
Diagnostic Sensitivity of the Revised Venous System in Brain Death in Children

 , , , , , , and
, , , , , , and
Abstract
1. Introduction
2. Methods
2.1. Study Population
2.2. Preliminary Anatomical Study of Infratentorial Veins in Children
2.3. Imaging Acquisition
2.4. Image Interpretation
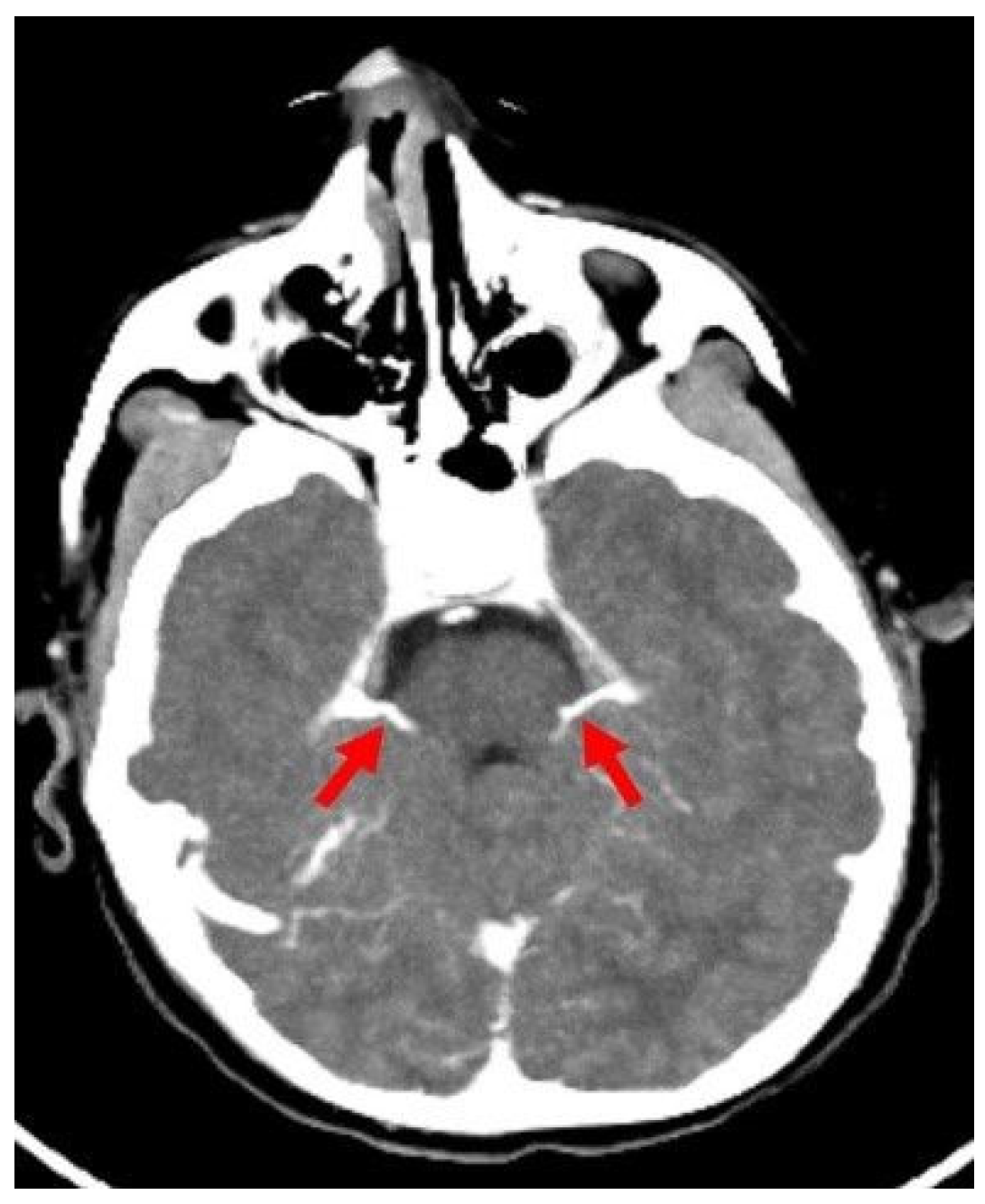
- A60-V60: Absence of opacification in M4 branches of the middle cerebral arteries (MCAs) and ICVs in the venous phase, based on the reference 4-point system by Frampas et al. [11].
- A20-V60: Absence of opacification in M4 branches of the MCAs in the arterial phase and ICVs in the venous phase, based on the revised arteriovenous scoring system by Nunes et al. [12].
- ICV-SPV: Absence of opacification in the ICVs and SPVs in the venous phase, based on the revised venous scoring system by Marchand et al. [10].
