Evaluating Food Safety Knowledge and Practices among Foodservice Staff in Al Madinah Hospitals, Saudi Arabia




Abstract
:1. Introduction
2. Materials and Methods
2.1. Questionnaire Design
2.2. Target Participants
2.3. Data Collection
2.4. Data Analysis
3. Result and Discussion
3.1. Samples Profile
3.2. Food Safety Training
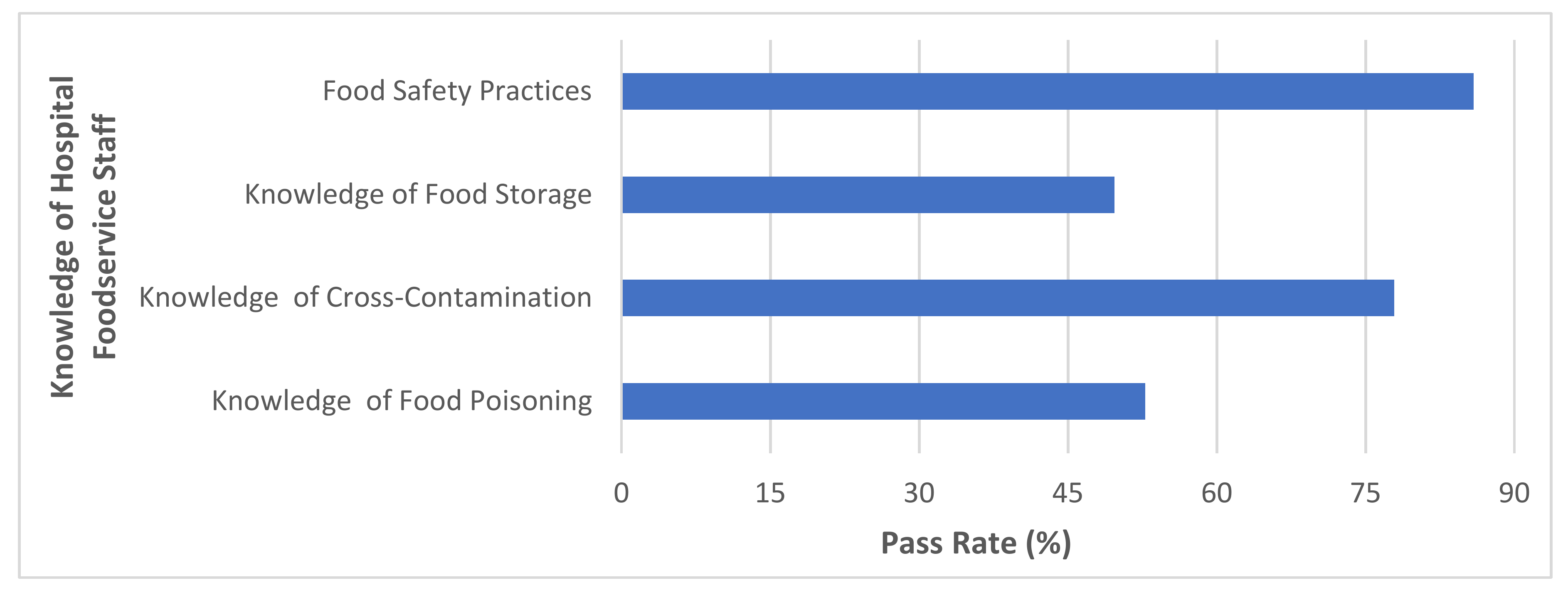
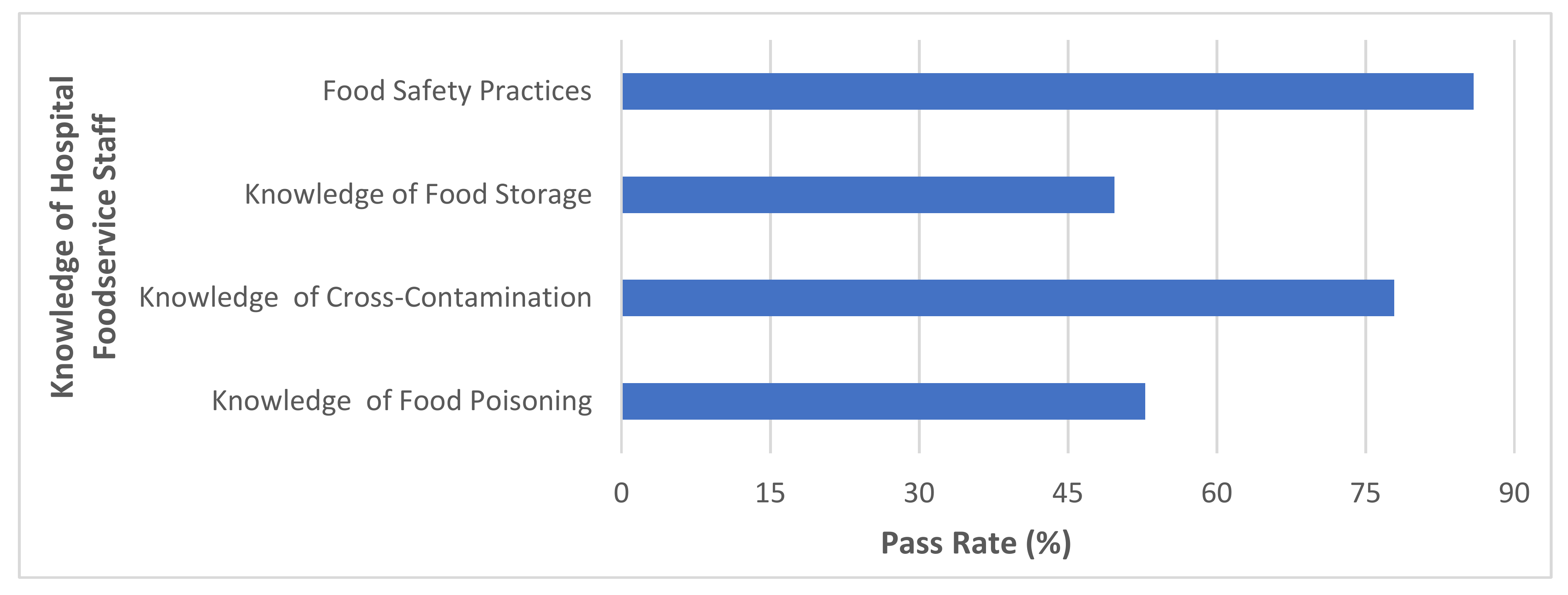
3.3. Food Handlers’ Knowledge
3.3.1. Knowledge of Food Poisoning
3.3.2. Knowledge of Cross-Contamination
3.3.3. Knowledge of Food Storage
3.4. Food Handlers’ Practices
3.5. Association between the Demographic Characteristics of Participants and Food Safety Knowledge
3.6. Association between the Demographic Characteristics of Participants and Food Safety Practices
3.7. Bivariate Correlation between Food Safety Knowledge and Food Safety Practices Using Spearman Rho Coefficient
3.8. Influence of Food Safety Knowledge on Food Safety Practices Using Linear Regression Model
3.9. Influence of Demographic Characteristics on Food Safety Knowledge and Food Safety Practices Using Linear Regression Model
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO Fact Sheet. Available online: http://www.who.int/mediacentre/factsheets/fs399/en/ (accessed on 17 November 2017).
