
Prostate Cancer Detection with mpMRI According to PI-RADS v2 Compared with Systematic MRI/TRUS-Fusion Biopsy: A Prospective Study

Abstract
:1. Introduction
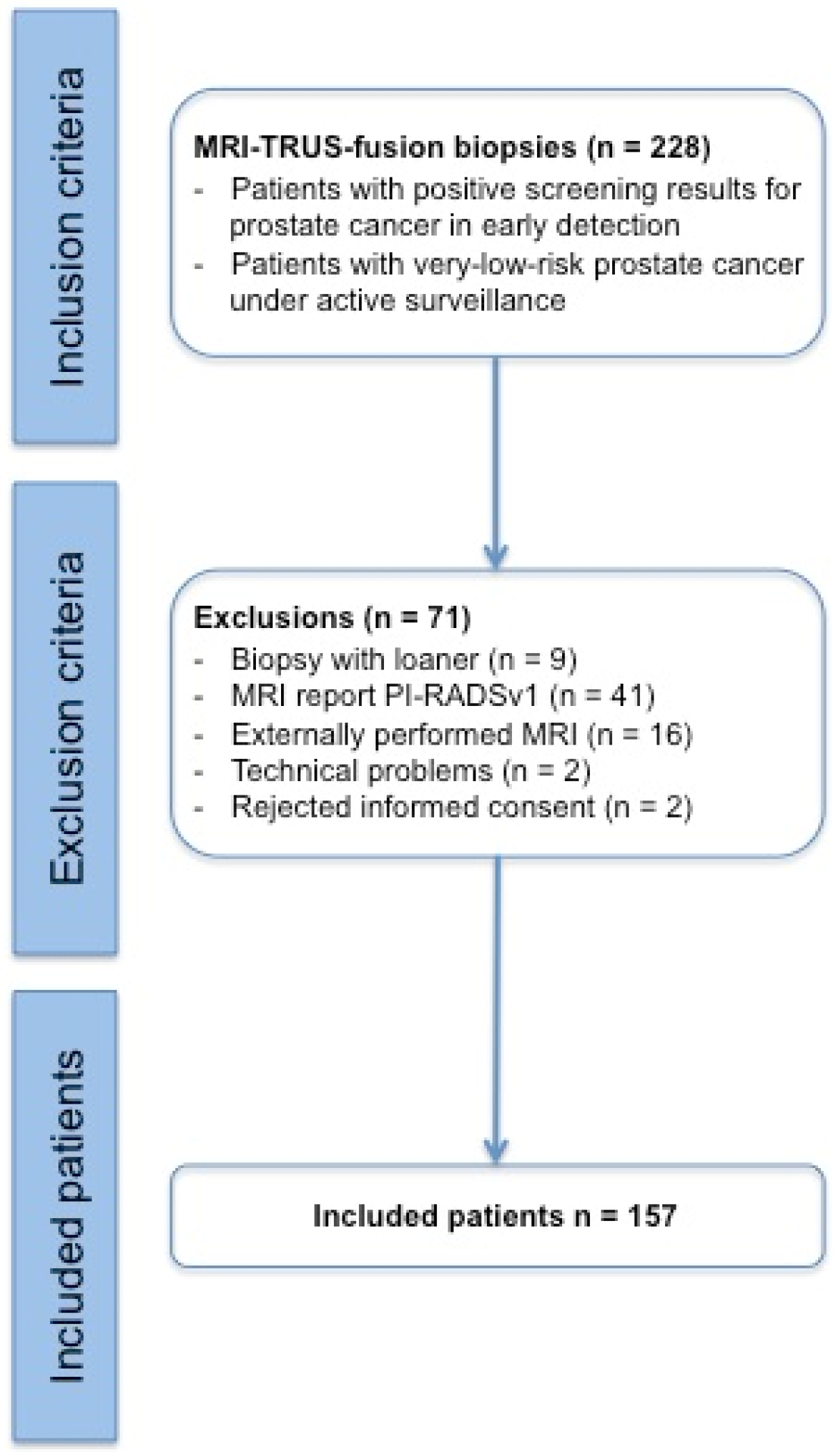
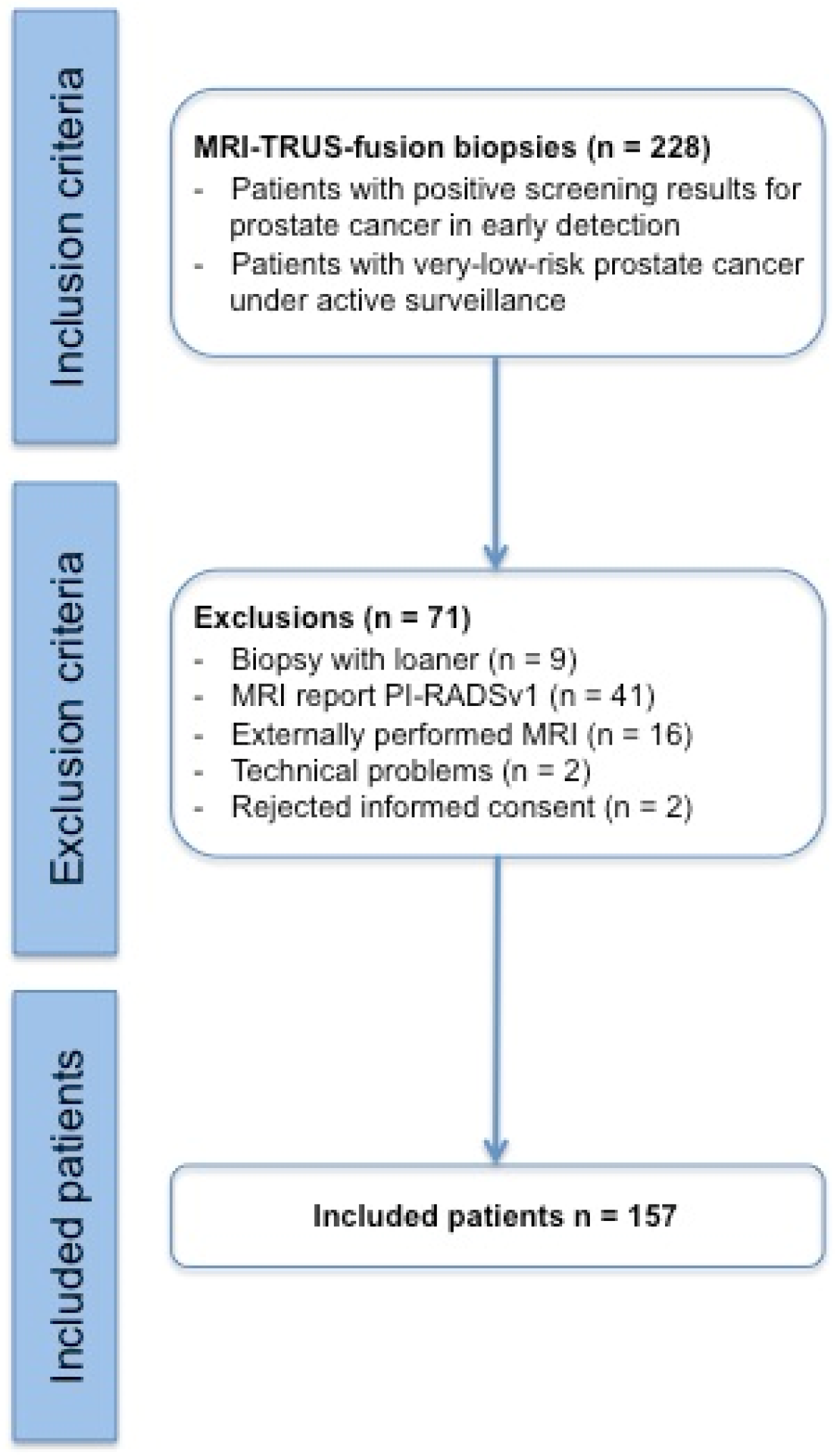
2. Materials and Methods
3. Results
3.1. MRI Lesions Reported with
3.1.1. PI-RADS v2 Score 5
3.1.2. PI-RADS v2 Score 4
3.1.3. PI-RADS v2 Score 3
3.1.4. PI-RADS v2 Score 2
3.2. Inconspicuous mpMRI Examinations and Biopsies Outside of Lesions
3.3. Sensitivity and Specificity of mpMRI for Prostate Cancer Detection
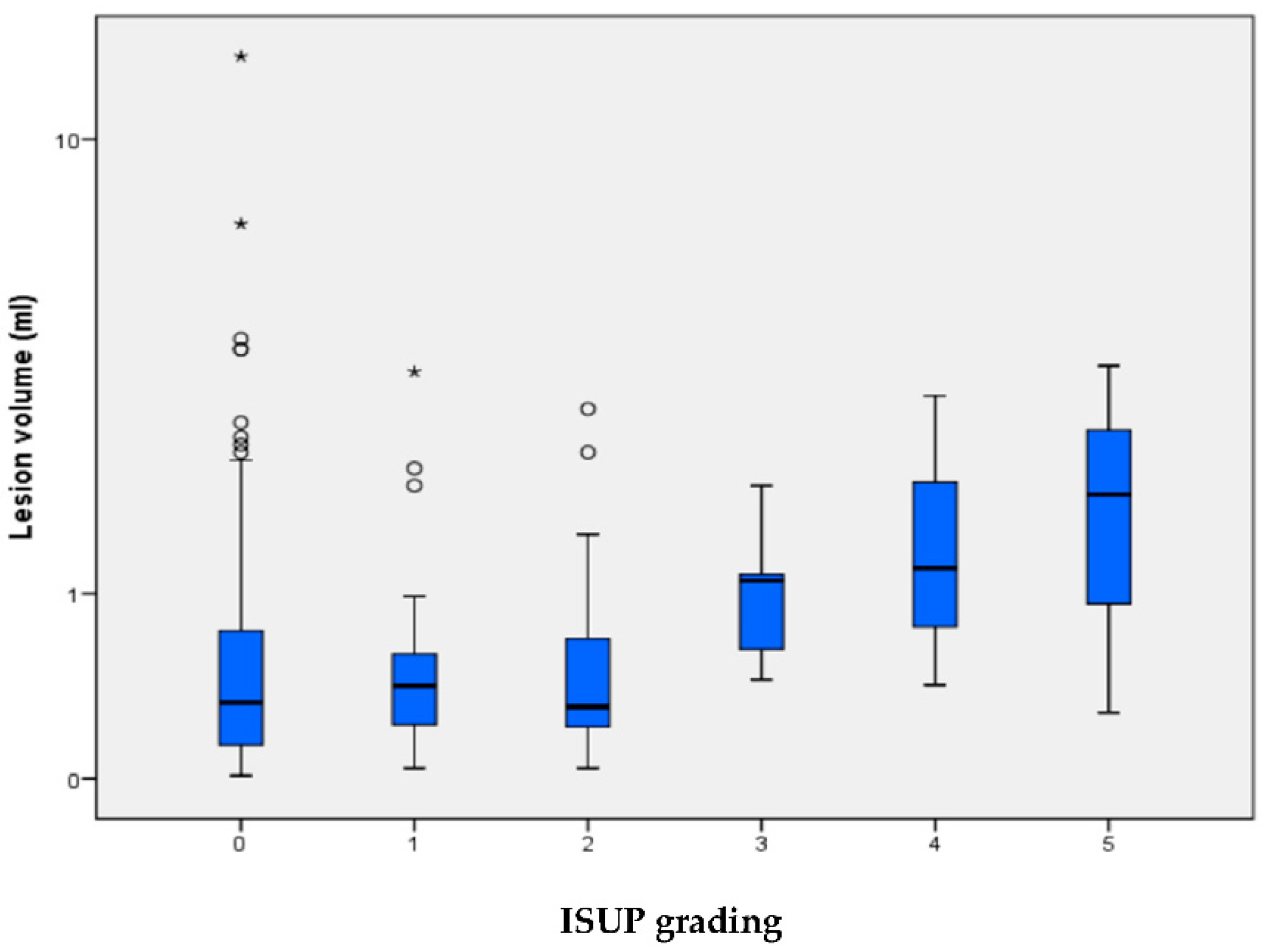
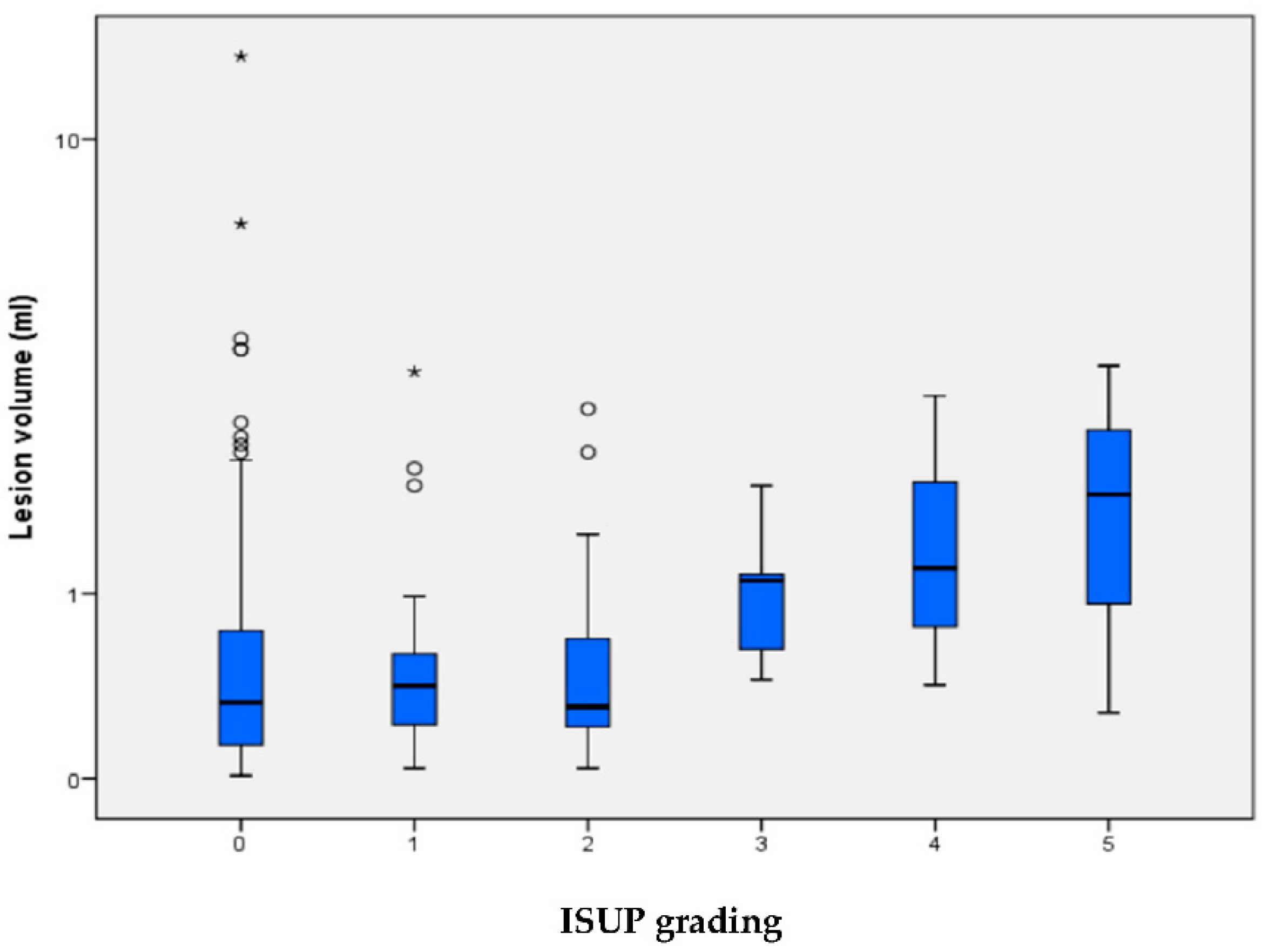
3.4. MRI Lesion Volume Relation with ISUP Grades and Cancer Prediction
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- Haas, G.P.; Delongchamps, N.; Brawley, O.W.; Wang, C.Y.; de la Roza, G. The worldwide epidemiology of prostate cancer: Perspectives from autopsy studies. Can. J. Urol. 2008, 15, 3866–3871. [Google Scholar] [PubMed]
- Siegel, R.; DeSantis, C.; Virgo, K.; Stein, K.; Mariotto, A.; Smith, T.; Cooper, D.; Gansler, T.; Lerro, C.; Fedewa, S.; et al. Cancer treatment and survivorship statistics, 2012. CA Cancer J. Clin. 2012, 62, 220–241. [Google Scholar] [CrossRef] [PubMed]
- Rawla, P. Epidemiology of Prostate Cancer. World J. Oncol. 2019, 10, 63–89. [Google Scholar] [CrossRef] [PubMed]
- Heidenreich, A.; Bastian, P.J.; Bellmunt, J.; Bolla, M.; Joniau, S.; van der Kwast, T.; Mason, M.; Matveev, V.; Wiegel, T.; Zattoni, F.; et al. EAU guidelines on prostate cancer. part 1: Screening, diagnosis, and local treatment with curative intent-update 2013. Eur. Urol. 2014, 65, 124–137. [Google Scholar] [CrossRef] [PubMed]
- Hoeks, C.M.; Barentsz, J.O.; Hambrock, T.; Yakar, D.; Somford, D.M.; Heijmink, S.W.; Scheenen, T.W.; Vos, P.C.; Huisman, H.; van Oort, I.M.; et al. Prostate cancer: Multiparametric MR imaging for detection, localization, and staging. Radiology 2011, 261, 46–66. [Google Scholar] [CrossRef] [PubMed]
