
Radiation Eye Dose for Physicians in CT Fluoroscopy-Guided Biopsy


Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
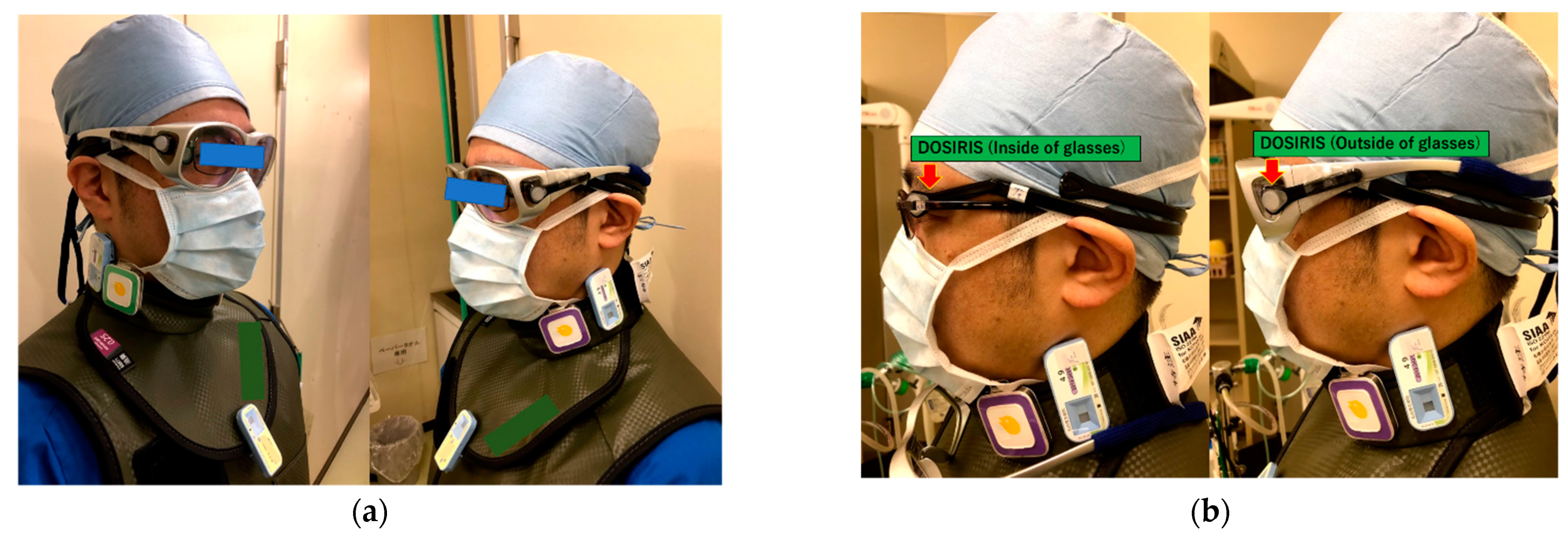
2.2. Dosimetry
2.3. Statical Analysis
3. Results
3.1. Physician Dose
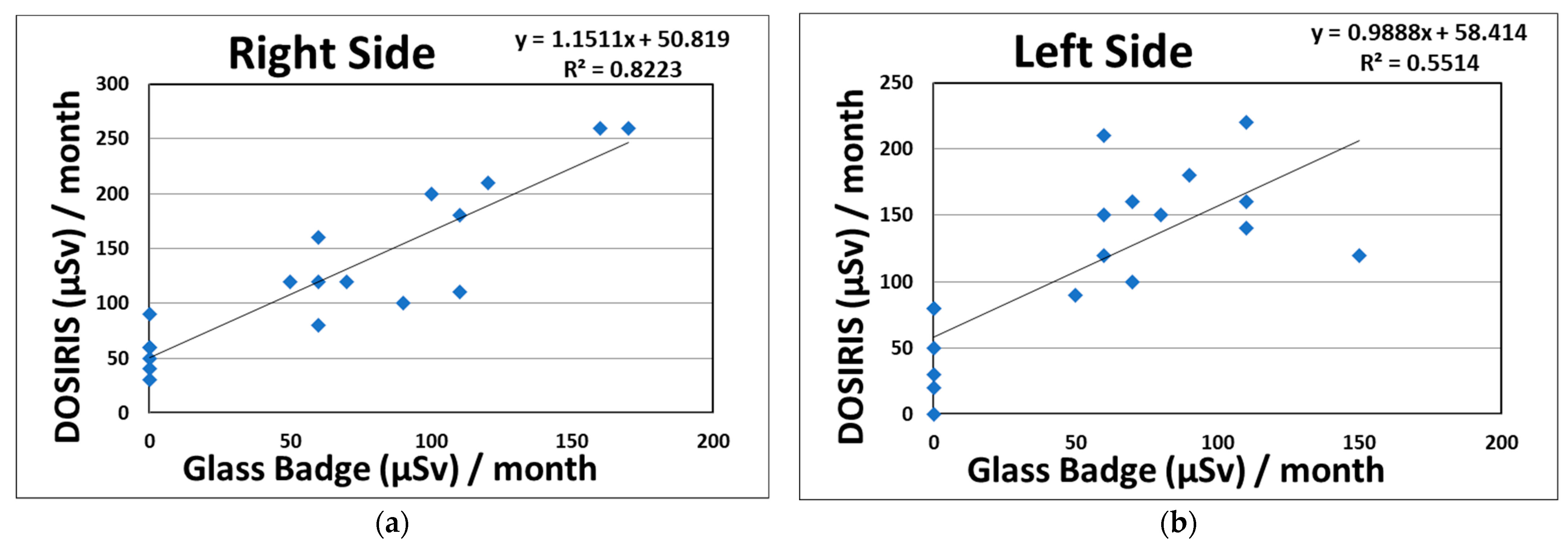
3.2. Relationship between the Eye Dosimeter and Neck Dosimeter or CT-Related Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- International Commission on Radiolocial Protoection. ICRP Statement on Tissue Reactions/Early and Late Effects of Radiation in Normal Tissues and Organs—Threshold Doses for Tissue Reactions in a Radiation Protection Context; ICRP Publication 118; ICRP: Ottawa, ON, Canada, 2012; Volume 41, pp. 1–322. [Google Scholar]
- International Atomic Energy Agency. Radiation Protection and Safety of Radiation Sources: International Basic Safety Standards. General Safety Requirements Part 3; IAEA: Vienna, Austria, 2014. [Google Scholar]
- Kawauchi, S.; Chida, K.; Hamada, Y.; Tsuruta, W. Lens dose reduction with a bismuth shield in neuro cone-beam computed tomography: An investigation on optimum shield device placement conditions. Radiol. Phys. Technol. 2021, 1–12. [Google Scholar] [CrossRef]
- Kawauchi, S.; Chida, K.; Moritake, T.; Hamada, Y.; Tsuruta, W. Radioprotection of eye lens using protective material in neuro cone-beam computed tomography: Estimation of dose reduction rate and image quality. Phys. Med. 2021, 82, 192–199. [Google Scholar] [CrossRef]
- Ishii, H.; Chida, K.; Satsurai, K.; Haga, Y.; Kaga, Y.; Abe, M.; Inaba, Y.; Zuguchi, M. Occupational eye dose correlation with neck dose and patient-related quantities in interventional cardiology procedures. Radiol. Phys. Technol. 2022, 1–9. [Google Scholar] [CrossRef]
- Silverman, S.G.; Tuncali, K.; Adams, D.F.; Nawfel, R.D.; Zou, K.H.; Judy, P.F. CT fluoroscopy-guided abdominal interventions: Techniques, results, and radiation exposure. Radiology 1999, 212, 673–681. [Google Scholar] [CrossRef]
- Paulson, E.K.; Sheafor, D.H.; Enterline, D.S.; McAdams, H.P.; Yoshizumi, T.T. CT fluoroscopy-guided interventional procedures: Techniques and radiation dose to radiologists. Radiology 2001, 220, 161–167. [Google Scholar] [CrossRef]
- Kim, G.R.; Hur, J.; Lee, S.M.; Lee, H.J.; Hong, Y.J.; Nam, J.E.; Kim, H.S.; Kim, Y.J.; Choi, B.W.; Kim, T.H.; et al. CT fluoroscopy-guided lung biopsy versus conventional CT-guided lung biopsy: A prospective controlled study to assess radiation doses and diagnostic performance. Eur. Radiol. 2011, 21, 232–239. [Google Scholar] [CrossRef]
