
A Preliminary Study to Design and Evaluate Pneumatically Controlled Soft Robotic Actuators for a Repetitive Hand Rehabilitation Task

Abstract
1. Introduction
2. Materials and Methods
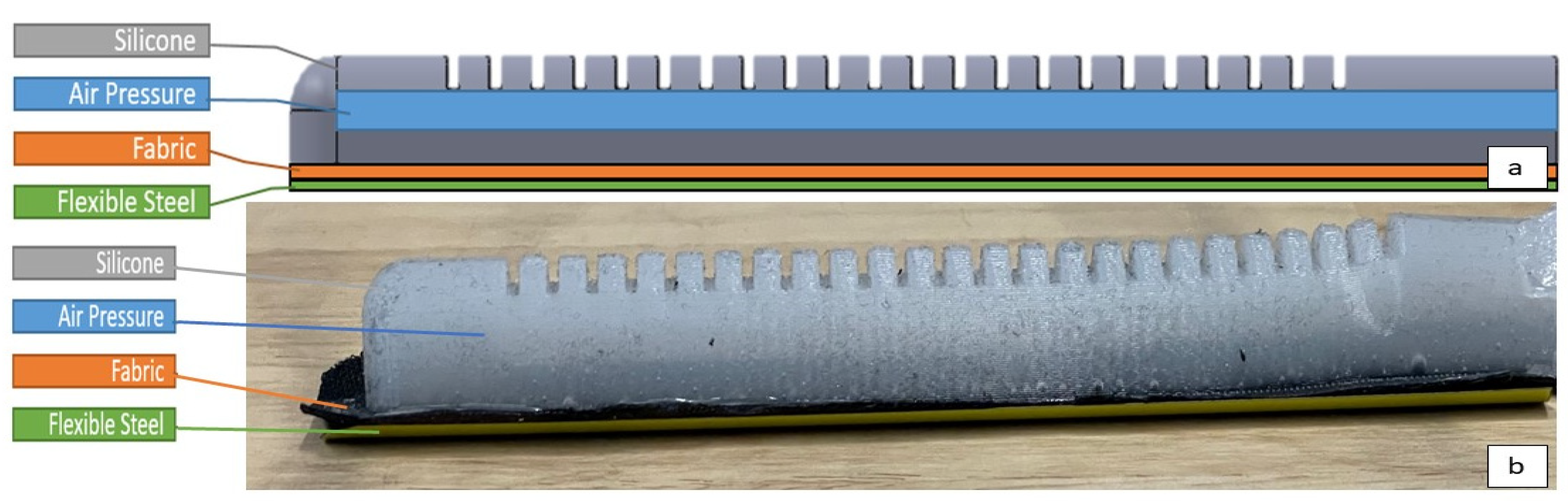
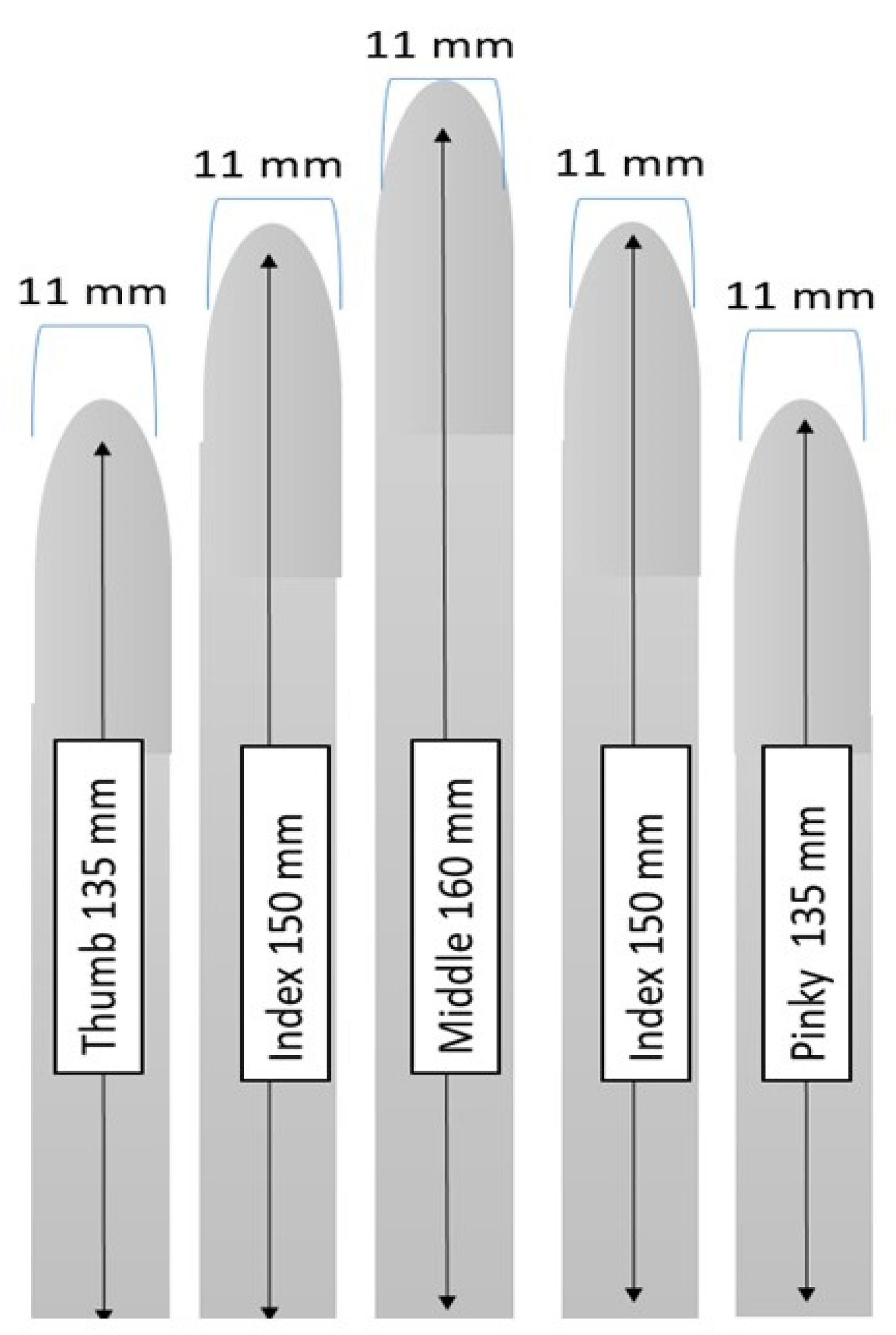
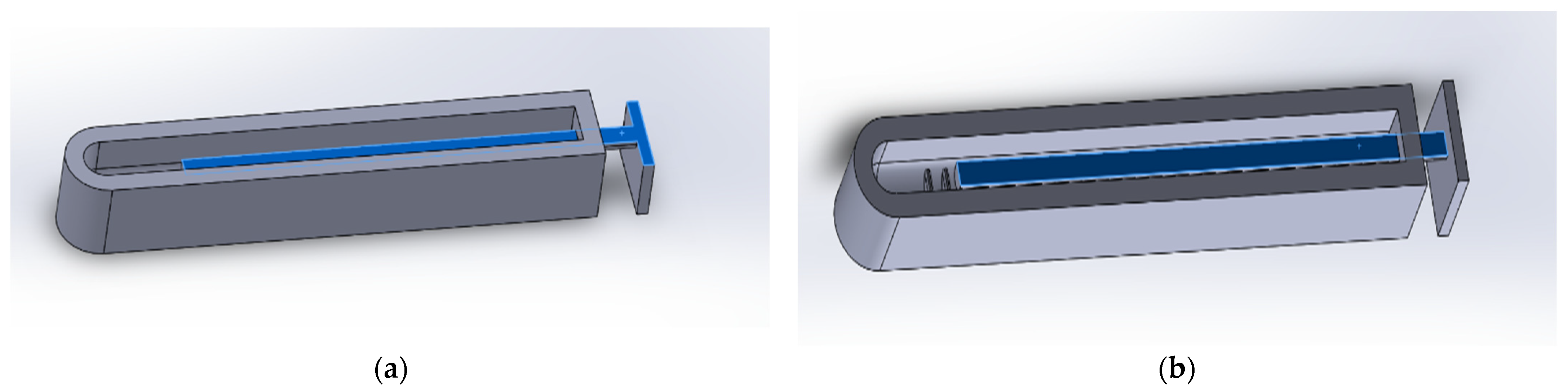
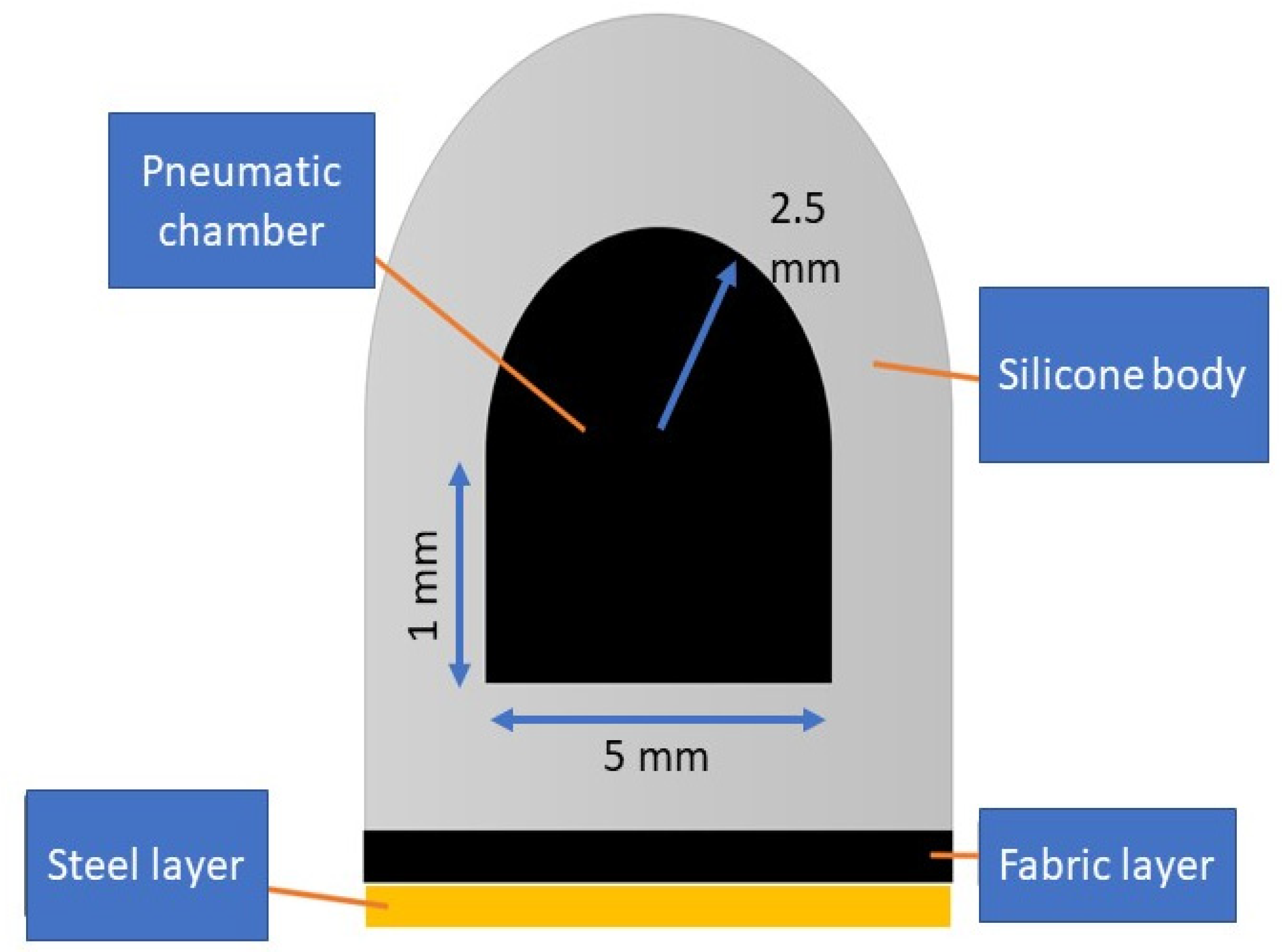
2.1. Soft Actuator Design and Fabrication
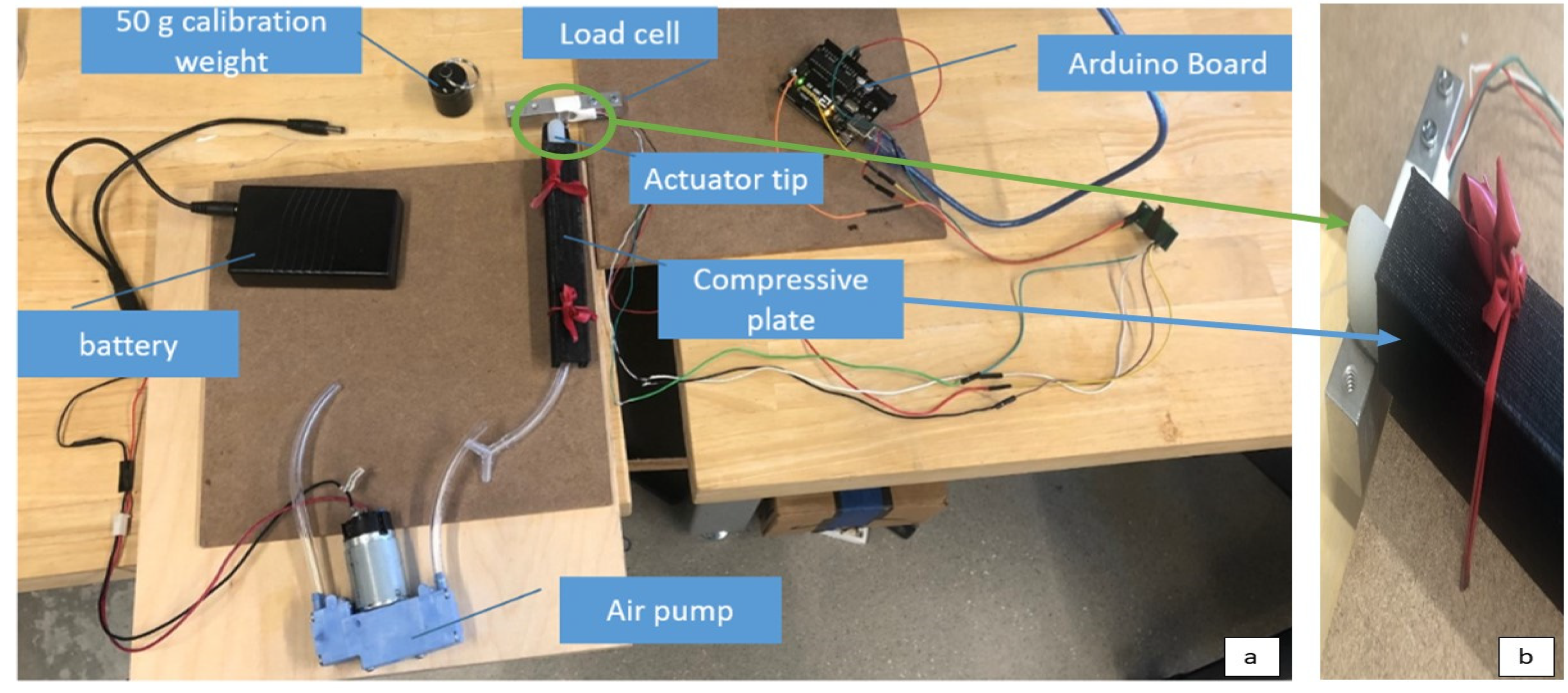
2.2. Blocked Tip Force Testing Setup
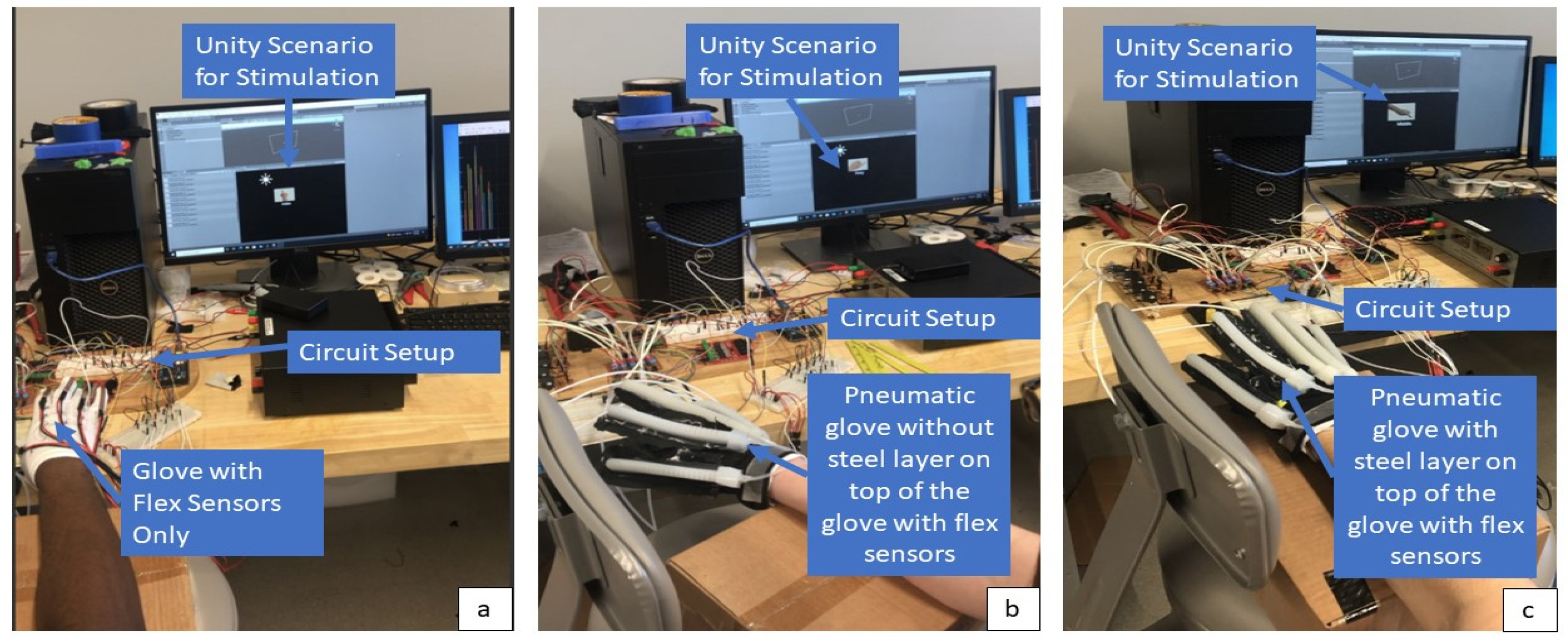
2.3. Human Subject Testing
3. Results
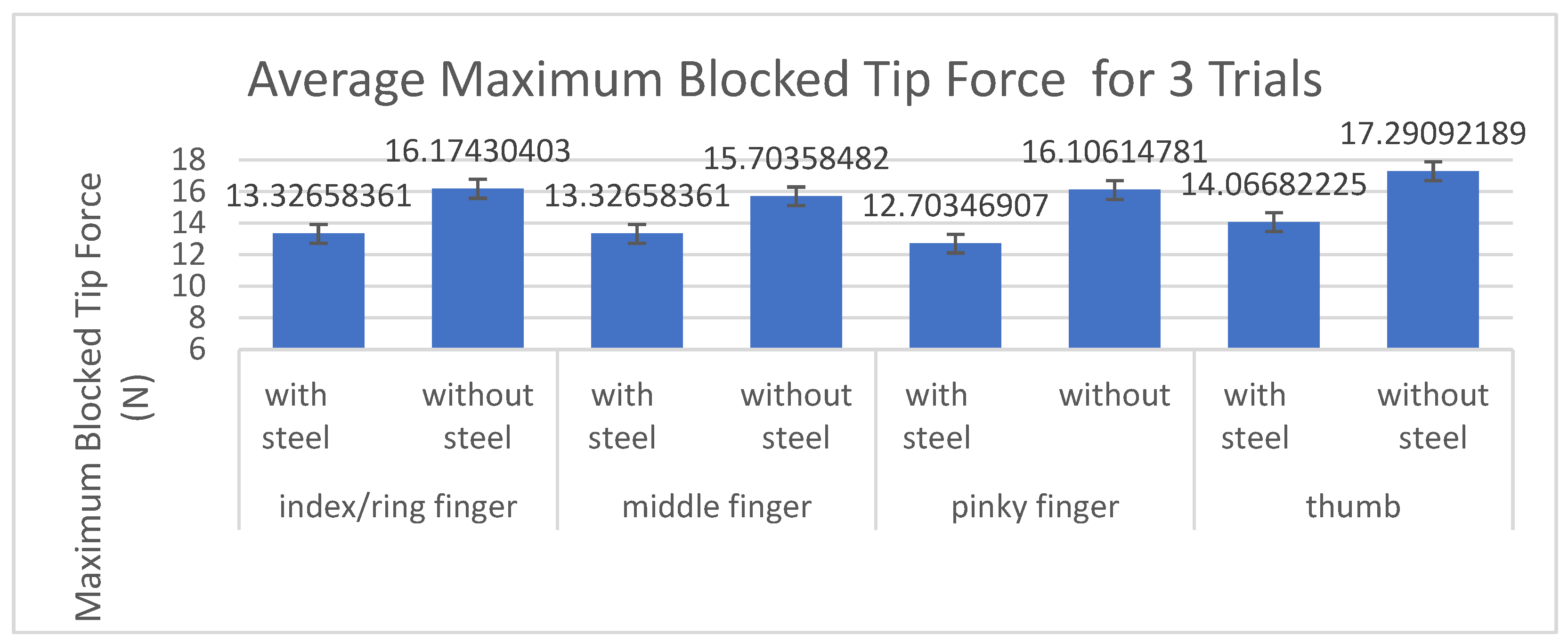
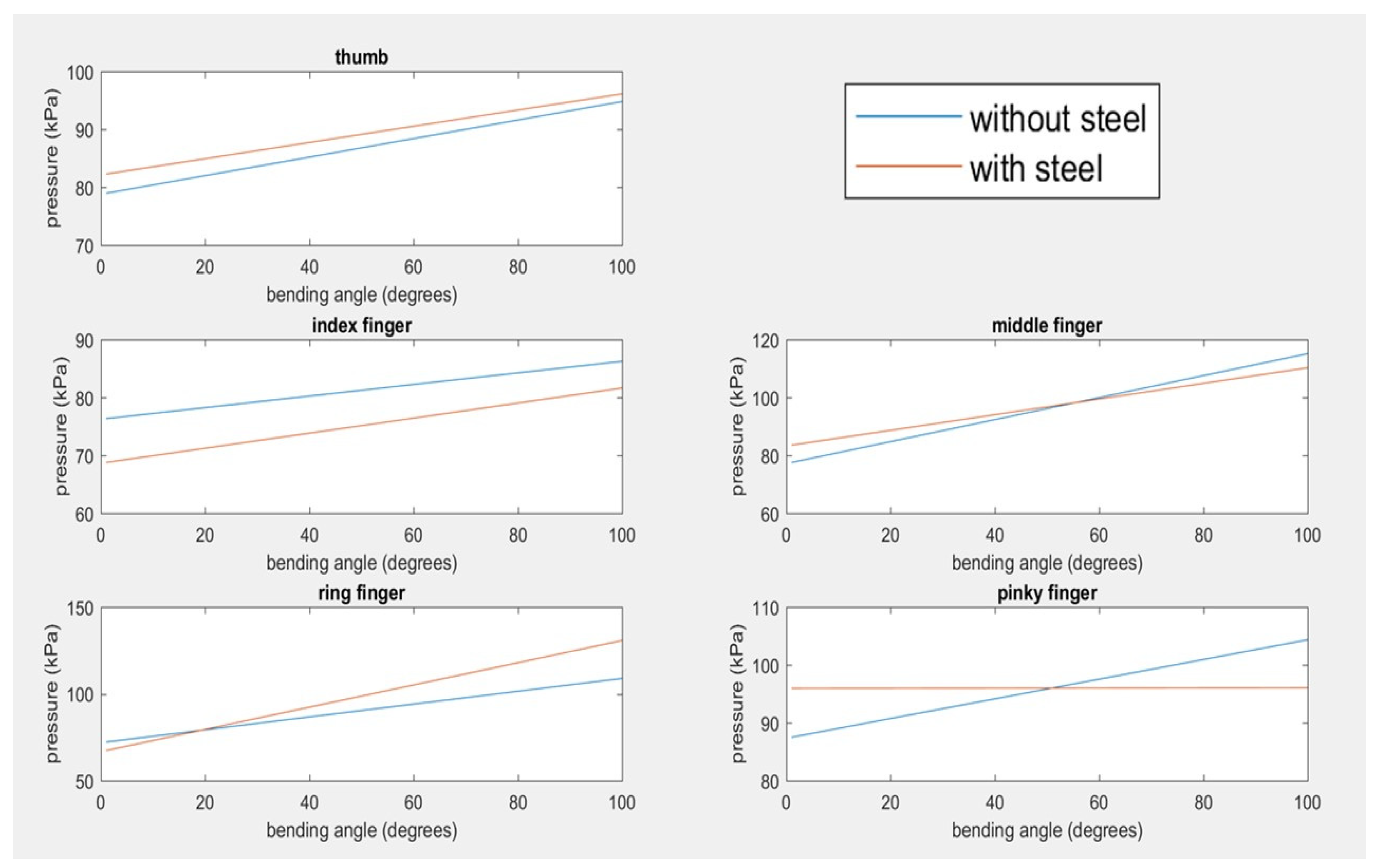
3.1. Blocked Tip Force Testing of Fabricated Soft Actuators
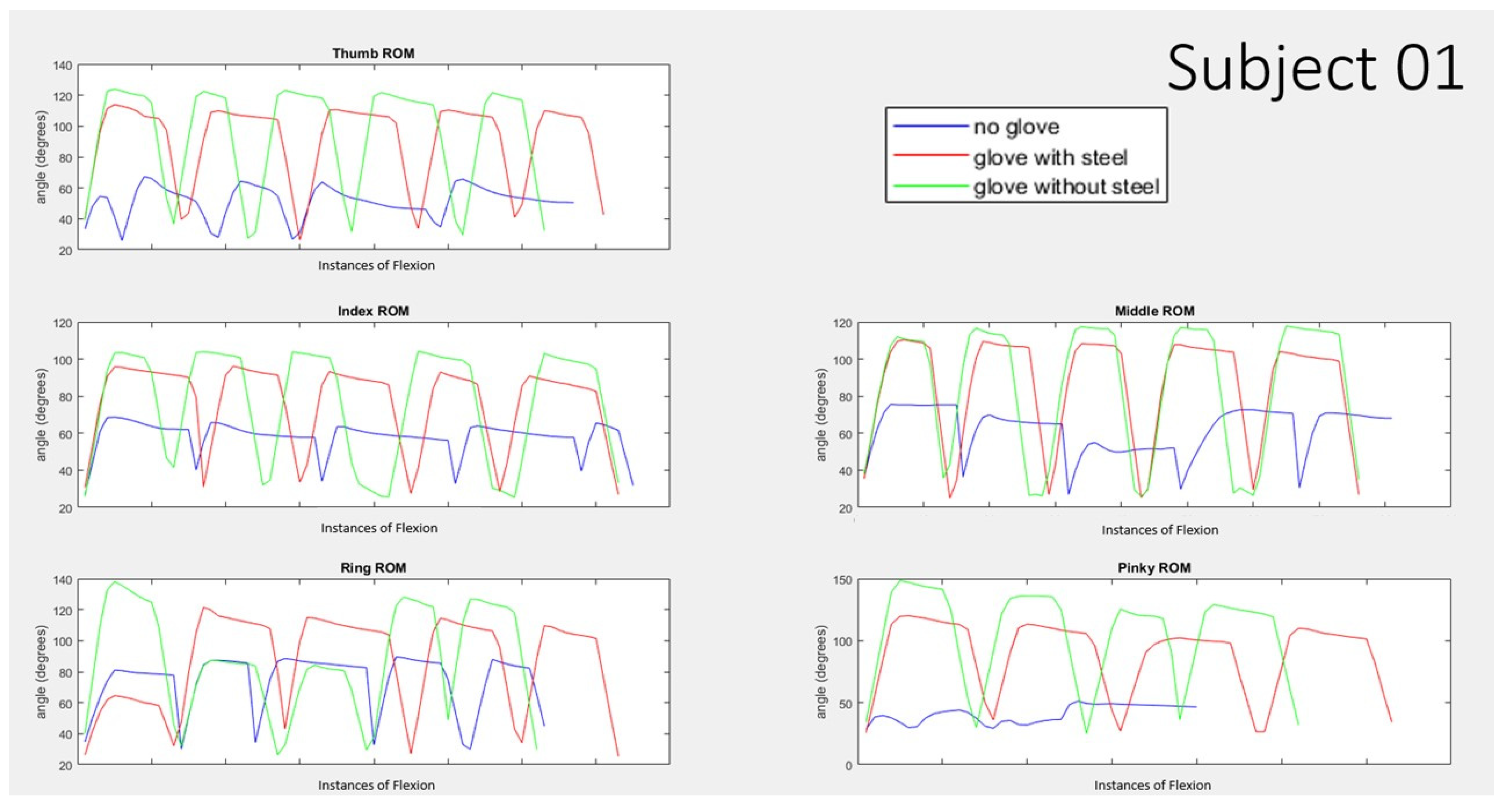
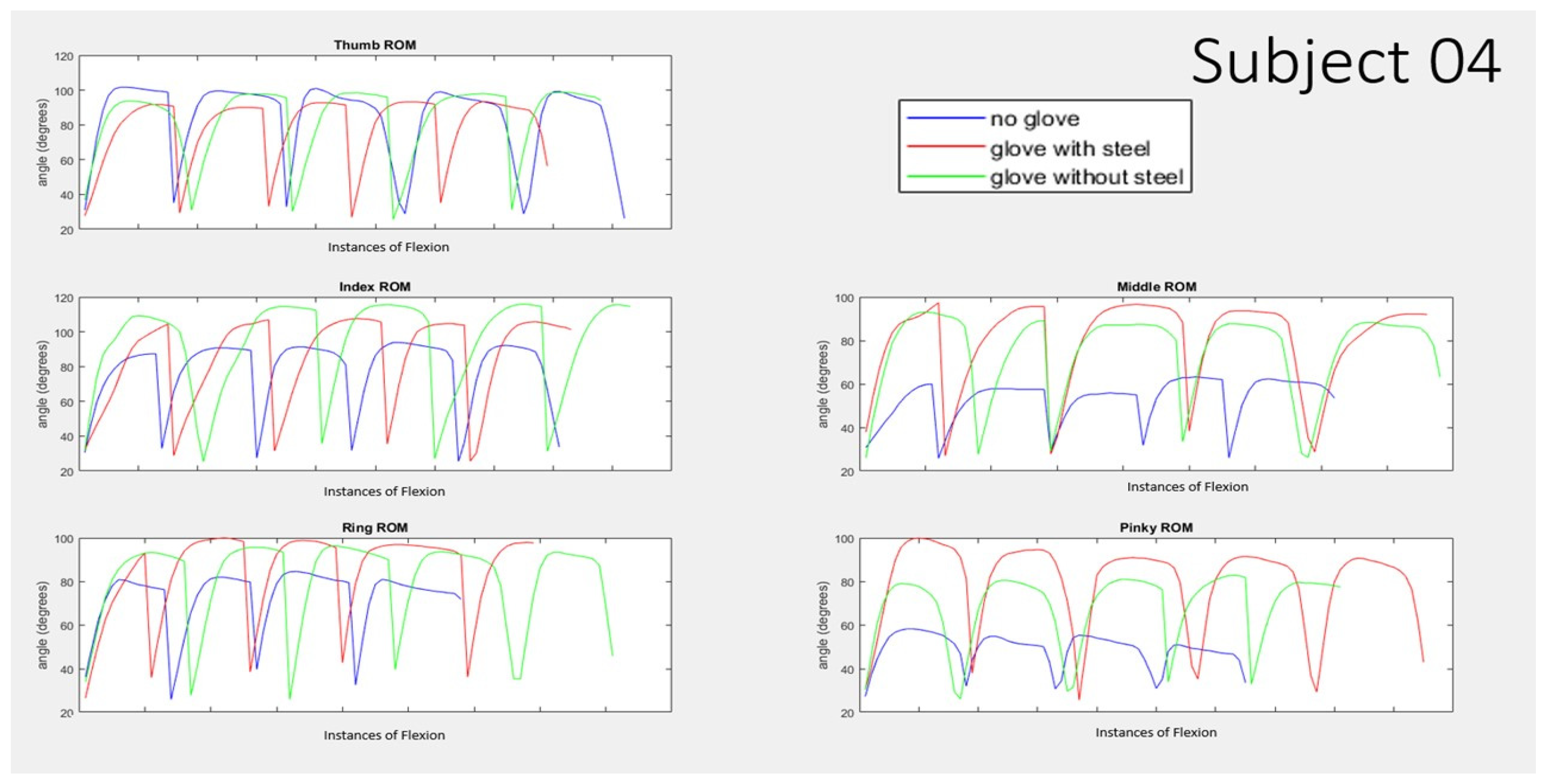
3.2. Range of Motion Testing on Human Subjects
3.3. Participants Comfort Ratings
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tsao, C.W.; Aday, A.W.; Almarzooq, Z.I.; Alonso, A.; Beaton, A.Z.; Bittencourt, M.S.; Boehme, A.K.; Buxton, A.E.; Carson, A.P.; Commodore-Mensah, Y.; et al. Heart Disease and Stroke Statistics—2022 Update: A Report from the American Heart Association. Circulation 2022, 145, e153–e639. [Google Scholar]
- Centers for Disease Control and Prevention. Underlying Cause of Death, 1999–2018. CDC WONDER Online Database. 2018. Available online: https://wonder.cdc.gov/ucd-icd10.html (accessed on 12 March 2020).
- Delgado, A. Stroke Recovery: Rehabilitation, Recovery, and Complications. Healthline, Healthline Media, 7 June 2018. Available online: https://www.healthline.com/health/stroke/recovery (accessed on 14 August 2022).