- Omari, R.; Frempong, G. Food safety concerns of fast food consumers in urban Ghana. Appetite 2016, 98, 49–54. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Joint External Evaluation of IHR Core Capacities of the Kingdom of Saudi Arabia: Mission Report; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- Haapala, I.; Probart, C. Food safety knowledge, perceptions, and behaviors among middle school students. J. Nutr. Educ. Behav. 2004, 36, 71–76. [Google Scholar] [CrossRef]
- Ministry of Health Portal, Saudi Arabia. Available online: http://www.moh.gov.sa/en/Ministry/Pages/default.aspx (accessed on 17 July 2018).
- Ayaz, W.; Priyadarshini, A.; Jaiswal, A. Food Safety Knowledge and Practices among Saudi Mothers. Foods 2018, 7, 193. [Google Scholar] [CrossRef] [PubMed]
- Food and Agricultural Organization. National Food Safety Systems in the Near East–A Situational Analysis. Available online: ftp://ftp.fao.org/es/esn/food/meetings/NE_wp3_en.pdf (accessed on 4 July 2018).
- Al-Kandari, D.; Jukes, D.J. A situation analysis of the food control systems in Arab Gulf Cooperation Council (GCC) countries. Food Control 2009, 20, 1112–1118. [Google Scholar] [CrossRef]
- Barrie, D. The provision of food and catering services in hospital. J. Hosp. Infect. 1996, 33, 13–33. [Google Scholar] [CrossRef]
- Lund, B.; Hunter, P. The Microbiological Safety of Food in Healthcare Settings; John Wiley & Sons: Hoboken, NJ, USA, 2008. [Google Scholar]
- Arduser, L.; Brown, D.R. HACCP and Sanitation in Restaurants and Food Service Operations, Atlantic Publishing Company. Available online: http://sphweb.bumc.bu.edu/otlt/MPH-Modules/BS/BS704_/BS704_Nonparametric2.html (accessed on 17 November 2017).
