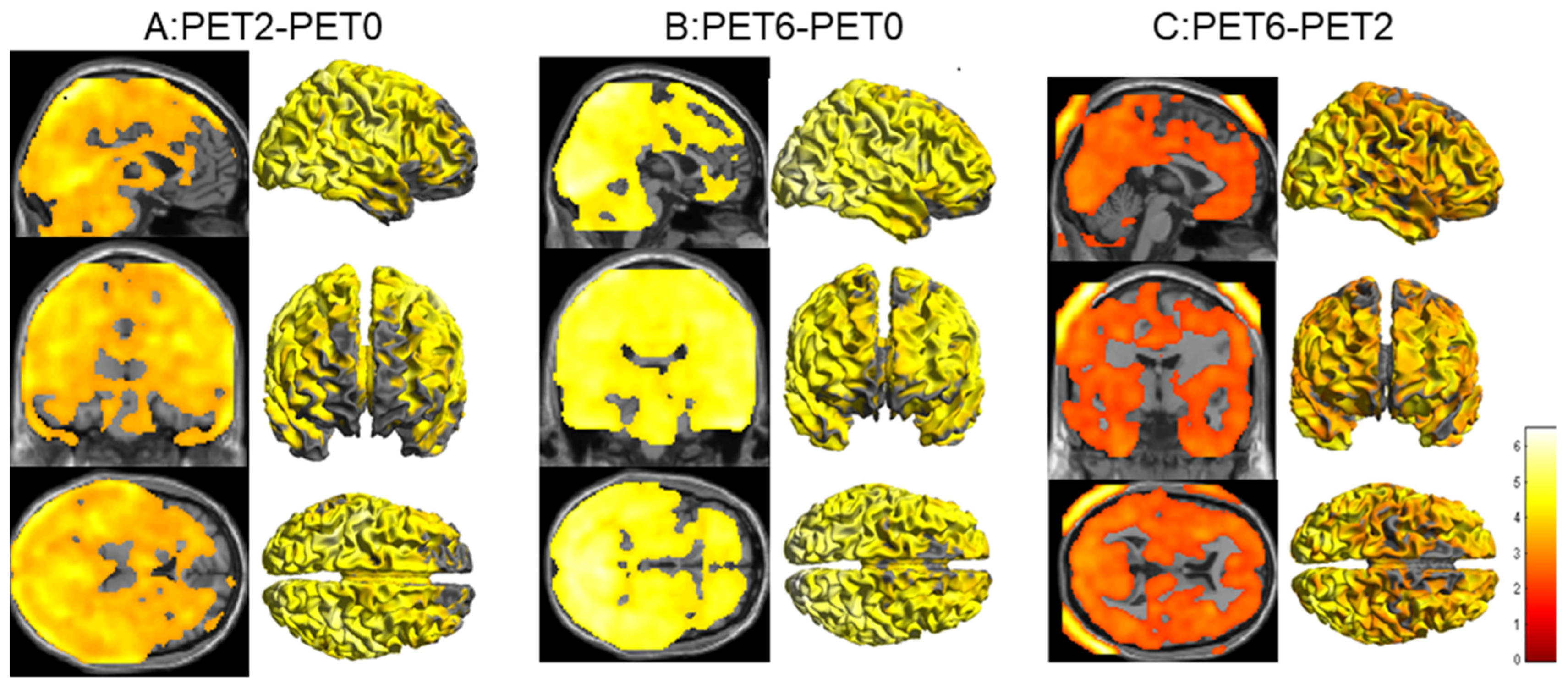
3.2. Comparison of Brain Metabolism at Baseline (PET0) and in the Interim of (PET2) Chemotherapy
3.3. Comparison of Brain Metabolism at Baseline (PET0), in the Interim of (PET2), and at the End of (PET6) Chemotherapy
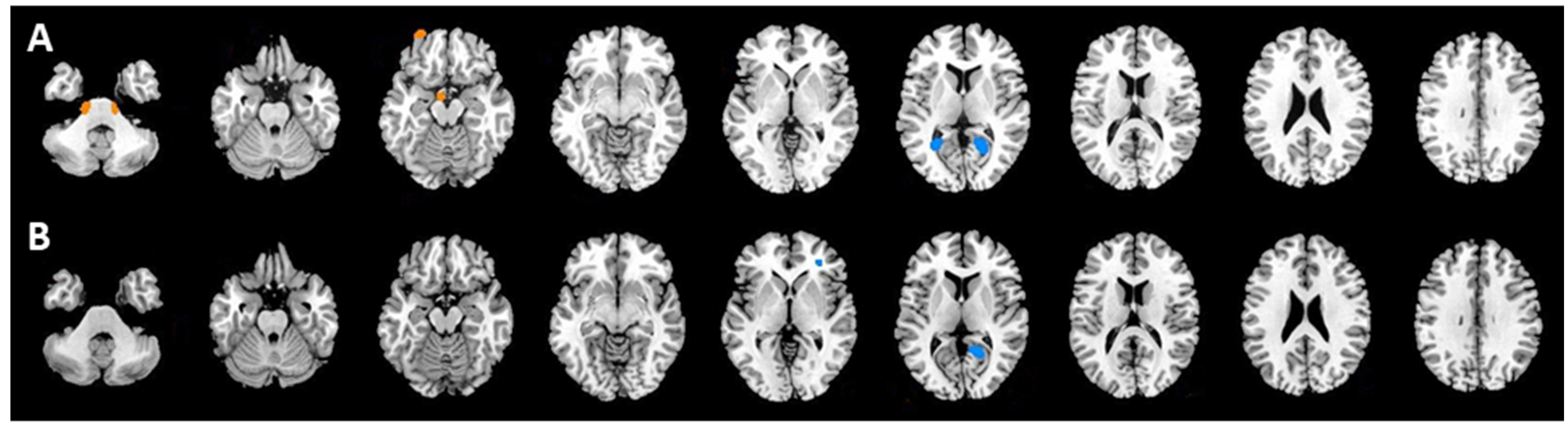
3.4. Correlations between Brain Glucose Metabolism Changes and Therapeutic Responses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Cheson, B.D.; Fisher, R.I.; Barrington, S.F.; Cavalli, F.; Schwartz, L.H.; Zucca, E.; Lister, T.A. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: The Lugano classification. J. Clin. Oncol. 2014, 32, 3059–3068. [Google Scholar] [CrossRef] [PubMed]
- Simo, M.; Rifa-Ros, X.; Rodriguez-Fornells, A.; Bruna, J. Chemobrain: A systematic review of structural and functional neuroimaging studies. Neurosci. Biobehav. Rev. 2013, 37, 1311–1321. [Google Scholar] [CrossRef] [PubMed]
- Allart-Vorelli, P.; Porro, B.; Baguet, F.; Michel, A.; Cousson-Gélie, F. Haematological cancer and quality of life: A systematic literature review. Blood Cancer J. 2015, 5, e305. [Google Scholar] [CrossRef] [PubMed]
- Chen, V.C.; Lin, T.Y.; Yeh, D.C.; Chai, J.W.; Weng, J.C. Predicting chemo-brain in breast cancer survivors using multiple MRI features and machine-learning. Magn. Reson. Med. 2019, 81, 3304–3313. [Google Scholar] [CrossRef]
- Williams, A.M.; Zent, C.S.; Janelsins, M.C. What is known and unknown about chemotherapy-related cognitive impairment in patients with haematological malignancies and areas of needed research. Br. J. Haematol. 2016, 174, 835–846. [Google Scholar] [CrossRef]
- O’Farrell, E.; MacKenzie, J.; Collins, B. Clearing the air: A review of our current understanding of “chemo fog”. Curr. Oncol. Rep. 2013, 15, 260–269. [Google Scholar] [CrossRef]
- Wang, X.M.; Walitt, B.; Saligan, L.; Tiwari, A.F.; Cheung, C.W.; Zhang, Z.J. Chemobrain: A critical review and causal hypothesis of link between cytokines and epigenetic reprogramming associated with chemotherapy. Cytokine 2015, 72, 86–96. [Google Scholar] [CrossRef]