- Sarti, M.; Brehmer, W.P.; Gay, S.B. Low-dose techniques in CT-guided interventions. Radiographics 2012, 32, 1109–1119. [Google Scholar] [CrossRef]
- Prosch, H.; Stadler, A.; Schilling, M.; Bürklin, S.; Eisenhuber, E.; Schober, E.; Mostbeck, G. CT fluoroscopy-guided vs. multislice CT biopsy mode-guided lung biopsies: Accuracy, complications and radiation dose. Eur. J. Radiol. 2012, 81, 1029–1033. [Google Scholar] [CrossRef]
- Nawfel, R.D.; Judy, P.F.; Silverman, S.G.; Hooton, S.; Tuncali, K.; Adams, D.F. Patient and personnel exposure during CT fluoroscopy-guided interventional procedures. Radiology 2000, 216, 180–184. [Google Scholar] [CrossRef]
- Irie, T.; Kajitani, M.; Itai, Y. CT fluoroscopy-guided intervention: Marked reduction of scattered radiation dose to the physician’s hand by use of a lead plate and an improved I-I device. J. Vasc. Interv. Radiol. 2001, 12, 1417–1421. [Google Scholar] [CrossRef]
- Buls, N.; Pagés, J.; de Mey, J.; Osteaux, M. Evaluation of patient and staff doses during various CT fluoroscopy guided interventions. Health Phys. 2003, 85, 165–173. [Google Scholar] [CrossRef]
- Aviles Lucas, P.; Dance, D.R.; Castellano, I.A.; Vano, E. Estimation of the peak entrance surface air kerma for patients undergoing computed tomography-guided procedures. Radiat. Prot. Dosim. 2005, 114, 317–320. [Google Scholar] [CrossRef]
- Neeman, Z.; Dromi, S.A.; Sarin, S.; Wood, B.J. CT fluoroscopy shielding decreases in scattered radiation for the patient and operator. J. Vasc. Interv. Radiol. 2006, 17, 1999–2004. [Google Scholar] [CrossRef] [Green Version]
- Hohl, C.; Suess, C.; Wildberger, J.E.; Honnef, D.; Das, M.; Mühlenbruch, G.; Schaller, A.; Günther, R.W.; Mahnken, A.H. Dose reduction during CT fluoroscopy: Phantom study of angular beam modulation. Radiology 2008, 246, 519–525. [Google Scholar] [CrossRef]
- Joemai, R.M.; Zweers, D.; Obermann, W.R.; Geleijns, J. Assessment of patient and occupational dose in established and new applications of MDCT fluoroscopy. Am. J. Roentgenol. 2009, 192, 881–886. [Google Scholar] [CrossRef]
- Yamao, Y.; Yamakado, K.; Takaki, H.; Yamada, T.; Kodama, H.; Nagasawa, N.; Nakatsuka, A.; Uraki, J.; Takeda, K. CT-fluoroscopy in chest interventional radiology: Sliding scale of imaging parameters based on radiation exposure dose and factors increasing radiation exposure dose. Clin. Radiol. 2013, 68, 162–166. [Google Scholar] [CrossRef]