- Lund, B.M. Microbiological food safety for vulnerable people. Int. J. Environ. Res. Public Health 2015, 12, 10117–10132. [Google Scholar] [CrossRef] [PubMed]
- Sumarjan, N.; Mohd, Z.M.S.; Mohd, R.S.; Zurinawati, M.; Mohd, H.M.H.; Saiful, B.M.F.; Hanafiah, M. Hospitality and Tourism: Synergizing Creativity and Innovation in Research; CRC Press: Boca Raton, FL, USA, 2013. [Google Scholar]
- Acikel, C.H.; Ogur, R.; Yaren, H.; Gocgeldi, E.; Ucar, M.; Kir, T. The hygiene training of food handlers at a teaching hospital. Food Control 2008, 19, 186–190. [Google Scholar] [CrossRef]
- Moreb, N.A.; Priyadarshini, A.; Jaiswal, A.K. Knowledge of food safety and food handling practices amongst food handlers in the Republic of Ireland. Food Control 2017, 80, 341–349. [Google Scholar] [CrossRef]
- Gong, S.; Wang, X.; Yang, Y.; Bai, L. Knowledge of food safety and handling in households: A survey of food handlers in Mainland China. Food Control 2016, 64, 45–53. [Google Scholar] [CrossRef]
- Sullivan, L. Nonparametric Test. Boston University School of Public Health, 2016. Available online: http://sphweb.bumc.bu.edu/otlt/MPH-Modules/BS/BS70_Nonparametric/BS704_Nonparametric2.html (accessed on 1 January 2017).
- Lindgreen, A.; Hingley, M.K.; Angell, R.J.; Memery, J. A Stakeholder Approach to Managing Food: Local, National and Global Issues; Routledge: New York, NY, USA, 2016. [Google Scholar]
- Askarian, M.; Kabir, G.; Aminbaig, M.; Memish, Z.A.; Jafari, P. Knowledge, attitudes, and practices of food service staff regarding food hygiene in Shiraz, Iran. Infect. Control Hosp. Epidemiol. 2004, 25, 16–20. [Google Scholar] [CrossRef] [PubMed]
- Buccheri, C.; Casuccio, A.; Giammanco, S.; Giammanco, M.; La Guardia, M.; Mammina, C. Food safety in hospital: Knowledge, attitudes and practices of nursing staff of two hospitals in Sicily, Italy. BMC Health Serv. Res. 2007, 7, 3745. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.K.; Abdul Halim, H.; Thong, K.L.; Chai, L.C. Assessment of food safety knowledge, attitude, self-reported practices, and microbiological hand hygiene of food handlers. Int. J. Environ. Res. Public Health 2017, 14, 55. [Google Scholar] [CrossRef]
- Lestantyo, D.; Husodo, A.H.; Iravati, S.; Shaluhiyah, Z. Safe Food Handling Knowledge, Attitude and Practice of Food Handlers in Hospital Kitchen. Int. J. Public Health Sci. 2017, 6, 324–330. [Google Scholar] [CrossRef]
- Osaili, T.M.; Obeidat, B.A.; Hajeer, W.A.; Al-Nabulsi, A.A. Food safety knowledge among food service staff in hospitals in Jordan. Food Control 2017, 78, 279–285. [Google Scholar] [CrossRef]
- Bou-Mitri, C.; Mahmoud, D.; Gerges, N. El.; Jaoude, M.A. Food safety knowledge, attitudes and practices of food handlers in lebanese hospitals: A cross-sectional study. Food Control 2018, 94, 78–84. [Google Scholar] [CrossRef]
- Al Kaabi, S.K.; lbrahim, A.A.E.; Salama, R.E. Assessment of Knowledge, Attitude and Practice of Food Safety Among Food Service Staff at Hamad General Hospital in 2006. Qatar Med. J. 2010, 19, 14–16. [Google Scholar] [CrossRef]
- Woh, P.Y.; Thong, K.L.; Behnke, J.M.; Lewis, J.W.; Zain, S.N.M. Evaluation of basic knowledge on food safety and food handling practices amongst migrant food handlers in Peninsular Malaysia. Food Control 2016, 70, 64–73. [Google Scholar] [CrossRef]
- Patah, M.O.R.A.; Issa, Z.M.; Nor, K.M. Food Safety Attitude of Culinary Arts Based Students in Public and Private Higher Learning Institutions (IPT). Int. Educ. Stud. 2009, 2, 168–178. [Google Scholar]
- Carbas, B.; Cardoso, L.; Coelho, A.C. Investigation on the knowledge associated with foodborne diseases in consumers of northeastern Portugal. Food Control 2013, 30, 54–57. [Google Scholar] [CrossRef]