- Ren, X.; Boriero, D.; Chaiswing, L.; Bondada, S.; St Clair, D.K.; Butterfield, D.A. Plausible biochemical mechanisms of chemotherapy-induced cognitive impairment (“chemobrain”), a condition that significantly impairs the quality of life of many cancer survivors. Biochim. Biophys. Acta Mol. Basis Dis. 2019, 1865, 1088–1097. [Google Scholar] [CrossRef]
- Seigers, R.; Schagen, S.B.; Van Tellingen, O.; Dietrich, J. Chemotherapy related cognitive dysfunction: Current animal studies and future directions. Brain Imaging Behav. 2013, 7, 453–459. [Google Scholar] [CrossRef]
- Khan, M.A.; Garg, K.; Bhurani, D.; Agarwal, N.B. Early manifestation of mild cognitive impairment in B-cell non-Hodgkin’s lymphoma patients receiving CHOP and rituximab-CHOP chemotherapy. Naunyn Schmiedebergs Arch. Pharmacol. 2016, 389, 1253–1265. [Google Scholar] [CrossRef] [PubMed]
- Chiaravalloti, A.; Pagani, M.; Di Pietro, B.; Danieli, R.; Tavolozza, M.; Travascio, L.; Caracciolo, C.R.; Simonetti, G.; Cantonetti, M.; Schillaci, O. Is cerebral glucose metabolism affected by chemotherapy in patients with Hodgkin’s lymphoma? Nucl. Med. Commun. 2013, 34, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Nonokuma, M.; Kuwabara, Y.; Takano, K.; Tamura, K.; Ishitsuka, K.; Yoshimitsu, K. Evaluation of regional cerebral glucose metabolism in patients with malignant lymphoma of the body using statistical image analysis. Ann. Nucl. Med. 2014, 28, 950–960. [Google Scholar] [CrossRef] [PubMed]
- Adams, H.J.; de Klerk, J.M.; Fijnheer, R.; Heggelman, B.G.; Dubois, S.V.; Nievelstein, R.A.; Kwee, T.C. Brain glucose metabolism in diffuse large B-cell lymphoma patients as assessed with FDG-PET: Impact on outcome and chemotherapy effects. Acta Radiol. 2016, 57, 733–741. [Google Scholar] [CrossRef] [PubMed]
- Joshi, S.; Ergin, A.; Wang, M.; Reif, R.; Zhang, J.; Bruce, J.N.; Bigio, I.J. Inconsistent blood brain barrier disruption by intraarterial mannitol in rabbits: Implications for chemotherapy. J. Neurooncol. 2011, 104, 11–19. [Google Scholar] [CrossRef]
- Graus, F.; Ariño, H.; Dalmau, J. Paraneoplastic neurological syndromes in Hodgkin and non-Hodgkin lymphomas. Blood 2014, 123, 3230–3238. [Google Scholar] [CrossRef]
- Nizamutdinov, D.; Patel, N.P.; Huang, J.H.; Fonkem, E. Intravascular Lymphoma in the CNS: Options for Treatment. Curr. Treat. Options Neurol. 2017, 19, 35. [Google Scholar] [CrossRef] [PubMed]
