Developing a Time-Based Evaluation Method for Functional Exercises of Emergency Medical Operations

 ,
,
Abstract
1. Introduction
2. Data and Methodology
2.1. Functional Exercise for DMOC
2.2. Work Breakdown and Unit Task-Time Measurement
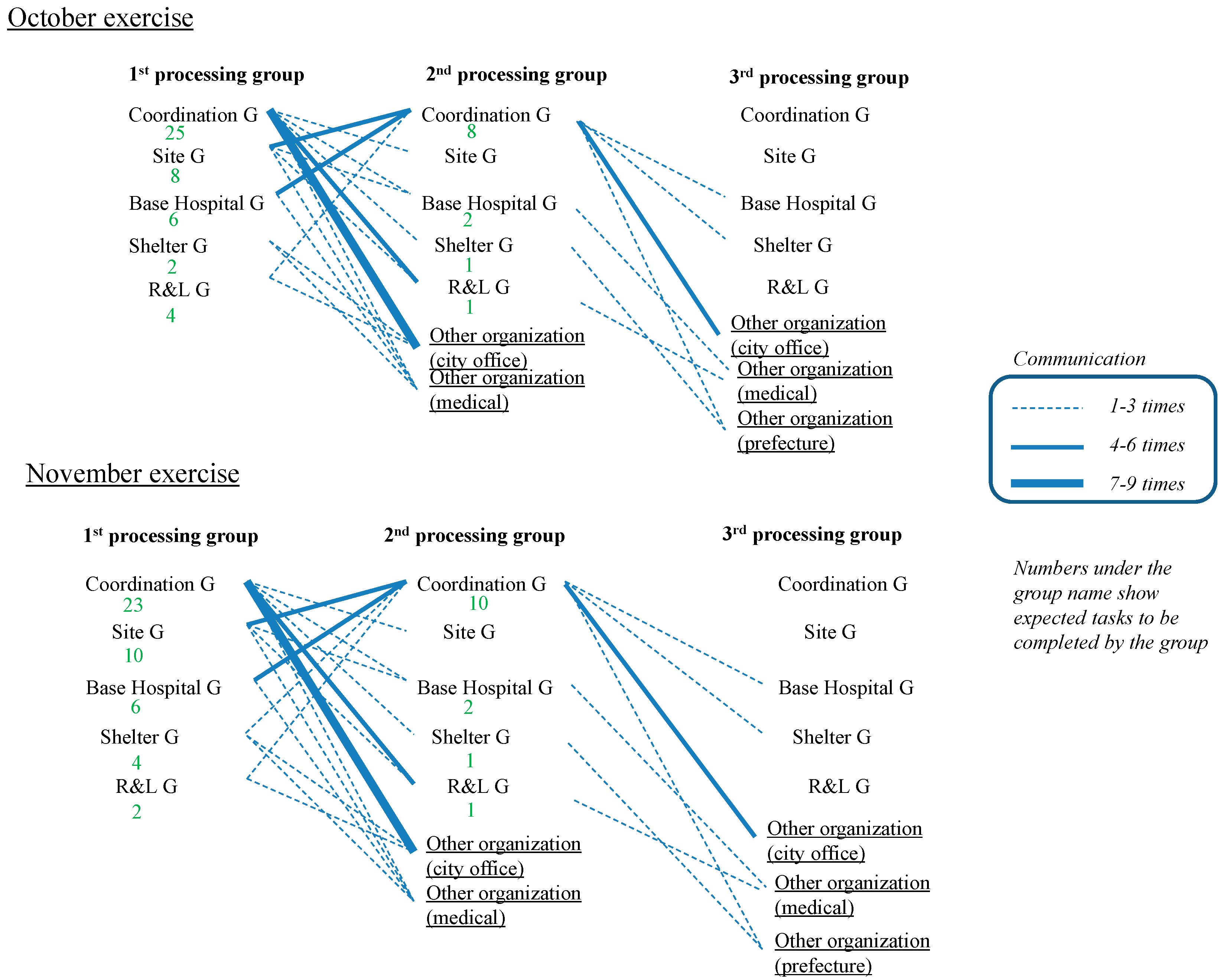
2.3. Defining Stages in the Communication Network
2.4. Defining Unit Task Types
- -
- “Request” refers to actions that send information to other groups to request certain actions toward goals. This is to send information in a task-oriented manner.