- Chida, K.; Kato, M.; Kagaya, Y.; Zuguchi, M.; Saito, H.; Ishibashi, T.; Takahashi, S.; Yamada, S.; Takai, Y. Radiation dose and radiation protection for patients and physicians during interventional procedure. J. Radiat. Res. 2010, 51, 97–105. [Google Scholar] [CrossRef] [Green Version]
- Chida, K.; Morishima, Y.; Inaba, Y.; Taura, M.; Ebata, A.; Takeda, K.; Shimura, H.; Zuguchi, M. Physician-received scatter radiation with angiography systems used for interventional radiology: Comparison among many X-ray systems. Radiat. Prot. Dosim. 2012, 149, 410–416. [Google Scholar] [CrossRef]
- Chida, K.; Kaga, Y.; Haga, Y.; Kataoka, N.; Kumasaka, E.; Meguro, T.; Zuguchi, M. Occupational Dose in Interventional Radiology Procedures. Am. J. Roentgenol. 2013, 200, 138–141. [Google Scholar] [CrossRef]
- Inaba, Y.; Chida, K.; Kobayashi, R.; Kaga, Y.; Zuguchi, M. Fundamental study of a real-time occupational dosimetry system for interventional radiology staff. J. Radiol. Prot. 2014, 34, N65. [Google Scholar] [CrossRef]
- Morishima, Y.; Chida, K.; Watanabe, H. Estimation of the Dose of Radiation Received by Patient and Physician during a Videofluoroscopic Swallowing Study. Dysphagia 2016, 31, 574–578. [Google Scholar] [CrossRef] [PubMed]
- Haga, Y.; Chida, K.; Kaga, Y.; Sota, M.; Meguro, T.; Zuguchi, M. Occupational Eye Dose in Interventional Cardiology Procedures. Sci. Rep. 2017, 7, 569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsubara, K.; Lertsuwunseri, V.; Srimahachota, S.; Krisanachinda, A.; Tulvatana, W.; Khambhiphant, B.; Sudchai, W.; Rehani, M. Eye lens dosimetry and the study on radiation cataract in interventional cardiologists. Phys. Med. 2017, 44, 232–235. [Google Scholar] [CrossRef] [PubMed]
- Vano, E.; Sanchez, R.M.; Fernandez, J.M. Strategies to optimize occupational radiation protection in interventional cardiology using simultaneous registration of patient and staff doses. J. Radiol. Prot. 2018, 38, 1077–1088. [Google Scholar] [CrossRef]
- Kato, M.; Chida, K.; Ishida, T.; Sasaki, F.; Toyoshima, H.; Oosaka, H.; Terata, K.; Abe, Y.; Kinoshita, T. Occupational radiation exposure dose of the eye in department of cardiac arrhythmia physician. Radiat. Prot. Dosim. 2019, 187, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Coppeta, L.; Pietroiusti, A.; Neri, A.; Spataro, A.; Angelis, E.D.; Perrone, S.; Magrini, A. Risk of radiation-induced lens opacities among surgeons and interventional medical staff. Radiol. Phys. Technol. 2019, 12, 26–29. [Google Scholar] [CrossRef]