- Geffen, D.B.; Blaustein, A.; Amir, M.C.; Cohen, Y. Post-traumatic stress disorder and quality of life in long-term survivors of Hodgkin’s disease and non-Hodgkin’s lymphoma in Israel. Leuk Lymphoma 2003, 44, 1925–1929. [Google Scholar] [CrossRef]
- Shrot, S.; Abebe-Campino, G.; Toren, A.; Ben-Haim, S.; Hoffmann, C.; Davidson, T. Fluorodeoxyglucose detected changes in brain metabolism after chemotherapy in pediatric non-hodgkin lymphoma. Pediatr. Neurol. 2019, 92, 37–42. [Google Scholar] [CrossRef]
- Zimmer, P.; Mierau, A.; Bloch, W.; Strüder, H.K.; Hülsdünker, T.; Schenk, A.; Fiebig, L.; Baumann, F.T.; Hahn, M.; Reinart, N.; et al. Post-chemotherapy cognitive impairment in patients with B-cell non-Hodgkin lymphoma: A first comprehensive approach to determine cognitive impairments after treatment with rituximab, cyclophosphamide, doxorubicin, vincristine and prednisone or rituximab and bendamustine. Leuk Lymphoma 2015, 56, 347–352. [Google Scholar] [CrossRef]
- Pomykala, K.L.; Ganz, P.A.; Bower, J.E.; Kwan, L.; Castellon, S.A.; Mallam, S.; Cheng, I.; Ahn, R.; Breen, E.C.; Irwin, M.R.; et al. The association between pro-inflammatory cytokines, regional cerebral metabolism, and cognitive complaints following adjuvant chemotherapy for breast cancer. Brain Imaging Behav. 2013, 7, 511–523. [Google Scholar] [CrossRef]
- Jung, J.; Kang, J.; Won, E.; Nam, K.; Lee, M.S.; Tae, W.S.; Ham, B.J. Impact of lingual gyrus volume on antidepressant response and neurocognitive functions in Major Depressive Disorder: A voxel-based morphometry study. J. Affect. Disord. 2014, 169, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Myers, J.S. Chemotherapy-related cognitive impairment: Neuroimaging, neuropsychological testing, and the neuropsychologist. Clin. J. Oncol. Nurs. 2009, 13, 413–421. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | Data |
|---|---|
| Age (mean ± standard deviations) | 47.8 ± 16.7 (18–81) |
| No. of male patients | 40 (55.6%) |
| No. of female patients | 32 (44.4%) |
| Ann Arbor Stage | |
| I–II | 35 (48.6%) |
| III–IV | 37 (51.4%) |
| IPI | |
| Low risk (0–1) | 44 (61.1%) |