- -
- “Report” refers to when a group sends information to others to share information and understanding. This is to send information in a relationship-building manner.
- -
- “Inquiry” is defined as when one group collects or receives information from other groups to conduct subsequent tasks.
- -
- “Decision making” is defined as a set of actions in one group that includes discussion, making decisions, and delegating decisions to other groups. This unit task includes making discussions among relevant players.
2.5. Team Performance Factors
2.6. Statistical Analysis
3. Results and Discussion
3.1. Visualization of Whole Communication Network Spanning across Groups
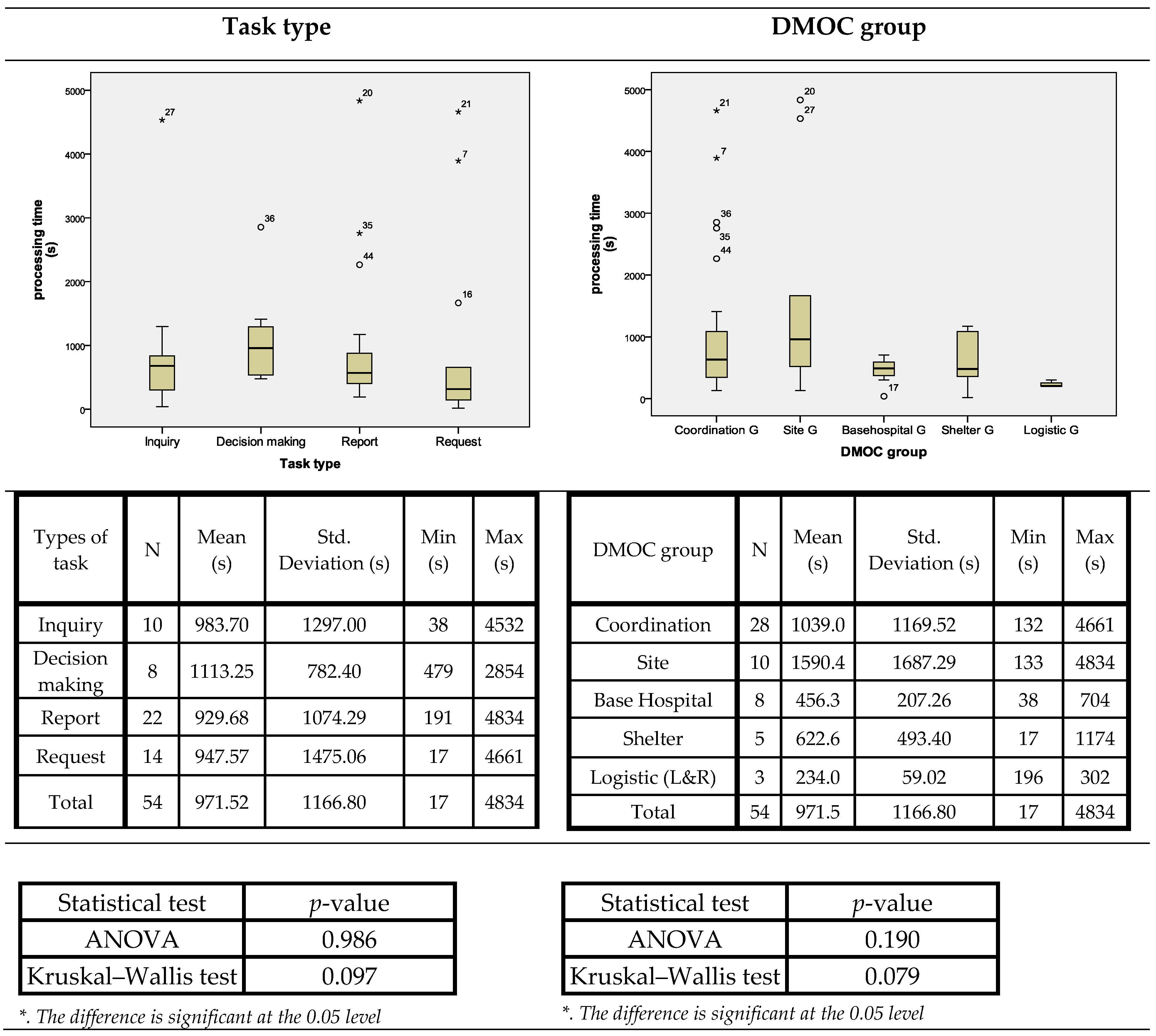
3.2. Factors of Task Processing Time
3.2.1. Analysis of the October Exercise
3.2.2. Analysis of the November Exercise
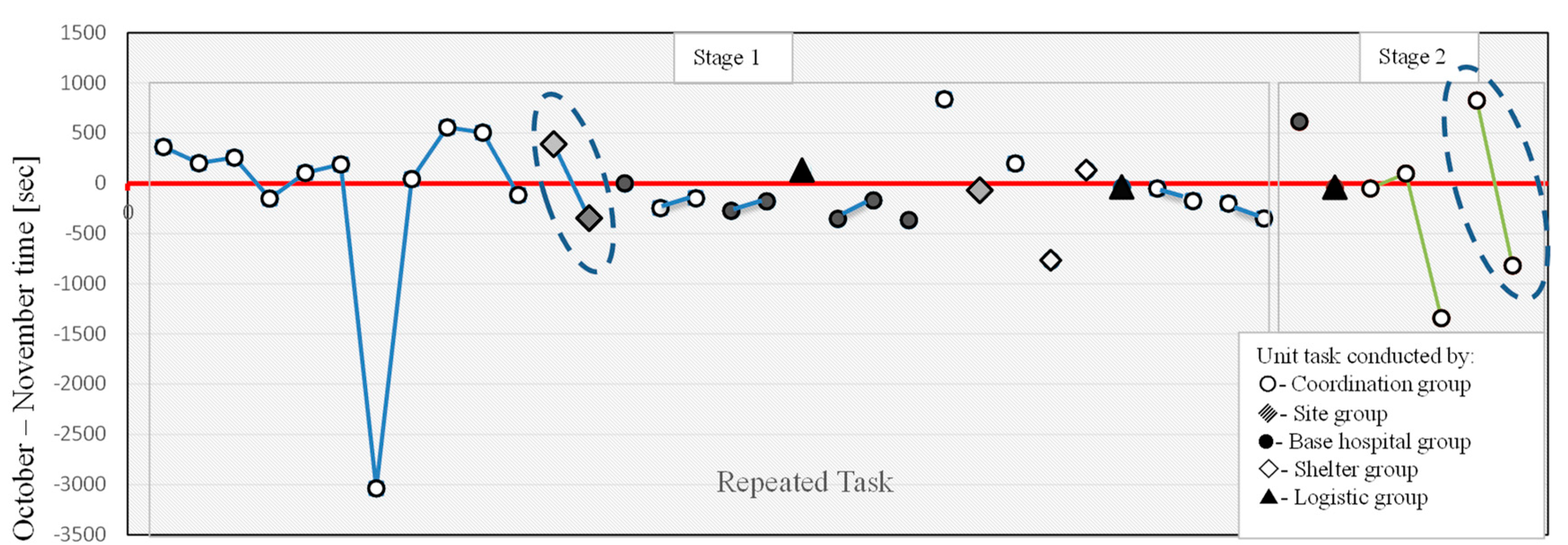
3.2.3. Analysis of Repeated Tasks in October and November Exercises
4. Conclusions and Further Implications
4.1. Conclusions
4.2. Limitations and Further Study
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Haddow, G.D.; Bullock, J.A.; Coppola, D.P. Introduction to Emergency Management, 5th ed.; Elsevier: Waltham, MA, USA, 2014; pp. 1–4. ISBN 978-0-12-407784-3. [Google Scholar]