- Fein, S.B.; Lando, A.M.; Levy, A.S.; Teisl, M.F.; Noblet, C. Trends in US consumers’ safe handling and consumption of food and their risk perceptions, 1988 through 2010. J. Food Prot. 2011, 74, 1513–1523. [Google Scholar] [CrossRef] [PubMed]
- Tabrizi, J.S.; Nikniaz, L.; Sadeghi-Bazargani, H.; Farahbakhsh, M.; Nikniaz, Z. Determinants of the food safety knowledge and practice among Iranian consumers: A population-based study from northwest of Iran. Br. Food J. 2017, 119, 357–365. [Google Scholar] [CrossRef]
- Al-Mohaithef, M. Food Hygiene in Hospitals: Evaluating Food Safety Knowledge, Attitudes and Practices of Foodservice Staff and Prerequisite Programs in Riyadh’s Hospitals, Saudi Arabia. Ph.D. Thesis, University of Birmingham, Birmingham, UK, 2014. [Google Scholar]
- Angelillo, I.F.; Viggiani, N.M.; Rizzo, L.; Bianco, A. Food handlers and foodborne diseases: Knowledge, attitudes, and reported behavior in Italy. J. Food Prot. 2000, 63, 381–385. [Google Scholar] [CrossRef] [PubMed]
- Yap, L.; Francis, S.L.; Shelley, M.; Lillehoj, C.; Montgomery, D.; Winham, D.M. Risky Food Handling Practices among Community-Residing Older Adults. FASEB J. 2016, 30, 674–677. [Google Scholar]
- Smigic, N.; Djekic, I.; Martins, M.L.; Rocha, A.; Sidiropoulou, N.; Kalogianni, E.P. The level of food safety knowledge in food establishments in three European countries. Food Control 2016, 63, 187–194. [Google Scholar] [CrossRef]
- Sibanyoni, J.J.; Tshabalala, P.A.; Tabit, F.T. Food safety knowledge and awareness of food handlers in school feeding programmes in Mpumalanga, South Africa. Food Control 2017, 73, 1397–1406. [Google Scholar] [CrossRef]
- Abdul-Mutalib, N.A.; Abdul-Rashid, M.F.; Mustafa, S.; Amin-Nordin, S.; Hamat, R.A.; Osman, M. Knowledge, attitude and practices regarding food hygiene and sanitation of food handlers in Kuala Pilah, Malaysia. Food Control 2012, 27, 289–293. [Google Scholar] [CrossRef]
- Nee, S.O.; Sani, N.A. Assessment of knowledge, attitudes and practices (KAP) among food handlers at residential colleges and canteen regarding food safety. Sains Malays. 2011, 40, 403–433. [Google Scholar]
- Sharif, L.; Obaidat, M.M.; Al-Dalalah, M.R. Food hygiene knowledge, attitudes and practices of the food handlers in the military hospitals. Food Nutr. Sci. 2013, 4, 245–251. [Google Scholar] [CrossRef]
- Da Cunha, D.T.; Stedefeldt, E.; de Rosso, V.V. The role of theoretical food safety training on Brazilian food handlers’ knowledge, attitude and practice. Food Control 2014, 43, 167–174. [Google Scholar] [CrossRef]
- Rebouças, L.T.; Santiago, L.B.; Martins, L.S.; Menezes, A.C.R.; Araújo, M.D.P.N.; de Castro Almeida, R.C. Food safety knowledge and practices of food handlers, head chefs and managers in hotels’ restaurants of Salvador, Brazil. Food Control 2017, 73, 372–381. [Google Scholar] [CrossRef]
- Choudhury, M.; Mahanta, L.B.; Goswami, J.S.; Mazumder, M.D. Will capacity building training interventions given to street food vendors give us safer food? A cross-sectional study from India. Food Control 2011, 22, 1233–1239. [Google Scholar] [CrossRef]
- Stratev, D.; Odeyemi, O.A.; Pavlov, A.; Kyuchukova, R.; Fatehi, F.; Bamidele, F.A. Food safety knowledge and hygiene practices among veterinary medicine students at Trakia University, Bulgaria. J. Infect. Public Health 2017, 10, 778–782. [Google Scholar] [CrossRef] [PubMed]
- Mekasha, T.; Neela, S.; Kumela, D. Food safety knowledge, practice and attitude of food handlers in traditional hotels of Jimma Town, Southern Ethiopia. Ann. Food Sci. Technol. 2016, 17, 507–517. [Google Scholar]
- Angelillo, I.F.; Viggiani, N.M.; Greco, R.M.; Rito, D. HACCP and food hygiene in hospitals knowledge, attitudes, and practices of food-services staff in Calabria, Italy. Infect. Control Hosp. Epidemiol. 2001, 22, 363–369. [Google Scholar] [CrossRef] [PubMed]