- Ishii, H.; Chida, K.; Satsurai, K.; Haga, Y.; Kaga, Y.; Abe, M.; Inaba, Y.; Zuguchi, M. A Phantom Study to Determine the Optimal Placement of Eye Dosemeters on Interventional Cardiology Staff. Radiat. Prot. Dosim. 2019, 185, 409–413. [Google Scholar] [CrossRef]
- Mortensen, C.; Chung, J.; Liu, D.; Ho, S.; Legiehn, G.; Machan, L.; Klass, D. Prospective study on total fluoroscopic time in patients undergoing uterine artery embolization: Comparing transradial and transfemoral approaches. Cardiovasc. Interv. Radiol. 2019, 42, 441–447. [Google Scholar] [CrossRef] [PubMed]
- Kato, M.; Chida, K.; Ishida, T.; Toyoshima, H.; Yoshida, Y.; Yoshioka, S.; Moroi, J.; Kinoshita, T. Occupational radiation exposure of the eye in neurovascular interventional physician. Radiat. Prot. Dosim. 2019, 185, 151–156. [Google Scholar] [CrossRef]
- Koenig, A.M.; Etzel, R.; Greger, W.; Viniol, S.; Fiebich, M.; Thomas, R.P.; Mahnken, A.H. Protective efficacy of different ocular radiation protection devices: A phantom study. Cardiovasc. Interv. Radiol. 2020, 43, 127–134. [Google Scholar] [CrossRef]
- Haga, Y.; Chida, K.; Sota, M.; Kaga, Y.; Abe, M.; Inaba, Y.; Suzuki, M.; Meguro, T.; Zuguchi, M. Hybrid Operating Room System for the Treatment of Thoracic and Abdominal Aortic Aneurysms: Evaluation of the Radiation Dose Received by Patients. Diagnostics 2020, 10, 846. [Google Scholar] [CrossRef] [PubMed]
- Mihić, M.S.; Pavelić, L.; Kortmiš, M.V.; Šiško, J.; Maltar-Strmečki, N.M.; Prlić, I. 3D-printed eye lens dosemeter holder for use in interventional radiology and interventional cardiology. Radiat. Meas. 2020, 135, 106385. [Google Scholar] [CrossRef]
- Matsubara, K.; Takei, Y.; Mori, H.; Kobayashi, I.; Noto, K.; Igarashi, T.; Suzuki, S.; Akahane, K. A multicenter study of radiation doses to the eye lenses of medical staff performing non-vascular imaging and interventional radiology procedures in Japan. Phys. Med. 2020, 74, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Inaba, Y.; Nakamura, M.; Zuguchi, M.; Chida, K. Development of Novel Real-Time Radiation Systems Using 4-Channel Sensors. Sensors 2020, 20, 2741. [Google Scholar] [CrossRef]
- Dehairs, M.; Marshall, N.M.; Bosmans, H.; Leghissa, M. Radiation protection operators and patients in a hybrid angio-MR suite. Phys. Med. 2020, 74, 143–154. [Google Scholar] [CrossRef] [PubMed]