- Lettieri, E.; Masella, C.; Radaelli, G. Disaster management: Findings from a systematic review. Disaster Prev. Manag. Int. J. 2009, 18, 117–136. [Google Scholar] [CrossRef]
- Coppola, D.P. Introduction to International Disaster Management; Elsevier: Waltham, MA, USA, 2006; pp. 1–15. ISBN 0-08-046573-0. [Google Scholar]
- Alexander, D. Principles of Emergency Planning and Management; Oxford University Press: Oxford, NY, USA, 2002; pp. 190–215. ISBN 978-0-19-521838-1. [Google Scholar]
- McLay, L.A.; Mayorga, M.E. Evaluating emergency medical service performance measures. Health Care Manag. Sci. 2010, 13, 124–136. [Google Scholar] [CrossRef] [PubMed]
- Kobusingye, O.C.; Hyder, A.A.; Bishai, D.; Joshipura, M.; Hicks, E.R.; Mock, C. Emergency medical services. Dis. Control Priorities Dev. Ctries. 2006, 2, 626–628. [Google Scholar]
- Dausey, D.J.; Buehler, J.W.; Lurie, N. Designing and conducting tabletop exercises to assess public health preparedness for manmade and naturally occurring biological threats. BMC Public Health 2007, 7, 92. [Google Scholar] [CrossRef] [PubMed]
- Skryabina, E.; Reedy, G.; Amlot, R.; Jaye, P.; Riley, P. What is the value of health emergency preparedness exercises? A scoping review study. Int. J. Disaster Risk Reduct. 2017, 21, 274–283. [Google Scholar] [CrossRef]
- Nazli, N.N.N.N.; Sipon, S.; Radzi, H.M. Analysis of training needs in disaster preparedness. Procedia Soc. Behav. Sci. 2014, 140, 576–580. [Google Scholar] [CrossRef]