- Hatem, S.M.; Saussez, G.; della Faille, M.; Prist, V.; Zhang, X.; Dispa, D.; Bleyenheuft, Y. Rehabilitation of Motor Function after Stroke: A Multiple Systematic Review Focused on Techniques to Stimulate Upper Extremity Recovery. Front. Hum. Neurosci. 2016, 10, 442. [Google Scholar] [CrossRef]
- Sawner, K.A.; Brunnstrom, S.; La Vigne, J.M. Brunnstrom’s Movement Therapy in Hemiplegia: A Neurophysiological Approach, 2nd ed.; Lippincott: Philadelphia, PA, USA, 1992. [Google Scholar]
- Pandian, S.; Arya, K.N.; Davidson, E.R. Comparison of Brunnstrom Movement Therapy and Motor Relearning Program in Rehabilitation of Post-Stroke Hemiparetic Hand: A Randomized Trial. J. Bodyw. Mov. Ther. 2012, 16, 330–337. [Google Scholar]
- Su, F.; Xu, W. Enhancing Brain Plasticity to Promote Stroke Recovery. Front. Neurol. 2020, 11, 554089. [Google Scholar] [CrossRef]
- Polygerinos, A.; Lyne, S.; Zheng, W.; Nicolini, F.L.; Whitesides, G.; Walsh, C. Towards a soft pneumatic glove for hand rehabilitation. In Proceedings of the 2013 IEEE/RSJ International Conference on Intelligent Robots and Systems, Tokyo, Japan, 3–7 November 2013; pp. 1512–1517. [Google Scholar]
- Polygerinos, P.; Wang, Z.; Galloway, K.C.; Wood, R.J.; Walsh, C.J. Soft robotic glove for combined assistance and at-home rehabilitation. Robot. Auton. Syst. 2015, 73, 135–143. [Google Scholar]
- Polygerinos, P.; Wang, Z.; Overvelde, J.T.B.; Galloway, K.C.; Wood, R.J.; Bertoldi, K.; Walsh, C.J. Modeling of Soft Fiber-Reinforced Bending Actuators. IEEE Trans. Robot. 2015, 31, 778–789. [Google Scholar]
- Heung, K.H.L.; Tong, R.K.Y.; Lau, A.T.H.; Li, Z. Robotic Glove with Soft-Elastic Composite Actuators for Assisting Activities of Daily Living. Soft Robot. 2019, 6, 289–304. [Google Scholar]
- Gerges, F.; Desai, J. Design of a Low Pressure Pneumatically Actuated Soft Robotic Glove for Stroke Rehabilitation. Biomed. Sci. Instrum. 2020, 56. [Google Scholar]
