
Micro-Ultrasound in the Detection of Clinically Significant Prostate Cancer: A Comprehensive Review and Comparison with Multiparametric MRI

 ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
3. Overview of Imaging Modalities
3.1. MRI Overview
3.2. Micro-Ultrasound Overview
4. Micro-Ultrasound Clinical Use
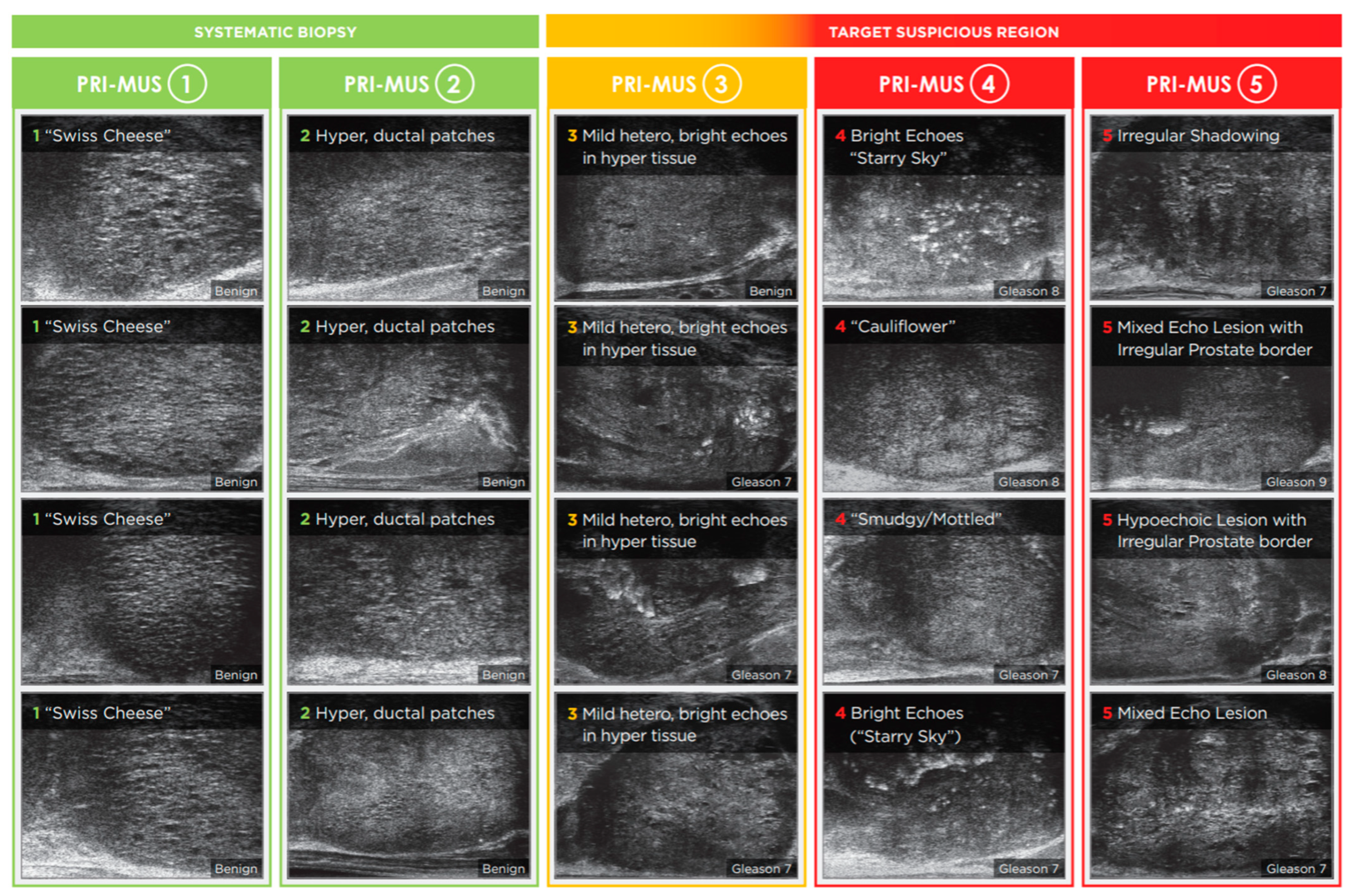
4.1. Development of PRI-MUS
4.2. Micro-US vs. TRUS and Systematic Biopsy
4.3. Micro-US vs. mpMRI
5. Discussion
Limitations and Challenges of Micro-US
6. Future Directions
6.1. Clinical Validation and Integration into Guidelines
6.2. Surgical Planning and Tumor Staging
6.3. Artificial Intelligence and Operator Standardization
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Kratzer, T.B.; Giaquinto, A.N.; Sung, H.; Jemal, A. Cancer statistics, 2025. CA Cancer J. Clin. 2025, 75, 10–45. [Google Scholar] [CrossRef] [PubMed]
- Litwin, M.S.; Tan, H.J. The Diagnosis and Treatment of Prostate Cancer: A Review. JAMA 2017, 317, 2532–2542. [Google Scholar] [CrossRef] [PubMed]
- Yacoub, J.H.; Verma, S.; Moulton, J.S.; Eggener, S.; Oto, A. Imaging-guided Prostate Biopsy: Conventional and Emerging Techniques. RadioGraphics 2012, 32, 819–837. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, H.U.; Bosaily, A.E.S.; Brown, L.C.; Gabe, R.; Kaplan, R.; Parmar, M.K.; Collaco-Moraes, Y.; Ward, K.; Hindley, R.G.; Freeman, A.; et al. Diagnostic accuracy of multi-parametric MRI and TRUS biopsy in prostate cancer (PROMIS): A paired validating confirmatory study. Lancet 2017, 389, 815–822. [Google Scholar] [CrossRef]
- Drost, F.J.H.; Osses, D.F.; Nieboer, D.; Steyerberg, E.W.; Bangma, C.H.; Roobol, M.J.; Schoots, I.G. Prostate MRI, with or without MRI-targeted biopsy, and systematic biopsy for detecting prostate cancer. Cochrane Database Syst. Rev. 2019, 4, CD012663. [Google Scholar] [CrossRef]
- Early Detection of Prostate Cancer: AUA/SUO Guideline (2023)-American Urological Association. Available online: https://www.auanet.org/guidelines-and-quality/guidelines/early-detection-of-prostate-cancer-guidelines (accessed on 22 April 2025).