- Howes, M.; McEwen, S.; Griffiths, M.; Harris, L. Food handler certification by home study: Measuring changes in knowledge and behavior. Dairy Food Environ. Sanit. 1996, 16, 737–744. [Google Scholar]
- McIntyre, L.; Vallaster, L.; Wilcott, L.; Henderson, S.B.; Kosatsky, T. Evaluation of food safety knowledge, attitudes and self-reported hand washing practices in FOODSAFE trained and untrained food handlers in British Columbia, Canada. Food Control 2013, 30, 150–156. [Google Scholar] [CrossRef]
- Ismail, F.H.; Chik, C.T.; Muhammad, R.; Yusoff, N.M. Food safety knowledge and personal hygiene practices amongst mobile food handlers in Shah Alam, Selangor. Procedia Soc. Behav. Sci. 2016, 222, 290–298. [Google Scholar] [CrossRef]
- Jianu, C.; Goleţ, I. Knowledge of food safety and hygiene and personal hygiene practices among meat handlers operating in western Romania. Food Control 2014, 42, 214–219. [Google Scholar] [CrossRef]
- Webb, M.; Morancie, A. Food safety knowledge of foodservice workers at a university campus by education level, experience, and food safety training. Food Control 2015, 50, 259–264. [Google Scholar] [CrossRef]
- Sani, N.A.; Siow, O.N. Knowledge, attitudes and practices of food handlers on food safety in food service operations at the Universiti Kebangsaan Malaysia. Food Control 2014, 37, 210–217. [Google Scholar] [CrossRef]
- Rosnani, A.H.; Son, R.; Mohhidin, O.; Toh, P.S.; Chai, L.C. Assessment of knowledge, attitude and practices concerning food safety among restaurant workers in Putrajaya, Malaysia. Food Sci. Qual. Manag. 2014, 32, 20–27. [Google Scholar]
- Baş, M.; Ersun, A.Ş.; Kıvanç, G. The evaluation of food hygiene knowledge, attitudes, and practices of food handlers’ in food businesses in Turkey. Food Control 2006, 17, 317–322. [Google Scholar] [CrossRef]
- Pacholewicz, E.; Barus, S.A.S.; Swart, A.; Havelaar, A.H.; Lipman, L.J.; Luning, P.A. Influence of food handlers’ compliance with procedures of poultry carcasses contamination: A case study concerning evisceration in broiler slaughterhouses. Food Control 2016, 68, 367–378. [Google Scholar] [CrossRef]

{kind=link}
| Demographic Characteristics | N (Total Number of Respondents) | Category | Respondents (N) | Percentage (%) |
|---|---|---|---|---|
| Nationality | 163 | Saudi | 99 | 60.7 |
| Non-Saudi | 64 | 39.3 | ||
| Gender | 162 | Male | 63 | 38.7 |
| Female | 99 | 60.7 | ||
| Age group | 163 | 20–30 | 84 | 51.5 |
| 31–40 | 58 | 35.6 | ||
| 41–50 | 16 | 9.8 | ||
| 51–60 | 5 | 3.1 | ||
| Education level | 163 | University degree | 94 | 57.7 |
| High school | 52 | 31.9 | ||
| Primary school | 14 | 8.6 | ||
| Less than that | 3 | 1.8 | ||
| Work experience | 163 | 1–7 years | 113 | 69.3 |
| 8–15 years | 31 | 19.0 | ||
| 16–25 years | 15 | 9.2 | ||
| More than 25 years | 4 | 2.5 |
| Questions | N | Categories | Respondents (N) | Percentage (%) |
|---|---|---|---|---|
| Have you received any food hygiene/safety practices training course? | 163 | Yes | 111 | 68.1 |
| No | 52 | 31.9 | ||
| What do you understand by “Hazard Analysis critical control Points” (HACCP)? | 163 | Food safety system by using computer | 8 | 4.9 |
| Process and temperature control | 42 | 25.8 | ||
| System to ensure safe food by identifying and controlling specific hazards | 104 | 63.8 | ||
| None of these | 9 | 5.5 |
| Questions | N | Categories | Respondents (N) | Percentage (%) |
|---|---|---|---|---|
| 1. What is food poisoning? | 163 | The illness resulting from eating food containing bacteria, viruses, pesticides, or toxins | 127 | 77.9 |
| The illness resulting from eating food containing mold, fungus, or yeast | 25 | 15.3 | ||