- Hamoen, E.H.; de Rooij, M.; Witjes, J.A.; Barentsz, J.O.; Rovers, M.M. Use of the Prostate Imaging Reporting and Data System (PI-RADS) for Prostate Cancer Detection with Multiparametric Magnetic Resonance Imaging: A Diagnostic Meta-analysis. Eur. Urol. 2015, 67, 1112–1121. [Google Scholar] [CrossRef]
- Weinreb, J.C.; Barentsz, J.O.; Choyke, P.L.; Cornud, F.; Haider, M.A.; Macura, K.J.; Margolis, D.; Schnall, M.D.; Shtern, F.; Tempany, C.M.; et al. PI-RADS Prostate Imaging—Reporting and Data System: 2015, Version 2. Eur. Urol. 2016, 69, 16–40. [Google Scholar] [CrossRef]
- Barentsz, J.O.; Richenberg, J.; Clements, R.; Choyke, P.; Verma, S.; Villeirs, G.; Rouviere, O.; Logager, V.; Futterer, J.J. ESUR prostate MR guidelines 2012. Eur. Radiol. 2012, 22, 746–757. [Google Scholar] [CrossRef]
- Renard Penna, R.; Brenot-Rossi, I.; Salomon, L.; Soulie, M. Prostate cancer imaging: MRI and nuclear imaging. Prog. Urol. 2015, 25, 933–946. [Google Scholar] [CrossRef]
- Roethke, M.C.; Kuru, T.H.; Schultze, S.; Tichy, D.; Kopp-Schneider, A.; Fenchel, M.; Schlemmer, H.P.; Hadaschik, B.A. Evaluation of the ESUR PI-RADS scoring system for multiparametric MRI of the prostate with targeted MR/TRUS fusion-guided biopsy at 3.0 Tesla. Eur. Radiol. 2014, 24, 344–352. [Google Scholar] [CrossRef] [PubMed]
- Schimmoller, L.; Quentin, M.; Arsov, C.; Lanzman, R.S.; Hiester, A.; Rabenalt, R.; Antoch, G.; Albers, P.; Blondin, D. Inter-reader agreement of the ESUR score for prostate MRI using in-bore MRI-guided biopsies as the reference standard. Eur. Radiol. 2013, 23, 3185–3190. [Google Scholar] [CrossRef] [PubMed]
- Kuru, T.H.; Herden, J.; Zugor, V.; Akbarov, I.; Pfister, D.; Porres, D.; Heidenreich, A. How to Perform Image-guided Prostate Biopsy: In-bore and Fusion Approaches. Eur. Urol. Focus 2016, 2, 151–153. [Google Scholar] [CrossRef] [PubMed]