- Cornford, P.; van den Bergh, R.C.N.; Briers, E.; Van den Broeck, T.; Brunckhorst, O.; Darraugh, J.; Eberli, D.; De Meerleer, G.; De Santis, M.; Farolfi, A.; et al. EAU-EANM-ESTRO-ESUR-ISUP-SIOG Guidelines on Prostate Cancer—2024 Update. Part I: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur. Urol. 2024, 86, 148–163. [Google Scholar] [CrossRef]
- Schoots, I.G.; Barentsz, J.O.; Bittencourt, L.K.; Haider, M.A.; Macura, K.J.; Margolis, D.J.A.; Moore, C.M.; Oto, A.; Panebianco, V.; Siddiquiet, M.M.; et al. PI-RADS Committee Position on MRI Without Contrast Medium in Biopsy-Naive Men With Suspected Prostate Cancer: Narrative Review. Am. J. Roentgenol. 2021, 216, 3–19. [Google Scholar] [CrossRef]
- Faria, R.; Soares, M.O.; Spackman, E.; Ahmed, H.U.; Brown, L.C.; Kaplan, R.; Emberton, M.; Sculpher, M.J. Optimising the Diagnosis of Prostate Cancer in the Era of Multiparametric Magnetic Resonance Imaging: A Cost-effectiveness Analysis Based on the Prostate MR Imaging Study (PROMIS). Eur. Urol. 2018, 73, 23–30. [Google Scholar] [CrossRef]
- Padhani, A.R.; Godtman, R.A.; Schoots, I.G. Key learning on the promise and limitations of MRI in prostate cancer screening. Eur. Radiol. 2024, 34, 6168–6174. [Google Scholar] [CrossRef]
- Ghadimi, M.; Thomas, A. Magnetic Resonance Imaging Contraindications. In StatPearls; StatPearls Publishing: Tampa, FL, USA, 2025. Available online: http://www.ncbi.nlm.nih.gov/books/NBK551669/ (accessed on 29 June 2025).
- Kinnaird, A.; Luger, F.; Cash, H.; Ghai, S.; Urdaneta-Salegui, L.F.; Pavlovich, C.P.; Brito, J.; Shore, N.D.; Struck, J.P.; Schostak, M.; et al. Microultrasonography-Guided vs MRI-Guided Biopsy for Prostate Cancer Diagnosis: The OPTIMUM Randomized Clinical Trial. JAMA 2025, 333, 1679–1687. [Google Scholar] [CrossRef]
- Pavlovich, C.P.; Cornish, T.C.; Mullins, J.K.; Fradin, J.; Mettee, L.Z.; Connor, J.T.; Reese, A.C.; Askin, F.B.; Luck, R.; Epstein, J.I.; et al. High-resolution transrectal ultrasound: Pilot study of a novel technique for imaging clinically localized prostate cancer. Urol. Oncol. Semin. Orig. Investig. 2014, 32, e27–e32. [Google Scholar] [CrossRef] [PubMed]
- Wiemer, L.; Hollenbach, M.; Heckmann, R.; Kittner, B.; Plage, H.; Reimann, M.; Asbach, P.; Friedersdorff, F.; Schlomm, T.; Hofbaue, S.; et al. Evolution of Targeted Prostate Biopsy by Adding Micro-Ultrasound to the Magnetic Resonance Imaging Pathway. Eur. Urol. Focus 2021, 7, 1292–1299. [Google Scholar] [CrossRef] [PubMed]
- Lughezzani, G.; Maffei, D.; Saita, A.; Paciotti, M.; Diana, P.; Buffi, N.M.; Colombo, P.; Elefante, G.M.; Hurle, R.; Lazzeri, M.; et al. Diagnostic Accuracy of Microultrasound in Patients with a Suspicion of Prostate Cancer at Magnetic Resonance Imaging: A Single-institutional Prospective Study. Eur. Urol. Focus 2021, 7, 1019–1026. [Google Scholar] [CrossRef]
- Ghai, S.; Eure, G.; Fradet, V.; Hyndman, M.E.; McGrath, T.; Wodlinger, B.; Pavlovich, C.P. Assessing Cancer Risk on Novel 29 MHz Micro-Ultrasound Images of the Prostate: Creation of the Micro-Ultrasound Protocol for Prostate Risk Identification. J. Urol. 2016, 196, 562–569. [Google Scholar] [CrossRef]
- Eure, G.; Fanney, D.; Lin, J.; Wodlinger, B.; Ghai, S. Comparison of conventional transrectal ultrasound, magnetic resonance imaging, and micro-ultrasound for visualizing prostate cancer in an active surveillance population: A feasibility study. Can. Urol. Assoc. J. 2019, 13, E70–E77. [Google Scholar] [CrossRef]
- Zhang, M.; Wang, R.; Wu, Y.; Jing, J.; Chen, S.; Zhang, G.; Xu, B.; Liu, C.; Chen, M. Micro-Ultrasound Imaging for Accuracy of Diagnosis in Clinically Significant Prostate Cancer: A Meta-Analysis. Front. Oncol. 2019, 9, 1368. [Google Scholar] [CrossRef]
- Abouassaly, R.; Klein, E.A.; El-Shefai, A.; Stephenson, A. Impact of using 29 MHz high-resolution micro-ultrasound in real-time targeting of transrectal prostate biopsies: Initial experience. World J. Urol. 2020, 38, 1201–1206. [Google Scholar] [CrossRef]