- Wang, Z.; Polygerinos, P.; Overvelde, J.T.; Galloway, K.C.; Bertoldi, K.; Walsh, C.J. Interaction Forces of Soft Fiber Reinforced Bending Actuators. IEEE/ASME Trans. Mechatron. 2017, 22, 717–727. [Google Scholar]
- Yap, H.K.; Lim, J.H.; Nasrallah, F.; Yeow, C.H. Design and preliminary feasibility study of a soft robotic glove for hand function assistance in stroke survivors. Front. Neurosci. 2017, 11, 547. [Google Scholar]
- Park, J.; Hwang, I.; Lee, W. Wearable Robotic Glove Design Using Surface-Mounted Actuators. Front. Bioeng. Biotechnol. 2020, 8, 548947–548959. [Google Scholar] [CrossRef]
- Park, S.; Weber, L.; Bishop, L.; Stein, J.; Ciocarlie, M. Design and development of effective transmission mechanisms on a tendon driven hand orthosis for stroke patients. In Proceedings of the 2018 IEEE International Conference on Robotics and Automation (ICRA), Brisbane, QLD, Australia, 21–25 May 2018; pp. 2281–2287. [Google Scholar] [CrossRef]
- Stano, G.; Percoco, G. Additive manufacturing aimed to soft robots fabrication: A review. Extrem. Mech. Lett. 2021, 42, 101079. [Google Scholar] [CrossRef]
- Zolfagharian, A.; Mahmud, M.P.; Gharaie, S.; Bodaghi, M.; Kouzani, A.Z.; Kaynak, A. 3D/4D-printed bending-type soft pneumatic actuators: Fabrication, modelling, and control. Virtual Phys. Prototyp. 2020, 15, 373–402. [Google Scholar]
- Tawk, C.; Mutlu, R.; Alici, G. A 3D Printed Modular Soft Gripper Integrated with Metamaterials for Conformal Grasping. Front. Robot. AI 2022, 8, 799230. [Google Scholar] [CrossRef]
- Stano, G.; Arleo, L.; Percoco, G. Additive Manufacturing for Soft Robotics: Design and Fabrication of Airtight, Monolithic Bending PneuNets with Embedded Air Connectors. Micromachines 2020, 11, 485. [Google Scholar] [CrossRef]