- Klima, D.A.; Seiler, S.H.; Peterson, J.B.; Christmas, A.B.; Green, J.M.; Fleming, G.; Thomason, M.H.; Sing, R.F. Full-scale regional exercises: Closing the gaps in disaster preparedness. J. Trauma Acute Care Surg. 2012, 73, 592–597. [Google Scholar] [CrossRef] [PubMed]
- National Incident Management System. Available online: https://www.fema.gov/national-incident-management-system (accessed on 25 June 2019).
- International Atomic Energy Agency (IAEA). Preparation, Conduct and Evaluation of Exercises to Test Preparedness for a Nuclear or Radiological Emergency; International Atomic Energy Agency: Vienna, Austria, 2005. [Google Scholar]
- Quarantelli, E.L. Disaster crisis management: A summary of research findings. J. Manag. Stud. 1988, 25, 373–385. [Google Scholar] [CrossRef]
- Russo, F.; Rindone, C. Civil risk manager at European level. WIT Trans. Ecol. Environ. 2013, 173, 765–778. [Google Scholar]
- Muttarak, R.; Pothisiri, W. The Role of Education on Disaster Preparedness: Case Study of 2012 Indian Ocean Earthquakes on Thailand’s Andaman Coast. Ecol. Soc. 2013, 18, 51. [Google Scholar] [CrossRef]
- Homeland Security Exercise and Evaluation Program (HSEEP). Available online: https://www.fema.gov/hseep (accessed on 8 June 2019).