- Claros, O.R.; Tourinho-Barbosa, R.R.; Fregeville, A.; Gallardo, A.C.; Muttin, F.; Carneiro, A.; Stabile, A.; Moschini, M.; Macek, P.; Cathala, N.; et al. Comparison of Initial Experience with Transrectal Magnetic Resonance Imaging Cognitive Guided Micro-Ultrasound Biopsies versus Established Transperineal Robotic Ultrasound Magnetic Resonance Imaging Fusion Biopsies for Prostate Cancer. J. Urol. 2020, 203, 918–925. [Google Scholar] [CrossRef] [PubMed]
- Cornud, F.; Lefevre, A.; Flam, T.; Dumonceau, O.; Galiano, M.; Soyer, P.; Camparo, P.; Barral, M. MRI-directed high-frequency (29MhZ) TRUS-guided biopsies: Initial results of a single-center study. Eur. Radiol. 2020, 30, 4838–4846. [Google Scholar] [CrossRef]
- Socarrás, M.E.R.; Rivas, J.G.; Rivera, V.C.; Elbers, J.R.; González, L.L.; Mercado, I.M.; Del Alamo, J.F.; Del Dago, P.J.; Sancha, F.G. Prostate Mapping for Cancer Diagnosis: The Madrid Protocol. Transperineal Prostate Biopsies Using Multiparametric Magnetic Resonance Imaging Fusion and Micro-Ultrasound Guided Biopsies. J. Urol. 2020, 204, 726–733. [Google Scholar] [CrossRef]
- Chessa, F.; Schiavina, R.; Ercolino, A.; Gaudiano, C.; Giusti, D.; Bianchi, L.; Pultrone, C.; Marcelli, E.; Distefano, C.; Lodigiani, L.; et al. Diagnostic accuracy of the Novel 29 MHz micro-ultrasound “ExactVuTM” for the detection of clinically significant prostate cancer: A prospective single institutional study. A step forward in the diagnosis of prostate cancer. Arch. Ital. Di Urol. E Androl. 2021, 93, 132–138. [Google Scholar] [CrossRef] [PubMed]
- Klotz, L.; Lughezzani, G.; Maffei, D.; Sánchez, A.; Pereira, J.G.; Staerman, F.; Cash, H.; Luger, F.; Lopez, L.; Sanchez-Salas, F.; et al. Comparison of micro-ultrasound and multiparametric magnetic resonance imaging for prostate cancer: A multicenter, prospective analysis. Can. Urol. Assoc. J. 2021, 15, E11–E16, Erratum in Can. Urol. Assoc. J. 2022, 16, E111. [Google Scholar] [CrossRef] [PubMed]
- Pavlovich, C.P.; Hyndman, M.E.; Eure, G.; Ghai, S.; Caumartin, Y.; Herget, E.; Young, J.D.; Wiseman, D.; Caughlin, C.; Gray, R.E.; et al. A multi-institutional randomized controlled trial comparing first-generation transrectal high-resolution micro-ultrasound with conventional frequency transrectal ultrasound for prostate biopsy. BJUI Compass 2021, 2, 126–133. [Google Scholar] [CrossRef]
- Sountoulides, P.; Pyrgidis, N.; Polyzos, S.A.; Mykoniatis, I.; Asouhidou, E.; Papatsoris, A.; Dellis, A.; Anastasiadis, A.; Lusuardi, L.; Hatzichristou, D. Micro-Ultrasound–Guided vs Multiparametric Magnetic Resonance Imaging-Targeted Biopsy in the Detection of Prostate Cancer: A Systematic Review and Meta-Analysis. J. Urol. 2021, 205, 1254–1262. [Google Scholar] [CrossRef]
- Ghai, S.; Perlis, N.; Atallah, C.; Jokhu, S.; Corr, K.; Lajkosz, K.; Incze, P.F.; Zlotta, A.R.; Jain, U.; Fleming, H.; et al. Comparison of Micro-US and Multiparametric MRI for Prostate Cancer Detection in Biopsy-Naive Men. Radiology 2022, 305, 390–398. [Google Scholar] [CrossRef]
- Hofbauer, S.L.; Luger, F.; Harland, N.; Plage, H.; Reimann, M.; Hollenbach, M.; Gusenleitner, A.; Stenzl, A.; Schlomm, T.; Wiemer, L.; et al. A non-inferiority comparative analysis of micro-ultrasonography and MRI-targeted biopsy in men at risk of prostate cancer. BJU Int. 2022, 129, 648–654. [Google Scholar] [CrossRef] [PubMed]
- You, C.; Li, X.; Du, Y.; Peng, L.; Wang, H.; Zhang, X.; Wang, A. The Microultrasound-Guided Prostate Biopsy in Detection of Prostate Cancer: A Systematic Review and Meta-Analysis. J. Endourol. 2022, 36, 394–402. [Google Scholar] [CrossRef]
- Cotter, F.; Perera, S.; Sathianathen, N.; Lawrentschuk, N.; Murphy, D.; Bolton, D. Comparing the Diagnostic Performance of Micro-Ultrasound-Guided Biopsy Versus Multiparametric Magnetic Resonance Imaging-Targeted Biopsy in the Detection of Clinically Significant Prostate Cancer: A Systematic Review and Meta-Analysis. Société Int. D’Urologie J. 2023, 4, 465–479. Available online: https://api.semanticscholar.org/CorpusID:265510002 (accessed on 23 May 2025). [CrossRef]
