

A Novel Method for the Generation of Realistic Lung Nodules Visualized Under X-Ray Imaging

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
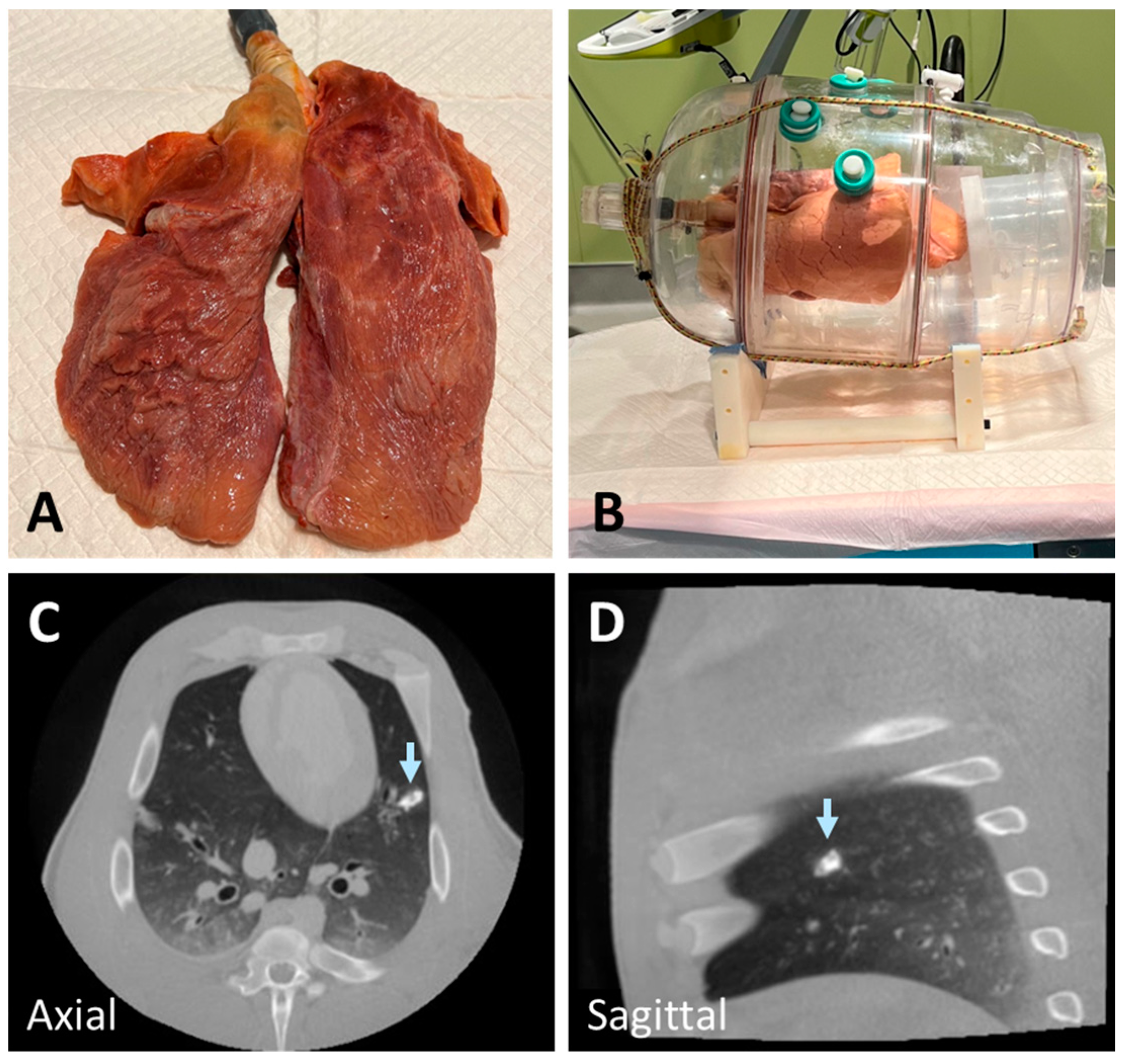
2.1. Ex Vivo Swine Lungs
2.2. Post-Mortem Swine Lungs
2.3. Lung Nodule Preparation and Injection
2.4. Imaging Protocol
3. Results
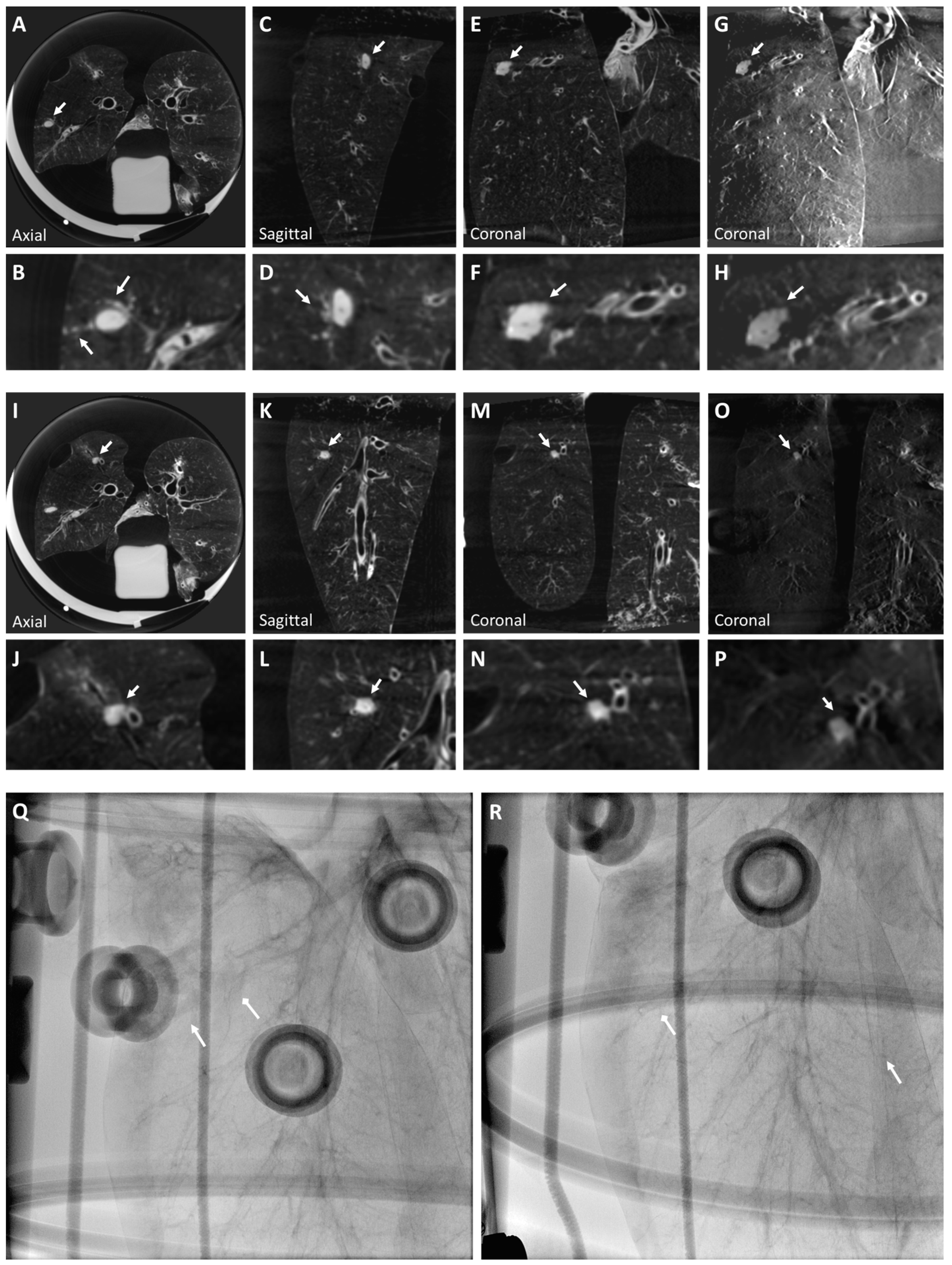
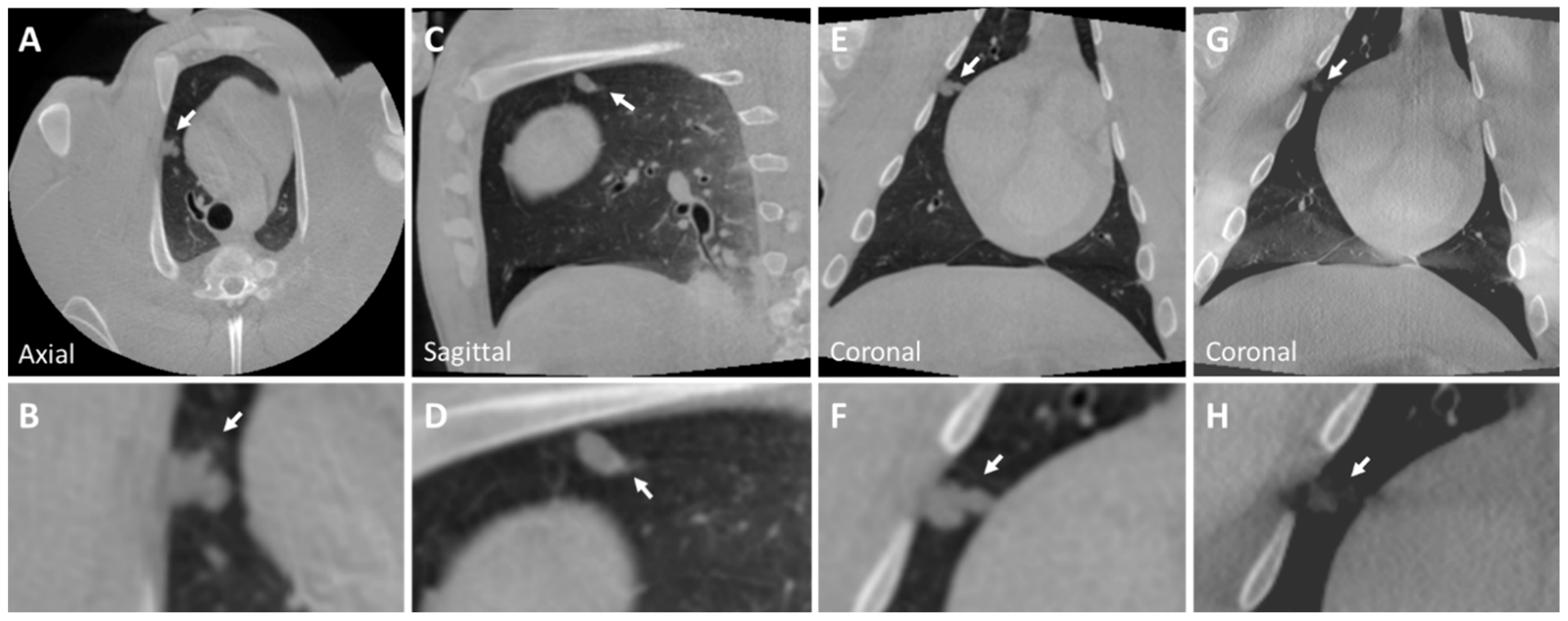
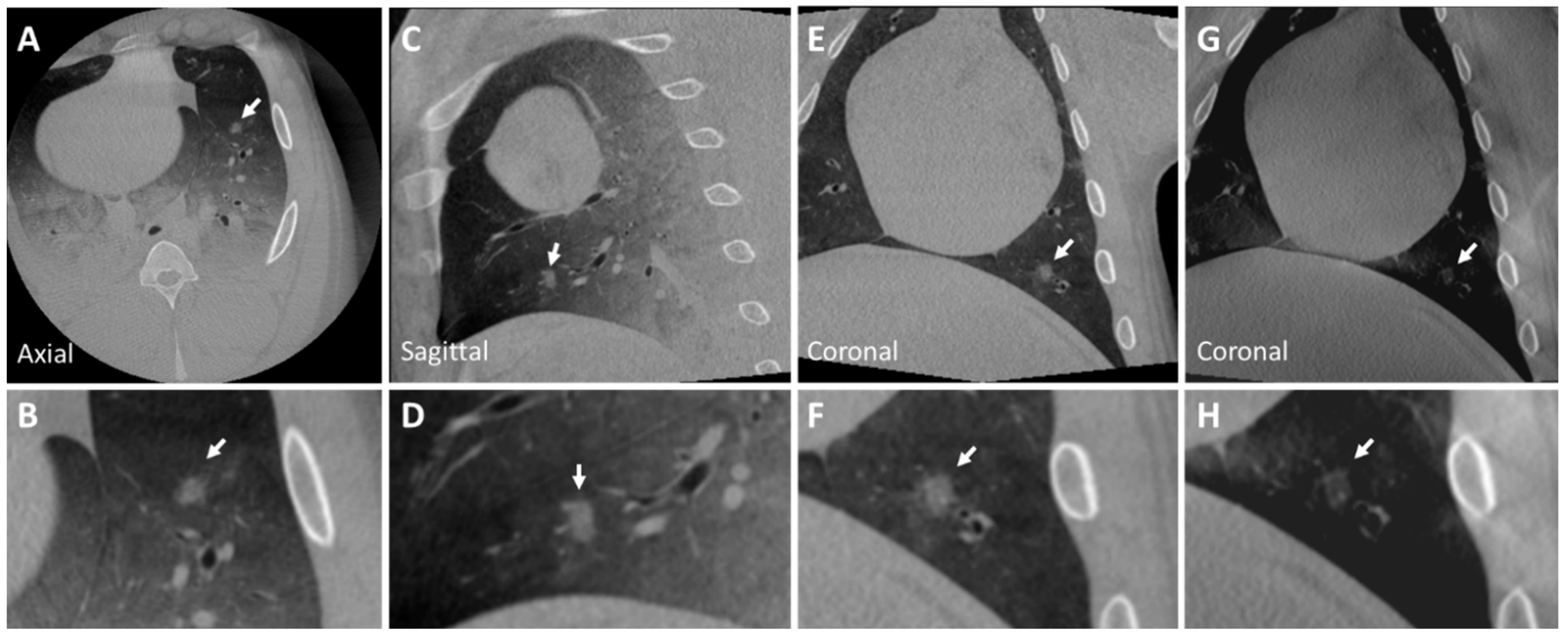
3.1. Ex Vivo Swine Lungs
3.2. Post-Mortem Swine Lungs
3.3. Recommendations
- ➢
- Pre-procedure preparation:
- Inflate the phantom lungs before injecting materials.
- Flush needles with a 5% dextrose solution to prevent premature polymerization of n-BCA.
- ➢
- Mixing the Material:
- Manual mixing is sufficient to create a realistic lesion that is not fully homogeneous.
- For a homogeneous lesion, thoroughly mix the n-BCA and ethiodized oil using a shaker.
- ➢
- Mixture for Solid Nodule:
- Use 1 g of n-BCA and 10 mcg of ethiodized oil.
- ➢
- Mixture for Ground Glass Nodule:
- Use 1 g of n-BCA.
- ➢
- Creating the Nodule:
- Inject slowly and steadily, completing the injection within 10 s.
- ➢
- Creating Pleural Extension:
- Inject half of the material slowly and steadily for over 5 s.
- Inject the remaining half slowly while retracting the needle, completing the injection over another 5 s until reaching the pleura.
- ➢
- Obtaining a Lobulated Contour Nodule:
- Move the needle tip in very small forward–backward and up–down motions (no more than 5 mm) during the injection.
- ➢
- Creating Spiculation (Malignant Nodule Characteristic):
