
Osteoid Osteoma in an Adult Wheelchair Basketball Player Mimicking Musculoskeletal Shoulder Pain: Red Flag or a Red Herring?

 ,
,  ,
,  , ,
, ,  and
and
Abstract
1. Introduction
2. Case Presentation
Investigations
3. Results
3.1. Differential Diagnosis
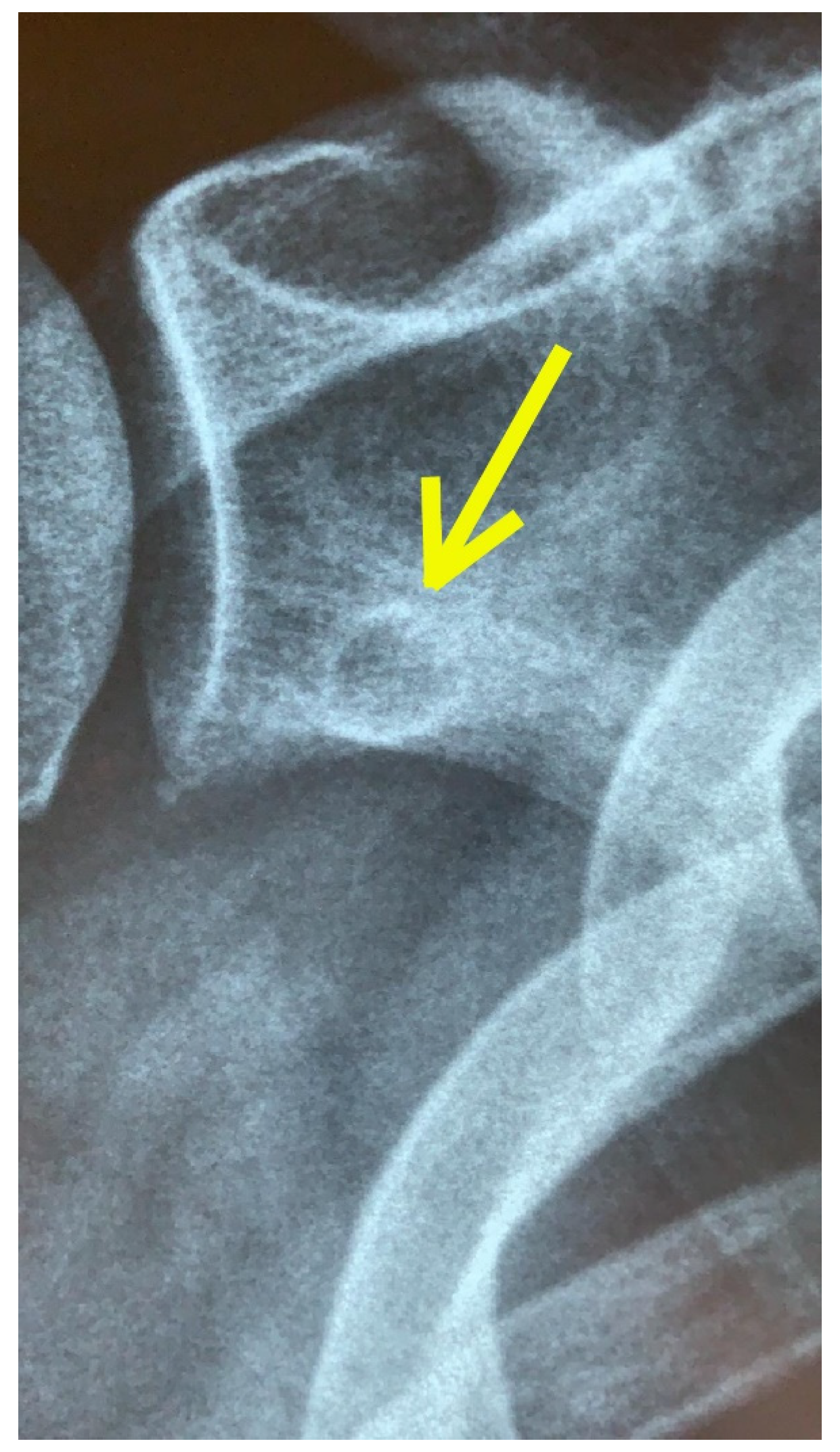
3.2. Imaging
3.3. Treatment
3.4. Outcome and Follow-Up
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Luime, J.J.; Koes, B.W.; Hendriksen, I.J.M.; Burdorf, A.; Verhagen, A.P.; Miedema, H.S.; Verhaar, J.A.N. Prevalence and incidence of shoulder pain in the general population; a systematic review. Scand. J. Rheumatol. 2004, 33, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Greving, K.; Dorrestijn, O.; Winters, J.C.; Groenhof, F.; Van Der Meer, K.; Stevens, M.; Diercks, R. Incidence, prevalence, and consultation rates of shoulder complaints in general practice. Scand. J. Rheumatol. 2011, 41, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, R.L.; Braman, J.P.; Laprade, R.F.; Ludewig, P.M. Comparison of 3-dimensional shoulder complex kinematics in individuals with and without shoulder pain, part 1: Sternoclavicular, acromioclavicular, and scapulothoracic joints. J. Orthop. Sports Phys. Ther. 2014, 44, 636–645. [Google Scholar] [CrossRef] [PubMed]
- Ostör, A.J.; Richards, C.A.; Prevost, A.T.; Speed, C.A.; Hazleman, B.L. Diagnosis and relation to general health of shoulder disorders presenting to primary care. Rheumatology 2005, 44, 800–805. [Google Scholar] [CrossRef] [PubMed]
- Fullerton, H.D.; Borckardt, J.J.; Alfano, A.P. Shoulder pain: A comparison of wheelchair athletes and nonathletic wheelchair users. Med. Sci. Sports Exerc. 2003, 35, 1958–1961. [Google Scholar] [CrossRef]
- Nyland, J.; Robinson, K.; Caborn, D.; Knapp, E.; Brosky, T. Shoulder rotator torque and wheelchair dependence differences of National Wheelchair Basketball Association players. Arch. Phys. Med. Rehabil. 1997, 78, 358–363. [Google Scholar] [CrossRef]
- Fairbairn, J.R.; Huxel Bliven, K.C. Incidence of Shoulder Injury in Elite Wheelchair Athletes Differ between Sports: A Critically Appraised Topic. J. Sport Rehabil. 2019, 28, 294–298. [Google Scholar] [CrossRef]
- Tuakli-Wosornu, Y.A.; Mashkovskiy, E.; Ottesen, T.; Gentry, M.; Jensen, D.; Webborn, N. Acute and Chronic Musculoskeletal Injury in Para Sport: A Critical Review. Phys. Med. Rehabil. Clin. N. Am. 2018, 29, 205–243. [Google Scholar] [CrossRef]
- Crespo-Ruiz, B.M.; Del Ama-Espinosa, A.J.; Gil-Agudo, A.M. Relation between kinematic analysis of wheelchair propulsion and wheelchair functional basketball classification. Adapt. Phys. Activ Q. 2011, 28, 157–172. [Google Scholar] [CrossRef]