- Dariane, C.; Ploussard, G.; Barret, E.; Beauval, J.-B.; Brureau, L.; Créhange, G.; Fromont, G.; Gauthé, M.; Mathieu, R.; Renard-Penna, R.; et al. Micro-ultrasound-guided biopsies versus systematic biopsies in the detection of prostate cancer: A systematic review and meta-analysis. World J. Urol. 2023, 41, 641–651. [Google Scholar] [CrossRef]
- Rojo, E.G.; Gómez, B.G.; Sutil, R.S.; Arzayus, D.V.; Quintas, J.J.; Barreras, S.G.; Menéndez, R.B.; Vallejo, E.P.; Montalvo, C.C.; Curtis, D.L.; et al. Comparison in Detection Rate of Clinically Significant Prostate Cancer Between Microultrasound-guided Prostate Biopsy (ExactVu) and Multiparametric Resonance Imaging-guided Prostate Biopsy (Koelis System). Urology 2024, 183, 163–169. [Google Scholar] [CrossRef]
- Zhou, S.R.; Choi, M.H.; Vesal, S.; Kinnaird, A.; Brisbane, W.G.; Lughezzani, G.; Maffei, D.; Fasulo, V.; Albers, P.; Zhang, L.; et al. Inter-reader Agreement for Prostate Cancer Detection Using Micro-ultrasound: A Multi-institutional Study. Eur. Urol. Open Sci. 2024, 66, 93–100. [Google Scholar] [CrossRef]
- Grover, V.P.B.; Tognarelli, J.M.; Crossey, M.M.E.; Cox, I.J.; Taylor-Robinson, S.D.; McPhail, M.J.W. Magnetic Resonance Imaging: Principles and Techniques: Lessons for Clinicians. J. Clin. Exp. Hepatol. 2015, 5, 246–255. [Google Scholar] [CrossRef] [PubMed]
- Turkbey, B.; Brown, A.M.; Sankineni, S.; Wood, B.J.; Pinto, P.A.; Choyke, P.L. Multiparametric prostate magnetic resonance imaging in the evaluation of prostate cancer. CA Cancer J. Clin. 2016, 66, 326–336. [Google Scholar] [CrossRef] [PubMed]
- Barentsz, J.O.; Richenberg, J.; Clements, R.; Choyke, P.; Verma, S.; Villeirs, G.; Rouviere, O.; Logager, V.; Fütterer, J.J. ESUR prostate MR guidelines 2012. Eur. Radiol. 2012, 22, 746–757. [Google Scholar] [CrossRef]
- Weinreb, J.C.; Barentsz, J.O.; Choyke, P.L.; Cornud, F.; Haider, M.A.; Macura, K.J.; Margolis, D.; Schnall, M.D.; Shtern, F.; Tempany, C.M.; et al. PI-RADS Prostate Imaging–Reporting and Data System: 2015, Version 2. Eur. Urol. 2016, 69, 16–40. [Google Scholar] [CrossRef]
- Woo, S.; Suh, C.H.; Kim, S.Y.; Cho, J.Y.; Kim, S.H. Diagnostic Performance of Prostate Imaging Reporting and Data System Version 2 for Detection of Prostate Cancer: A Systematic Review and Diagnostic Meta-analysis. Eur. Urol. 2017, 72, 177–188. [Google Scholar] [CrossRef]
- Turkbey, B.; Rosenkrantz, A.B.; Haider, M.A.; Padhani, A.R.; Villeirs, G.; Macura, K.J.; Tempany, C.M.; Choyke, P.L.; Cornud, F.; Margolis, D.J.; et al. Prostate Imaging Reporting and Data System Version 2.1: 2019 Update of Prostate Imaging Reporting and Data System Version 2. Eur. Urol. 2019, 76, 340–351. [Google Scholar] [CrossRef]
- Park, K.J.; Choi, S.H.; Kim, M.-H.; Kim, J.K.; Jeong, I.G. Performance of Prostate Imaging Reporting and Data System Version 2.1 for Diagnosis of Prostate Cancer: A Systematic Review and Meta-Analysis. J. Magn. Reason. Imaging 2021, 54, 103–112. [Google Scholar] [CrossRef] [PubMed]
- Kasivisvanathan, V.; Rannikko, A.S.; Borghi, M.; Panebianco, V.; Mynderse, L.A.; Vaarala, M.H.; Briganti, A.; Budäus, L.; Hellawell, G.; Hindley, R.G.; et al. MRI-Targeted or Standard Biopsy for Prostate-Cancer Diagnosis. N. Engl. J. Med. 2018, 378, 1767–1777. [Google Scholar] [CrossRef]
- Van Der Leest, M.; Cornel, E.; Israël, B.; Hendriks, R.; Padhani, A.R.; Hoogenboom, M.; Zamecnik, P.; Bakker, D.; Setiasti, A.Y.; Veltman, J.; et al. Head-to-head Comparison of Transrectal Ultrasound-guided Prostate Biopsy Versus Multiparametric Prostate Resonance Imaging with Subsequent Magnetic Resonance-guided Biopsy in Biopsy-naïve Men with Elevated Prostate-specific Antigen: A Large Prospective Multicenter Clinical Study. Eur. Urol. 2019, 75, 570–578. [Google Scholar] [CrossRef]