- Inject half of the material slowly for over 5 s.
- Inject the remaining portion rapidly in a single burst.
- ➢
- Preventing Pneumothorax:
- Retract the needle while injecting a small amount of material (approximately 0.1 cc) until the needle detaches from the pleura.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Aberle, D.R.; Adams, A.M.; Berg, C.D.; Black, W.C.; Clapp, J.D.; Fagerstrom, R.M.; Gareen, I.F.; Gatsonis, C.; Marcus, P.M.; Sicks, J.D. Reduced lung-cancer mortality with low-dose computed tomographic screening. N. Engl. J. Med. 2011, 365, 395–409. [Google Scholar]
- de Koning, H.J.; van der Aalst, C.M.; de Jong, P.A.; Scholten, E.T.; Nackaerts, K.; Heuvelmans, M.A.; Prokop, M.; Weenink, C.; Groen, H.J.M.; Lammers, J.W.J.; et al. Reduced Lung-Cancer Mortality with Volume CT Screening in a Randomized Trial. N. Engl. J. Med. 2020, 382, 503–513. [Google Scholar] [CrossRef] [PubMed]
- Gould, M.K.; Tang, T.; Liu, I.L.; Lee, J.; Zheng, C.; Danforth, K.N.; Kosco, A.E.; Smith, S.; Brown, K.; Greathouse, K.; et al. Recent Trends in the Identification of Incidental Pulmonary Nodules. Am. J. Respir. Crit. Care Med. 2015, 192, 1208–1214. [Google Scholar] [CrossRef]
- Schaefer, P.J.; Fabel, M.; Bolte, H.; Schaefer, F.K.; Jahnke, T.; Heller, M.; Felix, R.; Peters, P.E.; Meyer, J.; Braun, D.; et al. CT fluoroscopy-guided lung biopsy with novel steerable biopsy canula: Ex-vivo evaluation in ventilated porcine lung explants. Cardiovasc. Intervent. Radiol. 2010, 33, 828–834. [Google Scholar] [CrossRef]