- Annelli, J.F. The national incident management system: A multi-agency approach to emergency response in the United States of America. Rev. Sci. Tech. Int. Off. Epizoot. 2006, 25, 223–231. [Google Scholar] [CrossRef]
- Militello, L.G.; Patterson, E.S.; Bowman, L.; Wears, R. Information flow during crisis management: Challenges to coordination in the emergency operations center. Cogn. Technol. Work 2007, 9, 25–31. [Google Scholar] [CrossRef]
- Mendonça, D.; Fiedrich, F. Training for improvisation in emergency management: Opportunities and limits for information technology. Int. J. Emerg. Manag. 2006, 3, 348–363. [Google Scholar] [CrossRef]
- Phelps, R. Emergency Management Exercises: From Response to Recovery: Everything You Need to Know to Design a Great Exercise; Chandi Media: San Francisco, CA, USA, 2011; pp. 10–18. ISBN 0-9831143-0-7. [Google Scholar]
- Johnson, Y.J.; Herrmann, J.A.; Wallace, R.L.; Troutt, H.F.; Myint, M.S. Development and Implementation of a Functional Exercise to Assess Public Health Agency Response to Foodborne Bioterrorism. J. Homel. Secur. Emerg. Manag. 2009, 6, 49. [Google Scholar] [CrossRef]
- Savoia, E.; Agboola, F.; Biddinger, P. A Conceptual Framework to Measure Systems’ Performance during Emergency Preparedness Exercises. Int. J. Environ. Res. Public. Health 2014, 11, 9712–9722. [Google Scholar] [CrossRef] [PubMed]
- Gebbie, K.M.; Valas, J.; Merrill, J.; Morse, S. Role of exercises and drills in the evaluation of public health in emergency response. Prehospital Disaster Med. 2006, 21, 173–182. [Google Scholar] [CrossRef] [PubMed]
- Russo, F.; Rindone, C. Urban exposure: Training activities and risk reduction. WIT Trans. Ecol. Environ. 2014, 191, 991–1001. [Google Scholar]
- Canton, L.G. Emergency Management: Concepts and Strategies for Effective Programs; Wiley-Interscience: Hoboken, NJ, USA, 2007; pp. 116–124. ISBN 978-0-471-73487-1. [Google Scholar]
- Harvard School of Public Health. Public Health Emergency Preparedness Exercise Evaluation Toolkit; Harvard School of Public Health: Boston, MA, USA, 2013. [Google Scholar]
- Nelson, C.; Lurie, N.; Wasserman, J. Assessing public health emergency preparedness: Concepts, tools, and challenges. Annu. Rev. Public Health 2007, 28, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Vukmir, R.B. Survival from prehospital cardiac arrest is critically dependent upon response time. Resuscitation 2006, 69, 229–234. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Mangas, R.; Garcia-Ferrrer, A.; De Juan, A.; Arroyo, A.M. The probability of death in road traffic accidents. How important is a quick medical response? Accid. Anal. Prev. 2010, 42, 1048–1056. [Google Scholar] [CrossRef] [PubMed]
- California Department of Fish and Game. Drills & Exercises and Evaluation Guidance Manual; California Department of Fish and Game: Sacramento, CA, USA, 2010.
- Center for Health Policy. Public Health Emergency Exercise Toolkit; Columbia University: Columbia, NY, USA, 2006. [Google Scholar]
- WebEOC. EPA OSC Response. Available online: https://response.epa.gov/_help/WebEOCUserGuide.pdf (accessed on 25 April 2019).