- Arsov, C.; Rabenalt, R.; Blondin, D.; Quentin, M.; Hiester, A.; Godehardt, E.; Gabbert, H.E.; Becker, N.; Antoch, G.; Albers, P.; et al. Prospective randomized trial comparing magnetic resonance imaging (MRI)-guided in-bore biopsy to MRI-ultrasound fusion and transrectal ultrasound-guided prostate biopsy in patients with prior negative biopsies. Eur. Urol. 2015, 68, 713–720. [Google Scholar] [CrossRef]
- Quentin, M.; Blondin, D.; Arsov, C.; Schimmoller, L.; Hiester, A.; Godehardt, E.; Albers, P.; Antoch, G.; Rabenalt, R. Prospective evaluation of magnetic resonance imaging guided in-bore prostate biopsy versus systematic transrectal ultrasound guided prostate biopsy in biopsy naive men with elevated prostate specific antigen. J. Urol. 2014, 192, 1374–1379. [Google Scholar] [CrossRef]
- Samaratunga, H.; Delahunt, B.; Yaxley, J.; Srigley, J.R.; Egevad, L. From Gleason to International Society of Urological Pathology (ISUP) grading of prostate cancer. Scand. J. Urol. 2016, 50, 325–329. [Google Scholar] [CrossRef]
- Egevad, L.; Delahunt, B.; Srigley, J.R.; Samaratunga, H. International Society of Urological Pathology (ISUP) grading of prostate cancerAn ISUP consensus on contemporary grading. APMIS 2016, 124, 433–435. [Google Scholar] [CrossRef]
- Epstein, J.I.; Egevad, L.; Amin, M.B.; Delahunt, B.; Srigley, J.R.; Humphrey, P.A.; Grading, C. The 2014 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma: Definition of Grading Patterns and Proposal for a New Grading System. Am. J. Surg. Pathol. 2016, 40, 244–252. [Google Scholar] [CrossRef]
- Martorana, E.; Pirola, G.M.; Scialpi, M.; Micali, S.; Iseppi, A.; Bonetti, L.R.; Kaleci, S.; Torricelli, P.; Bianchi, G. Lesion volume predicts prostate cancer risk and aggressiveness: Validation of its value alone and matched with prostate imaging reporting and data system score. BJU Int. 2016, 120, 92–103. [Google Scholar] [CrossRef]