- Curtis, K.A.; Black, K. Shoulder pain in female wheelchair basketball players. J. Orthop Sports Phys. Ther. 1999, 29, 225–231. [Google Scholar] [CrossRef]
- De Witte, A.M.H.; Berger, M.A.M.; Hoozemans, M.J.M.; Veeger, H.E.J.; Van der Woude, L.H.V. Effects of Offense, Defense, and Ball Possession on Mobility Performance in Wheelchair Basketball. Adapt. Phys. Act. Q. 2017, 34, 382–400. [Google Scholar] [CrossRef]
- Vanlandewijck, Y.; Theisen, D.; Daly, D. Wheelchair propulsion biomechanics: Implications for wheelchair sports. Sports Med. 2001, 31, 339–367. [Google Scholar] [CrossRef]
- Curtis, K.A.; Dillon, D.A. Survey of wheelchair athletic injuries: Common patterns and prevention. Paraplegia 1985, 23, 170–175. [Google Scholar] [CrossRef] [PubMed]
- Goodman, C.C. Screening for medical problems in patients with upper extremity signs and symptoms. J. Hand Ther. 2010, 23, 105–125. [Google Scholar] [CrossRef] [PubMed]
- Goodman, C.C.; Heick, J.; Lazaro, T.R. Differential Diagnosis for Physical Therapist: Screening for Referral, 6th ed.; Saunders: Philadelphia, PA, USA, 2018. [Google Scholar]
- Ren, X.; Yang, L.; Duan, X.J. Three-dimensional printing in the surgical treatment of osteoid osteoma of the calcaneus: A case report. J. Int. Med. Res. 2017, 45, 372–380. [Google Scholar] [CrossRef] [PubMed]
- Jordan, R.W.; Koç, T.; Chapman, A.W.; Taylor, H.P. Osteoid osteoma of the foot and ankle--A systematic review. Foot Ankle Surg. 2015, 21, 228–234. [Google Scholar] [CrossRef]
- Kitsoulis, P.; Mantellos, G.; Vlychou, M. Osteoid osteoma. Acta Orthop. Belg. 2006, 72, 119–125. [Google Scholar]
- Dookie, A.L.; Joseph, R.M. Osteoid Osteoma; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Jaffe, H.L. Osteoid-osteoma: A benign osteoblastic tumor composed of osteoid and atypical bone. Arch. Surg. 1935, 31, 709–728. [Google Scholar] [CrossRef]
- Noordin, S.; Allana, S.; Hilal, K.; Nadeem, N.; Lakdawala, R.; Sadruddin, A.; Uddin, N. Osteoid osteoma: Contemporary management. Orthop Rev. 2018, 10, 7496. [Google Scholar] [CrossRef]
- Kumar, R.; Chandrashekhar, N.; Dasan, J.B.; Ashok, S.; Rastogi, S.; Gupta, V.; Hadi, M.; Choudhury, S. Recurrent osteoid osteoma: A case report with imaging features. Clin. Imaging 2003, 27, 269–272. [Google Scholar] [CrossRef]
- Gökalp, M.A.; Gözen, A.; Ünsal, S.Ş.; Önder, H.; Güner, S. Alternative Surgical Method for Treatment of Osteoid Osteoma. Med. Sci. Monit. 2016, 22, 580–586. [Google Scholar] [CrossRef] [PubMed]
- Mitsui, Y.; Gotoh, M.; Yoshida, T.; Hirai, Y.; Shinozaki, T.; Nakama, K.; Higuchi, F.; Nagata, K. Osteoid osteoma of the proximal humerus: A misleading case. J. Shoulder Elbow Surg. 2007, 17, e13–e15. [Google Scholar] [CrossRef]