- Inaba, Y.; Chida, K.; Murabayashi, Y.; Endo, M.; Otomo, K.; Zuguchi, M. An initial investigation of a wireless patient radiation dosimeter for use in interventional radiology. Radiol. Phys. Technol. 2020, 13, 321–326. [Google Scholar] [CrossRef]
- Haga, Y.; Chida, K.; Kimura, Y.; Yamanda, S.; Sota, M.; Kaga, Y.; Abe, M.; Meguro, T.; Zuguchi, M. Radiation eye dose to medical staff during respiratory endoscopy under X-ray fluoroscopy. J. Radiat. Res. 2020, 61, 691–696. [Google Scholar] [CrossRef]
- Matsubara, K.; Yoshida, S.; Hirosawa, A.; Chusin, T.; Furukawa, Y. Characterization of Small Dosimeters Used for Measurement of Eye Lens Dose for Medical Staff during Fluoroscopic Examination. Diagnostics 2021, 11, 150. [Google Scholar] [CrossRef]
- Osanai, M.; Sato, H.; Sato, K.; Kudo, K.; Hosoda, M.; Hosokawa, S.; Kitajima, M.; Tsushima, M.; Fujita, A.; Hosokawa, Y.; et al. Occupational Radiation Dose, Especially for Eye Lens: Hp(3), in Medical Staff Members Involved in Computed Tomography Examinations. Appl. Sci. 2021, 11, 4448. [Google Scholar] [CrossRef]
- Nemoto, M.; Chida, K. Reducing the Breast Cancer Risk and Radiation Dose of Radiography for Scoliosis in Children: A Phantom Study. Diagnostics 2020, 10, 753. [Google Scholar] [CrossRef]
- Matsunaga, Y.; Chida, K.; Kondo, Y.; Kobayashi, K.; Kobayashi, M.; Minami, K.; Suzuki, S.; Asada, Y. Diagnostic reference levels and achievable doses for common computed tomography examinations: Results from the Japanese nationwide dose survey. Br. J. Radiol. 2019, 92, 20180290. [Google Scholar] [CrossRef] [PubMed]
- Inaba, Y.; Nakamura, M.; Chida, K.; Zuguchi, M. Effectiveness of a novel real-time dosimeter in interventional radiology: A comparison of new and old radiation sensors. Radiol. Phys. Technol. 2018, 11, 445–450. [Google Scholar] [CrossRef] [PubMed]
- Chida, K.; Kato, M.; Inaba, Y.; Kobayashi, R.; Nakamura, M.; Abe, Y.; Zuguchi, M. Real-time patient radiation dosimeter for use in interventional radiology. Phys. Med. 2016, 32, 1475–1478. [Google Scholar] [CrossRef]
- Inaba, Y.; Chida, K.; Kobayashi, R.; Zuguchi, M. A Cross-Sectional Study of the Radiation Dose and Image Quality of X-ray Equipment Used in IVR. J. Appl. Clin. Med. Phys. 2016, 17, 391–401. [Google Scholar] [CrossRef] [PubMed]
- Inaba, Y.; Chida, K.; Kobayashi, R.; Haga, Y.; Zuguchi, M. Radiation Dose of Cardiac IVR X-ray Systems: A Comparison of Present and Past. Acta Cardiol. 2015, 70, 299–306. [Google Scholar] [CrossRef] [PubMed]