- Cash, H.; Maxeiner, A.; Stephan, C.; Fischer, T.; Durmus, T.; Holzmann, J.; Asbach, P.; Haas, M.; Hinz, S.; Neymeyer, J.; et al. The detection of significant prostate cancer is correlated with the Prostate Imaging Reporting and Data System (PI-RADS) in MRI/transrectal ultrasound fusion biopsy. World J. Urol. 2016, 34, 525–532. [Google Scholar] [CrossRef]
- Liddell, H.; Jyoti, R.; Haxhimolla, H.Z. mp-MRI Prostate Characterised PIRADS 3 Lesions are Associated with a Low Risk of Clinically Significant Prostate Cancer—A Retrospective Review of 92 Biopsied PIRADS 3 Lesions. Curr. Urol. 2015, 8, 96–100. [Google Scholar] [CrossRef] [PubMed]
- Valerio, M.; Donaldson, I.; Emberton, M.; Ehdaie, B.; Hadaschik, B.A.; Marks, L.S.; Mozer, P.; Rastinehad, A.R.; Ahmed, H.U. Detection of Clinically Significant Prostate Cancer Using Magnetic Resonance Imaging-Ultrasound Fusion Targeted Biopsy: A Systematic Review. Eur. Urol. 2015, 68, 8–19. [Google Scholar] [CrossRef]
- Le, J.D.; Tan, N.; Shkolyar, E.; Lu, D.Y.; Kwan, L.; Marks, L.S.; Huang, J.; Margolis, D.J.; Raman, S.S.; Reiter, R.E. Multifocality and prostate cancer detection by multiparametric magnetic resonance imaging: Correlation with whole-mount histopathology. Eur. Urol. 2015, 67, 569–576. [Google Scholar] [CrossRef]
- Boesen, L. Multiparametric MRI in detection and staging of prostate cancer. Dan. Med. J. 2017, 64, B5327. [Google Scholar] [PubMed]
- Schoots, I.G.; Roobol, M.J.; Nieboer, D.; Bangma, C.H.; Steyerberg, E.W.; Hunink, M.G. Magnetic resonance imaging-targeted biopsy may enhance the diagnostic accuracy of significant prostate cancer detection compared to standard transrectal ultrasound-guided biopsy: A systematic review and meta-analysis. Eur. Urol. 2015, 68, 438–450. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, M.M.; Rais-Bahrami, S.; Truong, H.; Stamatakis, L.; Vourganti, S.; Nix, J.; Hoang, A.N.; Walton-Diaz, A.; Shuch, B.; Weintraub, M.; et al. Magnetic resonance imaging/ultrasound-fusion biopsy significantly upgrades prostate cancer versus systematic 12-core transrectal ultrasound biopsy. Eur. Urol. 2013, 64, 713–719. [Google Scholar] [CrossRef] [PubMed]
- Miyagawa, T.; Ishikawa, S.; Kimura, T.; Suetomi, T.; Tsutsumi, M.; Irie, T.; Kondoh, M.; Mitake, T. Real-time Virtual Sonography for navigation during targeted prostate biopsy using magnetic resonance imaging data. Int. J. Urol. 2010, 17, 855–860. [Google Scholar] [CrossRef]
- Kuru, T.H.; Roethke, M.C.; Seidenader, J.; Simpfendorfer, T.; Boxler, S.; Alammar, K.; Rieker, P.; Popeneciu, V.I.; Roth, W.; Pahernik, S.; et al. Critical evaluation of magnetic resonance imaging targeted, transrectal ultrasound guided transperineal fusion biopsy for detection of prostate cancer. J. Urol. 2013, 190, 1380–1386. [Google Scholar] [CrossRef]
- Sonn, G.A.; Chang, E.; Natarajan, S.; Margolis, D.J.; Macairan, M.; Lieu, P.; Huang, J.; Dorey, F.J.; Reiter, R.E.; Marks, L.S. Value of targeted prostate biopsy using magnetic resonance-ultrasound fusion in men with prior negative biopsy and elevated prostate-specific antigen. Eur. Urol. 2014, 65, 809–815. [Google Scholar] [CrossRef]
- Chondros, K.; Karpathakis, N.; Heretis, I.; Mavromanolakis, E.; Chondros, N.; Sofras, F.; Mamoulakis, C. Validation of revised Epstein's criteria for insignificant prostate cancer prediction in a Greek subpopulation. Hippokratia 2015, 19, 30–33. [Google Scholar]
- Oon, S.F.; Watson, R.W.; O'Leary, J.J.; Fitzpatrick, J.M. Epstein criteria for insignificant prostate cancer. BJU Int. 2011, 108, 518–525. [Google Scholar] [CrossRef] [PubMed]