- Kransdorf, M.J.; Stull, M.A.; Gilkey, F.W.; Moser, R.P., Jr. Osteoid osteoma. Radiographics 1991, 11, 671–696. [Google Scholar] [CrossRef] [PubMed]
- Miyazaki, A.N.; Fregoneze, M.; Santos, P.D.; da Silva, L.A.; do Val Sella, G.; Neto, D.L.; Muchiuti Junior, M.; Checchia, S.L. Osteoid osteoma of the acromion simulating acromioclavicular pain. Rev. Bras. Ortop. 2014, 49, 82–85. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Ogose, A.; Sim, F.H.; O’Connor, M.I.; Unni, K.K. Bone tumors of the coracoid process of the scapula. Clin. Orthop. Relat. Res. 1999, 358, 205–214. [Google Scholar] [CrossRef]
- Zoboski, R.J. Occult osteoid osteoma presenting as shoulder pain: A case report. J. Chiropr. Med. 2012, 11, 207–214. [Google Scholar] [CrossRef][Green Version]
- Efstathopoulos, N.; Sapkas, G.; Xypnitos, F.N.; Lazarettos, I.; Korres, D.; Nikolaou, V.S. Recurrent intra-articular osteoid osteoma of the hip after radiofrequency ablation: A case report and review of the literature. Cases J. 2009, 17, 2–6439. [Google Scholar] [CrossRef]
- Dorfman, H.D. The spectrum of benign osteoblastic tumors. Int. J. Surg Pathol. 2010, 18, 75S–78S. [Google Scholar] [CrossRef]
- Atesok, K.I.; Alman, B.A.; Schemitsch, E.H.; Peyser, A.; Mankin, H. Osteoid osteoma and osteoblastoma. J. Am. Acad. Orthop. Surg. 2011, 19, 678–689. [Google Scholar] [CrossRef]
- Abboud, S.; Kosmas, C.; Novak, R.; Robbin, M. Long-term clinical outcomes of dual-cycle radiofrequency ablation technique for treatment of osteoid osteoma. Skelet. Radiol. 2016, 45, 599–606. [Google Scholar] [CrossRef]
- Sano, H.; Hatori, M.; Mineta, M.; Hosaka, M.; Itoi, E. Tumors masked as frozen shoulders: A retrospective analysis. J. Shoulder Elb. Surg. 2010, 19, 262–266. [Google Scholar] [CrossRef]
- Vijayan, S.; Jain, C.; Naik, M.A.; Rao, S.K. Osteoid osteoma of the calcaneus misdiagnosed as subtalar sprain. Indian J. Cancer 2019, 56, 350–353. [Google Scholar] [CrossRef]
- Weber, M.A.; Sprengel, S.D.; Omlor, G.W.; Lehner, B.; Wiedenhöfer, B.; Kauczor, H.U.; Rehnitz, C. Clinical long-term outcome, technical success, and cost analysis of radiofrequency ablation for the treatment of osteoblastomas and spinal osteoid osteomas in comparison to open surgical resection. Skelet. Radiol. 2015, 44, 981–993. [Google Scholar] [CrossRef] [PubMed]
- Sahin, C.; Oc, Y.; Ediz, N.; Altınay, M.; Bayrak, A.H. The safety and the efficacy of computed tomography guided percutaneous radiofrequency ablation of osteoid osteoma. Acta Orthop. Traumatol. Turc. 2019, 53, 360–365. [Google Scholar] [CrossRef] [PubMed]
- Farrar, J.T.; Young, J.P., Jr.; LaMoreaux, L.; Werth, J.L.; Poole, R.M. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain 2001, 94, 149–158. [Google Scholar] [CrossRef]