- Rouvière, O.; Puech, P.; Renard-Penna, R.; Claudon, M.; Roy, C.; Mège-Lechevallier, F.; Decaussin-Petrucci, M.; Dubreuil-Chambardel, M.; Magaud, L.; Remontet, L.; et al. Use of prostate systematic and targeted biopsy on the basis of multiparametric MRI in biopsy-naive patients (MRI-FIRST): A prospective, multicentre, paired diagnostic study. Lancet Oncol. 2019, 20, 100–109. [Google Scholar] [CrossRef] [PubMed]
- Prostate Cancer: Early Detection Guideline-American Urological Association. Available online: https://www.auanet.org/guidelines-and-quality/guidelines/prostate-cancer-early-detection-guideline?utm (accessed on 24 April 2025).
- Exact Imaging Announces Health Canada Approval and License for its ExactVu™ Micro-Ultrasound System for Prostate Imaging and Biopsy-Exact Imaging. Available online: https://www.exactimaging.com/press-releases/exact-imaging-announces-health-canada-approval-and-license (accessed on 22 April 2025).
- Urology of Virginia First US Practice to Acquire Novel ExactVu™ Micro-Ultrasound System for Prostate Imaging and Biopsy-Exact Imaging. Available online: https://www.exactimaging.com/press-releases/urology-of-virginia-first-us-practice-to-acquire-novel-exactvu-system (accessed on 22 April 2025).
- Ng, A.; Swanevelder, J. Resolution in ultrasound imaging. Contin. Educ. Anaesth. Crit. Care Pain 2011, 11, 186–192. [Google Scholar] [CrossRef]
- Vassallo, R.; Mannas, M.P.; Salcudean, S.E. Black PC. Developments in Ultrasound-Based Imaging for Prostate Cancer Detection. Prostate 2025, 85, 823–832. [Google Scholar] [CrossRef]
- PN 7095 PRI-MUS Anterior Quick Reference Poster EN Rev 1.2.pdf. Available online: https://www.exactimaging.com/images/manuals/English/PN%207095%20PRI-MUS%20Anterior%20Quick%20Reference%20Poster%20EN%20Rev%201.2.pdf (accessed on 22 April 2025).
- Schaer, S.; Rakauskas, A.; Dagher, J.; Rosa, S.L.; Pensa, J.; Brisbane, W.; Marks, L.; Kinnaird, A.; Abouassaly, R.; Klein, E.; et al. Assessing cancer risk in the anterior part of the prostate using micro-ultrasound: Validation of a novel distinct protocol. World J. Urol. 2023, 41, 3325–3331. [Google Scholar] [CrossRef]
- van Velthoven, R.; Diamand, R.; Mozer, P.; Barry de Longchamp, N. Letter to the Editor on “Comparison in Detection Rate of Clinically Significant Prostate Cancer Between Microultrasound-guided Prostate Biopsy (ExactVu) and Multiparametric Resonance Imaging-guided Prostate Biopsy (Koelis System)”. Urology 2024, 190, 173–174. [Google Scholar] [CrossRef]
- Rosenkrantz, A.B.; Ayoola, A.; Hoffman, D.; Khasgiwala, A.; Prabhu, V.; Smereka, P.; Somberg, M.; Taneja, S.S. The Learning Curve in Prostate MRI Interpretation: Self-Directed Learning Versus Continual Reader Feedback. Am. J. Roentgenol. 2017, 208, W92–W100. [Google Scholar] [CrossRef] [PubMed]
- Halstuch, D.; Baniel, J.; Lifshitz, D.; Sela, S.; Ber, Y.; Margel, D. Characterizing the learning curve of MRI-US fusion prostate biopsies. Prostate Cancer Prostatic Dis. 2019, 22, 546–551. [Google Scholar] [CrossRef]
- Kasabwala, K.; Patel, N.; Cricco-Lizza, E.; Shimpi, A.A.; Weng, S.; Buchmann, R.M.; Motanagh, S.; Wu, Y.; Banerjee, S.; Khani, F.; et al. The Learning Curve for Magnetic Resonance Imaging/Ultrasound Fusion-guided Prostate Biopsy. Eur. Urol. Oncol. 2019, 2, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Cash, H.; Hofbauer, S.L.; Shore, N.; Pavlovich, C.P.; Bulang, S.; Schostak, M.; Planken, E.; Jaspars, J.J.; Luger, F.; Klotz, L.; et al. Prostate Cancer Detection by Novice Micro-Ultrasound Users Enrolled in a Training Program. Société Int. D’Urologie J. 2022, 3, 62–68. [Google Scholar] [CrossRef]
- University of Alberta. A Phase 3, Multicenter, International, Non-Inferiority, Randomized Clinical Trial Comparing Screening for Prostate Cancer Using High Resolution Micro-Ultrasound Versus Multiparametric Magnetic Resonance Imaging (MUSIC-Screen); University of Alberta: Edmonton, AB, Canada, 2025; clinicaltrials.gov. Available online: https://clinicaltrials.gov/study/NCT06626022 (accessed on 23 May 2025).