- Jeldres, C.; Suardi, N.; Walz, J.; Hutterer, G.C.; Ahyai, S.; Lattouf, J.B.; Haese, A.; Graefen, M.; Erbersdobler, A.; Heinzer, H.; et al. Validation of the contemporary epstein criteria for insignificant prostate cancer in European men. Eur. Urol. 2008, 54, 1306–1313. [Google Scholar] [CrossRef] [PubMed]
- Sonn, G.A.; Fan, R.E.; Ghanouni, P.; Wang, N.N.; Brooks, J.D.; Loening, A.M.; Daniel, B.L.; To'o, K.J.; Thong, A.E.; Leppert, J.T. Prostate Magnetic Resonance Imaging Interpretation Varies Substantially Across Radiologists. Eur. Urol. Focus 2017, 5, 592–599. [Google Scholar] [CrossRef] [PubMed]
- Radtke, J.P.; Wiesenfarth, M.; Kesch, C.; Freitag, M.T.; Alt, C.D.; Celik, K.; Distler, F.; Roth, W.; Wieczorek, K.; Stock, C.; et al. Combined Clinical Parameters and Multiparametric Magnetic Resonance Imaging for Advanced Risk Modeling of Prostate Cancer-Patient-tailored Risk Stratification Can Reduce Unnecessary Biopsies. Eur. Urol. 2017, 72, 888–896. [Google Scholar] [CrossRef]
- Roethke, M.C.; Kuru, T.H.; Mueller-Wolf, M.B.; Agterhuis, E.; Edler, C.; Hohenfellner, M.; Schlemmer, H.P.; Hadaschik, B.A. Evaluation of an Automated Analysis Tool for Prostate Cancer Prediction Using Multiparametric Magnetic Resonance Imaging. PLoS ONE 2016, 11, e0159803. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variable | Value | Range or % |
|---|---|---|
| Men included in analysis, n, % | 157 | 100 |
| Age, years, median n, (IQR) | 65 | (58–70) |
| PSA level, ng/mL, median n, (IQR) | 7.07 | (4.91–10.4) |
| Suspicious DRE findings (≥T2), n, % | 61 | 38.85 |
| Prostate volume, mL, median n, (IQR) | 43 | (31–64) |
| PSAD, ng/mL/mL, median n, (IQR) | 0.14 | (0.097–0.23) |
| Patients without prior biopsy, n, % | 118 | 75.16 |
| Patients with prior biopsy, n, % | 39 | 24.84 |
| Patients with 1 prior biopsy, n, % | 25 | 15.92 |
| Patients with 2 prior biopsies, n, % | 10 | 6.37 |
| Patients with 3 prior biopsies, n, % | 4 | 2.55 |
| Patients undergoing active surveillance, n, % | 9 | 5.73 |