- Hegedus, E.J.; Goode, A.; Campbell, S.; Morin, A.; Tamaddoni, M.; Moorman, C.T., 3rd. Physical examination tests of the shoulder: A systematic review with meta-analysis of individual tests. Br. J. Sports Med. 2008, 42, 80–92. [Google Scholar] [CrossRef]
- Hegedus, E.J.; Goode, A.P.; Cook, C.E.; Michener, L.; Myer, C.A.; Myer, D.M.; A Wright, A.A. Which physical examination tests provide clinicians with the most value when examining the shoulder? Update of a systematic review with meta-analysis of individual tests. Br. J. Sports Med. 2012, 46, 964–978. [Google Scholar] [CrossRef]
- Hegedus, E.J.; Cook, C.; Lewis, J.; Wright, A.; Park, J.Y. Combining orthopedic special tests to improve diagnosis of shoulder pathology. Phys. Ther. Sport 2015, 16, 87–92. [Google Scholar] [CrossRef]
- Hanchard, N.C.A.; Lenza, M.; Handoll, H.H.G.; Takwoingi, Y. Physical tests for shoulder impingements and local lesions of bursa, tendon or labrum that may accompany impingement. Cochrane Database Syst. Rev. 2013, 2013, CD007427. [Google Scholar] [CrossRef]
- Brindisino, F.; Giovannico, G.; Maselli, F. Conservative management in a patient with massive rotator cuff tear and rheumatoid arthritis. J. Back Musculoskelet. Rehabil. 2020, 33, 329–337. [Google Scholar] [CrossRef]
- Wainner, R.S.; Fritz, J.M.; Irrgang, J.J.; Boninger, M.L.; Delitto, A.; Allison, S. Reliability and diagnostic accuracy of the clinical examination and patient self-report measures for cervical radiculopathy. Spine 2003, 28, 52–62. [Google Scholar] [CrossRef] [PubMed]
- Brindisino, F.; Pellicciari, L.; Lorusso, M.; Pennella, D.; Padua, R.; Di Bari, M. Cross-cultural adaptation, reliability, and validity of the Italian version of the Shoulder Disability Questionnaire. Musculoskelet. Sci. Pract. 2020, 46, 102123. [Google Scholar] [CrossRef] [PubMed]
- Apolone, G.; Mosconi, P. The Italian SF-36 Health Survey: Translation, validation and norming. J. Clin. Epidemiol. 1998, 51, 1025–1036. [Google Scholar] [CrossRef]
- Littlewood, C. Contractile dysfunction of the shoulder (rotator cuff tendinopathy): An overview. J. Man. Manip. Ther. 2012, 20, 209–213. [Google Scholar] [CrossRef] [PubMed]
- Steuri, R.; Sattelmayer, M.; Elsig, S.; Kolly, C.; Tal, A.; Taeymans, J.; Hilfiker, R. Effectiveness of conservative interventions including exercise, manual therapy and medical management in adults with shoulder impingement: A systematic review and meta-analysis of RCTs. Br. J. Sports Med. 2017, 51, 1340–1347. [Google Scholar] [CrossRef] [PubMed]