- University of Alberta. Micro-UltraSound in Cancer-Active Surveillance (MUSIC-AS); University of Alberta: Edmonton, AB, Canada, 2025; clinicaltrials.gov. Available online: https://clinicaltrials.gov/study/NCT05558241 (accessed on 23 May 2025).
- Regis, F.; Casale, P.; Persico, F.; Colombo, P.; Cieri, M.; Guazzoni, G.; Buffi, N.M.; Lughezzani, G. Use of 29-MHz Micro-ultrasound for Local Staging of Prostate Cancer in Patients Scheduled for Radical Prostatectomy: A Feasibility Study. Eur. Urol. Open Sci. 2020, 19, 20–23. [Google Scholar] [CrossRef]
- Fasulo, V.; Buffi, N.M.; Regis, F.; Paciotti, M.; Persico, F.; Maffei, D.; Uleri, A.; Saita, A.; Casale, P.; Hurle, R.; et al. Use of high-resolution micro-ultrasound to predict extraprostatic extension of prostate cancer prior to surgery: A prospective single-institutional study. World J. Urol. 2022, 40, 435–442. [Google Scholar] [CrossRef] [PubMed]
- Seaman, E.K.; Sawczuk, I.S.; Fatal, M.; Olsson, C.A.; Shabsigh, R. Transperineal prostate needle biopsy guided by transurethral ultrasound in patients without a rectum. Urology 1996, 47, 353–355. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Liu, X.; Zhang, J.; Peng, C. A Backing-Layer-Shared Miniature Dual-Frequency Ultrasound Probe for Intravascular Ultrasound Imaging: In Vitro and Ex Vivo Validations. Biosensors 2023, 13, 971. [Google Scholar] [CrossRef] [PubMed]
- Richemond, A.; Peters, M.; Schaer, S.; Dagher, J.; La Rosa, S.; Matthey, J.; Vietti-Violi, N.; Roth, B.; Lucca, I.; Valerio, M.; et al. Predicting pathological tumor volume in prostate cancer lesions: A head-to-head comparison of micro-ultrasound vs. MRI. Urol. Oncol. Semin. Orig. Investig. 2025, 43, e15–e21. [Google Scholar] [CrossRef]
- Bhattacharya, I.; Khandwala, Y.S.; Vesal, S.; Shao, W.; Yang, Q.; Soerensen, S.J.C.; Fan, R.E.; Ghanouni, P.; Kunder, C.A.; Brooks, J.D.; et al. A review of artificial intelligence in prostate cancer detection on imaging. Ther. Adv. Urol. 2022, 14, 17562872221128791. [Google Scholar] [CrossRef]
- Rohrbach, D.; Wodlinger, B.; Wen, J.; Mamou, J.; Feleppa, E. High-Frequency Quantitative Ultrasound for Imaging Prostate Cancer Using a Novel Micro-Ultrasound Scanner. Ultrasound Med. Biol. 2018, 44, 1341–1354. [Google Scholar] [CrossRef]
- Shao, Y.; Wang, J.; Wodlinger, B.; Salcudean, S.E. Improving Prostate Cancer (PCa) Classification Performance by Using Three-Player Minimax Game to Reduce Data Source Heterogeneity. IEEE Trans. Med. Imaging 2020, 39, 3148–3158. [Google Scholar] [CrossRef]
- Jiang, H.; Imran, M.; Muralidharan, P.; Patel, A.; Pensa, J.; Liang, M.; Benidir, T.; Grajo, J.R.; Joseph, J.P.; Terry, R.; et al. MicroSegNet: A deep learning approach for prostate segmentation on micro-ultrasound images. Comput. Med. Imaging Graph. 2024, 112, 102326. [Google Scholar] [CrossRef]

{kind=link}
| Study | Enrollment Years | N | Study Type | Patient Population (BN = Biopsy-Naïve, AS = Active Surveillance) | Analysis Focus | Key Findings |
|---|---|---|---|---|---|---|
| Pavlovich 2014 [13] | 2010–2011 | 25 | Prospective (Pilot Study) | 100% Biopsy-Proven PCa | Lesion | Higher-frequency (16–21 MHz) displayed promising, but mostly insignificant improvements over lower-frequency US |
| Ghai 2016 [16] | 2013–2016 | 100 Cines | Prospective Collection w/Retrospective Diagnostic Validation | 0% AS, Unknown BN | Lesion | PRI-MUS protocol displays potential to be comparable to PI-RADS |
| Eure 2019 [17] | 16 December | 9 | Prospective Paired Diagnostic | 100% AS | Patient | Micro-US and mpMRI clinically comparable, while both outperformed conventional US |
| Zhang 2019 [18] | NA * | 769 | Systematic Review | Mixed | Pooled | First micro-US meta-analysis establishing pooled data; sensitivity: 0.91; specificity: 0.49; AUC: 0.82 |
| Abouassaly 2020 [19] | January–August 2018 | 67 | Prospective Paired Diagnostic | 72% BN | Patient | Transition from conventional US to micro-US led to relatively increased csPCa detection |