- Kohriyama, K.; Shigehito, I.; Takaaki, K. Saigai iryo ni hitsuyona hinichijyosei (Awareness of unusual situations in disaster medical management). Risk Taisaku Dot Com. 2016, 53, 82–84. (In Japanese) [Google Scholar]
- Jain, S. A parametric approach to emergency response project management. In Proceedings of the PMI Research Conference: New Directions in Project Management, Montreal, QC, Canada, 19 July 2006. [Google Scholar]
- Fiedrich, F.; Gehbauer, F.; Rickers, U. Optimized resource allocation for emergency response after earthquake disasters. Saf. Sci. 2000, 35, 41–57. [Google Scholar] [CrossRef]
- Simonovic, S.P.; Ahmad, S. Computer-based Model for Flood Evacuation Emergency Planning. Nat. Hazards 2005, 34, 25–51. [Google Scholar] [CrossRef]
- Kitakyushu Fire Department. Kitakyushu Functional Exercise After Action Report; Kitakyushu Fire Department: Kitakyushu, Japan, 2008. (In Japanese) [Google Scholar]
- Taylor, F.W. The Principles of Scientific Management; Harper & Brothers: New York, NY, USA, 1911; pp. 1–77. [Google Scholar]
- Payne, S.C.; Youngcourt, S.S.; Watrous, K.M. Portrayals of F.W. Taylor across textbooks. J. Manag. Hist. 2006, 12, 385–407. [Google Scholar] [CrossRef]
- Monden, Y. Toyota Production System: An Integrated Approach to Just-in-Time, 4th ed.; CRC Press: Boca Raton, FL, USA, 2012; pp. 137–177. ISBN 978-1-4398-2097-1. [Google Scholar]
- Annett, J.; Duncan, K.D. Task analysis and training design. J. Occup. Psychol. 1967, 41, 211–221. [Google Scholar]
- Annett, J.; Stanton, N.A. Task Analysis; CRC Press: Boca Raton, FL, USA, 2000; pp. 9–24. ISBN 978-1-4200-2298-8. [Google Scholar]
- Habermas, J. What is universal pragmatics? In Communication and the Evolution of Society; McCarthy, T., Translator; Beacon Press: Boston, MA, USA, 1979; pp. 1–68. [Google Scholar]
- McGrath, J.E. Social Psychology: A Brief Introduction; Holt, Rinehart and Winston: London, UK, 1970; pp. 10–28. ISBN 978-0-03-910078-0. [Google Scholar]
- Gladstein, D.L. Groups in Context: A Model of Task Group Effectiveness. Adm. Sci. Q. 1984, 29, 499. [Google Scholar] [CrossRef]
- Hackman, J.R. The design of work teams. In Handbook of Organizational Behavior; Lorsch, J., Ed.; Prentice-Hall: Englewood Cliffs, NJ, USA, 1987; pp. 315–342. [Google Scholar]
- Jex, S.M.; Britt, T.W. Organizational Psychology: A Scientist-Practitioner Approach, 3rd ed.; Wiley: Hoboken, NJ, USA, 2014; pp. 411–436. ISBN 978-1-118-72407-1. [Google Scholar]
- Ministry of Health Malaysia. Manual on Mental Health and Psychosocial Response to Disaster in Community; Ministry of Health Malaysia: Putrajaya, Malaysia, 2013.
- Kowalski-Trakofler, K.M.; Vaught, C.; Scharf, T. Judgment and decision making under stress: An overview for emergency managers. Int. J. Emerg. Manag. 2003, 1, 278. [Google Scholar] [CrossRef]
- Hartsough, D.M.; Myers, D.G. Disaster Work and Mental Health: Prevention and Control of Stress among Workers; National Institute of Mental Health: Rockville, MD, USA, 1985.