- Ristori, D.; Miele, S.; Rossettini, G.; Monaldi, E.; Arceri, D.; Testa, M. Towards an integrated clinical framework for patient with shoulder pain. Arch. Physiother. 2018, 8, 7. [Google Scholar] [CrossRef] [PubMed]
- Desjardins-Charbonneau, A.; Roy, J.S.; Dionne, C.E.; Frémont, P.; MacDermid, J.C.; Desmeules, F. The efficacy of manual therapy for rotator cuff tendinopathy: A systematic review and meta-analysis. J. Orthop. Sports Phys. Ther. 2015, 45, 330–350. [Google Scholar] [CrossRef]
- Mourad, F.; Giovannico, G.; Maselli, F.; Bonetti, F.; Fernández de las Peñas, C.; Dunning, J. Basilar impression presenting as intermittent mechanical neck pain: A rare case report. BMC Musculoskelet. Disord. 2016, 17, 7. [Google Scholar] [CrossRef]
- Mourad, F.; Maselli, F.; Cataldi, F.; Pennella, D.; Pt, C.F.-D.; Dunning, J. Hip bone marrow edema presenting as low back pain: A case report. Physiother. Theory Pract. 2020, 36, 249–257. [Google Scholar] [CrossRef]
- Sizer, P.S.; Brismée, J.M.; Cook, C. Medical screening for red flags in the diagnosis and management of musculoskeletal spine pain. Pain Pract. 2007, 7, 53–71. [Google Scholar] [CrossRef]
- Boissonnault, W.; Goodman, C. Physical therapists as diagnosticians: Drawing the line on diagnosing pathology. J. Orthop. Sports Phys. Ther. 2006, 36, 351–353. [Google Scholar] [CrossRef] [PubMed]
- Louw, A.; Zimney, K.; Puentedura, E.J.; Diener, I. The efficacy of pain neuroscience education on musculoskeletal pain: A systematic review of the literature. Physiother. Theory Pract. 2016, 32, 332–355. [Google Scholar] [CrossRef] [PubMed]
- Goyal, S.; Said, H.G. Osteoid osteoma (OO) of the coracoid: A case report of arthroscopic excision and review of literature. SICOT J. 2015, 10, 1–17. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Szendroi, M.; Kollo, K.; Antal, I.; Lakatos, J.; Szoke, G. Intraarticular osteoid osteoma. Clinical features, imaging results, and comparison with extraarticular localization. J. Rheumatol. 2004, 31, 957–964. [Google Scholar] [CrossRef] [PubMed]
- Bauer, T.W.; Zehr, R.J.; Belhobek, G.H.; Marks, K.E. Juxta- articular osteoid osteoma. Am. J. Surg Pathol. 1991, 15, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Yochum, T.R.; Rowe, L.J. Essentials of Skeletal Radiology; Williams and Wilkins: Baltimore, MD, USA, 1987; pp. 816–822. [Google Scholar]
- Chai, J.W.; Hong, S.H.; Choi, J.-Y.; Koh, Y.H.; Lee, J.W.; Kang, H.S. Radiologic Diagnosis of Osteoid Osteoma: From Simple to Challenging Findings. Radiographics 2010, 30, 737–749. [Google Scholar] [CrossRef]
- Marin, R.; Papierski, P. Unusual presentation of an osteoid osteoma. Mil. Med. 1996, 161, 438–440. [Google Scholar] [CrossRef]