- Chen, A.C.; Pastis, N.J.; Machuzak, M.S.; Gildea, T.R.; Simoff, M.J.; Gillespie, C.T.; Kwiatkowski, D.; Patel, S.; Anderson, S.; Bar-Shalom, R.; et al. Accuracy of a Robotic Endoscopic System in Cadaver Models with Simulated Tumor Targets: ACCESS Study. Respiration 2020, 99, 56–61. [Google Scholar] [CrossRef]
- de Ruiter, Q.M.B.; Karanian, J.W.; Bakhutashvili, I.; Esparza-Trujillo, J.A.; Varble, N.A.; van der Sterren, W.; van der Molen, A.J.; Kooijman, N.; Hooft, L.; Krestin, G.P.; et al. Endobronchial Navigation Guided by Cone-Beam CT-Based Augmented Fluoroscopy without a Bronchoscope: Feasibility Study in Phantom and Swine. J. Vasc. Interv. Radiol. 2020, 31, 2122–2131. [Google Scholar] [CrossRef]
- Jin, K.N.; Lee, K.W.; Kim, T.J.; Song, Y.S.; Kim, D.I. Computed tomography guided percutaneous injection of a mixture of lipiodol and methylene blue in rabbit lungs: Evaluation of localization ability for video-assisted thoracoscopic surgery. J. Korean Med. Sci. 2014, 29, 129–136. [Google Scholar] [CrossRef]
- Jackson, P.; Steinfort, D.P.; Kron, T.; Siva, S. Practical Assessment of Bronchoscopically Inserted Fiducial Markers for Image Guidance in Stereotactic Lung Radiotherapy. J. Thorac. Oncol. 2016, 11, 1363–1368. [Google Scholar] [CrossRef]
- Bhagat, N.; Fidelman, N.; Durack, J.C.; Thomas, D.; Gupta, A.; Chang, A.; Hartman, C.; Balthazar, M.; Tsai, P.; Pasternack, M.; et al. Complications associated with the percutaneous insertion of fiducial markers in the thorax. Cardiovasc. Intervent. Radiol. 2010, 33, 1186–1191. [Google Scholar] [CrossRef]
- Markelj, P.; Tomaževič, D.; Likar, B.; Pernuš, F. A review of 3D/2D registration methods for image-guided interventions. Med. Image Anal. 2012, 16, 642–661. [Google Scholar] [CrossRef] [PubMed]