- Chida, K.; Inaba, Y.; Morishima, Y.; Taura, M.; Ebata, A.; Yanagawa, I.; Takeda, K.; Zuguchi, M. Comparison of Dose at an Interventional Reference Point Between the Displayed Estimated Value and Measured Value. Radiol. Phys. Technol. 2011, 4, 189–193. [Google Scholar] [CrossRef]
- Chida, K.; Inaba, Y.; Saito, H.; Ishibashi, T.; Takahashi, S.; Kohzuki, M.; Zuguchi, M. Radiation dose of interventional radiology system using a flat-panel detector. Am. J. Roentgenol. 2009, 193, 1680–1685. [Google Scholar] [CrossRef]
- Chida, K.; Inaba, Y.; Masuyama, H.; Yanagawa, I.; Mori, I.; Saito, H.; Maruoka, S.; Zuguchi, M. Evaluating the performance of a MOSFET dosimeter at diagnostic X-ray energies for interventional radiology. Radiol. Phys. Technol. 2009, 2, 58–61. [Google Scholar] [CrossRef]
- Chida, K.; Saito, H.; Otani, H.; Kohzuki, M.; Takahashi, S.; Yamada, S.; Shirato, K.; Zuguchi, M. Relationship between fluoroscopic time, dose-area product, body weight, and maximum radiation skin dose in cardiac interventional procedures. Am. J. Roentgenol. 2006, 186, 774–778. [Google Scholar] [CrossRef]
- Kato, M.; Chida, K.; Munehisa, M.; Sato, T.; Inaba, Y.; Suzuki, M.; Zuguchi, M. Non-Lead Protective Aprons for the Protection of Interventional Radiology Physicians from Radiation Exposure in Clinical Settings: An Initial Study. Diagnostics 2021, 11, 1613. [Google Scholar] [CrossRef]
- Chida, K.; Takahashi, T.; Ito, D.; Shimura, H.; Takeda, K.; Zuguchi, M. Clarifying and visualizing sources of staff-received scattered radiation in interventional procedures. Am. J. Roentgenol. 2011, 197, W900–W903. [Google Scholar] [CrossRef] [PubMed]
- Zuguchi, M.; Chida, K.; Taura, M.; Inaba, Y.; Ebata, A.; Yamada, S. Usefulness of non-lead aprons in radiation protection for physicians performing interventional procedures. Radiat. Prot. Dosim. 2008, 131, 531–534. [Google Scholar] [CrossRef]
- International Atomic Energy Agency. Implications for Occupational Radiation Protection of the New Dose Limit for the Lens of the Eye; TECDOC 1731; IAEA: Vienna, Austria, 2013; pp. 1–34. [Google Scholar]
- International Commission on Radiolocial Protection. The 2007 Recommendations of the International Commission on Radiological Protection; ICRP Publication 103; ICRP: Ottawa, ON, Canada, 2007; Volume 37, pp. 1–332. [Google Scholar]
- Martin, C.J. A 20 mSv dose limit for the eye: Sense or no sense? J. Radiol. Prot. 2021, 31, 385. [Google Scholar] [CrossRef] [PubMed]