| Days from mpMRI to biopsy, median n, (IQR) | 24 | (12–41) |
| mpMRI with no lesion, n, % | 11 | 7.01 |
| mpMRI with 1 lesion, n, % | 67 | 42.68 |
| mpMRI with 2 lesions, n, % | 55 | 35.03 |
| mpMRI with ≥3 lesions, n, % | 24 | 15.29 |
| Total number of lesions, n, % | 258 | 100 |
| PI-RADS v2 score 1, n, % | 1 | 0.39 |
| PI-RADS v2 score 2, n, % | 13 | 5.06 |
| PI-RADS v2 score 3, n, % | 50 | 19.4 |
| PI-RADS v2 score 4, n, % | 157 | 60.9 |
| PI-RADS v2 score 5, n, % | 37 | 14.3 |
| Total biopsies per patient, median n, (IQR) | 20 | (18–20) |
| Systematic biopsies per patient, median n, (IQR) | 11 | (8–13) |
| Biopsies per lesion, median n, (IQR) | 4 | (3–5) |
| mpMRI | ISUP | ||||||
|---|---|---|---|---|---|---|---|
| PI-RADS | n | 0 * | 1 | 2 | 3 | 4 | 5 |
| no lesion | 11 | 9 (81.8%) | 2 (18.2%) | - | - | - | - |
| 1 | 1 | 1 (100%) | - | - | - | - | - |
| 2 | 13 | 10 (76.9%) | 3 (23.1%) | - | - | - | - |
| 3 | 50 | 38 (76.0%) | 10 (20.0%) | 2 (4.0%) | - | - | - |
| 4 | 157 | 99 (63.1%) | 33 (21.0%) | 19 (12.1%) | 4 (2.5%) | 1 (0.6%) | 1 (0.6%) |
| 5 | 37 | 15 (40.5%) | 6 (16.2%) | 7 (18.9%) | 4 (10.8%) | 3 (8.1%) | 2 (5.4%) |
| total | |||||||
| Cancer-Predicting Variables | Sensitivity, % | Specificity, % | PPV, % | NPV, % |
|---|---|---|---|---|
| mpMRI | 95.5 | 15.5 | 45.7 | 82.4 |
| DRE | 49.3 | 70.0 | 65.0 | 55.0 |
| PSAD | 64.2 | 66.6 | 58.9 | 71.4 |
| DRE + PSAD | 32.8 | 92.2 | 75.9 | 64.8 |
| mpMRI + DRE | 49.3 | 72.2 | 56.9 | 65.7 |
| mpMRI + PSAD | 61.2 | 73.3 | 63.1 | 71.7 |
| mpMRI + DRE + PSAD | 34.3 | 50.0 | 77.4 | 13.2 |
| PI-RADS | Lesion | ISUP Grades | csPCa | Total | PCa | csPCa | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Score | n | Volume, mL | 0 * | 1 | 2 | 3 | 4 | 5 | n | n | Risk, % | Risk, % |
| ≤0.5 | 26 | 7 | 2 | 0 | 0 | 0 | 2 | 35 | 25.7 | 5.7 | ||
| 3 | 50 | 0.5–1 | 7 | 2 | 0 | 0 | 0 | 0 | 0 | 9 | 22.2 | 0.0 |