- Marechal, L.; Balland, P.; Lindenroth, L.; Petrou, F.; Kontovounisios, C.; Bello, F. Toward a Common Framework and Database of Materials for Soft Robotics. Soft Robot. 2021, 8, 284–297. [Google Scholar]
- Jing, X.; Chen, S.; Zhang, C.; Xie, F. Increasing Bending Performance of Soft Actuator by Silicon Rubbers of Multiple Hardness. Machines 2022, 10, 272. [Google Scholar] [CrossRef]
- Li, S.; Francisco, G.E. New insights into the pathophysiology of post-stroke spasticity. Front. Hum. Neurosci. 2015, 9, 192. [Google Scholar] [CrossRef]
- Yap, H.K.; Lim, J.H.; Goh, J.C.H.; Yeow, C.H. Design of a soft robotic glove for hand rehabilitation of stroke patients with clenched fist deformity using inflatable plastic actuators. J. Med. Dev. 2016, 10, 044504. [Google Scholar] [CrossRef]
- Singh, A.P. Hand Anatomy and Function. Bone and Spine. Boneandspine.Com. Available online: https://boneandspine.com/hand-anatomy-and-function/ (accessed on 12 November 2019).
- Jarque-Bou, N.J.; Vergara, M.; Sancho-Bru, J.L. Estimation of the Abduction/Adduction Movement of the Metacarpophalangeal Joint of the Thumb. Appl. Sci. 2021, 11, 3158. [Google Scholar] [CrossRef]
- Arya, K.N.; Pandian, S.; Puri, V. Rehabilitation methods for reducing shoulder subluxation in post-stroke hemiparesis: A systematic review. Top Stroke Rehabil. 2018, 25, 68–81. [Google Scholar] [CrossRef]
- Mason, C.R.; Gomez, J.E.; Ebner, T.J. Hand Synergies during Reach-to-Grasp. J. Neurophysiol. 2001, 86, 2896–2910. [Google Scholar] [CrossRef]
- Nizamis, K.; Rijken, N.H.M.; Mendes, A.; Janssen, M.M.H.P.; Bergsma, A.; Koopman, B.F.J.M. A Novel Setup and Protocol to Measure the Range of Motion of the Wrist and the Hand. Sensors 2018, 18, 3230. [Google Scholar] [CrossRef]