- Inaba, Y.; Hitachi, S.; Watanuki, M.; Chida, K. Occupational Radiation Dose to Eye Lenses in CT-Guided Interventions Using MDCT-Fluoroscopy. Diagnostics 2021, 11, 646. [Google Scholar] [CrossRef] [PubMed]
- Ishii, H.; Haga, Y.; Sota, M.; Inaba, Y.; Chida, K.M. Performance of the DOSIRISTM eye lens dosimeter. J. Radiol. Prot. 2019, 39, N19. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Characteristics | Ave. ± SD | Median | Range |
|---|---|---|---|
| Age (years) | 51.8 ± 20.8 | 55.5 | 5.0–88.0 |
| Body Mass Index | 23.2 ± 3.9 | 22.7 | 15.8–34.3 |
| CT-fluoroscopic acquisition number | 26.2 ± 15.5 | 22.0 | 8.0–96.0 |
| CT-fluoroscopic time (s) | 20.0 ± 11.8 | 17.1 | 5.9–72.1 |
| CT-fluoroscopic mAs | 464.1 ± 327.4 | 376.0 | 118.0–2105.0 |
| CTDI vol (mGy) | 10.2 ± 5.3 | 7.7 | 3.3–29.6 |
| DLP (mGy*cm) | 215.1 ± 88.5 | 186.7 | 76.2–539.9 |
| Target depth (mm) | 60.5 ± 21.6 | 56.5 | 14.3–119.5 |
| (μSv) | Right Side | Left Side |
|---|---|---|
| Eye dose (DOSIRIS), Hp (3) | 2250 | 2060 |
| Neck dose (Glass Badge), Hp (3) | 1160 | 1020 |
| (μSv) | Outside of Eyeglasses | Inside of Eyeglasses | Protective Effect (%) |
|---|---|---|---|
| Right eye dose (DOSIRIS), Hp (3) | 720 | 520 | 27.8 |
| Left eye dose (DOSIRIS), Hp (3) | 800 | 500 | 37.5 |
| Determination Coefficient (R2) | CT-Acquisitions No. | CT-Fluoroscopic Time (s) | CT-Fluoroscopic mAs |
|---|---|---|---|
| Right eye dose (DOSIRIS), Hp (3) | 0.463 | 0.441 | 0.497 |
| Left eye dose (DOSIRIS), Hp (3) | 0.507 | 0.486 | 0.524 |
| Right neck dose (Glass Badge), Hp (3) | 0.788 | 0.799 | 0.745 |
| Left neck dose (Glass Badge), Hp (3) | 0.666 | 0.675 | 0.592 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Inaba, Y.; Hitachi, S.; Watanuki, M.; Chida, K. Radiation Eye Dose for Physicians in CT Fluoroscopy-Guided Biopsy. Tomography 2022, 8, 438-446. https://doi.org/10.3390/tomography8010036
Inaba Y, Hitachi S, Watanuki M, Chida K. Radiation Eye Dose for Physicians in CT Fluoroscopy-Guided Biopsy. Tomography. 2022; 8(1):438-446. https://doi.org/10.3390/tomography8010036
Chicago/Turabian StyleInaba, Yohei, Shin Hitachi, Munenori Watanuki, and Koichi Chida. 2022. "Radiation Eye Dose for Physicians in CT Fluoroscopy-Guided Biopsy" Tomography 8, no. 1: 438-446. https://doi.org/10.3390/tomography8010036
APA StyleInaba, Y., Hitachi, S., Watanuki, M., & Chida, K. (2022). Radiation Eye Dose for Physicians in CT Fluoroscopy-Guided Biopsy. Tomography, 8(1), 438-446. https://doi.org/10.3390/tomography8010036