- Simone, F.C.; Knaap, D.C. Undiagnosed brodies abscess in a gymnast after surgical fixation of a tibial fracture. J. Chiropr. Med. 2007, 6, 159–162. [Google Scholar]
- Brindisino, F.; Passudetti, V.; Pennella, D.; Giovannico, G.; Heick, J.D. Recognition of pulmonary pathology in a patient presenting with shoulder pain. Physiother. Theory Pract. 2020, 27, 1–11. [Google Scholar] [CrossRef]
- Lollino, N.; Brunocilla, P.R.; Poglio, F.; Vannini, E.; Lollino, S.; Lancia, M. 2012 Non-orthopaedic causes of shoulder pain: What the shoulder expert must remember. Musculoskelet. Surg. 2012, 96, 63–68. [Google Scholar] [CrossRef]
- Walsh, R.M.; Sadowski, G.E. Systemic disease mimicking musculoskeletal dysfunction: A case report involving referred shoulder pain. J. Orthop. Sports Phys. Ther. 2001, 31, 696–701. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Grunau, G.L.; Darlow, B.; Flynn, T.; O’Sullivan, K.; O’Sullivan, P.B.; Forster, B.B. Red flags or red herrings? Redefining the role of red flags in low back pain to reduce overimaging. Br. J. Sports Med. 2018, 52, 488–489. [Google Scholar] [CrossRef] [PubMed]
- Finucane, L.M.; Downie, A.; Mercer, C.; Greenhalgh, S.M.; Boissonnault, W.G.; Pool-Goudzwaard, A.; Beneciuk, J.M.; Leech, R.L.; Selfe, J. International Framework for Red Flags for Potential Serious Spinal Pathologies. J. Orthop. Sports Phys. Ther. 2020, 50, 350–372. [Google Scholar] [CrossRef] [PubMed]
- Borsa, P.A.; Laudner, K.G.; Sauers, E.L. Mobility and stability adaptations in the shoulder of the overhead athlete. Sports Med. 2008, 38, 17–36. [Google Scholar] [CrossRef] [PubMed]
- Aytar, A.; Zeybek, A.; Pekyavas, N.O.; Tigli, A.A.; Ergun, N. Scapular resting position, shoulder pain and function in disabled athletes. Prosthet. Orthot. Int. 2015, 39, 390–396. [Google Scholar] [CrossRef]
- Glanzmann, M.C.; Imhoff, A.B.; Schwyzer, H.K. Osteoid osteoma of the shoulder and elbow: From diagnosis to minimally invasive removal. Int. Orthop. 2013, 37, 2403–2408. [Google Scholar] [CrossRef]
- Barreto, R.; Braman, J.P.; Ludewig, P.; Ribeiro, L.P.; Camargo, P.R. Bilateral magnetic resonance imaging findings in individuals with unilateral shoulder pain. J. Shoulder Elb. Surg. 2019, 28, 1699–1706. [Google Scholar] [CrossRef]
- Lee, C.S.; Goldhaber, N.H.; Davis, S.M.; Dilley, M.L.; Brock, A.; Wosmek, J.; Lee, E.H.; Lee, R.K.; Stetson, W.B. Shoulder MRI in asymptomatic elite volleyball athletes shows extensive pathology. J. ISAKOS 2020, 5, 10–14. [Google Scholar] [CrossRef]
- McCarthy, C.J.; Arnall, F.A.; Strimpakos, N.; Freemont, A.; Oldham, J.A. The Biopsychosocial Classification of Non-Specific Low Back Pain: A Systematic Review. Phys. Ther. Rev. 2004, 9, 17–30. [Google Scholar] [CrossRef]