- Yabo, F.; Yang, L.; Tonghe, W.; Walter, J.C.; Tian, L.; Xiaofeng, Y. Deep learning in medical image registration: A review. Phys. Med. Biol. 2020, 65, 20TR01. [Google Scholar]
- Setser, R.; Chintalapani, G.; Bhadra, K.; Casal, R.F. Cone beam CT imaging for bronchoscopy: A technical review. J. Thorac. Dis. 2020, 12, 7416–7428. [Google Scholar] [CrossRef] [PubMed]
- Silvestri, G.A.; Herth, F.J.; Keast, T.; Rai, L.; Gibbs, J.; Wibowo, H.; Berman, S.; D’Angelo, J.; Chiang, K.; Rajan, S.; et al. Feasibility and safety of bronchoscopic transparenchymal nodule access in canines: A new real-time image-guided approach to lung lesions. Chest 2014, 145, 833–838. [Google Scholar] [CrossRef]
- Nelson, G.; Wu, M.; Hinkel, C.; Krishna, G.; Funk, T.; Rosenberg, J.; Zhang, Y.; Li, Y.; Patel, S.; Wang, J.; et al. Improved targeting accuracy of lung tumor biopsies with scanning-beam digital X-ray tomosynthesis image guidance. Med. Phys. 2016, 43, 6282. [Google Scholar] [CrossRef]
- Bolte, H.; Riedel, C.; Muller-Hulsbeck, S.; Freitag-Wolf, S.; Kohl, G.; Drews, T.; Stoeckel, D.; Peters, P.; Langer, C.; Seidensticker, M.; et al. Precision of computer-aided volumetry of artificial small solid pulmonary nodules in ex vivo porcine lungs. Br. J. Radiol. 2007, 80, 414–421. [Google Scholar] [CrossRef]
- Sterman, D.H.; Keast, T.; Rai, L.; Gibbs, J.; Wibowo, H.; Draper, J.; Berman, S.; D’Angelo, J.; Chiang, K.; Rajan, S.; et al. High yield of bronchoscopic transparenchymal nodule access real-time image-guided sampling in a novel model of small pulmonary nodules in canines. Chest 2015, 147, 700–707. [Google Scholar] [CrossRef]