| Claros 2020 [20] | February 2017–September 2018 | 269 | Retrospective Cohort | 26% BN | Patient | Overall DR not statistically different, but targeted micro biopsies had significantly higher detection rates |
| Cornud 2020 [21] | February–June 2019 | 118 Patients, 144 Lesions | Prospective Paired Diagnostic | 67% BN, 18% AS | Mixed | mpMRI and micro-US both had instances of missed lesions, but only mpMRI missed csPCa lesions |
| Socarras 2020 [22] | February 2018–September 2019 | 194 | Prospective Paired Diagnostic | 66% BN | Patient | PRI-MUS had statistically significantly improved sensitivity and NPV over PI-RADS |
| Chessa 2021 [23] | June–September 2018 | 83 | Prospective Paired Diagnostic | 100% Biopsy-Proven PCa | Patient | Micro-US sensitivity considerably worse for anterior/transition zone lesions compared to peripheral zone |
| Klotz 2021 [24] | NA * | 1040 | Prospective Multicenter Paired Diagnostic | 66% BN, 6.3% AS | Patient | Micro-US sensitivity superior to mpMRI with non-inferior specificity |
| Lughezzani 2021 [15] | October 2017–September 2019 | 320 | Prospective Paired Diagnostic | 63% BN | Patient | mpMRI and micro-US roughly equivocal; systematic biopsy found 10.3% of csPCa missed by targeted biopsy |
| Pavlovich 2021 [25] | 2013–2016 | 1676 | Prospective Multicenter RCT | 0% AS, Unknown BN | Patient | No statistically significant difference between micro-US and conventional US; both saw improvements after PRI-MUS training |
| Sountoulides 2021 [26] | NA * | 1125 | Systematic Review/Meta-Analysis | Unspecified | Patient | No significant differences in mpMRI and micro-US for detection of GG ≥ 2 or GG ≥ 3 csPCa |
| Wiemer 2021 [14] | February-December 2018 | 159 | Prospective Paired Diagnostic | 45% BN, 29% AS | Patient | mpMRI and micro-US fusion superior modality; suggests elimination of systematic biopsy |
| Ghai 2022 [27] | May 2019–September 2020 | 94 | Prospective Paired Diagnostic | 100% BN | Patient | Comparable mpMRI and micro-US csPCa detection rates, with mpMRI preventing more biopsies; no added value of systematic biopsy to mpMRI/micro-US fusion |
| Hofbauer 2022 [28] | January–December 2019 | 203 | Prospective Multicenter Paired Diagnostic | 72% BN | Patient | Micro-US discovered 97% of csPCa detected by mpMRI; micro-US non-inferior to mpMRI |
| You 2022 [29] | NA * | 1081 | Systematic Review/Meta-Analysis | Unspecified | Patient | No significant differences in mpMRI and micro-US for detection of GG = 1, GG ≥ 2, or GG ≥ 3 csPCa |
| Cotter 2023 [30] | NA * | 1759 | Systematic Review/Meta-Analysis | 0% AS, Unknown BN | Patient | No statistically significant difference in sensitivity or specificity between micro-US and mpMRI |
| Dariane 2023 [31] | NA * | 2967 | Systematic Review/Meta-Analysis | Unspecified | Patient | Micro-US outperforms systematic biopsy with higher detection of csPCa and lower non-clinically significant PCa |
| Rojo 2024 [32] | May 2021–June 2022 | 80 | Prospective Multicenter Paired Diagnostic | 0% AS, Unknown BN | Patient | No significant difference between micro-US and mpMRI detected |
| Zhou 2024 [33] | 2022–2023 | 56 Patients | Prospective Collection w/Retrospective Diagnostic Validation | 74% BN, 21% AS | Lesion | All six urologists agreed on lesion only 33% of the time; lowest sensitivity and agreement found with anterior prostate lesions |
| Kinnaird (OPTIMUM) 2025 [12] | December 2021–September 2024 | 678 | Prospective Multicenter RCT | 100% BN | Patient | Solo micro-US, mpMRI and micro-US fusion, and conventional mpMRI fusion all non-inferior for csPCa detection; solo systematic biopsy was inferior to all modalities for detection of csPCa |
| Study | N | Definition of csPCa | Sensitivity | Specificity | PPV | NPV | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| MRI | TRUS | MRI | TRUS | MRI | TRUS | MRI | TRUS | |||
| PROMIS (2017) [4] | 576 | GG ≥ 3 or cancer core length ≥6 mm | 93% * | 48% | 41% | 96% * | 51% | 90% * | 89% * | 74% |
| GG ≥ 2 or cancer core length ≥4 mm | 87% * | 60% | 47% | 98% * | 69% | 98% * | 72% * | 65% | ||