| The illness resulting from eating food such as egg, milk, peanuts, fish, wheat or soy | 6 | 3.7 | ||
| The illness resulting from the absence of some enzymes that are needed to digest foods fully | 5 | 3.1 | ||
| 2. Food poisoning can be divided into two categories: intoxication or infection and the difference between them is: | 163 | Intoxication is caused only by the ingestion of high dose of pathogenic cells | 41 | 25.2 |
| Intoxication is caused only by the consumption of chemical toxins | 27 | 16.6 | ||
| Intoxication is caused by the consumption of microbial or chemical toxins | 82 | 50.3 | ||
| None of these | 13 | 8.0 | ||
| 3. What are the most important factors to control the growth of bacteria? | 163 | Light and oxygen | 16 | 9.8 |
| Time and temperature | 81 | 49.7 | ||
| Oxygen and temperature | 54 | 33.1 | ||
| None of these | 12 | 7.4 | ||
| 4. Most pathogens are likely to grow at pH range of: | 163 | Less than 1 | 38 | 23.3 |
| 2–4 | 40 | 24.5 | ||
| 4–7 | 59 | 36.2 | ||
| Above 7 | 26 | 16.0 | ||
| 5. What is the most common bacteria that can cause foodborne illness? | 163 | E. coli | 16 | 9.8 |
| Salmonella | 60 | 36.8 | ||
| Bacillus cereus | 15 | 9.2 | ||
| All of the above | 72 | 44.2 | ||
| 6. How food contaminated with food poisoning bacteria can be recognized? | 163 | Tasting it | 10 | 6.1 |
| Smelling it | 20 | 12.3 | ||
| Looking at it (Changes in color or texture) | 102 | 62.6 | ||
| None of these | 31 | 19.0 | ||
| 7. How bacteria can be transferred to the food: | 163 | People | 13 | 8.0 |
| Insects | 9 | 5.5 | ||
| Raw meat and vegetables | 8 | 4.9 | ||
| All of the above | 133 | 81.6 | ||
| Pass rate (%) 52.8 Mean score ± standard deviation 0.52 ± 0.5 | ||||
| Questions | N | Categories | Respondents (N) | Percentage (%) |
|---|---|---|---|---|
| 1. Cross-contamination is the transfer of harmful microorganism from: | 163 | Food to food | 30 | 18.4 |
| Person to food | 21 | 12.9 | ||
| Contact surfaces to food | 30 | 18.4 | ||
| All of the above | 82 | 50.3 | ||
| 2. Why is it important to wash your hands after handling raw meat? | 163 | To prevent spread of bacteria | 40 | 24.5 |
| To avoid cross-contamination | 31 | 19.0 | ||
| To avoid food poisoning | 13 | 8.0 | ||
| All of the above | 79 | 48.5 | ||
| 3. What is the purpose of using gloves during preparation of food? | 163 | To protect food from any contamination | 54 | 33.1 |
| To protect food handlers from contamination | 7 | 4.3 | ||
| To protect food preparation equipment from contamination | 7 | 4.3 | ||
| Both of A and B | 95 | 58.3 | ||
| 4. Why must raw and cooked food be separated during food preparation and refrigeration? | 163 | Kitchen will be more organized | 7 | 4.3 |
| The flavor may be affected | 22 | 13.5 | ||
| To avoid cross-contamination | 124 | 76.1 | ||
| None of these | 10 | 6.1 | ||
| 5. The safe use of a cutting board and utensils for fresh produce and raw meat shall be in the case of: | 163 | Washing the cutting board and utensil with hot water | 36 | 22.1 |
| Using fresh produce before raw meat | 10 | 6.1 | ||
| Using a specific cutting board and utensils for fresh produce and another cutting board and utensils for raw meat | 113 | 69.3 | ||
| Washing the cutting board and utensils with cold water | 4 | 2.5 | ||
| 6. Which of the following is the correct way to clean the kitchen countertop and stove? | 163 | Clean with dry rag | 5 | 3.1 |
| Clean with wet rag | 11 | 6.7 | ||
| Clean with detergent and warm water | 76 | 46.6 | ||
| All of the above | 71 | 43.6 | ||
| Pass rate (%) 77.9 Mean score ± standard deviation 0.77 ± 0.41 | ||||
| Questions | N | Categories | Respondents (N) | Percentage (%) |
|---|---|---|---|---|
| 1. What is the recommended temperature for a refrigerator? | 163 | 12 °C | 24 | 14.7 |