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Greer, D.M.; Kirschen, M.P.; Lewis, A.; Gronseth, G.S.; Rae-Grant, A.; Ashwal, S.; Babu, M.A.; Bauer, D.F.; Billinghurst, L.; Corey, A.; et al. Pediatric and Adult Brain Death/Death by Neurologic Criteria Consensus Guideline. Neurology 2023, 101, 1112–1132. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, T.A.; Ashwal, S.; Mathur, M.; Mysore, M.R.; Bruce, D.; Conway, E.E., Jr.; Duthie, S.E.; Hamrick, S.; Harrison, R.; Kline, A.M.; et al. Guidelines for the determination of brain death in infants and children: An update of the 1987 Task Force recommendations. Crit. Care Med. 2011, 39, 2139–2155. [Google Scholar] [CrossRef] [PubMed]
- Beecher, H.K. A definition of irreversible coma: Report of the ad hoc Committee of the Harvard Medical School to examine the definition of brain death. JAMA 1968, 205, 337–340. [Google Scholar] [CrossRef]
- McKinnon, N.K.; Maratta, C.; Zuckier, L.S.; Boyd, J.G.; Chassé, M.; Hornby, L.; Kramer, A.; Kromm, J.; Mooney, O.T.; Muthusami, P.; et al. Ancillary investigations for death determination in infants and children: A systematic review and meta-analysis. Can. J. Anaesth. 2023, 70, 749–770. [Google Scholar] [CrossRef]
- Hwang, D.Y.; Gilmore, E.J.; Greer, D.M. Assessment of brain death in the neurocritical care unit. Neurosurg. Clin. N. Am. 2013, 24, 469–482. [Google Scholar] [CrossRef] [PubMed]
- Kirschen, M.P.; Lewis, A.; Greer, D.M. The 2023 American Academy of Neurology, American Academy of Pediatrics, Child Neurology Society, and Society of Critical Care Medicine Pediatric and Adult Brain Death/Death by Neurologic Criteria Determination Consensus Guidelines: What the Critical Care Team Needs to Know. Crit. Care Med. 2024, 52, 376–386. [Google Scholar]
- Natalie, H.; McDonald, M.J. Ancillary studies in evaluating pediatric brain death. J. Pediatr. Intensive Care 2017, 6, 234–239. [Google Scholar]
- Garrett, M.P.; Williamson, R.W.; Bohl, M.A.; Bird, C.R.; Theodore, N. Computed tomography angiography as a confirmatory test for the diagnosis of brain death. J. Neurosurg. 2018, 128, 639–649. [Google Scholar] [CrossRef]
- Wahlster, S.; Wijdicks, E.F.M.; Patel, P.V.; Greer, D.M.; Hemphill, J.C., 3rd; Carone, M.; Mateen, F.J. Brain death declaration: Practices and perceptions worldwide. Neurology 2015, 84, 1870–1879. [Google Scholar] [CrossRef]
- Marchand, A.J.; Seguin, P.; Malledant, Y.; Taleb, M.; Raoult, H.; Gauvrit, J.Y. Revised CT angiography venous score with consideration of infratentorial circulation value for diagnosing brain death. Ann. Intensive Care 2016, 6, 88. [Google Scholar] [CrossRef]
- Frampas, E.; Videcoq, M.; de Kerviler, E.; Ricolfi, F.; Kuoch, V.; Mourey, F.; Tenaillon, A.; Dupas, B. CT angiography for brain death diagnosis. AJNR Am. J. Neuroradiol. 2009, 30, 1566–1570. [Google Scholar] [CrossRef] [PubMed]
- Nunes, D.M.; Maia, A.C.M., Jr.; Boni, R.C.; da Rocha, A.J. Impact of skull defects on the role of CTA for brain death confirmation. AJNR Am. J. Neuroradiol. 2019, 40, 1177–1183. [Google Scholar] [CrossRef] [PubMed]
- Akdogan, A.I.; Pekcevik, Y.; Sahin, H.; Pekcevik, R. Assessment of cerebral circulatory arrest via CT angiography and CT perfusion in brain death confirmation. Korean J. Radiol. 2021, 22, 395–404. [Google Scholar] [CrossRef]
- Berenguer, C.M.; Davis, F.E.; Howington, J.U. Brain death confirmation: Comparison of computed tomographic angiography with nuclear medicine perfusion scan. J. Trauma 2012, 68, 553–559. [Google Scholar] [CrossRef]
- Shankar, J.; Vandorpe, R. CT perfusion for confirmation of brain death. AJNR Am. J. Neuroradiol. 2013, 34, 1175–1179. [Google Scholar] [CrossRef]
- Hoffmann, O.; Salih, F.; Masuhr, F. Computed tomography angiography in the diagnosis of brain death: Implementation and results in Germany. Eur. J. Neurol. 2024, 31, e16209. [Google Scholar] [CrossRef]
- Sundaram, R.; Rooney, K.; Koteeswaran, S.K. The use of cerebral CT angiography as an ancillary investigation to support a clinical diagnosis of death using neurological criteria. Anaesthesia 2024, 79, 321. [Google Scholar] [CrossRef] [PubMed]