- Mitchell, J.T.; Dyregrov, A. Traumatic stress in disaster workers and emergency personnel. In International Handbook of Traumatic Stress Syndromes; Springer: Berlin/Heidelberg, Germany, 1993; pp. 905–914. [Google Scholar]
- Janis, I.L. Decision making under stress. Handb. Stress Theor. Clin. Asp. 1982, 2, 56–74. [Google Scholar]
- Driskell, J.E.; Salas, E. Group decision making under stress. J. Appl. Psychol. 1991, 76, 473. [Google Scholar] [CrossRef]
- Driskell, J.E.; Salas, E.; Johnston, J. Does stress lead to a loss of team perspective? Group Dyn. Theory Res. Pract. 1999, 3, 291. [Google Scholar] [CrossRef]
- Poulton, E.C. Arousing environmental stresses can improve performance, whatever people say. Aviat. Space Environ. Med. 1976, 5, 1193–1204. [Google Scholar]
- West, R.; MacDougal, K.; Ward, L. Analyzing fatigue, stress and human errors in Emergency Operation Centre management: The consequences of using different cognitive modelling frameworks. In Proceedings of the 14th International Conference on Cognitive Modeling, University Park, PA, USA, 13 July 2016. [Google Scholar]
- Brown, C.; Hearty, L.; Heideman, M.; Moran, C.; Pearce, L. Guidebook for Team Support Workers in Emergency Operation Centers; Justice Institute of British Columbia: New Westminster, BC, Canada, 2015. [Google Scholar]
- Maddala, G.S. Limited-Dependent and Qualitative Variables in Econometrics; Cambridge University Press: Cambridge, UK, 1983; pp. 149–182. ISBN 978-0-511-81017-6. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Potential Factors of Task Processing Time | Availability of Data in DMOC Exercises | |
|---|---|---|
| Individual level | Member skills and training | Not observed |
| Personality characteristics of team member | Not observed | |
| Group level | Structure of group | Communication domain |
| Level of cohesiveness | Not observed | |
| Group size | Number of members in each group | |
| Environmental level | Task characteristic | Unit task types |
| Level of heavy workload at a particular time | Number of simultaneously processed unit tasks in a group | |
| Temporal phase | Stages of team project | Elapsed time |
| Stage in communication network | ||
| Variable | Variable Types (Unit) |
|---|---|
| DMOC group | Dummy variable Coordination Site Base Hospital Shelter Logistics and Reinforcement (L&R) |
| Communication domain | Dummy variable Within DMOC With outside groups |
| Unit task type | Dummy variable Report Request Inquiry Decision making |
| Simultaneously processed unit tasks | Countable number (piece) |
| Elapsed time | Continues number (second) |
| Stage in communication network | Dummy variable Stage 1 Stage 2 |
| Variable | Coefficient | p-Value |
|---|---|---|
| Constant | 1746.0 ** | 0.000 |
| DMOC groups | ||
| Base Hospital Group | −1153.9 ** | 0.004 |
| Shelter Group | −840.0 * | 0.023 |
| Logistics and Reinforcement (L&R) Group | −630.0 | 0.117 |
| Coordination Group | −618.9 | 0.072 |
| Communication domain (within DMOC) | 482.5 | 0.053 |
| Unit task type | ||
| Inquiry | −1063.4 * | 0.012 |
| Report | −855.2 ** | 0.005 |
| Request | −1186.3 ** | 0.008 |
| Simultaneously processed unit tasks | 35.0 | 0.326 |
| Elapsed time | 0.004 | 0.942 |
| Stage (Stage 1) | −758.5 * | 0.017 |
| Number of observations | 57 | |
| Uncensored/right censored | 54/3 | |
| Wald chi-square (11) | 29.39, p = 0.002 | |
| Log pseudo likelihood | −425.221 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
To, N.T.; Kato, T.; Imai, M.; Taninobu, M.; Kohriyama, K.; Ito, S. Developing a Time-Based Evaluation Method for Functional Exercises of Emergency Medical Operations. Safety 2019, 5, 49. https://doi.org/10.3390/safety5030049
To NT, Kato T, Imai M, Taninobu M, Kohriyama K, Ito S. Developing a Time-Based Evaluation Method for Functional Exercises of Emergency Medical Operations. Safety. 2019; 5(3):49. https://doi.org/10.3390/safety5030049
Chicago/Turabian StyleTo, Ngoc Thang, Takaaki Kato, Misaki Imai, Masao Taninobu, Kazuaki Kohriyama, and Shigehiko Ito. 2019. "Developing a Time-Based Evaluation Method for Functional Exercises of Emergency Medical Operations" Safety 5, no. 3: 49. https://doi.org/10.3390/safety5030049
APA StyleTo, N. T., Kato, T., Imai, M., Taninobu, M., Kohriyama, K., & Ito, S. (2019). Developing a Time-Based Evaluation Method for Functional Exercises of Emergency Medical Operations. Safety, 5(3), 49. https://doi.org/10.3390/safety5030049