| 4 °C | 104 | 63.8 | ||
| 1 °C | 18 | 11.0 | ||
| Below 0 °C | 17 | 10.4 | ||
| 2. Can bacteria in food be killed by freezing at −18 °C? | 163 | Yes, totally | 53 | 32.5 |
| Yes, partly | 56 | 34.4 | ||
| Not at all | 31 | 19.0 | ||
| Do not know | 23 | 14.1 | ||
| 3. Where should raw meat be stored? | 163 | The top shelf of the fridge | 75 | 46.0 |
| The bottom shelf of fridge | 50 | 30.7 | ||
| The center of fridge | 21 | 12.9 | ||
| None of those | 17 | 10.4 | ||
| 4. Should thawed meat be frozen for later use? | 163 | Yes | 38 | 23.3 |
| No | 106 | 65.0 | ||
| Maybe | 10 | 6.1 | ||
| Do not know | 9 | 5.5 | ||
| 5. What is the recommended temperature for a freezer? | 163 | −18 °C | 118 | 72.4 |
| −4 °C | 30 | 18.4 | ||
| 0 °C | 8 | 4.9 | ||
| 4 °C | 7 | 4.3 | ||
| 6. How often do you check the temperature of the refrigerator and the freezer? | 163 | everyday | 127 | 77.9 |
| every two days | 14 | 8.6 | ||
| every week | 14 | 8.6 | ||
| every month | 8 | 4.9 | ||
| 7. Where should fruit and vegetables be stored? | 163 | The top shelf of the fridge | 43 | 26.4 |
| The bottom shelf of fridge | 57 | 35.0 | ||
| The center of fridge | 55 | 33.7 | ||
| None of those | 8 | 4.9 | ||
| Pass rate (%) 49.7 Mean score ± standard deviation 0.49 ± 0.50 | ||||
| Questions | N | Categories | Respondents (N) | Percentage (%) |
|---|---|---|---|---|
| 1. How often do you wash your hands with water and soap before food preparation? | 163 | Always | 154 | 94.5 |
| Sometimes | 6 | 3.7 | ||
| My hands are already clean | 3 | 1.8 | ||
| Never | 0 | 0 | ||
| 2. How often do you wear gloves when you handle food during preparation? | 163 | I always wear gloves | 132 | 81.0 |
| I do not feel comfortable wearing gloves during the preparation of food | 6 | 3.7 | ||
| I sometimes wear gloves | 20 | 12.3 | ||
| I never wear gloves | 5 | 3.1 | ||
| 3. How often do you use mask when you prepare or distribute foods? | 163 | I use mask when I suffer from flu | 21 | 12.9 |
| I always use mask | 115 | 70.6 | ||
| I sometimes use mask | 13 | 8.0 | ||
| I find it difficult to breathe when wearing mask | 14 | 8.6 | ||
| 4. How often do you wear head covering when you prepare or distribute foods? | 163 | I always wear head covering | 134 | 82.2 |
| I do not wear head covering as I have short hair | 3 | 1.8 | ||
| I sometimes cover my head | 10 | 6.1 | ||
| I don’t like wearing head cover | 16 | 9.8 | ||
| 5. Which of the following is the correct way to wash hands? | 163 | Wash with running cold water, wipe dry | 6 | 3.7 |
| Wash with running warm water, wipe dry | 12 | 7.4 | ||
| Wash hands with cold water and soap and then wipe dry | 30 | 18.4 | ||
| Wash hands with running warm water and soap and then wipe dry | 115 | 70.6 | ||
| 6. What should food employees do if they have an infected wound on their hand? | 163 | Report the wound to the manager | 21 | 12.9 |
| Cover the wound with a clean, impermeable bandage | 8 | 4.9 | ||
| Wear disposable gloves | 15 | 9.2 | ||
| All the above | 119 | 73.0 | ||
| 7. Which of the following is the correct way to wash hands after handling raw meat? | 163 | Wipe with towel | 5 | 3.1 |
| Wash with cold water, wipe dry | 6 | 3.7 | ||
| Wash with warm water, wipe dry | 9 | 5.5 | ||
| Wash with warm water and soap, wipe dry | 143 | 87.7 | ||
| 8. Food handlers with which of the following symptoms should not cook for others? | 163 | Diarrhea and fever | 12 | 7.4 |
| Sore throat | 4 | 2.5 | ||
| Flu | 7 | 4.3 | ||
| All the above | 140 | 85.9 | ||
| Pass rate (%) 85.9 Mean score ± standard deviation 0.92 ± 0.26 | ||||
| Food Safety Knowledge | |||||
|---|---|---|---|---|---|
| Variables | N | p-Value | Pass Rate % | Mean Score | p-Value |
| Nationality Saudis | 163 | 0.05 | 46.6% | 0.7677 | 0.04 |