| Low-intermediate risk (2) | 14 (19.4%) |
| High-intermediate risk (3) | 10 (13.9%) |
| High risk (4–5) | 4 (5.6%) |
| B symptoms | |
| Positive | 31 (43.1%) |
| Negative | 41 (56.9%) |
| Germinal center (GC) | |
| GC | 30 (41.7%) |
| Non-GC | 42 (58.3%) |
| Comparison | Region | Talairach Coordinates | T Score | p Values (Uncorrected) | ||
|---|---|---|---|---|---|---|
| x | y | z | ||||
| CR&NonCR (PET2) | ||||||
| hypermetabolism | Right pons 1 | 10 | −26 | −50 | 1.96 | 0.026 |
| Right pons 2 | 16 | −24 | −44 | 1.95 | 0.027 | |
| Left pons | −14 | −24 | −40 | 1.76 | 0.041 | |
| hypometabolism | Right lingual gyrus | 28 | −56 | 8 | 2.12 | 0.018 |
| Left lingual gyrus | −20 | −56 | 8 | 2.33 | 0.011 | |
| CR&NonCR (PET6) | ||||||
| hypometabolism | Left lingual gyrus | −18 | −54 | 8 | 2.30 | 0.011 |
| Left inferior frontal gyrus | −32 | −38 | 2 | 2.55 | 0.006 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhu, H.; Li, F.; Chang, Y.; Sun, Y.; Wang, N.; Wang, R. Evaluation of the Effects of R-CHOP Chemotherapy on Brain Glucose Metabolism in Patients with Diffuse Large B Cell Lymphoma: A Baseline, Interim, and End-of-Treatment PET/CT Study. Tomography 2022, 8, 2565-2573. https://doi.org/10.3390/tomography8050214
Zhu H, Li F, Chang Y, Sun Y, Wang N, Wang R. Evaluation of the Effects of R-CHOP Chemotherapy on Brain Glucose Metabolism in Patients with Diffuse Large B Cell Lymphoma: A Baseline, Interim, and End-of-Treatment PET/CT Study. Tomography. 2022; 8(5):2565-2573. https://doi.org/10.3390/tomography8050214
Chicago/Turabian StyleZhu, Haiyan, Fei Li, Yan Chang, Yabing Sun, Nan Wang, and Ruimin Wang. 2022. "Evaluation of the Effects of R-CHOP Chemotherapy on Brain Glucose Metabolism in Patients with Diffuse Large B Cell Lymphoma: A Baseline, Interim, and End-of-Treatment PET/CT Study" Tomography 8, no. 5: 2565-2573. https://doi.org/10.3390/tomography8050214
APA StyleZhu, H., Li, F., Chang, Y., Sun, Y., Wang, N., & Wang, R. (2022). Evaluation of the Effects of R-CHOP Chemotherapy on Brain Glucose Metabolism in Patients with Diffuse Large B Cell Lymphoma: A Baseline, Interim, and End-of-Treatment PET/CT Study. Tomography, 8(5), 2565-2573. https://doi.org/10.3390/tomography8050214