- Zhao, J.; Jalving, R.; Huang, R.; Knepper, A.; Ruina, R.; Shepherd, J. A Helping Hand: Soft Orthosis with Integrated Optical Strain Sensors and EMG Control. IEEE Robot. Autom. Mag. 2016, 23, 55–64. [Google Scholar]
- Jiang, Y.; Chen, D.; Liu, P.; Jiao, X.; Ping, Z.; Xu, Z.; Li, J.; Xu, Y. Fishbone-inspired soft robotic glove for hand rehabilitation with multi-degrees-of-freedom. In Proceedings of the 2018 IEEE International Conference on Soft Robotics (RoboSoft), Livorno, Italy, 24–28 April 2018; pp. 394–399. [Google Scholar]
- Chizhik, D.; Hejrati, B. Development and comprehensive evaluation of a new spring-steel-driven glove for grasping assistance during activities of daily living. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2022, 236, 259–268. [Google Scholar]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Fabrication Steps | Fabrication Process |
|---|---|
| 1 | Actuators body molds and pneumatic chamber rods were designed using Dassault Systemes’ SolidWorks 2020 version. |
| 2 | Additive manufacturing used to 3D print molds and chamber rods using Polylactic acid (PLA) material. This material is easily available and not expensive. It is also supported by most of the 3D printers. |
| 3 | Dragon Skin 10 Medium, liquid silicone, was poured in the 3D printed finger molds with pneumatic chambers. This liquid silicon allows curing process which converts liquid silicon into stretchable solid form. |
| 4 | A polyester fabric layer was placed on the top that allows bending motion when pressurized. Nylon material was used. |
| 5 | The setup then placed in a room temperature for approximately 24 h prior to demolding the fabricated soft actuator. |
| 6 | Gently removed the pneumatic chamber rod from the actuator which makes the proximal area of the fabricated soft actuator open. |