- Aziz Rizk, A.; Shankar, J. Computed Tomography Angiography as Ancillary Testing for Death Determination by Neurologic Criteria: A Technical Review. Tomography 2024, 10, 1139–1147. [Google Scholar] [CrossRef]
- Almus, E.; Bıyıklı, E.; Yapıcı, Ö.; Almus, F.; Girgin, F.İ.; Öztürk, N. Brain death in children: Is computed tomography angiography reliable as an ancillary test? Pediatr. Radiol. 2023, 53, 131–141. [Google Scholar] [CrossRef]
- Şahin, H.; Pekçevik, Y. CT angiography as a confirmatory test in diagnosis of brain death: Comparison between three scoring systems. Diagn. Interv. Radiol. 2015, 21, 177. [Google Scholar] [CrossRef]
- Sawicki, M.; Bohatyrewicz, R.; Safranow, K.; Walecka, A.; Walecki, J.; Rowinski, O.; Solek-Pastuszka, J.; Czajkowski, Z.; Guzinski, M.; Burzynska, M.; et al. Computed tomographic angiography criteria in the diagnosis of brain death—Comparison of sensitivity and interobserver reliability of different evaluation scales. Neuroradiology 2014, 56, 609–620. [Google Scholar] [CrossRef] [PubMed]
- Welschehold, S.; Kerz, T.; Boor, S.; Reuland, K.; Thömke, F.; Reuland, A.; Beyer, C.; Wagner, W.; Müller-Forell, W.; Giese, A. Detection of intracranial circulatory arrest in brain death using cranial CT-angiography. Eur. J. Neurol. 2013, 20, 173–179. [Google Scholar] [CrossRef] [PubMed]
- Srairi, M.; Meluchova, Z.; Paoletti, M.; Ahmad, M.; Abaziou, T.; Atthar, V.; Gilles Georget, G.; Mrozek, S.; Larcher, C.; Osinski, D.; et al. Diagnostic accuracy of a revised computed tomography angiography score for brain death confirmation, combining supra-tentorial arteries and infratentorial veins. Eur. J. Radiol. 2020, 130, 109132. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Number (%) |
|---|---|
| Sex | |
| Male | 30 (69.8) |
| Female | 13 (30.2) |
| Etiology of brain death | |
| Trauma | 12 (27.9) |
| Cardiac arrest | 12 (27.9) |
| Asphyxia | 9 (20.9) |
| İnfection | 5 (11.6) |
| İntoxication | 2 (4.7) |
| Metabolic disease | 2 (4.7) |
| Terminal stage tumor | 1 (2.3) |
| Variable | n/% |
|---|---|
| Open Fontanel | 12 (27.9) |
| Craniectomy | 2 (4.7) |
| Fracture | 5 (11.6) |
| Shunt | 5 (11.6) |
| Variable | n/% |
|---|---|
| DCE + TH | 40 (93) |
| SAH | 6 (13) |
| IVH | 10 (23.3) |
| Scoring System | Agreement for Diagnosis of Brain Death | |
|---|---|---|
| κ | % | |
| A20-V60 | 0.909 | 97.6 |
| A60-V60 | 0.927 | 95.3 |
| ICV-SPV | 0.876 | 93.0 |
| OS | 29 d < 1 y (n:8) | 1–6 y (n:6) | >6 y (n:22) | |
|---|---|---|---|---|
| CTA (%) | ||||
| A20-V60 | 86.0 | 95.5 | 84.6 | 81.8 |
| A60-V60 | 79.1 | 87.5 | 92.3 | 81.8 |
| ICV-SPV | 88.4 | 87.5 | 84.6 | 86.3 |
| OSD+ | OSD− | p | |
|---|---|---|---|
| CTA (%) | |||
| A20-V60 | 84.2 | 87.1 | 1.0 |
| A60-V60 | 68.4 | 86.2 | 0.477 |
| ICV-SPV | 89.5 | 87.8 | 1.0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Çinar, H.G.; Ucan, B.; Bulut, H.; Yılmaz, Ş.; Göncü, S.; Gün, E.; Özbudak, P.; Üstün, C.; Üner, Ç. Diagnostic Sensitivity of the Revised Venous System in Brain Death in Children. Tomography 2025, 11, 30. https://doi.org/10.3390/tomography11030030
Çinar HG, Ucan B, Bulut H, Yılmaz Ş, Göncü S, Gün E, Özbudak P, Üstün C, Üner Ç. Diagnostic Sensitivity of the Revised Venous System in Brain Death in Children. Tomography. 2025; 11(3):30. https://doi.org/10.3390/tomography11030030
Chicago/Turabian StyleÇinar, Hasibe Gökçe, Berna Ucan, Hasan Bulut, Şükriye Yılmaz, Sultan Göncü, Emrah Gün, Pınar Özbudak, Canan Üstün, and Çiğdem Üner. 2025. "Diagnostic Sensitivity of the Revised Venous System in Brain Death in Children" Tomography 11, no. 3: 30. https://doi.org/10.3390/tomography11030030
APA StyleÇinar, H. G., Ucan, B., Bulut, H., Yılmaz, Ş., Göncü, S., Gün, E., Özbudak, P., Üstün, C., & Üner, Ç. (2025). Diagnostic Sensitivity of the Revised Venous System in Brain Death in Children. Tomography, 11(3), 30. https://doi.org/10.3390/tomography11030030