| Non-Saudi | 24.5% | 0.6250 | |||
| Gender Male | 162 | 0.094 | 24.7% | 0.6349 | 0.70 |
| Female | 46.3% | 0.7576 | |||
| Age groups 20–30 | 163 | 0.03 | 40.5% | 0.7857 | 0.00 |
| 31–40 | 20.2% | 0.5690 | |||
| 41–50 | 8.0% | 0.8125 | |||
| 51–60 | 2.5% | 0.8000 | |||
| Education level University degree | 163 | 0.00 | 48.5% | 0.8404 | 0.00 |
| High school | 19.6% | 0.6154 | |||
| Primary school | 3.1% | 0.3571 | |||
| Less than that | 0.0% | 0.0000 | |||
| How long have you engaged in Food service in hospitals? 1–7 years | 163 | 0.42 | 46.6% | 0.6726 | 0.49 |
| 8–15 years | 15.3% | 0.8065 | |||
| 16–25 years | 7.4% | 0.8000 | |||
| More than 25 years | 1.8% | 0.7500 | |||
| Have you received any food hygiene/safety practices training course? Yes | 163 | 0.00 | 52.8% | 0.7748 | 0.00 |
| No | 18.4% | 0.5769 | |||
| Food Safety Practices | |||||
|---|---|---|---|---|---|
| Variables | N | p-Value | Pass Rate % | Mean Score | p-Value |
| Nationality Saudis | 163 | 0.64 | 51.5% | 0.8485 | 0.09 |
| Non-Saudi | 34.4% | 0.8750 | |||
| Gender Male | 162 | 0.79 | 34% | 0.8730 | 0.25 |
| female | 52.5% | 0.8586 | |||
| Age groups 20–30 | 163 | 0.15 | 41.7% | 0.8095 | 0.10 |
| 31–40 | 31.3% | 0.8793 | |||
| 41–50 | 9.8% | 1.0000 | |||
| 51–60 | 3.1% | 1.0000 | |||
| Education level University degree | 163 | 0.05 | 52.8% | 0.9149 | 0.00 |
| High school | 27% | 0.8462 | |||
| Primary school | 4.9% | 0.5714 | |||
| Less than that | 1.2% | 0.6667 | |||
| How long have you engaged in Food service in hospitals? 1–7 years | 163 | 0.26 | 57.1% | 0.8230 | 0.49 |
| 8–15 years | 17.8% | 0.9355 | |||
| 16–25 years | 8.6% | 0.9333 | |||
| More than 25 years | 2.5% | 1.0000 | |||
| Have you received any food hygiene/safety practices training course? Yes | 163 | 0.02 | 61.3% | 0.9009 | 0.00 |
| No | 24.5% | 0.7692 | |||
| Food Safety Practice | Food Safety Knowledge | |||
|---|---|---|---|---|
| Spearman’s rho | Food safety practice | Correlation Coefficient | 1.000 | 0.209 ** |
| Sig. (2-tailed) | - | 0.007 | ||
| N | 163 | 163 | ||
| Food safety knowledge | Correlation Coefficient | 0.209 ** | 1.000 | |
| Sig. (2-tailed) | 0.007 | - | ||
| N | 163 | 163 | ||
| Mean | Std. Dev | Constant | B | p-Value | Adjusted R2 | |
|---|---|---|---|---|---|---|
| Food safety practice (dependent variable) | 5.67 | 1.54 | 3.375 | - | - | 0.223 |
| Food safety knowledge (independent variable) | 12.06 | 3.87 | - | 0.190 | 0.000 * |
| Independent Variables | Dependent Variable | |
|---|---|---|
| Food Safety Knowledge | Food Safety Practices | |
| Coefficient | Coefficient | |
| Nationality | 0.124 | 0.123 |
| Gender | 0.401 | 0.864 |
| Age | 0.246 | 0.183 |
| Education | 0.000 ** | 0.000 ** |
| Service Length | 0.011 ** | 0.532 |
| Trainings | 0.063 | 0.269 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alqurashi, N.A.; Priyadarshini, A.; Jaiswal, A.K. Evaluating Food Safety Knowledge and Practices among Foodservice Staff in Al Madinah Hospitals, Saudi Arabia. Safety 2019, 5, 9. https://doi.org/10.3390/safety5010009
Alqurashi NA, Priyadarshini A, Jaiswal AK. Evaluating Food Safety Knowledge and Practices among Foodservice Staff in Al Madinah Hospitals, Saudi Arabia. Safety. 2019; 5(1):9. https://doi.org/10.3390/safety5010009
Chicago/Turabian StyleAlqurashi, Nada Ahmad, Anushree Priyadarshini, and Amit K. Jaiswal. 2019. "Evaluating Food Safety Knowledge and Practices among Foodservice Staff in Al Madinah Hospitals, Saudi Arabia" Safety 5, no. 1: 9. https://doi.org/10.3390/safety5010009
APA StyleAlqurashi, N. A., Priyadarshini, A., & Jaiswal, A. K. (2019). Evaluating Food Safety Knowledge and Practices among Foodservice Staff in Al Madinah Hospitals, Saudi Arabia. Safety, 5(1), 9. https://doi.org/10.3390/safety5010009