| 7 | The fabricated actuator then placed vertically with an open end submerged in a small cup filled with the same liquid material for closing its end. |
| 8 | A small drill was used to create a hole at the proximal end to access the pneumatic chamber which connect with air tubes. |
| 9 | Sil-Proxy, glue for silicone, was then used to seal the connection between the air tube and the pneumatic chamber. |
| 10 | A flexible steel layer was placed between the cloth glove and the fabricated actuator followed by performing stitching around the sides. |
| Middle | Index/Ring | Thumb | Pinky | Average All Fingers | |
|---|---|---|---|---|---|
| Percent decrease in blocked tip force when adding steel layer | 15.14% | 17.61% | 18.65% | 21.13% | 18.13% |
| Active Unassisted ROM Peak Angle Data | |||
|---|---|---|---|
| Average Angle (Degrees) | Standard Error (Degrees) | ||
| Thumb | no pneumatic glove | 91.03 | 5.05 |
| with pneumatic glove without steel | 92.33 | 5.40 | |
| with pneumatic glove with steel | 96.18 | 4.10 | |
| Index | no pneumatic glove | 87.20 | 5.61 |
| with pneumatic glove without steel | 91.54 | 4.83 | |
| with pneumatic glove with steel | 97.39 | 3.53 | |
| Middle | no pneumatic glove | 68.60 | 5.48 |
| with pneumatic glove without steel | 76.62 | 6.24 | |
| with pneumatic glove with steel | 74.49 | 6.21 | |
| Ring | no pneumatic glove | 79.01 | 6.83 |
| with pneumatic glove without steel | 83.96 | 6.94 | |
| with pneumatic glove with steel | 82.51 | 7.16 | |
| Pinky | no pneumatic glove | 52.40 | 3.78 |
| with pneumatic glove without steel | 82.79 | 8.38 | |
| with pneumatic glove with steel | 86.25 | 7.34 | |
| Peak Angles and Associated Pressures for 10 Subjects | |||||||