| GG ≥ 2 | 88% * | 48% | 45% | 99% * | 65% | 99% * | 76% * | 63% | ||
| csPCa Detection Rate | GG1PCa DR | |||||||||
| MRI | TRUS | MRI | TRUS | |||||||
| PRECISION (2018) [41] | 500 | GG ≥ 2 | 38% * | 26% | 9% * | 22% | – | – | – | – |
| Van der Leest (2019) [42] | 626 | GG ≥ 2 | 25% | 23% | 14% | 25% * | – | – | – | – |
| MRI-FIRST (2019) [43] | 251 | GG ≥ 2 | 32% | 30% | 6% | 20% * | – | – | – | – |
| Study | N | Population (BN = Biopsy-Naïve, AS= Active Surveillance) | csPCa Detection Rate | Any PCa DR | Sensitivity | NPV | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Micro | Conv | Micro | Conv | Micro | Conv | Micro | Conv | |||
| Pavlovich (2014) [13] | 69 | 100% Biopsy-Proven PCa | 65% | 38% | – | – | 65% | 38% | 71% | 55% |
| Eure (2019) [17] | 9 | 100% Active Surveillance | 33% | 11% | 78% | 22% | 56–89% | 11% | 96–98% | 93% |
| Abouassaly (2020) [19] | 67 | 72% Biopsy-Naïve | 57% | 45% | – | – | – | – | – | – |
| Claros (2020) [20] | 222 | 26% Biopsy-Naïve | 40% | 32% | 68% | 64% | – | – | – | – |
| Pavlovich (2021) [25] | 1676 | 0% AS, Unknown BN | 35% | 37% | 50% | 54% | 61% | 38% | 92% | 92% |
| Study | N | Total Confirmed csPCa | Estimated Cores Taken Per Patient | Concordant Micro-US and mpMRI PCa | No. of Discordant csPCa Lesions or Cases | Confirmed csPCa Lesions or Cases among Discordant Targets | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Targeted | Systematic | Micro | mpMRI | Micro | mpMRI | SB | ||||
| Cornud (2020) [21] | 144 Lesions | 74 | – | – | 79% (114/144) | 17 | 13 | 4 | 0 | – |
| Lughezzani (2021) [15] | 320 Patients | 116 | 4 | 9 | 74% (189/255) | 20 | 14 | 3 | 3 | 12 |
| Wiemer (2021) [14] | 159 Patients | 78 | 8 | 8 | 44% (32/72) | 27 | 13 | 20 | 1 | 3 |
| Micro-US Study | Study Design | No. Subjects Enrolled | No. Centers | Key Findings |
|---|---|---|---|---|
| Klotz (2021) [24] | Prospective Paired Diagnostic | 1040 | 11 | Micro-US sensitivity superior and specificity non-inferior to mpMRI |
| Hofbauer (2022) [28] | Prospective Paired Diagnostic | 203 | 3 | Micro-US non-inferior to mpMRI for detection of csPCa |
| Rojo (2024) [32] | Prospective Paired Diagnostic | 80 | 4 * | No differences in csPCa detection found between micro-US and mpMRI |
| Kinnaird (OPTIMUM) (2025) [12] | RCT | 802 | 20 | Micro-US non-inferior to mpMRI for detection of csPCa |
| Study | No. of Studies | No. of Patients | Micro-US: mpMRI csPCa Detection Ratio | Micro-US: mpMRI GG = 1 PCa Detection Ratio | ||
|---|---|---|---|---|---|---|
| Sountoulides (2021) [26] | 13 | 1125 | 1.05 (0.93–1.19) | 0.94 (0.73–1.22) | ||
| You (2022) * [29] | 11 | 1081 | 1.01 (0.83–1.22) | 0.92 (0.68–1.25) | ||
| csPCa Sensitivity | csPCa Specificity | |||||
| Micro | mpMRI | Micro | mpMRI | |||
| Cotter (2023) [30] | 12 | 1759 | 89% (83–93%) | 86% (73–93%) | 31% (23–40%) | 32% (18–50%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
DuBois, J.; Smani, S.; Golos, A.; Rivera Lopez, C.; Lokeshwar, S.D. Micro-Ultrasound in the Detection of Clinically Significant Prostate Cancer: A Comprehensive Review and Comparison with Multiparametric MRI. Tomography 2025, 11, 80. https://doi.org/10.3390/tomography11070080
DuBois J, Smani S, Golos A, Rivera Lopez C, Lokeshwar SD. Micro-Ultrasound in the Detection of Clinically Significant Prostate Cancer: A Comprehensive Review and Comparison with Multiparametric MRI. Tomography. 2025; 11(7):80. https://doi.org/10.3390/tomography11070080
Chicago/Turabian StyleDuBois, Julien, Shayan Smani, Aleksandra Golos, Carlos Rivera Lopez, and Soum D. Lokeshwar. 2025. "Micro-Ultrasound in the Detection of Clinically Significant Prostate Cancer: A Comprehensive Review and Comparison with Multiparametric MRI" Tomography 11, no. 7: 80. https://doi.org/10.3390/tomography11070080
APA StyleDuBois, J., Smani, S., Golos, A., Rivera Lopez, C., & Lokeshwar, S. D. (2025). Micro-Ultrasound in the Detection of Clinically Significant Prostate Cancer: A Comprehensive Review and Comparison with Multiparametric MRI. Tomography, 11(7), 80. https://doi.org/10.3390/tomography11070080