- Koes, B.W.; van Tulder, M.; Lin, C.-W.C.; Macedo, L.G.; McAuley, J.; Maher, C. An updated overview of clinical guidelines for the management of non-specific low back pain in primary care. Eur. Spine J. 2010, 19, 2075–2094. [Google Scholar] [CrossRef]
- Maselli, F.; Palladino, M.; Barbari, V.; Storari, L.; Rossettini, G.; Testa, M. The diagnostic value of Red Flags in thoracolumbar pain: A systematic review. Disabil. Rehabil. 2020, 19, 1–17. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1st week (3 sessions) |
|
| 2nd week (3 sessions) |
|
| 3rd week (2 sessions) |
|
| 4th week (2 sessions) |
|
| 5th week (1 session) and 6th week (1 session) |
|
| 1st Day Examination | 6th-Week Follow Up | ||||||||||||||
| NPRS 6/10 | NPRS 0/10 | ||||||||||||||
| SDQ 12 (activity) 8 (participation, psychosocial factors) | SDQ 2 (activity) 1 (participation, psychosocial factors) | ||||||||||||||
| SF 36 | SF 36 | ||||||||||||||
| Physical Functioning | Limitations—Physical Health | Pain | General Health | Energy/Fatigue | Social Activities | Limitation—Emotional Problems | Emotional Well-Being | Physical Functioning | Limitations—Physical Health | Pain | General Health | Energy/Fatigue | Social Activities | Limitation—Emotional Problems | Emotional Well-Being |
| 35 | 0 | 30 | 37 | 55 | 25 | 66 | 56 | 70 | 100 | 61 | 72 | 75 | 75 | 100 | 80 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maselli, F.; Storari, L.; Lorusso, M.; Mourad, F.; Pennella, D.; Barbari, V.; Salomon, M.; Brindisino, F. Osteoid Osteoma in an Adult Wheelchair Basketball Player Mimicking Musculoskeletal Shoulder Pain: Red Flag or a Red Herring? Tomography 2022, 8, 389-401. https://doi.org/10.3390/tomography8010032
Maselli F, Storari L, Lorusso M, Mourad F, Pennella D, Barbari V, Salomon M, Brindisino F. Osteoid Osteoma in an Adult Wheelchair Basketball Player Mimicking Musculoskeletal Shoulder Pain: Red Flag or a Red Herring? Tomography. 2022; 8(1):389-401. https://doi.org/10.3390/tomography8010032
Chicago/Turabian StyleMaselli, Filippo, Lorenzo Storari, Mariangela Lorusso, Firas Mourad, Denis Pennella, Valerio Barbari, Mattia Salomon, and Fabrizio Brindisino. 2022. "Osteoid Osteoma in an Adult Wheelchair Basketball Player Mimicking Musculoskeletal Shoulder Pain: Red Flag or a Red Herring?" Tomography 8, no. 1: 389-401. https://doi.org/10.3390/tomography8010032
APA StyleMaselli, F., Storari, L., Lorusso, M., Mourad, F., Pennella, D., Barbari, V., Salomon, M., & Brindisino, F. (2022). Osteoid Osteoma in an Adult Wheelchair Basketball Player Mimicking Musculoskeletal Shoulder Pain: Red Flag or a Red Herring? Tomography, 8(1), 389-401. https://doi.org/10.3390/tomography8010032