- Chen, A.; Machuzak, M.; Edell, E.; Silvestri, G.A. Peripheral Bronchoscopy Training Using a Human Cadaveric Model and Simulated Tumor Targets. J. Bronchol. Interv. Pulmonol. 2016, 23, 83–86. [Google Scholar] [CrossRef]
- Brassel, F.; Meila, D. Evolution of Embolic Agents in Interventional Neuroradiology. Clin. Neuroradiol. 2015, 25 (Suppl. S2), 333–339. [Google Scholar] [CrossRef]
- Judge, E.P.; Hughes, J.M.; Egan, J.J.; Maguire, M.; Molloy, E.L.; O’Dea, S. Anatomy and bronchoscopy of the porcine lung. A model for translational respiratory medicine. Am. J. Respir. Cell Mol. Biol. 2014, 51, 334–343. [Google Scholar] [CrossRef]
- Swensen, S.J.; Viggiano, R.W.; Midthun, D.E.; Müller, N.L.; Sherrick, A.; Yamashita, K.; Naidich, D.P.; Patz, E.F.; Hartman, T.E.; Muhm, J.R.; et al. Lung nodule enhancement at CT: Multicenter study. Radiology 2000, 214, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Yangsean, C.; Gil, B.M.; Chung, M.H.; Yoo, W.J.; Jung, N.Y.; Kim, Y.H.; Kwon, S.S.; Kim, J. Comparing attenuations of malignant and benign solitary pulmonary nodule using semi-automated region of interest selection on contrast-enhanced CT. J. Thorac. Dis. 2019, 11, 2392–2401. [Google Scholar]
- Usui, T.; Macleod, M.R.; McCann, S.K.; Senior, A.M.; Nakagawa, S. Meta-analysis of variation suggests that embracing variability improves both replicability and generalizability in preclinical research. PLoS Biol. 2021, 19, e3001009. [Google Scholar] [CrossRef]