|---|---|---|---|---|---|---|---|
| Average Values for Peak Angle, Associated Pressure, and Standard Error | % Difference of with vs. without Steel | ||||||
| Finger | Condition | Angle (Degrees) | Standard Error for Angle | Pressure (kPa) | Standard Error for Pressure | Angle (%) | Pressure (%) |
| Thumb | without steel | 61.17 | 3.97 | 92.27 | 2.32 | 3.63 | −4.79 |
| with steel | 58.95 | 4.43 | 96.69 | 3.07 | |||
| Index | without steel | 85.80 | 4.12 | 81.98 | 4.11 | −1.42 | 1.46 |
| with steel | 87.02 | 5.39 | 80.78 | 2.71 | |||
| Middle | without steel | 64.81 | 4.92 | 95.71 | 1.64 | 6.71 | −2.37 |
| with steel | 60.46 | 4.39 | 97.98 | 3.00 | |||
| Ring | without steel | 69.70 | 6.86 | 90.90 | 2.23 | 20.29 | −8.24 |
| with steel | 55.56 | 5.22 | 98.39 | 2.01 | |||
| Pinky | without steel | 97.97 | 6.69 | 96.28 | 2.69 | 24.36 | −1.85 |
| with steel | 74.11 | 5.89 | 98.06 | 1.84 | |||
| Finger | Condition | Percentage (%) |
|---|---|---|
| Thumb | without steel | 67.20 |
| with steel | 64.76 | |
| Index | without steel | 98.40 |
| with steel | 99.79 | |
| Middle | without steel | 94.48 |
| with steel | 88.13 | |
| Ring | without steel | 88.22 |
| with steel | 70.33 | |
| Pinky | without steel | 186.97 |
| with steel | 141.44 | |
| Average | without steel | 107.05 |
| with steel | 92.89 | |
| Average not including pinky | without steel | 87.07 |
| with steel | 80.75 |
| Participants’ Comfort Rating of Glove | ||||||
|---|---|---|---|---|---|---|
| Flexion | Extension | At Rest | ||||
| Average Score | Standard Deviation | Average Score | Standard Deviation | Average Score | Standard Deviation | |
| Thumb | 4.50 | 1.08 | 4.6 | 0.84 | 4.7 | 0.67 |
| Index | 3.90 | 1.6 | 3.8 | 1.55 | 4.2 | 1.48 |
| Middle | 4.5 | 0.97 | 4.4 | 1.07 | 4.3 | 1.25 |