| ≥1 | 5 | 1 | 0 | 0 | 0 | 0 | 0 | 6 | 16.7 | 0.0 | ||
| ≤0.5 | 69 | 22 | 13 | 1 | 0 | 1 | 15 | 106 | 34.9 | 14.2 | ||
| 4 | 157 | 0.5–1 | 18 | 10 | 4 | 2 | 0 | 0 | 6 | 34 | 47.1 | 17.6 |
| ≥1 | 12 | 1 | 2 | 1 | 1 | 0 | 4 | 17 | 29.4 | 23.5 | ||
| ≤0.5 | 5 | 3 | 4 | 0 | 1 | 0 | 5 | 13 | 61.5 | 38.5 | ||
| 5 | 37 | 0.5–1 | 3 | 3 | 0 | 0 | 0 | 0 | 0 | 6 | 50.0 | 0.0 |
| ≥1 | 7 | 0 | 3 | 4 | 2 | 2 | 11 | 18 | 61.1 | 61.1 | ||
| ≤0.5 | 100 | 32 | 19 | 1 | 1 | 1 | 22 | 154 | 35.1 | 14.3 | ||
| total | 244 | 0.5–1 | 28 | 15 | 4 | 2 | 0 | 0 | 6 | 49 | 42.9 | 12.2 |
| ≥1 | 24 | 2 | 5 | 5 | 3 | 2 | 15 | 41 | 41.5 | 36.6 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sauck, A.; Keller, I.; Hainc, N.; Pfofe, D.; Najafi, A.; John, H.; Hohmann, J. Prostate Cancer Detection with mpMRI According to PI-RADS v2 Compared with Systematic MRI/TRUS-Fusion Biopsy: A Prospective Study. Tomography 2022, 8, 2020-2029. https://doi.org/10.3390/tomography8040169
Sauck A, Keller I, Hainc N, Pfofe D, Najafi A, John H, Hohmann J. Prostate Cancer Detection with mpMRI According to PI-RADS v2 Compared with Systematic MRI/TRUS-Fusion Biopsy: A Prospective Study. Tomography. 2022; 8(4):2020-2029. https://doi.org/10.3390/tomography8040169
Chicago/Turabian StyleSauck, Anja, Isabelle Keller, Nicolin Hainc, Denis Pfofe, Arash Najafi, Hubert John, and Joachim Hohmann. 2022. "Prostate Cancer Detection with mpMRI According to PI-RADS v2 Compared with Systematic MRI/TRUS-Fusion Biopsy: A Prospective Study" Tomography 8, no. 4: 2020-2029. https://doi.org/10.3390/tomography8040169
APA StyleSauck, A., Keller, I., Hainc, N., Pfofe, D., Najafi, A., John, H., & Hohmann, J. (2022). Prostate Cancer Detection with mpMRI According to PI-RADS v2 Compared with Systematic MRI/TRUS-Fusion Biopsy: A Prospective Study. Tomography, 8(4), 2020-2029. https://doi.org/10.3390/tomography8040169