- Ko, M.J.; Lim, C.Y. General considerations for sample size estimation in animal study. Korean J. Anesthesiol. 2021, 74, 23–29. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Diameter (mm) | CT Attenuation (HU) | |
|---|---|---|
| Lung Nodule | <30 | 50 (30) |
| Ground Glass Nodule | <30 | −200–−500 |
| Nodule 1 | 11 × 6.5 | |
| Nodule 2 | 8 × 7 | −360 (±55) |
| Nodule 3 | 10 × 9 | 25 (20) |
| Nodule 4 | 9 × 8 | −330 (50) |
| Nodule 5 | 16 × 12 | −310 ( |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peker, A.; Sinha, A.; King, R.M.; Minnaard, J.; Sterren, W.v.d.; Bydlon, T.; Bankier, A.A.; Gounis, M.J. A Novel Method for the Generation of Realistic Lung Nodules Visualized Under X-Ray Imaging. Tomography 2024, 10, 1959-1969. https://doi.org/10.3390/tomography10120142
Peker A, Sinha A, King RM, Minnaard J, Sterren Wvd, Bydlon T, Bankier AA, Gounis MJ. A Novel Method for the Generation of Realistic Lung Nodules Visualized Under X-Ray Imaging. Tomography. 2024; 10(12):1959-1969. https://doi.org/10.3390/tomography10120142
Chicago/Turabian StylePeker, Ahmet, Ayushi Sinha, Robert M. King, Jeffrey Minnaard, William van der Sterren, Torre Bydlon, Alexander A. Bankier, and Matthew J. Gounis. 2024. "A Novel Method for the Generation of Realistic Lung Nodules Visualized Under X-Ray Imaging" Tomography 10, no. 12: 1959-1969. https://doi.org/10.3390/tomography10120142
APA StylePeker, A., Sinha, A., King, R. M., Minnaard, J., Sterren, W. v. d., Bydlon, T., Bankier, A. A., & Gounis, M. J. (2024). A Novel Method for the Generation of Realistic Lung Nodules Visualized Under X-Ray Imaging. Tomography, 10(12), 1959-1969. https://doi.org/10.3390/tomography10120142