| Ring | 4.1 | 1.2 | 4.5 | 0.97 | 4.2 | 1.48 |
| Pinky | 4.5 | 1.08 | 4.9 | 0.32 | 4.6 | 1.26 |
| Author and Reference | Year Published | Tip Force Output | Pressure Required (kPa) | Weight | Extension Method |
|---|---|---|---|---|---|
| Polygerinos et al. [10] | 2015 | 8 N | 345 | 285 g | none |
| Wang et al. [13] | 2016 | 8 N | 345 | 285 g | none |
| Zhao et al. [30] | 2016 | 5 N | 270 | / | none |
| Yap et al. [31] | 2017 | 9.12 N | 120 | 180 g | none |
| Heung et al. [11] | 2019 | / | 200 | 207 g | Torque compensating layer |
| Gerges et al. [12] | 2019 | 9.5 N | 180 | 120 g | none |
| Chizik et al. [32] | 2021 | 14 N | 120 | 196 g | Spring layer of metal |
| Rieger and Desai | 2022 | 12 N | 120 | 149 g | Steel layer |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rieger, C.; Desai, J. A Preliminary Study to Design and Evaluate Pneumatically Controlled Soft Robotic Actuators for a Repetitive Hand Rehabilitation Task. Biomimetics 2022, 7, 139. https://doi.org/10.3390/biomimetics7040139
Rieger C, Desai J. A Preliminary Study to Design and Evaluate Pneumatically Controlled Soft Robotic Actuators for a Repetitive Hand Rehabilitation Task. Biomimetics. 2022; 7(4):139. https://doi.org/10.3390/biomimetics7040139
Chicago/Turabian StyleRieger, Claire, and Jaydip Desai. 2022. "A Preliminary Study to Design and Evaluate Pneumatically Controlled Soft Robotic Actuators for a Repetitive Hand Rehabilitation Task" Biomimetics 7, no. 4: 139. https://doi.org/10.3390/biomimetics7040139
APA StyleRieger, C., & Desai, J. (2022). A Preliminary Study to Design and Evaluate Pneumatically Controlled Soft Robotic Actuators for a Repetitive Hand Rehabilitation Task. Biomimetics, 7(4), 139. https://doi.org/10.3390/biomimetics7040139